
Abstract
The population of older adults in the United States is steadily growing and identifying factors that contribute to healthy aging is a public health priority. Changes in body composition are a hallmark of the aging process and have been implicated in the loss of physical function among older adults. In particular, age-related declines in muscle strength and power occur at a faster rate than the loss of muscle mass (sarcopenia), and this suggests a decrease in muscle quality of older adults. Muscle quality has traditionally been defined as muscle function (strength or power) per unit of muscle size (mass or cross-sectional area) and a growing body of literature suggests that lower body muscle quality may be critical for maintaining functional independence with age. However, the literature regarding the definition of muscle quality and its relationship with health outcomes in older adults has not been adequately reviewed. Thus, the aim of this report is to highlight the contemporary literature regarding age-related changes in muscle quality and its relationship with health outcomes in community-dwelling older adults.
‘Muscle quality . . . is emerging as a salient contributor to health and physical function in older adults.’
Introduction
The percentage of adults aged 65 years and older continues to grow and it is estimated that this group will constitute 20% of the adult population in the United States by 2030. 1 This is important as there is a substantial increase in the prevalence of physical limitations with age; adults ≥80 years are ~2.5 times more likely to experience one or more physical limitations (eg, walking ¼ of a mile, climbing 10 steps, reaching overhead) than adults aged 50 to 59 years (43% vs 17%, respectively). 2 Therefore, establishing the role of modifiable factors that contribute to physical function during aging is a major public health priority.
Muscle quality, traditionally defined as muscle force per unit of muscle cross-sectional area,3,4 is emerging as a salient contributor to health and physical function in older adults.5-8 The ability to complete functional activities (rising from a chair, stair ascent), as well as success with other domains of physical function including gait speed and balance, is strongly determined by the major lower extremity muscle groups (quadriceps, hamstrings, and gluteals). Therefore, it is likely that the quality of these muscle groups is critical for maintaining functional independence with age. Despite this, there remains a relative paucity of research delineating the importance of leg muscle quality for health outcomes (eg, functional and metabolic parameters) in older adults. Recently, Barbat-Artigas et al 9 published a review article regarding different measurement techniques for assessing muscle quality in older adults. However, the relationship between leg muscle quality and health outcomes in older adults remains inadequately characterized and may have important clinical implications. Thus, this report seeks to review studies that have examined muscle quality in relation to health outcomes in community-dwelling older men and women. Better characterizing the health implications of muscle quality (eg, its relationship with various functional and metabolic outcomes in older adults) is valuable as it may help inform the development of intervention strategies to facilitate healthy aging.
We identified studies that examined muscle quality and health outcomes in older adults via literature searches on relevant electronic databases through June 2013 using specific search terms, including “muscle quality,” “specific tension,” “specific strength,” “specific torque,” “specific power,” “normalized force,” “physical function,” “health outcomes,” and “older adults.” Our search was not constrained by the type of measurement technique used to define muscle function and muscle size. However, because our review is focused on measurement of leg muscle quality, studies that examined the quality of other muscle groups (eg, plantar flexors, upper extremity) in older adults have been excluded.10 -13 Finally, although muscle quality has been examined in cohorts of young adults, this review is focused on community-dwelling older adults and is therefore limited to studies that involved noninstitutionalized men and women aged ≥50 years.
Changes in Body Composition: Hallmarks of the Aging Process
Several adverse changes in body composition occur during the aging process, and these include a progressive reduction in skeletal muscle mass known as sarcopenia. 14 Sarcopenia, originally proposed by Rosenberg in 1989, 15 has been associated with functional impairment 16 and physical disability,17,18 and has also been identified as a predictor of incident physical limitations among older adults.19,20 However, sarcopenia is accompanied by concomitant declines in muscle function (strength and power), which both occur at a faster rate than the loss of muscle mass. 9
Dynapenia, the age-related loss of muscle strength, 21 is only partially explained by the decline in skeletal muscle mass (sarcopenia). For instance, it was recently shown that cross-sectional area of the quadriceps muscle only accounted for 6% to 8% of the variability in muscle strength among older adults. 4 While a comprehensive review of the physiologic mechanisms underlying dynapenia is beyond the scope of this review, a brief discussion is warranted. It is likely that the complex interplay of neurologic and muscular mechanisms contributes to dynapenia, and these factors have previously been reviewed in detail.22,23 The most prominent mechanisms hypothesized to play a role in dynapenia include a reduction in central activation, decreased motor unit size and number (eg, denervation of type II muscle fibers), as well as alterations in intrinsic force-generating capacity of muscle, dihydropyridine and ryanodine receptors, myocellular lipid infiltration and inflammatory cytokine production. Although additional research is necessary to elucidate the mechanisms most responsible for dynapenia, the above factors are likely instrumental in the more rapid decline in muscle strength relative to muscle size.
