
Abstract
This review summarizes the extant evidence of the effects of exercise training on anxiety among healthy adults, adults with a chronic illness, and individuals diagnosed with an anxiety disorder. A brief discussion of selected proposed mechanisms that may underlie relations of exercise and anxiety is also provided. The weight of the available empirical evidence indicates that exercise training reduces symptoms of anxiety among healthy adults, chronically ill patients, and patients with panic disorder. Preliminary data suggest that exercise training can serve as an alternative therapy for patients with social anxiety disorder, generalized anxiety disorder, and obsessive–compulsive disorder. Anxiety reductions appear to be comparable to empirically supported treatments for panic and generalized anxiety disorders. Large trials aimed at more precisely determining the magnitude and generalizability of exercise training effects appear to be warranted for panic and generalized anxiety disorders. Future well-designed randomized controlled trials should (a) examine the therapeutic effects of exercise training among understudied anxiety disorders, including specific phobias, social anxiety disorder and posttraumatic stress disorder; (b) focus on understudied exercise modalities, including resistance exercise training and programs that combine exercise with cognitive-behavioral therapies; and (c) elucidate putative mechanisms of the anxiolytic effects of exercise training.
‘Psychologists and psychiatrists diagnose anxiety disorders using well-defined criteria and information obtained in response to standardized questions presented during interviews.’
Following initial background information, this review provides a summary of the empirical evidence of the effects of exercise training on anxiety symptoms and disorders. The article finishes with a brief summary of suggested plausible mechanisms of the anxiolytic effects of exercise training.
Anxiety
Anxiety refers to unpleasant feelings of apprehension and thoughts of worry that are often combined with activation of the autonomic nervous system. It can be an adaptive response to an objective or perceived threat but it also can be maladaptive if the anxiety becomes severe and chronic. 1 Cognitive 2 and neurobiological models 3 have been offered to explain the development and expression of anxiety and anxiety disorders. Models that integrate these 2 approaches 4 ultimately may prove to be the most useful.
It is useful to distinguish between state and trait dimensions of anxiety. 5 State anxiety refers to transient feelings of tension and worry that can vary in intensity from moment-to-moment. Commonly used words to describe the presence or absence of these feelings (also known as symptoms) including tension, worry, nervous, jittery, calmness, and relaxation. A large body of experimental evidence demonstrates that anxiety symptoms are transiently reduced by approximately ¼ to ½ standard deviation in response to an acute bout of exercise.6-9 The magnitude of improvement in state anxiety after a single bout of exercise appears largest for individuals experiencing high anxiety, but even those with below average anxiety often report feeling fewer anxiety symptoms after acute exercise. 10
Trait anxiety refers to an individual’s predisposition and/or proneness to appraise an event or stimulus as threatening. Trait anxiety has a biological basis and is both relatively stable over time and sensitive to change in response to targeted interventions.11,12 Interventions designed to reduce trait anxiety symptoms, including cognitive and behavioral therapies,13,14 chronic massage, 15 and relaxation training, 16 produce moderate-to-large reductions in trait anxiety scores.
Anxiety Disorders
Anxiety disorders are a group of debilitating conditions characterized by excessive, chronic maladaptive anxiety symptoms that are often accompanied by strong autonomic nervous system activation, altered anxiety-related cognitions, and altered behavior (eg, avoidance). Psychologists and psychiatrists diagnose anxiety disorders using well-defined criteria and information obtained in response to standardized questions presented during interviews.
Pathological anxiety currently is classified into 6 disorders: specific phobia, social anxiety disorder (SAD), generalized anxiety disorder (GAD), panic disorder (with or without agoraphobia), obsessive–compulsive disorder (OCD), and posttraumatic stress disorder (PTSD). The widely used criteria for diagnosing these anxiety disorders, based on the current Diagnostic and Statistical Manual, 17 were revised in May 2013. The criteria for several of the disorders remained essentially the same, but OCD and PTSD were put into categories separate from the anxiety disorders, and 3 new anxiety disorders were added (substance-induced anxiety disorder, anxiety disorder attributable to another medical condition, and separation anxiety disorder).
Anxiety disorders are the most prevalent type of mental health disorder, affecting approximately 40 million Americans annually, 18 with an estimated annual cost in excess of $44 billion due to direct costs of treating anxiety and a variety of indirect costs such as reduced work productivity.19,20 The lifetime prevalence of any anxiety disorder is higher among women (~31%) compared with men (19%). 21 Limited evidence has suggested higher prevalence rates of anxiety disorders among non-Hispanic whites compared to other race/ethnicity groups,22,23 while people aged 15 to 24 years experience episodes of anxiety 40% more often than people aged 25 to 54 years. 24
Anxiety disorders are also associated with significant personal impairment as evidenced by strong and independent associations with reduced health-related quality of life, 25 increased disability,26-28 increased absenteeism from work, 29 and increased use of health care resources.30,31 Individuals with an anxiety disorder also report significantly more medically unexplained physical symptoms compared to individuals without an anxiety disorder. 32
There are effective drug and cognitive-behavioral treatments for anxiety disorders,33,34 but more than 40% of patients report no current treatment. 26 Some are disinterested in treatment, others have difficulty adhering to treatment, and others have inadequate insurance or other barriers that result in no or suboptimal treatment. 35 Notable drawbacks of pharmacotherapy include well-established negative side effects such as nausea and sexual dysfunction. 36 Because anxiety disorders are heterogeneous, pharmacotherapy may attenuate some symptoms but exacerbate others. Selective serotonin reuptake inhibitors have shown efficacy for anxiety symptom improvement37,38 but often amplify sleep disturbances39,40 and weight gain. 41 Behavioral treatments have also demonstrated efficacy,42,43 but there are logistical barriers associated with those treatments including the expense and the need for extensive specialized training among practitioners. Widespread access to cognitive-behavioral therapy is currently unavailable and would require pervasive policy changes. 44 Thus, there is a need for effective, accessible, low-cost remedies for anxiety disorders, and regular physical activity may have a role to play in helping lower anxiety among people who suffer from anxiety disorders.
