
Abstract
Sarcopenia is associated with substantial health and economic consequences and is emerging as a major public health problem in the older population. The effects of sarcopenia may increase the risk for adverse health outcomes in older adults, and strategies need to be developed to maintain healthy aging. Although several intervention strategies have been proposed, resistance training (RT) has been suggested as the most effective stimulus for optimizing improvements in physical function and body composition with age. Although RT has been established as a safe and efficacious intervention for the prevention and treatment of sarcopenia, very few older adults regularly participate in RT programs. Community-based RT programs may be a feasible strategy because of their accessibility, cost-effectiveness, and lower-intensity training stimuli. However, the effects of these interventions on health outcomes in older adults have not been adequately reviewed. This report will describe the health effects associated with sarcopenia and summarize the major findings from community-based RT interventions on different health outcomes in older adults. Finally, it is suggested that all older adults who demonstrate the ability to safely participate in RT comply with the guidelines recommended by the American College of Sports Medicine.
Because the age-related decrease in skeletal muscle mass may lead to declines in physical function, establishing the efficacy of intervention strategies that preserve skeletal muscle mass is critical.
Introduction
The aging process is characterized by a reduction in skeletal muscle mass known as sarcopenia. 1 Sarcopenia is associated with the subsequent development of functional limitations in older adults2-4 and has recently been recognized as a major public health problem. The percentage of older adults who experience sarcopenia-related declines in physical function is likely to increase as a recent estimate suggests that 20% of the US population will be aged 65 years and older by 2030. 5
Although other interventions have been investigated, resistance training (RT) has been suggested as the most effective strategy for delaying and treating the negative consequences associated with sarcopenia in older adults. 6 The American College of Sports Medicine recommends that all older adults participate in regular RT for health promotion and the maintenance of functional independence. 7 Despite the potential positive effects, only 39% of Americans aged 65 years and older accumulate recommended physical activity levels, 8 and only 12% perform RT at least twice per week. 9 Currently, there are few safe and effective RT programs that are available and affordable for older adults. 10 However, RT in community- based settings (eg, senior centers, recreational clubs, and places of worship) may increase accessibility and be a feasible alternative to the programs typically offered in health clubs. Several investigations have reported the effects on physical function and muscle strength following community-based RT in cohorts involving older adults. However, to our knowledge, the impact of such programs for improving health outcomes in older adults has not been reviewed. This report seeks to summarize the effects of RT performed in community-based settings on physical function, muscle strength, body composition, and blood chemistry in older adults.
We identified studies that investigated the effects of RT on health outcomes via literature searches on relevant electronic databases through July 2011 using specific search terms, including community- based, resistance training, resistive training, strength training, weight training, exercise, physical function, older adults, elderly, and muscle strength. Our search was limited to community-based studies that indicated RT was the primary intervention strategy. However, no restrictions were imposed on the type or intensity of training stimulus. In addition, community-based interventions frequently employ quasi-experimental research designs; thus, we chose to include randomized controlled trials and investigations without a true control group. Finally, because this review is focused on community-dwelling older adults, we chose to include only those studies that involved noninstitutionalized adults aged 50 years and older.