It has previously been reported that skeletal muscle mass declines at a rate of 6% per decade after the age of 50 years. 24 In contrast, muscle strength and power decline at rates of 1% to 2% and 3.5% per year, respectively, in older adults, 25 although the reported rate of decline has varied among studies. 26 Notably, both low muscle strength27,28 and power29,30 have been implicated in the development of adverse health outcomes among older adults. Thus, the disproportionate reduction in muscle strength and power relative to mass suggests a decrease in muscle quality and may increase susceptibility to functional limitation and physical disability.
Muscle Quality
Measurement
Several published studies have examined the relationship between leg muscle quality and various health outcomes in community-dwelling older adults (see Table 1). However, because a standardized assessment procedure for muscle quality has not been established, numerous definitions have been suggested and a variety of measurement techniques have been used. To our knowledge, studies that have investigated muscle quality have been conducted in research laboratories and thus used relatively expensive and sophisticated equipment. The most common measurement techniques for assessing leg muscle function include determination of strength via isokinetic dynamometry,3-5,31-39 isometric dynamometry,36,40-45 strain gauge, 46 and assessment of strength or power using the one-repetition maximum technique44,47 -51 or the Nottingham power rig. 6 Lower extremity muscle size has been predominantly measured by estimating skeletal muscle mass via dual-energy X-ray absorptiometry scanning,* although anthropometry 52 , ultrasound scanning 42 , and urinary creatinine excretion37,52 have also been used. In addition, other studies have used computed tomography4,34,36,38,49 and magnetic resonance imaging35,41,43 -45,51 for quantification of muscle cross-sectional area or volume.
Summary of Studies That Have Examined the Relationship Between Muscle Quality (MQ) and Health Outcomes in Older Adults.
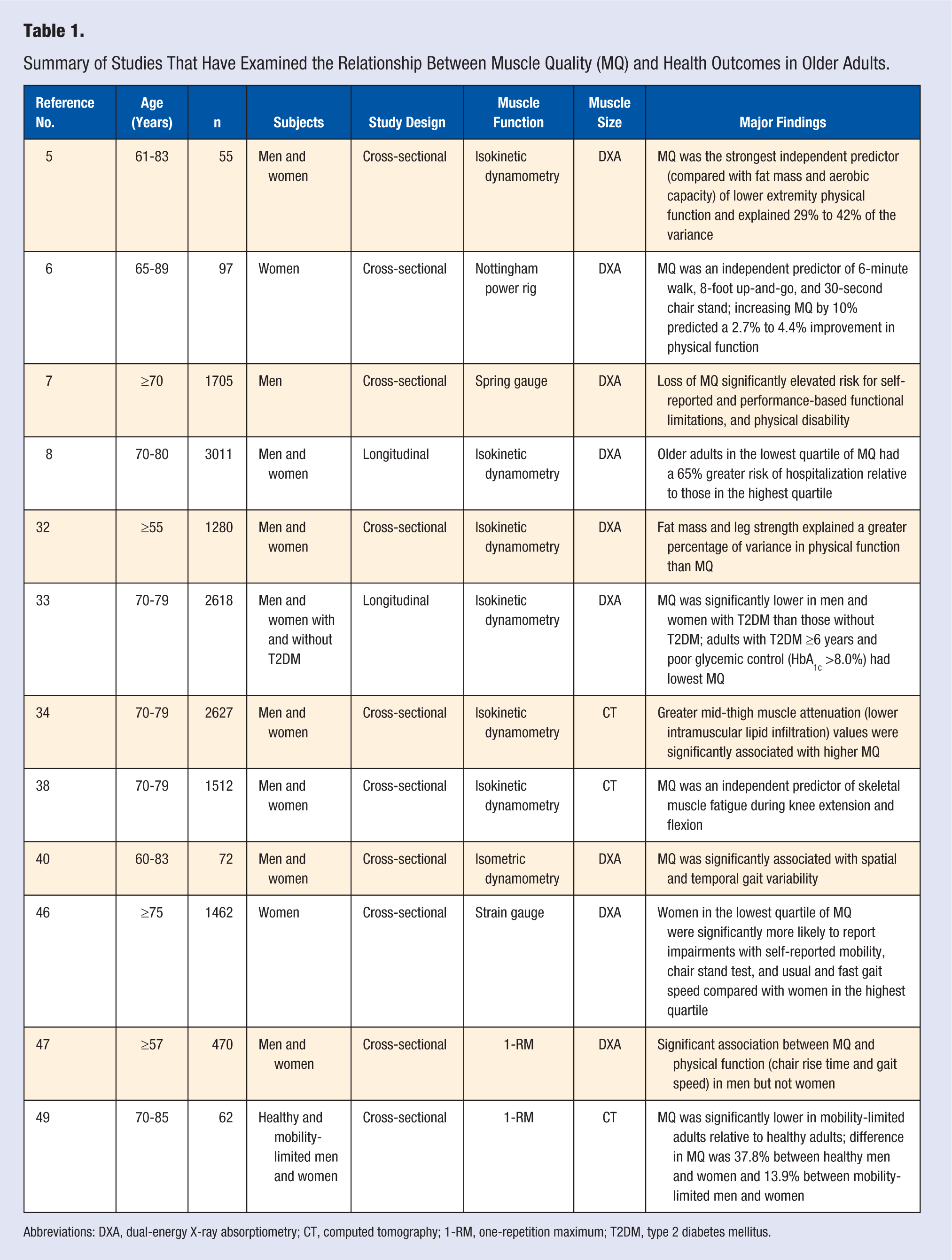
Abbreviations: DXA, dual-energy X-ray absorptiometry; CT, computed tomography; 1-RM, one-repetition maximum; T2DM, type 2 diabetes mellitus.
Age-Related Changes
