
Abstract
Dietary or supplemental calcium intake has long been encouraged for optimal bone health. However, more recently, the safety of calcium supplementation has been questioned because of a possible association between supplemental calcium and cardiovascular risk. Whereas calcium may have a beneficial or neutral effect on cardiovascular risk factors such as blood pressure, cholesterol, weight, and diabetes, available evidence does not provide a definitive answer for an association with cardiovascular disease (CVD). To date, no calcium trials have studied cardiovascular disease as a primary end point, and larger trials with longer follow-up are needed. In this review, we present results from observational studies and randomized controlled trials (RCTs) that have evaluated calcium intake (dietary or supplemental) in relation to cardiovascular risk factors and cardiovascular disease as a secondary outcome. Results from RCTs are mixed regarding CVD risk in those using supplemental calcium with or without vitamin D, and more large-scale randomized trials designed specifically with CVD as the primary end point are needed. Evidence suggests that it is reasonable to encourage adequate dietary calcium intake, especially for postmenopausal women who are at greatest risk for osteoporotic fracture.
‘Recently, the role of calcium supplementation in relation to cardiovascular disease (CVD) has come into question, specifically in terms of the impact of calcium supplementation on CVD outcomes.’
Introduction
Adequate calcium intake remains an integral part of osteoporosis prevention according to guidelines from the National Osteoporosis Foundation 1 and Institute of Medicine (IOM). 2 The consensus of these organizations is that women younger than 50 years require 1000 mg of calcium daily and that women older than 50 years require 1200 mg daily, ideally through dietary consumption. Recently, the role of calcium supplementation in relation to cardiovascular disease (CVD) has come into question, specifically in terms of the impact of calcium supplementation on CVD outcomes. This review assesses the current literature on calcium supplementation and CVD outcomes, including risk factors such as blood pressure, lipids, diabetes, inflammation, and vascular calcification.
Calcium and Blood Pressure
Epidemiological data has shown that both dietary and supplemental calcium are associated with small reductions in systolic and diastolic blood pressure.3,4 Calcium downregulates the renin-angiotensin system and facilitates a more favorable sodium-potassium balance, which may explain a potential mechanism for reducing blood pressure.5,6 A diet rich in calcium (approximately 1200 mg) from dairy products and produce (such as kale and broccoli) has been associated with a relatively lower blood pressure compared with a diet higher in fat and sodium and low in calcium, magnesium, potassium, and fiber. 7 According to the National Health and Nutrition Examination Survey III (NHANES III), increased dietary calcium was associated with lower rates of age-related increase in systolic blood pressure. 8 In 2006, a Cochrane review suggested a causal association between supplemental calcium and lower blood pressure. The evidence, however, was weak because of poor quality of the studies, which often overestimated the treatment effects. 9
The most definitive study to date on calcium effects on blood pressure has been the Women’s Health Initiative (WHI) Calcium/Vitamin D Supplementation (CaD) study. This study randomized 36 282 women to daily intake of 1000 mg calcium carbonate with 400 IU vitamin D versus placebo. 10 No significant differences were found between CaD supplementation compared with placebo for mean systolic or diastolic blood pressure change over time. In the 17 122 normotensive women at baseline, CaD did not reduce either blood pressure or the risk of developing hypertension over the 7-year follow-up (relative risk [RR] = 1.01; 95% confidence interval [CI] = 0.96-1.06). Although this was a large trial, only postmenopausal women were included, so the results may not be generalizable to men or premenopausal women. In addition, blood pressure was not a primary outcome measure, and at baseline and during the trial, many women were taking personal calcium and vitamin D supplements, which may have obscured any association. Despite this limitation, subgroup analyses of participants with low calcium and vitamin D intake at baseline did not find a clinically significant blood pressure effect. 11 Whether or not the same effects would be seen without vitamin D supplementation was not determined.
Calcium and Body Weight
It has been hypothesized that calcium intake may limit weight gain by inhibiting intracellular adipocyte calcium and activating lipolysis. 12 Human and animal studies have shown that increased dietary calcium intake may reduce visceral adipose tissue accumulation, increase rate of weight loss in obese individuals, and lower adiposity in individuals with hypertension.12,13 Barr 14 evaluated data from randomized controlled trials (RCTs) of dairy products and calcium supplementation and found little evidence to support reduced body weight or fat mass from either source of calcium. In another RCT (n = 40), 1000 mg of supplemental calcium carbonate for 6 months was not found to affect weight in obese adults compared with placebo. 15 Recker et al 16 also evaluated 17 calcium supplementation trials, and only 1 demonstrated weight loss in the supplemented group after 4 years of 1200 mg calcium carbonate supplementation. In the WHI CaD trial both the CaD and placebo groups had weight gain (1.4% ± 10.5% vs 1.7% ± 12%, respectively); however, differences from baseline were significantly smaller in women assigned to calcium and vitamin D (P = .03). 10
Calcium and Lipids
Animal studies have shown that high calcium intake might protect against vascular disease by binding to intestinal fatty and bile acids and enhancing lipid excretion.17,18 A 1-year study by Reid et al 19 (n = 223 postmenopausal women) found that 1000 mg of supplemental calcium citrate resulted in positive lipid changes, including increased high-density lipoprotein (HDL) levels and increased HDL to low-density lipoprotein (LDL) cholesterol ratio. Another RCT (n = 193 men and women aged 30-74 years) demonstrated a trend toward more favorable lipid effects in the calcium group (1000 or 2000 mg calcium carbonate daily) versus placebo after 4 months. Mean total cholesterol level dropped 1.3% more in calcium groups (P = .43), and mean HDL dropped 1.1% less in the calcium group versus placebo (P = .71). 20 Short-term studies have also shown positive lipid changes with calcium supplementation.21,22
Smaller trials have found a neutral or harmful effect on lipids. In a trial of 47 women, daily supplementation with 1000 mg calcium and 800 units vitamin D3 daily had a null effect on LDL after 12 weeks. 23 As part of the WHI CaD trial, lipid assays were performed on a random sample of 6% of participants, and a significant LDL increase was found in women assigned to active CaD (0.2% ± 20.9% vs 2.6% ± 20.7%, P = .02). 10 In a further substudy (n = 1191), CaD (1000 mg calcium carbonate/400 IU vitamin D) supplementation was not associated with lipid changes over 5 years compared with placebo. 24 The authors note that further trials are needed to assess lipid effects using other doses of elemental calcium.