Sarcopenia
Sarcopenia is typically accompanied by a consequent reduction in muscle strength, 11 functional impairment, 3 and a heightened risk of physical disability.2,12 The prevalence of sarcopenia is estimated to be ~45% among adults aged 60 years and older, and recent cross- sectional data suggest that the direct health care cost attributable to sarcopenia in the US in 2000 was $18.5 billion. 13 Because sarcopenia is associated with substantial functional and economic consequences, the development and implementation of effective intervention strategies represents an urgent public health priority. After 55 years of age, a large percentage of older adults report difficulty walking 0.4 km or carrying 11 kg. 14 Moreover, 57% of men and 70% of women are physically unable to perform heavy housework after 80 years of age. 14 Furthermore, it has been reported that low thigh muscle cross-sectional area increased the risk of major disability (eg, inability to perform activities of daily living [ADLs], walk one quarter of a mile, or climb 10 steps) by 40% in the Health, Aging, and Body Composition study cohort, 4 and epidemiological data indicate that sarcopenia is associated with a 3- to 4-fold increased risk of physical disability. 2 In addition, functional impairment has been commonly identified as a predictor of incident falls in older adults,15,16 and the health consequences associated with falling are considerable.17-19
Because the age-related decrease in skeletal muscle mass may lead to declines in physical function, establishing the efficacy of intervention strategies that preserve skeletal muscle mass is critical. Pharmacological interventions, such as hormone replacement therapy, have demonstrated inconsistent findings and have been associated with an increased risk for adverse clinical outcomes in older adults. 20 Because the safety of some pharmacological approaches is questionable, RT has been suggested as the safest and most effective stimulus for the maintenance of skeletal muscle mass and eliciting improvements in physical function. 20 Although the beneficial effects of regular RT in older adults are well-established, less is known regarding the effectiveness of community-based interventions that use lower-intensity training protocols. Community-based RT programs may be an adequate public health strategy for curtailing the negative effects associated with sarcopenia in older adults.
Community-Based RT Interventions