Both cross-sectional3,35,52 and longitudinal4,31 studies have investigated age-related changes in leg muscle quality among community-dwelling older adults. For instance, Metter et al 52 reported that muscle quality (isometric knee extensor strength/leg lean mass) was 39% and 31% lower in men and women, respectively, from age 20 to 80 years. Importantly, the difference between young and older adults was similar (31% for men and 39% for women) when muscle size was determined using anthropometry to estimate cross-sectional area of the thigh. Likewise, Jubrias et al 35 reported that muscle quality was 21% lower (~1.5% each year) from age 65 to 80 years in a cross-sectional study of older men and women. In a more recent cross-sectional analysis, Newman et al 3 reported that lower extremity muscle quality (isokinetic knee extensor strength/leg lean mass) was 10% lower in men and 11% lower in women across ages 70 to 79 years. Other studies have observed age-related differences in some, but not all, indices of leg muscle quality.36,37 Therefore, there appears to be general agreement among cross-sectional studies that muscle quality is lower in older adults relative to their younger counterparts.
However, only a few longitudinal studies have determined the rate of decline in muscle quality among community-dwelling older adults. Goodpaster et al 31 reported that leg muscle quality declined at a rate of 5.4% to 8.6% over 3 years among older men and women. Likewise, Delmonico et al 4 found that leg muscle quality declined 13.1% and 11.1% over 5 years in older men and women, respectively. Although muscle size was quantified using different measurement instruments (dual-energy X-ray absorptiometry scanning vs computed tomography), both studies provide evidence that the rate of decline in muscle quality exceeds that of sarcopenia (~6% per decade after the age of 50 years). However, both studies were conducted using a sample of well-functioning older men and women from the Health, Aging, and Body Composition Study cohort. In addition, both studies defined muscle quality using the same index of muscle strength (isokinetic dynamometry). It is unknown whether a similar age-related decline in muscle quality would be observed using a different index of muscle function (isometric strength, leg power).