Calcium and Inflammation
Elevation of inflammatory biomarkers such as C-reactive protein (CRP) are predictive of CVD risk. 25 The atherothrombotic process is fueled by inflammatory activity, and research is ongoing to understand the role of reducing inflammatory biomarkers to treat CVD. 26 Calcium may play a role in inflammation because it has been shown to inhibit apoptosis mediated by cytokines. 27 However, there is limited data on the relationship between calcium supplementation and impact on inflammatory markers such as CRP and cytokines.
In a small study (n = 39) of postmenopausal women given daily calcium of 1000 mg with 800 IU vitamin D for 3 months, no change was observed in serum circulating cytokines or CRP from baseline. 23 Furthermore, in a subset of women participating in a RCT (n = 116 women), no difference in serum CRP levels was found between those randomized to 1000 mg supplemental calcium citrate daily and those randomized to placebo after 1 year. 28 Another 3-year RCT of calcium 500 mg with 700 IU vitamin D3 daily versus placebo (n = 314) also found no differences in CRP or interleukin (IL)-6. 29 In contrast, a pilot RCT evaluating the effects of vitamin D and calcium on biomarkers in 92 colorectal adenoma patients, found that calcium supplementation reduced IL-6, IL-1β, and IL-8 (decreases of 37%, 11%, and 27% respectively). 30 Further research is required to determine whether there is a relationship between calcium supplementation and inflammatory markers and whether or not this would affect CVD risk.
Calcium and Insulin
Calcium is vital for insulin-mediated intracellular processes and for optimal insulin secretion. 31 It has been hypothesized that adequate calcium intake lowers insulin resistance and reduces risk of developing type 2 diabetes. 32 Animal models have shown some evidence that calcium supplementation may protect against the development of insulin resistance, as suggested through vitamin D inhibition. 33
Large observational studies have demonstrated an inverse association between calcium intake and type 2 diabetes.29,34 In the Women’s Health Study (n = 10 066 women age ≥45), higher intake of dietary and supplemental calcium was associated with lower prevalence of metabolic syndrome (P for trend <.0001). 34 In the Nurses’ Health Study (n = 83 779), total calcium intake (from diet plus supplements) was also inversely associated with type 2 diabetes (RR = 0.79; P for trend <.001). Calcium intake >1200 mg combined with >800 IU vitamin D was associated with a 33% lower risk of type 2 diabetes compared with an intake of <600 mg and <400 IU calcium and vitamin D, respectively (RR = 0.67; 95% CI = 0.49-0.90). 29 This inverse association between calcium intake and type 2 diabetes mellitus (DM) was also found in the Black Women’s Health Study (n = 59 000 women, 21-69 years old); however, after adjusting for magnesium intake, this association was not found to be statistically significant. 35
A meta-analysis conducted in 2007 reviewed observational studies and clinical trials that assessed the role of vitamin D and calcium in glucose homeostasis. Data from the observational studies found an inverse relationship between metabolic syndrome prevalence and dairy intake (OR = 0.71; 95% CI = 0.57-0.89). This inverse association was also found with combined calcium and vitamin D intake and type 2 DM (OR = 0.82; 95% CI = 0.72-0.93). Combined evidence from clinical trials suggested that adequate daily calcium and vitamin D intake may be more effective for the prevention of type 2 DM in high-risk populations. 32
More recent trials have not demonstrated such a positive effect. In 1 RCT (n = 40), obese adults receiving a low-calorie diet were assigned to calcium carbonate 1000 mg daily or placebo for 6 months. No effect was seen on weight, body composition, insulin resistance, or blood pressure. 15 In the Calcium and Vitamin D for Diabetes Mellitus RCT (n = 92; mean age = 57 years), prediabetic participants were randomized to supplementation with calcium carbonate 800 mg or vitamin D 2000 IU daily or combined calcium and vitamin D versus placebo over 16 weeks. Vitamin D with or without calcium was shown to improve insulin secretion; however, supplementation with calcium alone did not have any significant effect. 36 More RCTs are needed to assess the role of calcium and/or vitamin D supplementation in maintaining glucose homeostasis in both healthy and prediabetic individuals.