Epidemiology of Physical Activity and Anxiety
Bidirectional relationships between physical activity and anxiety are plausible. Elevated symptoms of anxiety or the fear of anxiety-related sensations 45 may reduce not only physical activity levels but also the desire to exercise, 46 or being physically active may reduce anxiety symptoms. A limited amount of population-based evidence from nationally representative cross-sectional and prospective cohort studies supports that regular physical activity protects against anxiety disorders and anxiety symptoms. The odds of reductions in anxiety symptoms associated with being physically active on average range from 30% to 55% compared to those reporting little or no physical activity.47,48 These observations are supported by recently published cross-sectional data obtained from large Norwegian (N = 38 743), 49 British (N = 9309), 50 and US 51 community samples showing anxiety symptoms are inversely related to physical activity level. Data also have emerged from a study of 1793 US adults over age 45 with physician-diagnosed arthritis. 52 The findings showed that the prevalence of elevated anxiety symptoms was lower (26%) among those patients who reported exercising 150 or more minutes per week compared to those who reported being physically inactive (43%).
Some of the available cross-sectional results, such as those from a nationally representative sample of 8098 U.S. adults aged 15 to 54 (see Figure 1), suggest that physical activity protects against the most prevalent anxiety disorders in a dose-dependent fashion. 47
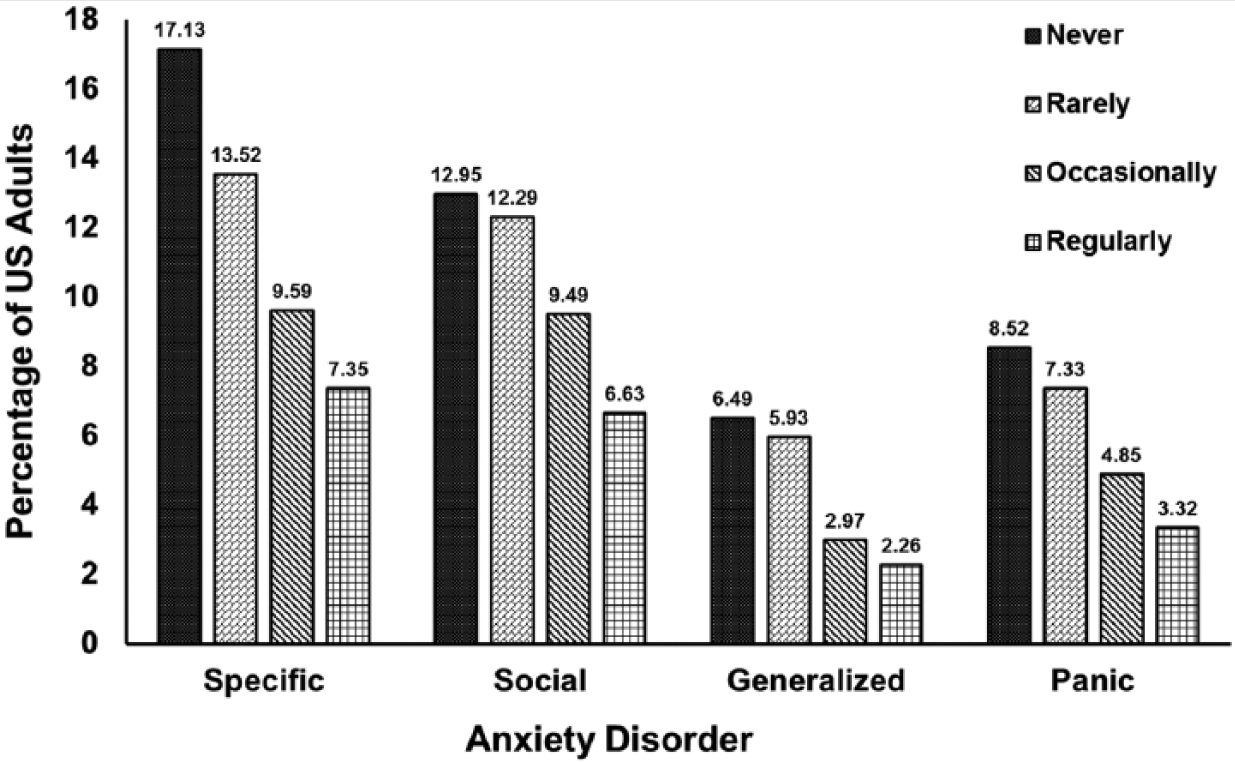
Percentage of Adults With Specific Phobia, Social Anxiety Disorder, Generalized Anxiety Disorder, and Panic Disorder in Relation to Physical Activity Level.