Several investigations have shown that RT is an efficacious modality for increasing muscle strength and improving physical function in older adults.21-25 However, these studies have typically been conducted in laboratory- and gymnasium-based research settings and used resistance exercise machines. Fewer studies have examined the efficacy of community-based programs that use a lighter training stimulus (eg, resistance tubing, ankle cuff weights, and elastic bands) for improving muscle strength and physical function in the elderly population. Because sarcopenia is associated with devastating health consequences,2-4,12 it is paramount that exercise programs attenuate reductions in skeletal muscle mass and facilitate meaningful improvements in functional abilities. Recently, several published studies have investigated the effects of community-based RT on physical function and muscle strength in older cohorts (see Table 1).
Summary of Community-Based Resistance Training (RT) Studies and Effects on Health Outcomes in Older Adults
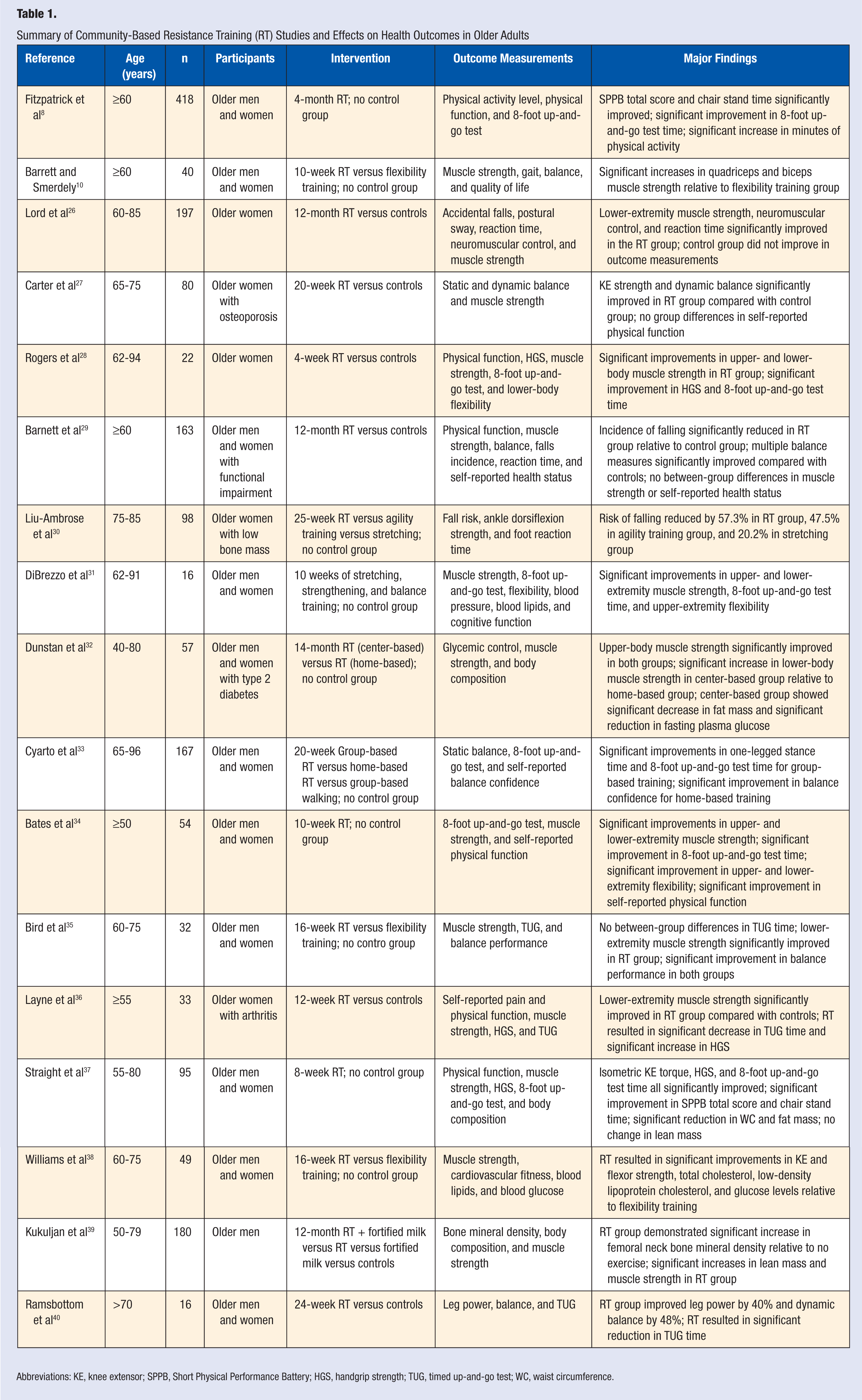
Abbreviations: KE, knee extensor; SPPB, Short Physical Performance Battery; HGS, handgrip strength; TUG, timed up-and-go test; WC, waist circumference.
One community-based study combined RT with dietary modifications 37 and another encouraged increased consumption of fruits and vegetables but did not measure compliance with dietary recommendations. 28 In addition, it should be noted that some community-based RT interventions involve familiarization sessions or interventions delivered in local fitness centers, and these studies have been included in this report. The duration of all interventions ranged from 4 weeks to 14 months, and all reported the effects of RT on some objective or self-reported measure indicative of physical function.
Physical Function
Although a universal definition for what constitutes physical function has not been established, numerous measurement techniques have been developed and used to assess functional abilities. Performance on functional assessments has been shown to provide a valid prediction of institutionalization, risk of falling, mortality, 41 difficulty performing ADLs, 42 and mobility-related disability. 43 It has been estimated that 20% to 30% of community-dwelling adults >70 years report mobility-related disability and difficulty completing ADLs such as bathing, dressing, and eating. 44 Because sarcopenia increases susceptibility to functional limitations 11 and physical disability,2,12 preserving muscle strength (a determinant of function) and functional abilities may reduce the incidence of adverse health events in older adults.