Calcium and Vascular Calcification
Vascular and valvular calcifications are predictive of CVD events.37,38 In dialysis patients, high calcium-based phosphate binders have been associated with vascular calcification and mortality.39,40 Hypercalcemia measured by spinal X ray has also been associated with aortic calcification and is predictive of CVD events. 41 Carotid artery plaque thickness has also been found to be associated with high serum calcium levels. 42 The ensuing question remains whether calcium supplementation contributes to vascular calcification in other populations. In an ancillary WHI substudy (n = 754; age = 50-59 years; mean duration = 7 years), no association was found between CaD supplementation and coronary artery calcium as measured by cardiac computed tomography (P = .74). 43 No RCTs of calcium supplementation have been designed with vascular calcification as the primary outcome.
To date, there have been no trials evaluating the effects of calcium on CVD as the primary outcome; however, we do have data that have been extrapolated from RCTs done on fractures and osteoporosis. These data as well as data from other observational studies are presented, showing mixed results that demonstrate either a protective, harmful, or null effect of calcium supplementation on CVD risk.
Calcium and Cardiac Risk: Observational Studies
Few observational studies have demonstrated a protective association between calcium and CVD risk. In the Iowa Women’s Health Study (n = 34 486; age = 55-69 years), there was a relatively lower incidence of death from ischemic heart disease (IHD) in women with the highest calcium intake (via diet or supplements) compared with the lowest intake. 44 For women with high dietary calcium and no supplemental calcium, the IHD mortality RR was 0.63 (95% CI = 0.40-0.98), and for high supplemental calcium and low dietary calcium, the RR was 0.66 (95% CI = 0.36-1.23). These results suggest that both dietary and supplemental calcium are associated with reduced IHD mortality. 44 The Nurses’ Health Study (n = 85 764) also found that women in the highest quintile of dietary calcium intake had an adjusted RR of ischemic stroke of 0.69 (95% CI = 0.50-0.95; P for trend = .03) compared with those in the lowest quintile. 45
Other observational studies have found that dietary calcium intake is not associated with CVD risk, stroke, and coronary heart disease (CHD) mortality.46 -49 In the Japan Collaborative Cohort Study, dietary calcium intake was inversely associated with mortality from stroke in men and women but was not associated with mortality from CHD. 50 In the Health Professionals Follow-up Study (n = 39 800; age = 40-75 years), men were followed for 12 years with a dietary questionnaire. 51 Neither dietary nor supplemental intakes of calcium were associated with IHD in men (RR = 0.97, 95% CI = 0.81-1.16, and RR = 0.87, 95% CI = 0.64-1.19, respectively). 51 Another study (n = 9910) showed a marginal risk reduction in MI, stroke, or death in women (age = 60-89 years) who had received >600 days of calcium and vitamin D supplementation compared with women who received ≤90 days of supplementation during 2 years of follow-up (RR = 0.82; 95% CI = 0.67-1.01). 52
Recent observational studies have found a harmful association between supplemental calcium and CVD risk. In a prospective analysis of a population-based cohort study of women from the Kuopio Osteoporosis Risk Factor and Prevention Study (KORFPS, n = 10 555 women, age = 52-62 years), supplemental calcium or calcium plus vitamin D supplementation was associated with risk of CHD in women when compared with nonusers of supplements (RR = 1.24; 95% CI = 1.02-1.52). The study was limited, in that dose and formulation varied for both calcium and vitamin D among participants, and there was no differentiation between those on calcium or those on calcium with vitamin D. 53