Not all epidemiological evidence suggests a dose–response relationship, however.53-55 Additional evidence is also needed concerning the role of potential moderator variables (eg, age, sex, race/ethnicity, and physical activity characteristics). One prominent population-based study of mono- and di-zygotic twins concluded that the association between physical inactivity and greater anxiety symptoms was noncausal and the result of common genetic factors affecting both anxiety symptoms and physical activity. 56 A key limitation of this investigation is that it focused on leisure-time exercise, a metric that excluded the more commonly performed lifestyle physical activities. Even if it is ultimately shown that there is no causal relationship between physical activity and anxiety in the general population, it would not necessarily mean that exercise training is unable to cause improvements in symptoms of anxiety for some people. 57
Effects of Exercise Training by Healthy Adults on Anxiety
Table 1 provides a summary of published systematic or quantitative reviews of exercise effects on anxiety. Since 1990, there have been 6 quantitative reviews that have summarized the effects of exercise training on anxiety where most or all of the data were based on findings from healthy adults.8,58-62 In the earliest review, 408 effect sizes were calculated from data obtained from 104 studies. The effects of exercise training on state and trait anxiety outcomes were reported separately. 8 On average, after chronic exercise both state anxiety (effect size = 0.25, based on 83 effects) and trait anxiety (effect size = 0.34, based on 62 effects) were reduced significantly. The length of exercise training was significantly related to the overall mean effect size such that programs of greater than 9 weeks elicited significantly larger anxiety reductions. Notably, only 13 of 104 (12.5%) studies were randomized controlled trials (RCTs).
Summary of Systematic or Quantitative Reviews of Exercise Effects on Anxiety.
In another early meta-analytic review, the authors derived 33 effect sizes, 13 for state anxiety and 20 for trait anxiety, from 22 investigations of the effect of regular physical activity on anxiety among individuals without a medical diagnosis. 60 An overall mean effect size of −0.04 was reported; however, the moderator analyses indicated that regular physical activity could reduce anxiety when the outcome measure was trait anxiety.
A subsequent meta-analysis examined 20 studies (22 effects) of physical activity and anxiety found nonsignificant mean effect sizes for investigations of the effect of acute exercise and exercise training on anxiety. 61 This analysis had a smaller number of effects included, and the meta-analytic techniques used both to calculate and to aggregate effect sizes were unclear.
As a partial replication of the meta-analytic review completed by Petruzzello and colleagues, 8 Long and van Stavel 59 conducted a meta-analysis with an expanded, updated study sample. Seventy-six effects were derived from 40 studies using either a within-subjects or a between-subjects design to examine the effects of exercise training on anxiety symptoms in adults without a medical or psychiatric condition. 59 Overall mean effects of 0.45 and 0.36 were found for 26 effects derived from within-subjects designs and 50 effects derived from between-subjects designs, respectively. 59 A number of methodological limitations attenuate the meaningfulness of these findings, especially the lack of randomization in most of the studies (n = 25/40).
More recently, a meta-analysis in this category focused on 49 investigations, 40 of which were RCTs of exercise training effects on anxiety symptoms. 62 The results showed an overall weighted effect size of 0.48 (95% confidence interval [CI] = 0.33-0.63). Moderator analyses showed significantly larger effect sizes for participants 31 to 45 years of age compared to participants aged 45 years or older and for an exercise frequency of 3 to 4 times per week compared to 1 to 2 times or more than 5 times per week. 62 It should be noted, however, that the contrast results for exercise frequency likely achieved significance because 32 of the 40 effect sizes included in the moderator analysis were in the 3 to 4 times per week category. Limitations of this investigation include that the aggregated mean effect size was calculated across effects derived from investigations with within- and between-subjects designs. This is contraindicated because effect sizes calculated from within-subjects designs use the standard deviation of the change score, whereas the pooled baseline standard deviation is used in a between-subjects design. Moreover, the transient and persistent effects of exercise were confounded by including effect sizes derived from both acute and chronic exercise studies.
The most recent meta-analysis in this category focused on healthy adults and had several other exclusion criteria not used in other meta-analyses (eg, studies that measured anxiety immediately after exercise were excluded); thus, only 13 studies were analyzed. The overall mean reduction in anxiety was 0.22, and the effect was higher (0.53) among those studies that involved random assignment to the exercise or comparison condition. 58
At least 5 RCTs have investigated the effects of strength training on anxiety symptoms in healthy adults and 4 of 5 trials were conducted with older adults.69-73 Based on these experiments, we estimated the magnitude of the effect of resistance exercise training on reducing anxiety as 0.54, and not enough information is available to determine if age moderates this effect. 74
A systematic review of 8 studies has been carried out examining the influence of yoga on anxiety. Although the methodological quality of the studies was inadequate to conclude that the regular performance of yoga reduces anxiety, the authors did note that yoga appeared to be a promising treatment for reducing anxiety. 64
In summary, the weight of the available evidence summarized here and elsewhere indicates that even healthy adults who are free of stressful physical or mental illnesses (eg, an anxiety disorder) report fewer or less intense feelings of anxiety after both strength and aerobic-type exercise training.
Patients With a Chronic Illness
Although anxiety symptoms and disorders, which are strongly and independently associated with reduced health-related quality of life and disability,25-27 are more common among individuals with a chronic illness,75-79 anxiety symptoms often remain undetected and/or untreated. It is plausible that exercise training could be especially beneficial for individuals at increased risk for experiencing anxiety symptoms because they must cope with health-related threats of a chronic illness.