Findings from the studies summarized in Table 1 suggest that community-based RT does confer significant functional benefits. In particular, the effects of community-based RT interventions on muscle strength are overwhelmingly positive. The majority of studies reported significant improvements in lower-extremity muscle strength,10,26-28,31,32,34-37,38,39 and only 1 study reported no between-group differences in muscle strength with training. 29 For example, Layne and colleagues 36 conducted a 12-week randomized controlled trial in older women with arthritis and found that the increase in lower-extremity muscle strength was significantly greater in the RT group (32.3%) relative to the control group (7.3%). Likewise, a 2002 study by Carter et al 27 found that RT resulted in a 12.8% greater increase in isometric knee extensor strength compared with a control group in a cohort of older women with osteoporosis. Furthermore, Straight et al 37 observed a 12.6% within-group improvement in isometric knee extensor torque following RT. In addition to lower-extremity muscle strength, a few studies have reported significant improvements in handgrip strength,28,36,37 and reduced handgrip strength has been identified as a predictor of incident disability (eg, difficulty with ADLs and mobility) in older adults. 45
Physical disability is characterized by difficulty performing ADLs and functional tasks; thus, several studies have investigated the effects of community-based RT on selected measures of self-reported and performance-based physical function.8,27-29,33-37,40 Bates et al 34 found that a 10-week RT program in various community-based settings resulted in significant improvements in SF-36 physical functioning domain scores. Furthermore, Straight and colleagues 37 reported that gait speed (as measured by the 8-foot up-and-go test) and ability to rise from a seated position both significantly improved following a combined RT and dietary intervention at 4 Rhode Island senior centers. In general, multiple intervention trials have demonstrated a significant reduction in the duration required by participants to perform either the 8-foot up-and-go test or the timed up-and-go test after a training program,8,28,31,33,34,36,37,40 both of which have been previously shown to predict the risk of adverse health outcomes in older adults.46,47
The health consequences attributable to falling are substantial, and a few studies have examined the effects of community-based RT interventions on the risk of falling and reported beneficial effects.29,30 For example, Barnett et al 29 found that the incidence of self-reported falls during a 12-month randomized controlled trial was 40% lower in the RT group relative to the control group. Similarly, Liu-Ambrose and colleagues 30 conducted a 25-week study in older women with low bone mass and found a substantial reduction in the risk of falling in older adults who performed RT (57.3%), whereas a much smaller decrease was observed in the stretching group (20.2%). Furthermore, other studies have reported that community-based RT resulted in significant improvements in balance measures10,27,33,35,40 and self-reported balance confidence, 33 which may positively impact risk of falling in older adults.
Additional Health Outcomes
In addition to the positive effects on physical function and muscle strength, a few studies have observed improvements in other health parameters, including metabolic function and body composition. For example, Dunstan et al 32 reported that community-based RT was associated with a modest improvement in glycemic control in older adults with type 2 diabetes. In regard to body composition, they reported a significant decrease in waist circumference and fat mass and the attenuation of lean mass following the 14-month community-based program. Comparably, Straight et al 37 found a significant reduction in waist circumference and fat mass; however, no significant within-group differences in lean mass were observed. In another report using the same cohort, Cottell et al 48 reported that community-based RT and dietary modifications resulted in a significant reduction in biochemical values, including triacylglycerol concentrations as well as systolic and diastolic blood pressure. No significant improvements were noted in any other measures of lipoprotein metabolism or blood glucose regulation. Conversely, Williams et al 38 found that a 16-week RT intervention resulted in significant improvements in total cholesterol, low-density lipoprotein cholesterol, and glucose concentrations relative to a flexibility training group.
Conclusion
Collectively, the major findings from these studies suggest that community-based RT interventions may be an effective strategy for improving various health outcomes in older adults. This review indicates that RT performed in community- based settings has a beneficial effect on muscle strength and physical function in older adults. However, future research is necessary to ascertain the more specific effects on metabolic parameters and body composition. Despite the need for more published data on health outcomes such as markers of metabolic health and body composition, community-based RT holds promise as an intervention strategy for precluding potential sarcopenia-related health declines in the elderly population. Because community-based interventions may be a more accessible and cost-effective alternative to RT programs typically available in health clubs, they may increase the percentage of older adults who perform regular RT and have positive health and economic implications. Recently, a retrospective analysis indicated that older adults who attended a community-based exercise program ≥1 session per week had an ~20% fewer annual health care expenditure than those reported by controls. 49 Thus, the successful implementation of evidence-based RT interventions in community settings may be a feasible public health strategy for conferring meaningful health benefits and achieving current RT recommendations from the American College of Sports Medicine. Finally, it is strongly suggested that older adults participating in community-based programs obtain medical clearance and adhere to accepted RT guidelines in order to minimize the potential for adverse health events.