The European Prospective Investigation into Cancer and Nutrition Study (n = 23 980; age = 35-64 years) evaluated calcium intake, both dietary and supplemental, and myocardial infarction (MI) risk in women. 54 An inverse association between MI and dietary calcium intake was observed (RR = 0.69; 95% CI = 0.50-0.94). However, higher risk of MI was observed among users of supplemental calcium plus other supplements compared with nonusers of any supplements (RR = 1.86; 95% CI = 1.17-2.96). In women who took supplemental calcium alone, the associated risk was even higher for MI (RR = 2.39; 95% CI = 1.12-5.12). No association with stroke or CVD mortality was observed with supplemental calcium. The authors noted a low prevalence of supplemental-calcium-only users and found that close to half of supplement users did not report the names of their supplements. It is possible that this low statistical power for calcium-only users as well as unreported supplemental calcium may have affected the accuracy of the results. 54
The National Institute of Health AARP Diet and Health Study (n = 388 229 men and women; age = 50-71 years) investigated whether dietary or supplemental calcium is associated with mortality from CVD, heart disease, and cerebrovascular disease. Mean follow-up time was 12 years, and during that time 7904 CVD deaths were reported for men and 3874 CVD deaths were reported for women. Supplemental calcium intake was associated with an increased risk of CVD mortality in men especially from heart disease (RR = 1.19; 95% CI = 1.03-1.37) but not cerebrovascular disease (RR = 1.14; 95% CI = 0.81-1.61). Interestingly, this association was not seen in women for either CVD death (RR = 1.06; 95% CI = 0.96-1.18) heart disease death (RR = 1.05; 95% CI = 0.93-1.18), or cerebrovascular disease death (RR = 1.08; 95% CI = 0.87-1.33). Dietary calcium was not associated with CVD mortality in both men and women. 55
In contrast, NHANES III (n = 20 024 men and women; age 17 years or older) found no association between dietary or supplemental calcium intake and risk of CVD death. Serum calcium levels were also measured in this study, and no association was found between serum calcium levels and dietary or supplemental calcium intake. When results were stratified by gender, low dietary calcium intake (<1000 mg/d) was associated with increased risk of CVD mortality in men, whereas in women, low dietary calcium intake was associated with decreased risk of CVD mortality (P interaction = .025). 56
The recent Swedish mammography prospective longitudinal cohort study (n = 61 433 women followed for a median of 19 years) did however show an association between higher dietary calcium intake (>1400 mg/d) compared with lower intake (600-1000 mg/d) and all-cause mortality (RR = 1.40; 95% CI = 1.17-1.67), CVD (RR = 1.49; 95% CI = 1.09-2.02), and IHD (RR = 2.14; 95% CI = 1.48-3.09). These effects were not attenuated with vitamin D intake. No association with stroke mortality was observed. No association with supplemental calcium and all-cause mortality was found except among those with concomitant high dietary calcium intake (RR = 2.57; 95% CI = 1.19-5.55). 57
In summary, except for the latter study, dietary calcium has not been associated with increased CVD or stroke risk in observational studies to date. In addition, no association has been observed between supplemental calcium and increased stroke risk. However, the question of calcium supplementation and its association with CVD risk remains controversial.44 -46,51,54
RCTs: Calcium Alone
To date, there are 5 reports from 4 RCTs that provide data on CVD outcomes in those using calcium supplementation alone versus placebo (Table 1). Baron et al 58 studied the effect of calcium on colorectal adenomas (n = 930; mean age = 61 years) using calcium carbonate 3 g daily versus placebo, over 4 years. Incidental data showed no significant difference in the occurrence of CVD or stroke between groups (50 vs 46 for CVD and 12 vs 11 for stroke—calcium vs placebo, respectively).
RCT of Calcium Only.
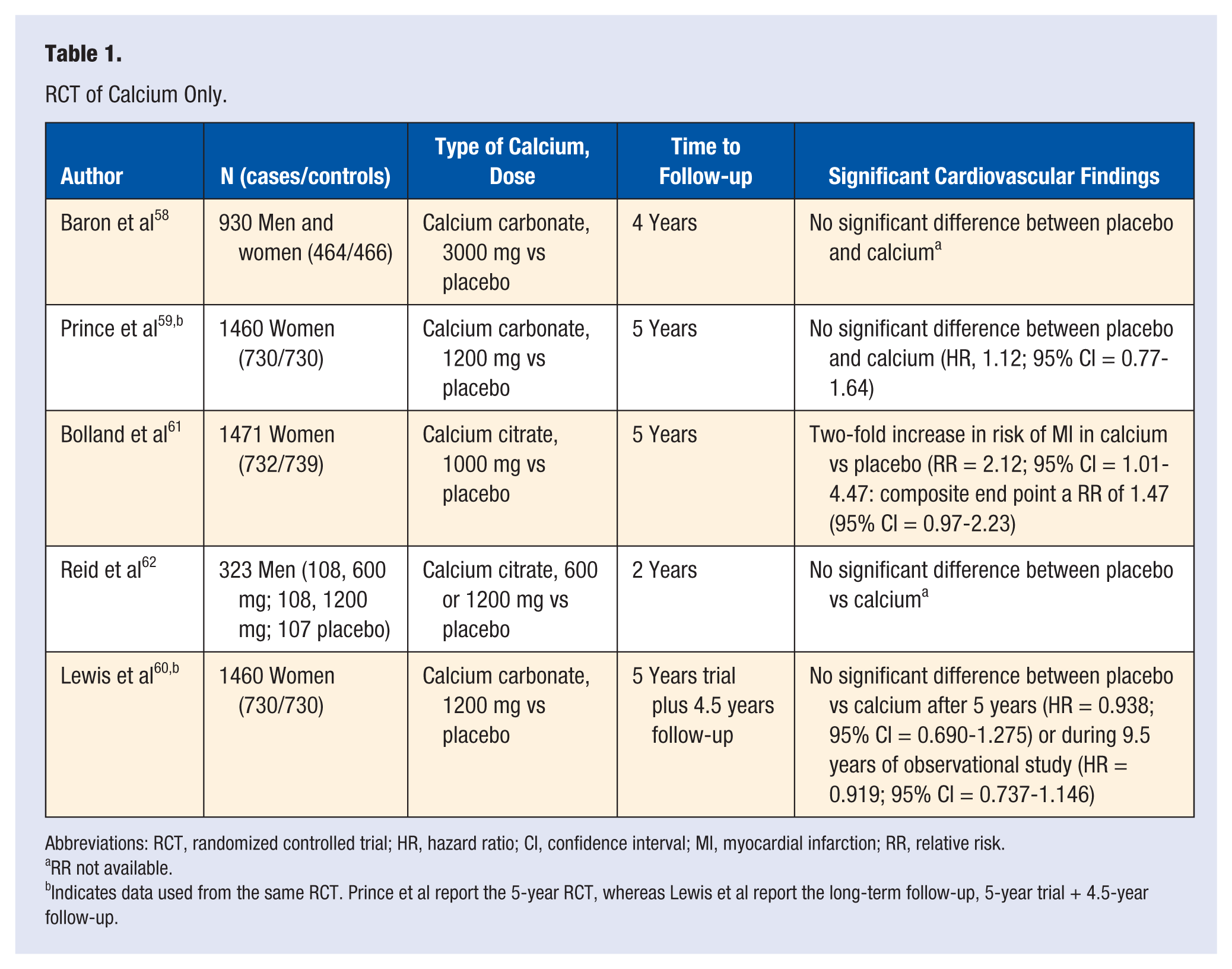
Abbreviations: RCT, randomized controlled trial; HR, hazard ratio; CI, confidence interval; MI, myocardial infarction; RR, relative risk.