Kugler and colleagues 63 conducted a meta-analytic review of 13 studies, 4 lacking a control group, which examined the effect of rehabilitation exercise programs on anxiety among patients with coronary heart disease. A mean anxiety reduction of 0.31 standard deviation units was found, suggesting that exercise training is effective for the attenuation of anxiety in persons undergoing cardiac rehabilitation. However, because the review did not focus on RCTs that compared exercise training to a control condition, whether exercise is the key element for rehabilitation-related improvements in anxiety is uncertain. Failure to focus on RCTs is also true of a more recent meta-analytic review of exercise training effects on cardiovascular patients. 80 Recent small randomized trials with cardiovascular patients have shown positive effects. For example, 12 weeks of strength training significantly reduced anxiety among ischemic stroke patients. 81 Cardiac rehabilitation experts believe that the available evidence shows that exercise training reduces psychological stress and that this reduces the risk of mortality among cardiovascular disease patients. 82
One meta-analysis has focused on RCTs of exercise training effects on anxiety outcomes among patients with a variety of medical illnesses. 65 Seventy-five effects were derived from 40 RCTs of exercise training effects on patients with a chronic illness. Figure 2 depicts mean effect sizes across illness types, including 21 studies of patients with cardiovascular disease, 15 studies of patients with fibromyalgia, 10 studies of patients with multiple sclerosis, 9 studies of patients with psychological disorders, 8 studies of patients with cancer, 4 studies of patients with chronic pain, and 4 studies of patients with other medical illness (eg, obesity, lupus, and epilepsy). Random effects models, which allow the simultaneous estimation of variance attributed to both sampling error and random population variance, were used to aggregate overall mean effect size delta (Δ) and to examine whether the effect varied according to selected moderator variables. Delta represents the cumulative mean effect size aggregated across all effect sizes derived from each study included in the meta-analysis. Exercise training significantly reduced anxiety symptoms among patients by a mean effect size delta of 0.29 (95% CI = 0.23-0.36). Meta-regression analysis, which simultaneously considers multiple effect modifiers and their interactions while controlling other extraneous factors that can confound comparisons between effects derived from all studies, indicated that the mean effect size significantly varied according to exercise program length, session duration, and the time frame of anxiety report. Exercise programs of no more than 12 weeks (Δ = 0.39; 95% CI = 0.28-0.49), using exercise sessions of at least 30 minutes (Δ = 0.36; 95% CI = 0.27-0.44), and an anxiety report time frame greater than the past week resulted in the largest anxiety improvements (Δ = 0.44; 95% CI = 0.29-0.59). 65
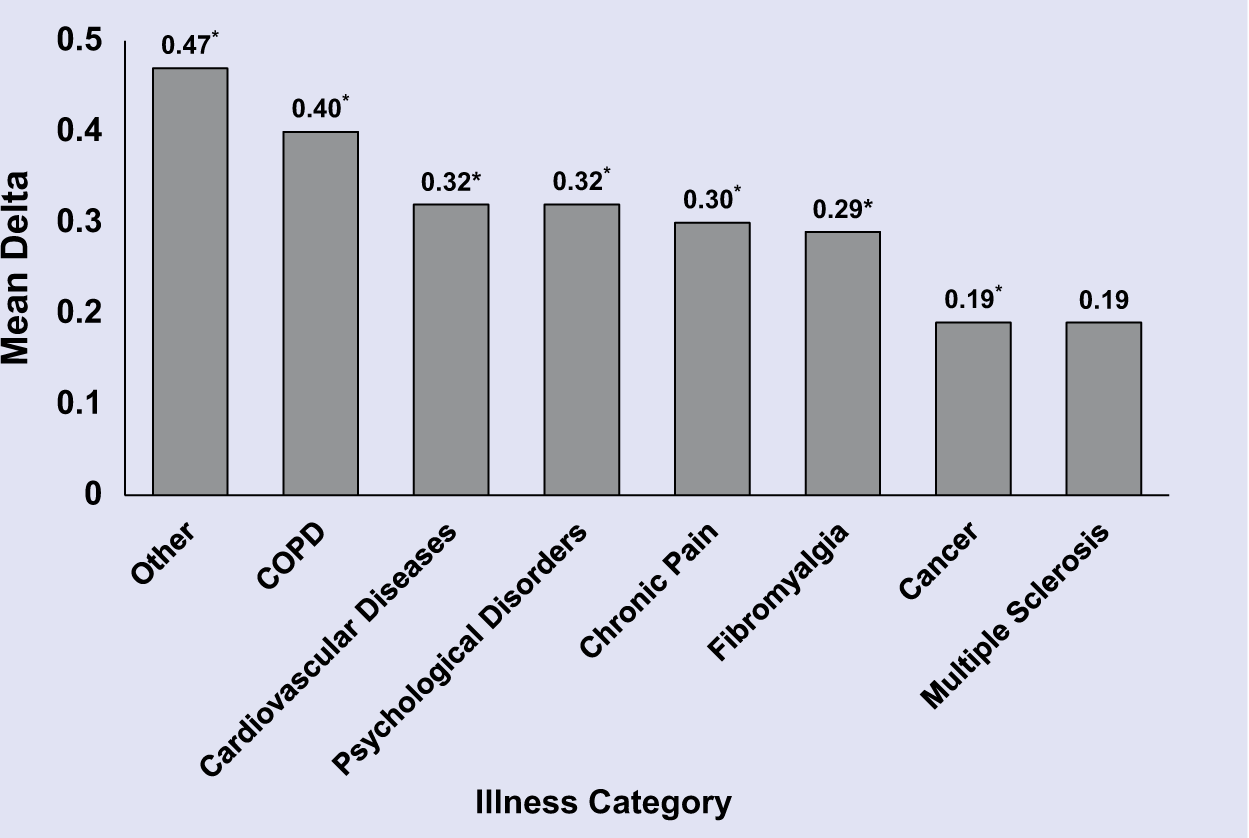
Aggregated Effect of Exercise (Mean Delta) on Anxiety Symptoms Across Illness Types.