Health Outcomes
As the population of older adults in the United States continues to grow, delineating the most salient contributors to functional and metabolic health is of considerable interest. In the context of this review, the health implications of muscle quality can be understood as its relationship with functional (eg, ability to complete functional tasks, physical disability) and metabolic outcomes (eg, glycemic control, intramuscular lipid infiltration) in community-dwelling older adults.
Physical function, as measured by various performance-based assessments, can predict health outcomes in older adults, including self-reported physical disability 53 and mobility-related disability,54,55 as well as nursing home admission and mortality. 53 Recently, multiple studies have indicated a relationship between muscle quality and physical function in community-dwelling older men and women.5-8,46,47 For instance, Misic et al 5 found that muscle quality was a stronger independent predictor of lower extremity physical function than aerobic fitness and fat mass. In that study, muscle quality explained 29% to 42% of the variance in dynamic physical function whereas the explained variance from aerobic fitness and fat mass was much lower (5% to 6%). Furthermore, we recently demonstrated that muscle quality (leg extension power/lower extremity mineral-free lean mass) was an independent predictor of performance on the 6-minute walk, 8-foot up-and-go, and 30-second chair stand in community-dwelling older women. 6 In contrast, Fragala et al 47 reported a significant association between muscle quality and physical function (chair rise time and gait speed) in men; however, this relationship was not observed in women. Muscle quality has also been implicated in the development of physical disability and risk of hospitalization. For instance, a recent study by Hairi et al 7 found that loss of muscle quality significantly increased risk for self-reported and performance-based functional limitation, as well as physical disability (activities of daily living) in older men. Moreover, Cawthon et al 8 reported that older adults with the lowest muscle quality had a 65% greater risk of hospitalization compared with those with the highest muscle quality.
While the above studies support the contribution of muscle quality to physical function, fewer studies have investigated the relationship between muscle quality and metabolic outcomes in older adults. However, Park et al 33 reported an accelerated loss of leg muscle quality (isokinetic knee extensor strength/leg muscle mass) in older men and women with type 2 diabetes relative to nondiabetic adults. Notably, muscle quality was lowest among older adults who had been diagnosed with type 2 diabetes for ≥6 years and in those adults with elevated glycosylated hemoglobin (HbA1c >8.0%). In a different analysis using the Health ABC cohort, Goodpaster et al 34 reported that the skeletal muscle attenuation coefficient (indicator of intramuscular lipid infiltration) of the mid-thigh was significantly associated with muscle quality. Those adults with a greater muscle attenuation value (lower intramuscular lipid content) had higher muscle quality. Interestingly, Newman et al 3 observed a quadratic relationship between overall body fat and muscle quality, such that muscle quality was lowest at the high and low extremes of body fatness and optimal at percent body fat ranges of 16% to 22% in men and 26% to 34% in women. Other research has shown that muscle quality is significantly lower in obese older adults relative to nonobese men and women. 39 However, additional research is necessary to better characterize the impact of adiposity and weight status (normal weight vs overweight/obese) on muscle quality in older adults.
Exercise Interventions
Regular aerobic and muscle-strengthening activity is recommended by the American College of Sports Medicine for maintenance of health and functional independence of older adults. 56 In addition to a myriad of well-known health benefits, participation in exercise and physical activity can positively affect both components of muscle quality in older adults by altering muscle function (increasing strength/power), muscle size (increasing muscle mass), and reducing intramuscular lipid infiltration.