RR not available.
Indicates data used from the same RCT. Prince et al report the 5-year RCT, whereas Lewis et al report the long-term follow-up, 5-year trial + 4.5-year follow-up.
An Australian study of 1460 postmenopausal women (mean age = 75 years) evaluated calcium carbonate supplementation (1200 mg/d) and fracture prevention. 59 No difference was found in IHD between the calcium group and the placebo group (RR = 1.12; 95% CI = 0.77-1.64). 59 Lewis et al 60 performed an additional analysis from this trial, which assessed the combined outcome of death or hospitalization from CVD from both the 5-year RCT and the 4.5-year follow-up. No increased risk was seen during the 5-year RCT (RR = 0.94; 95% CI = 0.69-1.28) or during the 9.5 years of RCT plus follow-up (RR = 0.92; 95% CI = 0.74-1.15).
The 5-year Auckland Calcium Bone Study of 1471 postmenopausal women (mean age = 74 years) examined the effects of calcium citrate (1000 mg daily) versus placebo on MI and a composite end point of MI, stroke, or sudden death. 61 Results found a 2-fold increased risk of self-reported MI in the calcium group versus placebo after medical record confirmation (RR = 2.12; 95% CI = 1.01-4.47) and for the composite end point (RR = 1.47; 95% CI = 0.97-2.23). However, the authors then looked further at unreported events using the national database of hospital admissions in New Zealand and found no significant increase risk in MI or composite end point (RR = 1.49, 95% CI = 0.86-2.57, P = .058 and RR = 1.21, 95% CI = 0.84-1.74, P = .043, respectively). 61
Finally, another study evaluated bone mineral density in 323 healthy men (mean age = 57 years) randomized to calcium citrate 600 mg, 1200 mg, or placebo. Vascular events were more common in both calcium groups (n = 5 events) when compared with the placebo group (n = 0); however, this was not statistically different (P = .24). 62
RCTs: Calcium Plus Vitamin D
Three trials evaluating bone mineral density or fracture incidence have reported data on CVD outcomes in women randomized to CaD supplementation versus placebo (Table 2). Brazier et al 63 looked at the safety of CaD supplementation when used to improve bone mineral density in women >65 years of age with vitamin D deficiency (n = 192). Women were randomized to receive calcium carbonate 1000 mg + vitamin D3 800 IU daily or placebo. There was no statistical difference between CVD events in the CaD group compared with the placebo group (6 vs 5 CVD events reported, respectively). 63
RCTs of Calcium Plus Vitamin D.