Why shorter exercise programs and longer exercise sessions resulted in larger anxiety improvements among the trials included in the meta-analysis was uncertain. Although included data did not permit a rigorous test of the potential moderating effect of adherence, the available evidence suggested that adherence may play a critical role in the moderating effects found for program length and session duration. Mean adherence rates for shorter length programs were significantly larger than programs of a greater length, while adherence rates for trials using session durations of less than 30 minutes were nonsignificantly worse than rates for trials using session durations greater than 30 minutes. 65 Adherence may be tightly linked to exercise-induced symptom improvements because the ability to accurately quantify the efficacy of an intervention decreases as intervention attrition increases. Thus, one limitation of the reviewed trials was that approximately one third of the effects were derived from trials that provided no information about adherence. 65
It also was uncertain why approximately 80% of investigations used an anxiety report time frame of 1 week or less, but it may have resulted from the misconception that trait anxiety scores are insensitive to change in response to interventions of only a few months. However, trait anxiety scores, which are based on a time frame longer than 1 week, are sensitive to change in response to short-term interventions including cognitive and behavioral therapies, long-term massage, and relaxation training.13,15,16,64
The meta-analytic findings discussed above underscore the need for well-designed trials into the effects of exercise on anxiety among patients with understudied illnesses, including those with chronic obstructive pulmonary disease, cancer, chronic pain, autoimmune and inflammatory disorders, and especially patients with an anxiety disorder. Small trials with renal transplant patients and intellectually disabled individuals do show that exercise training appears to reduce anxiety symptoms in these understudied groups.83,84 A recent trial with men and women undergoing chemotherapy showed nonsignificant improvements in anxiety after a multimodal intervention that included high intensity cardiorespiratory (85% to 95% of maximal heart rate) and resistance training (85% to 95% of 1 repetition maximum). 85
Exercise Effects Among Patients With Anxiety Disorders
There has been less available evidence regarding the effects of exercise training among individuals diagnosed with an anxiety disorder. Two recent reviews concluded that the limited available evidence suggests that exercise training may be an effective adjuvant or adjunct therapy for clinically significant anxiety.66,67 A recent meta-analysis of 7 RCTs of aerobic exercise effects on patients with a DSM-IV defined anxiety disorder concluded that aerobic exercise training is not an effective treatment for anxiety disorders when time spent exercising was accounted for by the control condition. 68 Following a summary of the evidence from early studies of mixed samples of anxiety disorder patients, the available evidence of exercise effects for each anxiety disorder is presented in sections ordered by prevalence.
Early Studies
In one early study, 44 inpatients with a DSM-III anxiety disorder completed aerobic exercise, usually walking or jogging, for 1 hour, 5 sessions per week for 8 weeks. 86 All patients exhibited improvements except those diagnosed with social phobia. Patients with GAD and agoraphobia without panic attacks maintained improvements at a 1-year follow-up. 86 However, a key limitation of this study was the lack of a control comparison.
A second early study examined the effects of aerobic and nonaerobic exercise among 79 inpatients with various DSM-III-R anxiety disorders. 87 Patients were randomly assigned to aerobic or nonaerobic exercise of 1 hour, 3 sessions per week for 8 weeks. Patients in both exercise groups showed similar and significant reductions in anxiety independent of changes in aerobic capacity, 87 suggesting that increases in aerobic fitness are not necessary to elicit reductions in anxiety. Limitations included the absence of a control group and concomitantly administered treatments.
In a third early study, walking was compared to jogging in 52 inpatients over an 8-week exercise training protocol and at a 6-month follow-up. The authors reported persistent anxiety reductions 6 months after 8 weeks of aerobic exercise training. Psychological improvements were not significantly different between jogging and walking. 88 However, lack of a control group prevents the ability to draw a meaningful conclusion about exercise training effects on anxiety.
Specific Phobias
Although epidemiological studies suggest that physically active people are at reduced risk for specific phobias,47,48 there appears to be no published RCTs or others studies that have examined the influence of exercise training on specific phobias.
SAD Patients
There is a small body of information about the influence of chronic exercise on SAD. The information is difficult to interpret due to lack of a control group,86,89 low numbers of SAD patients,87,90 and the inability to isolate exercise effects.91,92 The most recent evidence stems from a study of unmedicated patients (n = 56) with SAD who were randomly assigned to an 8-week intervention that involved either aerobic exercise or mindfulness-based stress reduction (MBSR). Exercise participants were provided a gym membership and asked to complete at least 2 individual and 1 group exercise session each week. The MBSR group completed a 2.5 hour group class once per week, a 1-day retreat and daily practice. The improvements in social anxiety symptoms immediately (effect size range of 0.51 to 0.70) and 4 months (effect size range of 0.49 to 0.54) after the exercise intervention were as large as those found for MBSR. 89 Brain imaging data were obtained in response to a self-referential encoding task and tasks involving attention to autobiographical negative social anxiety-related memories. Exercise and MBSR training were associated with equivalent reductions in self-reported emotional reactivity in response to the negative social anxiety-related memories and both groups had similar patterns of change in brain responses measured with functional magnetic resonance imaging (fMRI). 93 Exercise and MBSR training also were associated with similar reductions in self-endorsement of negative social traits and increases in positive social traits but the brain neural fMRI responses to these activities after exercise training differed from those found for MBSR. 94 The effects of exercise training per se cannot be determined from these findings because of the absence of a control group that did not receive treatment.