However, despite mounting evidence that suggests a relationship between muscle quality and health outcomes in older adults, very few intervention studies have included muscle quality as a primary outcome of interest.44,45,48,50,51,57 For example, Tracy et al 44 found that nine weeks of unilateral leg strength training resulted in significant increases in muscle quality of the trained leg in both men (+14%) and women (+16%). Similarly, Brooks et al 48 conducted a 16-week study in older men and women with type 2 diabetes and found a substantial improvement in muscle quality of the exercise group (+28%) whereas a reduction in muscle quality was observed in the control group (−4%). Conversely, Reid et al 50 reported changes in muscle quality (specific power) following an exercise intervention in older adults with mobility limitations (Short Physical Performance Battery score = 7.7). Specifically, muscle quality significantly improved following 12 weeks of high-velocity power training or slow-velocity resistance training compared with a control group.
Muscle lipid infiltration is associated with poor muscle quality 34 ; however, it may also attenuate the magnitude of a training response following exercise. Marcus et al 45 reported that 12 weeks of exercise training significantly improved muscle quality in older adults with low intramuscular adipose tissue, but this was not evident in those with greater levels. Thus, while exercise training appears to be an efficacious intervention strategy for improving leg muscle quality in older adults, its value is based on limited empirical evidence and additional training studies are needed in both healthy and functionally limited older adults to corroborate these findings. In addition, no studies have attempted to determine if a change in muscle quality following a training intervention is associated with a change in physical function. Research should continue to explore the effects of training-induced changes in muscle quality and whether these translate to improved functional abilities in older adults.
Future Directions
Collectively, these findings suggest that muscle quality is an important contributor to health outcomes, including physical function and potentially the risk of metabolic disease, in community-dwelling older adults. Further research will be necessary to ascertain the impact of muscle quality on different metabolic outcomes; however, a small number of published studies do suggest a relationship.
This review also highlights the efficacy of exercise interventions (particularly resistance training) for improving muscle quality. However, these training studies were all conducted in research laboratories. Community-based exercise programs that use a lighter training stimulus, but that have greater translational value, should also be evaluated. We have previously reported the health benefits of community-based resistance training programs for older adults 58 ; however, the impact of such interventions for ameliorating muscle quality should be further explored.
In addition, the potential benefits of weight loss interventions for muscle quality warrant further investigation. Recent studies have shown that weight loss can positively affect the health of obese older adults, such as eliciting improvements in physical function.59 -61 Presently, the effects of weight loss interventions on muscle quality have not been well characterized. It is plausible that weight loss could positively impact muscle quality by reducing mid-thigh muscle lipid infiltration, 62 which is elevated in obesity 63 and is associated with muscle quality in older adults. 34 However, no study has attempted to determine if a change in muscle lipid infiltration following weight loss is associated with improved muscle quality. Furthermore, higher protein consumption (~30% of energy intake) during intentional weight loss can help maintain skeletal muscle mass relative to changes in adiposity, 43 and this may also have a beneficial effect. However, dietary-induced weight loss is typically accompanied by involuntary reductions in lean mass and exercise may help attenuate these changes.64,65 It has recently been shown that resistance training during intentional weight loss can significantly improve muscle power in older women, despite a decline in appendicular lean body mass. 66 While this suggests improved muscle function despite a change in lean mass, additional studies are needed to ascertain the effects of combined exercise and diet interventions on muscle quality in older adults.
Finally, muscle quality has been exclusively determined in laboratory settings, and little research has been devoted to development of a measurement technique feasible for use in clinical settings by practitioners. It is likely that assessment of muscle quality in clinical settings may be limited by a number of factors (access to equipment, assessment time, ease of administration). Determination of muscle function and muscle size using inexpensive field-based methods may provide an opportunity for assessment of muscle quality in community-based and clinical settings. Recently, we reported that a field-based estimate of muscle quality (handgrip strength normalized for body mass index) predicted lower extremity physical function similarly to a more sophisticated laboratory-based approach in community-dwelling older women. 6 However, other field-based techniques exist to measure both muscle function (eg, manual muscle testing) and muscle size (eg, bioelectrical impedance analysis). Future research should attempt to develop a standardized assessment protocol for measurement of muscle quality in clinical settings by practitioners, as this could prove beneficial for predicting physical function in older adults. Finally, establishing sex-specific cut-points for muscle quality (similar to those proposed for the diagnosis of sarcopenia) may have particular clinical utility for demarcating older adults at the greatest risk for development of future physical disability.