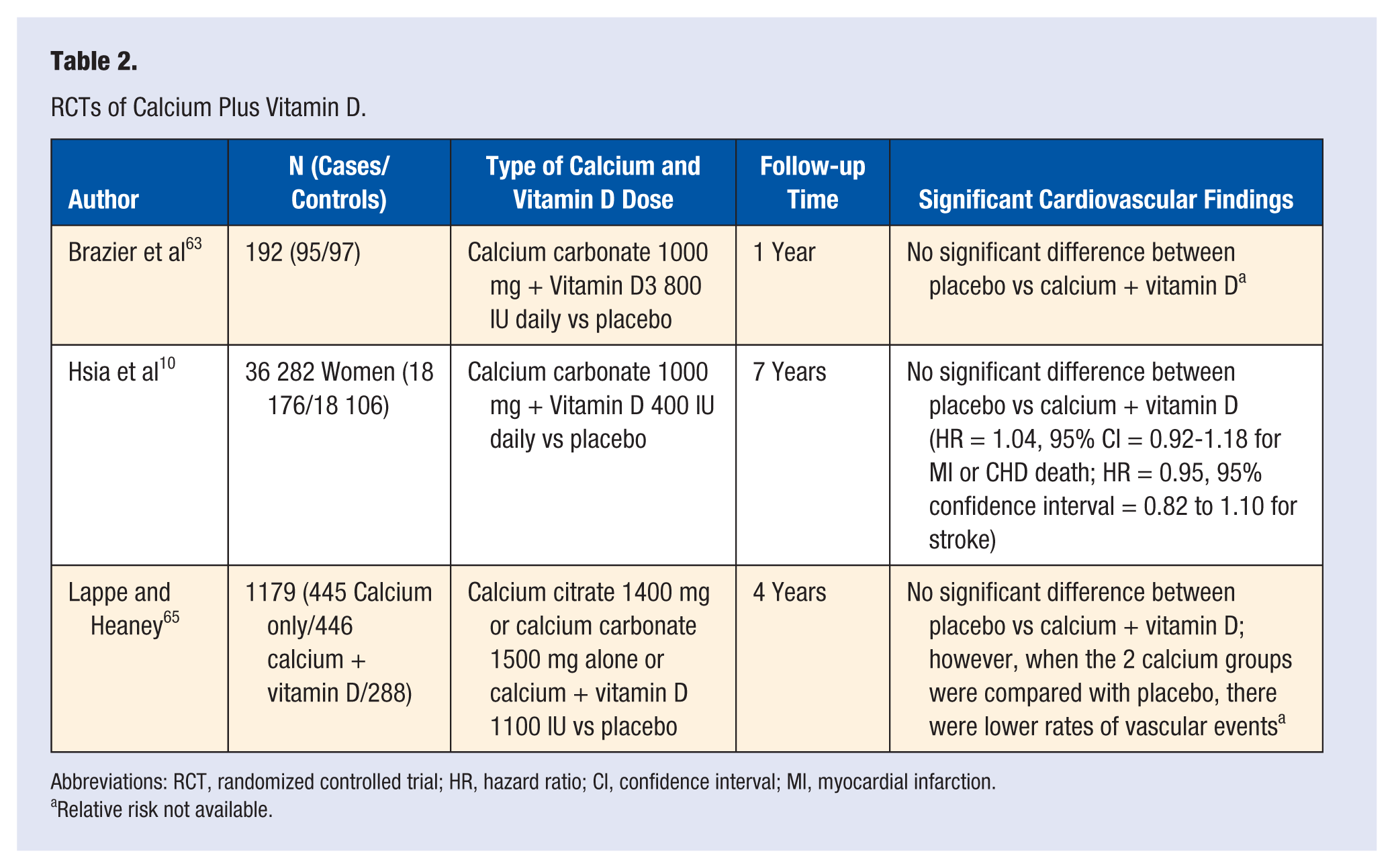
Abbreviations: RCT, randomized controlled trial; HR, hazard ratio; CI, confidence interval; MI, myocardial infarction.
Relative risk not available.
The WHI CaD trial randomized 36 282 postmenopausal women (mean age = 62.4 years) to calcium carbonate 1000 mg with vitamin D 400 IU daily or to placebo. 10 During a 7-year follow-up period, CaD supplementation was not associated with CVD risk (RR = 1.04, 95% CI = 0.92-1.18 for MI or CHD death; RR = 0.95, 95% CI = 0.82-1.10 for stroke). 10 LaCroix et al 64 also evaluated the effects of CaD supplementation on overall mortality in the WHI CaD trial. Supplementation with CaD did not have a statistically significant effect on mortality rates compared with placebo; however, there was a trend toward reduction in risk of death, especially from cancer (RR = 0.89; 95% CI = 0.77-1.03). Among women younger than 70 years, CaD supplementation appeared to reduce risks of total, CVD, and cancer death; however, it is important to note that these finding were not statistically significant. The authors conclude that further testing with higher dose supplements in even larger trials is needed. 64
In a 4-year study on cancer risk (n = 1170, age >55 years), women were randomized to either double placebo, calcium (1400 mg calcium citrate or 1500 mg calcium carbonate) plus vitamin D, or calcium plus vitamin D versus placebo. No increased risk of MI or other vascular events was found in either of the calcium groups compared with placebo. The vascular event rate trended lower in the combined calcium group (4.76/1000 persons/year) compared with the placebo group (6.94 events/1000 persons/year). 65
Meta-analyses: Calcium and Cardiovascular Disease
Results from 2 meta-analyses and a comprehensive review provide reassuring evidence that current available data do not support increased risk of CVD or stroke with calcium supplementation. 66 However, 2 other meta-analyses suggest the opposite.67,68 In 2010, Wang et al 66 evaluated data from 10 prospective studies and 8 RCTs, which reported CVD outcomes of supplemental calcium alone, calcium plus vitamin D, and vitamin D alone. The pooled data demonstrated no apparent effect, either beneficial or harmful, of calcium supplementation with or without vitamin D. Among the RCTs, the pooled RR was 1.14 (95% CI = 0.92-1.41) for supplemental calcium alone; RR = 1.04 (95% CI = 0.92-1.18) for calcium plus vitamin D; and RR = 0.90 (95% CI = 0.77-1.05) for supplemental vitamin D alone. The authors describe the limitations of this study, including limited statistical power because of few eligible studies.