GAD Patients
One small RCT has examined the effects of 6 weeks of either resistance exercise training (RET) or aerobic exercise training (AET) on GAD remission and associated signs and symptoms. 95
Thirty sedentary women, aged 18 to 37 years, diagnosed by clinicians blinded to treatment allocation with a primary DSM-IV diagnosis of GAD and not engaged in treatment other than stabilized pharmacotherapy, were randomly allocated to RET, AET, or wait list (WL). RET involved 2 weekly sessions of lower-body weightlifting that began at 50% of 1-repetition maximum at week 1 and progressed by 5% weekly. AET involved 2 weekly sessions of cycling matched with RET on body region exercised, positive work completed during each session, time actively engaged in exercise, and load progression.
The high adherence (100%) and compliance to the prescribed exercise dose (>99%) and the absence of adverse events indicated that exercise training was well-tolerated. Remission rates were 60%, 40%, and 30% following RET, AET, and WL, respectively (Figure 3). The number needed to treat of 3 for RET suggests that, on average, for every 10 GAD patients who perform 6 weeks of RET 3 additional remissions would be expected compared to untreated patients. Much more data are needed to confirm the magnitude and consistency of these findings.
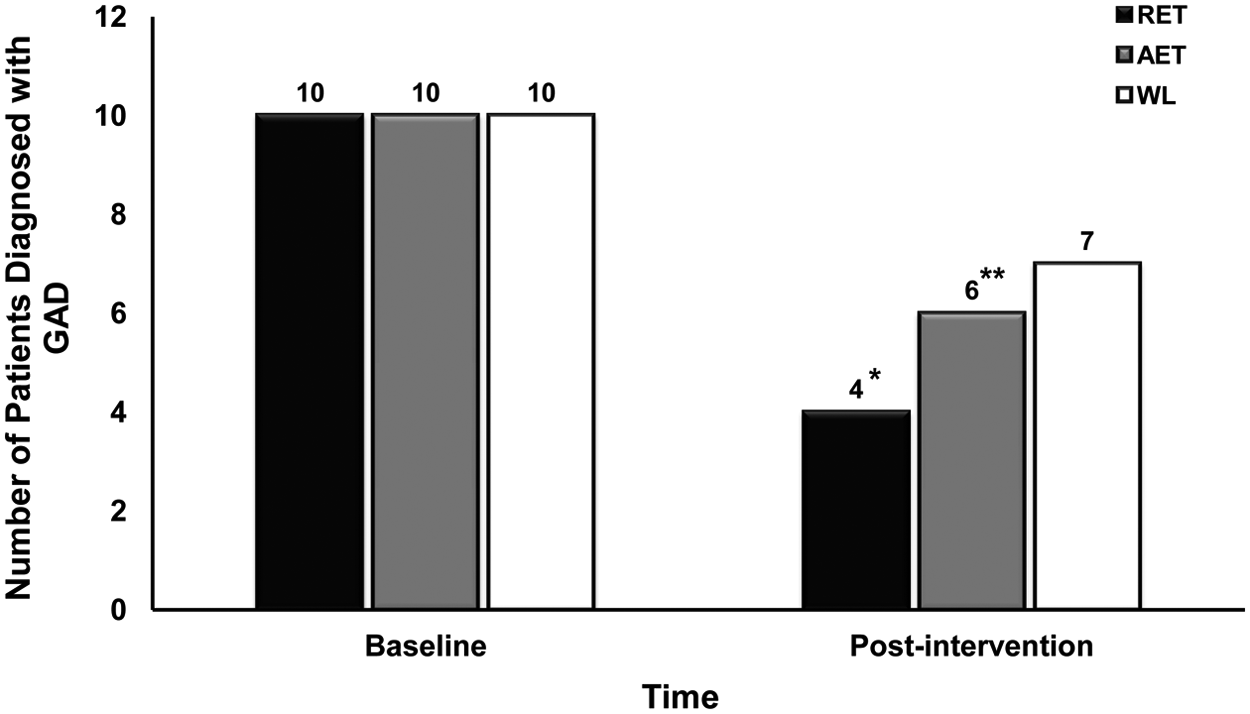
Remission Among Women With Generalized Anxiety Disorder at Baseline and Following a 6-Week Exercise Intervention.
Compared to WL, exercise training significantly reduced worry symptoms and resulted in moderate-sized improvements (Hedges’ d ≥ 0.40) in trait anxiety and concentration as well as other symptoms that co-occur with GAD including depression, fatigue and vigor, physical and mental dimensions of quality of life, and pain intensity. Although differences between AET and RET were not hypothesized because exercise conditions were matched on multiple features of the exercise stimulus, RET resulted in significant remission and larger magnitude effects for 9 secondary outcomes.95,96 One factor that may have contributed to the better outcomes for RET is that the AET sessions were perceived as significantly less intense (RPE = 9; “very light”) than the RET sessions (RPE = 14; “somewhat hard” and “hard”).