Bolland et al 67 conducted a meta-analysis of 15 RCTs of calcium supplements alone (≥500 mg/d). Criteria for this analysis included trials with duration longer than 1 year, with ≥100 participants and mean age >40 years. Five studies had patient-level data that showed 143 MIs in those taking calcium supplements alone compared with 111 in those taking placebo (RR = 1.31; 95% CI = 1.02-1.67; P = .035). The authors also noted a trend for increased stroke risk (RR = 1.20; 95% CI = 0.96-1.50; P = .11); composite end point of MI, stroke, or sudden death (RR = 1.18; 95% CI = 1.00-1.39; P = .057); and death (RR = 1.09; 95% CI = 0.96-1.23; P = .18), although nonsignificant. On an individual trial level, no study found increased CVD risk; however, pooled trial-level data from 11 of the 15 studies showed 166 MIs in the calcium groups compared with 130 in placebo groups (pooled RR = 1.27; 95% CI = 1.01-1.59; P = .038). Only 2 of the trials adjudicated CVD outcomes, whereas the others relied on self-reported events, hospital admissions, and death certificates, which was a significant study limitation. Furthermore, statistical power was limited in this analysis because many of the trials reported only a small number of CVD events. This study only assessed calcium alone, and so the question remains whether the addition of vitamin D would mitigate any potential risk.
In 2011, Bolland et al 68 reanalyzed their prior meta-analysis by incorporating data from the WHI CaD trial. They evaluated the WHI data with the goal of determining whether concomitant personal calcium allowed during the study had an impact on CVD outcomes. In the WHI CaD trial, 19 564 women (54%) were taking personal calcium at baseline. Women randomized to CaD supplementation or placebo and not taking personal calcium supplements were found to have increased risk for clinical MI or revascularization (RR = 1.16; 95% CI = 1.01-1.34; P = .04) and for clinical MI or stroke (RR = 1.16; 95% CI = 1.00-1.35; P = .05). However, there was no increase in risk for women who were taking personal calcium supplements at baseline (RR = 1.06; 95% CI = 0.92-1.23; P = .40). When data from the WHI CaD participants not taking personal calcium supplements was reassessed with data from the earlier meta-analysis by Bolland et al, it was found that 1384 of 28 072 collective participants had an incident MI or stroke. Calcium supplementation with or without vitamin D increased the risk of MI (RR = 1.24; 95% CI = 1.07-1.45; P = .004) and the combined risk of MI or stroke (RR = 1.15; 95% CI = 1.03-1.27; P = .009). The authors concluded that calcium supplements with or without vitamin D increase the risk of CVD events, especially MI, and that this finding was camouflaged in the WHI CaD study by the use of personal calcium supplements. 68
A recent review of calcium supplementation assessed observational studies and RCTs that reported data on calcium intake and CVD risk. 69 Pooled data from 11 observational studies of dietary calcium did not show an association between dietary calcium intake and risk of CAD or stroke (RR = 0.92, 95% CI = 0.90-1.07, and RR = 0.86, 95% CI = 0.69-1.06, respectively). Combined data from the 5 RCTs was not significant for CAD or stroke (RR = 1.01, 95% CI = 0.78-1.30, and RR = 0.80, 95% CI = 0.63-1.01, respectively). In RCTs looking at CVD outcomes, the combined RR of CVD was 1.14 (95% CI = 0.92-1.41) for calcium supplements versus placebo and 0.99 (95% CI = 0.79-1.22) for calcium plus vitamin D supplements versus placebo. The authors conclude that although current evidence demonstrates that dietary or supplemental calcium has no significant impact on CVD risk, RCTs designed with CVD as a primary outcome are needed to specifically address this dilemma. 69
Finally, Larsson et al 70 conducted a meta-analysis of 11 prospective observational studies to assess the association between dietary calcium and stroke risk. Results found that in those with low dietary calcium intake (<700 mg/d), a 300 mg/d increase in calcium intake was associated with a reduction in stroke risk (RR = 0.82; 95% CI = 0.76-088), whereas a slightly increased risk of stroke was seen in those with high dietary calcium intake (≥700 mg/d; RR = 1.03, 95% CI = 1.01-1.06). Of the 11 studies, 3 also reported data on supplemental calcium intake and stroke, and no association was observed (RR = 0.90; 95% CI = 0.74-1.08). 70
Current Guidelines
An important consideration when evaluating calcium risk is to understand the data on calcium benefit. The 7-year WHI CaD trial showed the CaD group to have a 1.06% improvement in hip bone density (P ≤ .01) but no reduction in hip or total fracture (RR = 0.88, 95% CI = 0.72-1.08, and RR = 0.96, 95% CI = 0.91-1.02, respectively). An elevated risk of kidney stones was also observed in the treated group. The authors suggest that the vitamin D dose of 400 IU daily may have been too low for fracture benefit. 71 A 2007 meta-analysis evaluated 29 RCTs that used calcium supplementation alone or with vitamin D and whose primary outcome was either fracture or bone mineral density. Pooled data from 17 trials showed that calcium was associated with a 12% reduction in fracture (RR = 0.88; 95% CI = 0.83-0.95; P = .0004). Data from 23 trials linked calcium with a 0.54% decrease in hip bone loss (95% CI = 0.35-0.73; P < .0001). The authors note that treatment effect was not significantly different between supplementation with calcium alone or calcium with vitamin D and that treatment was most therapeutic at doses of calcium ≥1200 mg and vitamin D doses of ≥800 IU. 72