Overall, findings were of comparable magnitude to the effects of other empirically supported treatments for GAD including pharmacotherapy, relaxation therapy, cognitive therapy, and CBT.37,38,97,98
Obsessive-Compulsive Disorder Patients
Two quasi-experimental studies have examined the effect of exercise training on OCD symptoms. A 6-week exercise intervention was associated with reductions in Yale-Brown Obsessive Compulsive Scale symptoms from the severe to moderate range among 11 OCD patients. 99 A 12-week pilot trial similarly examined the effect of the addition of aerobic exercise training to regular care on OCD symptoms among 15 patients diagnosed with OCD who had received pharmacotherapy or CBT treatment for at least 3 months. 100 Patients completed moderate-intensity aerobic exercise training for 20 to 40 minutes, 3 to 4 sessions per week for 12 weeks. OCD symptom severity was significantly reduced (effect size = 1.69), and clinically meaningful reductions were demonstrated for 69% and 50% of patients at posttreatment and at a 6-month follow-up, respectively. 100 Although this preliminary study lacked a true control condition, the results do suggest both the potential efficacy of exercise training and the need for well-designed RCTs.
One small randomized trial has examined the effects of yoga on OCD. 101 Twelve patients practiced a version of kundalini yoga and were compared to 10 patients assigned to mindfulness meditation. At 3 months, the yoga group improved more than the meditation group on the Yale-Brown Obsessive Compulsive Scale (34.8% reduction vs 13.9%). A limitation of yoga studies is that both the absolute and relative (to maximum capacity) dose of exercise is uncertain. Thus, while we can learn whether yoga does or does not influence anxiety, it is not possible to fully document dose–response effects.
Building on prior research, Abrantes and colleagues 102 recently published the design and rationale for an NIH-funded RCT testing the efficacy of a 12-week moderate-intensity aerobic exercise intervention on OCD severity, nonspecific anxiety, depression, quality of life, fitness, and cognition among 102 OCD patients currently engaged in pharmacotherapy and/or CBT. The authors postulate that exercise may provide a valuable treatment augmentation for patients with OCD, particularly among those with residual symptoms. 102
PTSD Patients
Although there are several rationales for why exercise may be especially helpful for PTSD, including positive effects of exercise on associated symptoms of PTSD (eg, depression, 103 insomnia, 104 cognitive dysfunction, 105 and fatigue 106 ), there have been no published RCTs of exercise effects on PTSD. Three studies without control groups by Motta and colleagues 107 have reported reduced PTSD symptom severity, as well as anxiety and depression, following modest exercise training interventions.108-110 For example, 26 patients with PTSD attributable to a wide range of traumas performed a 10-week program of aerobic exercise for 30 minutes at 60% to 80% HRmax for 2 to 3 days/week. Nine participants who met a liberal adherence criterion of 12 exercise bouts during the 10-week period showed significant improvements in PTSD symptom severity, depression, and anxiety, and these improvements persisted at 1-month follow-up. 99 A second study assessed 15 adolescent females with PTSD living in a residential treatment facility. 109 Eleven participants met the adherence criterion, averaging 22 bouts of 20 minutes of aerobic exercise across an 8-week intervention. Findings showed improved PTSD severity, which persisted at 1-month postintervention. 109 A third study showed improved PTSD symptom severity, anxiety, and depression among 12 institutionalized female adolescents with PTSD in response to 3 sessions per week of 25 minutes of aerobic exercise at 60% to 90% HRmax for 5 weeks. 110 These studies, conducted primarily with children and adolescents, are limited by small, heterogeneous samples, lack of a control condition, and/or low adherence rates. Nonetheless, this preliminary evidence suggests that exercise may be an effective treatment for PTSD and associated symptoms.
Panic Disorder Patients
Broocks and colleagues conducted the first randomized, placebo-controlled investigation of the efficacy of 10 weeks of aerobic exercise training in the treatment of panic disorder. 111 Forty-six outpatients diagnosed with moderate to severe panic disorder with or without agoraphobia (DSM-III-R) were randomly assigned to either 10 weeks of walking/running a 4-mile route 3 to 4 times per week, clomipramine (112.5 mg/day), or placebo. Both exercise and medication resulted in significant decreases in anxiety symptoms compared to the placebo condition, suggesting that exercise training may be as effective as pharmacotherapy. Outpatients who completed the exercise program reported large reductions in anxiety (effect size = 1.10) compared to those who took daily placebo pills. The clomipramine treatment group had lower attrition and resulted in earlier reductions in anxiety symptoms. 111 Because of the strong research design, this experiment provided strong evidence that exercise training can attenuate symptoms among anxiety disorder patients. A follow-up study with 75 panic disorder patients compared the effects of 10 weeks of (a) exercise + 40 mg/day of paroxetine, 112 (b) exercise + placebo, (c) relaxation + placebo, or (d) relaxation + paroxetine. 113 Improvements in clinician- and self-derived anxiety symptoms were large and similar for all the groups. Thus, adding an antidepressant did not augment the anxiety improvements associated with regular exercise and exercise training was similar to relaxation in relieving anxiety.
The therapeutic effects of 12 weeks of aerobic exercise training for panic disorder patients also has been compared to CBT. 114 Patients were randomized to 12 weeks of group exercise 3 times per week (n = 17) or cognitive-behavioral group therapy (CBT; n = 19) once per week. Both treatments improved symptoms of anxiety significantly. CBT provided greater relief than exercise immediately after treatment and at 6- and 12-month follow-ups. Clearly, larger trials aimed at determining the generalizability of the positive effects of exercise training for panic disorder patients is warranted.
Studies of Mixed Samples of SAD, GAD, and Panic Disorder Patients
The effect of adding a moderate intensity home-based exercise program to 8 to 10 weeks of group CBT was examined in an RCT of 74 patients who had SAD, GAD, or panic disorder. 91 The authors reported that the addition of 30-minute bouts of moderate intensity walking exercise up to a goal of 150 minutes per week to CBT resulted in large reductions (effect size = 1.36) in anxiety for the group as a whole compared to the CBT control condition. 91
Physical Activity Could Reduce Anxiety via Multiple Mechanisms
There are multiple mechanisms by which exercise training could reduce anxiety. Detailed presentations of these possibilities have been presented by others elsewhere.3,115-123 Here, we provide a brief sketch of only the more prominent psychological and neurobiological mechanisms that have been suggested to underlie the anxiolytic effects of exercise training.
Self-Concept/Self-Esteem
Self-concept refers to how people perceive various characteristics of themselves (eg, “I am good at games and sports”), whereas self-esteem refers to how people feel about themselves (eg, “Physically I am happy with myself”). Because increases in physical activity have been associated with increased physical self-esteem in randomized trials 124 and impaired self-esteem has been associated with elevated symptoms of anxiety, 125 it is possible that exercise training could improve anxiety through increases in physical self-esteem or self-concept. One correlational study of 1036 young women showed that physical activity had inverse, indirect associations with symptoms of social phobia, GAD, and OCD that were expressed through positive association with specific and global physical self-concept and self-esteem (M. P. Herring, P. J. O’Connor, and R. K. Dishman, 2013, unpublished data). These correlational findings suggest that physical activity might reduce the risks of anxiety disorders among young women by positive influences on physical self-concept and self-esteem.
Exposure
Exposure therapy is a major component of CBT for anxiety disorders. Anxiety symptoms can be produced during exercise; consequently, exercise can be used to expose people to anxiety symptoms in a controlled, safe environment. Exercise may relieve anxiety by teaching persistence in the presence of negative somatic symptoms that individuals had learned to avoid.126,127 The addition of neutral or positive social interactions with exercise-induced anxiety symptoms also may allow individuals to “unlearn” links between their anxiety symptoms and conditioned stimuli that contribute to social or other phobias. 126 A body of rodent research, showing that physical inactivity reduces multiple aspects of learning, provides a plausible neurobiological basis for using exercise to assist in learning that anxiety symptoms can occur in the absence of threatening stimuli.
Expectation/Placebo Effect
Exercise training may help people feel less anxious because individuals expect that it will result in that outcome. There is evidence that expectations are associated with improvements in mental health after exercise training.128-130 Research on this hypothesis has been hampered by the difficulty in creating an adequate placebo condition for exercise training.
Adaptations in the γ-Aminobutyric Acid (GABA) Neurotransmitter System
The most commonly prescribed anti-anxiety drugs enhance the effects of GABA. A limited amount of evidence supports the idea that exercise-training-induced adaptations in GABA could result in reductions in anxiety. Chronic activity-wheel running in rats can increase levels of GABA, decrease the number of GABAA receptors in the corpus striatum, and increase open-field locomotion. 131 These findings are consistent with an anxiolytic effect according to the limbic-motor integration model of locomotor behavior proposed by Mogenson and Yang. 132
Adaptations in the Norepinephrine Neurotransmitter System
Norepinephrine is thought to play a complex role in anxiety, and it can both increase and decrease anxiety. Norepinephrine is a modulatory neurotransmitter that usually is coreleased with the inhibitory peptide/trophic factor galanin. A substantial body of research on rodents suggests that regular physical activity both enhances galanin and inhibits norepinephrine activity,133-135 and this is linked to reductions in anxiety-like behavior in rodents 122 and could plausibly contribute to reductions in anxiety after exercise training.
Adaptations in the Serotonin Neurotransmitter System
Excessive central nervous system release of serotonin (5-hydroxytryptamine, 5-HT) is anxiogenic. Regular physical activity has effects on the brain that include (a) reductions in 5-HT levels in the central amygdala, 112 (b) reductions in messenger RNA for the 5-HT1a transporter, and (c) increases in the number of 5-HT1a autoreceptors, which inhibit the release of 5-HT.120,133 Such adaptations in the serotonin system are associated with greater social exploratory behavior in rodents; thus, the animals exhibit less anxiety-like behavior when they are regularly physically active. 136
Summary
The available evidence from RCTs indicates that exercise training can improve anxiety symptoms among healthy adults, patients with a chronic illness, and patients with panic disorder and GAD. The effects of exercise training appear to be comparable to other empirically supported treatments for panic and generalized anxiety. Well-designed pilot RCTs examining the therapeutic effects of exercise training are needed among understudied anxiety disorders, including specific phobias, SAD, and PTSD. Large trials aimed at determining the magnitude and generalizability of the effect appear to be warranted for panic and GADs. Future well-designed RCTs are also needed that focus on understudied exercise modalities, including resistance exercise training, and the elucidation of putative mechanisms of the anxiolytic effects of exercise training.