The IOM comprehensively reviewed scientific data on calcium intake and concluded that calcium and vitamin D do play a key role in skeletal health. However, there was inconclusive and insufficient evidence regarding extraskeletal impacts on cancer, CVD, diabetes, and autoimmune disorders. For optimal bone health in otherwise normal persons, the IOM recommends the following daily dietary intake: 600 IU vitamin D for men and women 19 to 70 years of age, and 800 IU for men and women >70 years. The recommended daily requirements for calcium are 1000 mg for men 19 to 70 years old and women 19 to 50 years old and 1200 mg for women >51 and men >70 years. 2 The National Osteoporosis Foundation recommends similar dietary calcium intake and emphasizes that calcium supplementation is not required for those who consume adequate dietary calcium. Calcium citrate supplements do not need to be taken with food, other calcium supplements are absorbed best when taken with food. Absorption of calcium is ideal when taken in amounts of ≤500 mg at a time (from diet or supplements). 1
In contrast to the IOM, the United States Preventive Services Task Force (USPSTF) recently concluded that there is insufficient evidence to recommend vitamin D with or without calcium for the primary prevention of fractures in premenopausal women or men. For healthy, community-dwelling postmenopausal women, the task force recommended against supplementation at doses of 1000 mg or less of calcium carbonate and 400 IU or less of vitamin D3 daily because there is no evidence that fracture prevention is achieved with these doses. Additionally, the task force concluded that more research is needed to determine whether higher calcium doses confer fracture protection and to determine the balance of benefits and risk. However, vitamin D supplementation alone was recommended for those >65 years who are at risk for falls. 73
The USPSTF cites data from the WHI that supplementation with CaD resulted in increased incidence of nephrolithiasis. The task force also highlighted research gaps, including the need for comparing the efficacy of different formulations of calcium, and that prospective studies are needed to assess the potential benefits of early calcium and vitamin D supplementation on fracture incidence in later life. The USPSTF did not consider data on calcium alone and highlighted the fact that none of the data used in their review of available evidence reported adverse cardiovascular outcomes. 73
The meta-analysis conducted for the USPSTF recommendations was based largely on the null findings from the WHI CaD Trial because the WHI accounted for 69% of the pooled populations. 74 In a teaching commentary from the North American Menopause Society, it was pointed out that the USPSTF recommendations did not take into account the WHI subanalysis, which showed that in women ≥60 years, a 21% reduction in hip fracture was seen with CaD supplementation. Furthermore, in compliant participants who were not taking personal supplements at baseline, a 30% hip fracture reduction was seen. The authors conclude, “Current recommendations for calcium intake call for 1,000 mg per day for women ages 19-50 and 1,200 mg per day for women over age 50 to ensure bone health. Given recent concerns that calcium supplements may raise risk for CVD and kidney stones, women should aim to meet this recommendation primarily by eating a calcium-rich diet and taking calcium supplements only if needed to reach the RDA goal.” 75
Conclusion
The evidence to date suggests that dietary calcium does not increase CVD risk and may even reduce risk. However, the majority of data regarding the relationship between calcium intake and CVD risk has been extrapolated from observational studies. Results are inherently limited because of design flaws, including the possible presence of confounding factors, recall bias, inability to accurately determine causality, and researcher bias in outcome assessment. Results from the few RCTs are mixed regarding CVD risk in those using supplemental calcium with or without vitamin D, although the majority of studies found no increased risk. This question still remains to be more definitively answered by large-scale, randomized trials designed specifically with CVD as the primary end point. Available evidence suggests that if there is a risk, it is more likely to be attributed to calcium supplementation alone. Larger and longer RCTs are needed to confirm this association, although these trials may be economically challenging to conduct. The utility of calcium supplementation is still being debated, yet evidence suggests that it is reasonable to encourage adequate dietary calcium intake, especially for postmenopausal women who are at greatest risk for osteoporotic fracture.
Footnotes
Acknowledgements
This work was supported by contracts from the National Heart, Lung and Blood Institutes, numbers N01-HV-68161, N01-HV-68162, N01-HV-68163, and N01-HV-68164; grants U0164829, U01 HL649141, U01 HL649241, T32HL69751, and 1R03AG032631 from the National Institute on Aging; GCRC grant MO1-RR00425 from the National Center for Research Resources; CTSI Grant UL1TR000124 and grants from the Gustavus and Louis Pfeiffer Research Foundation, Danville, NJ; The Women’s Guild of Cedars-Sinai Medical Center, Los Angeles, CA; The Ladies Hospital Aid Society of Western Pennsylvania, Pittsburgh, PA; and QMED, Inc, Laurence Harbor, NJ; the Edythe L. Broad Women’s Heart Research Fellowship, Cedars-Sinai Medical Center, Los Angeles, CA; and the Barbra Streisand Women’s Cardiovascular Research and Education Program, Cedars-Sinai Medical Center, Los Angeles, CA.