
Abstract
Obesity and climate change are 2 modern world dilemmas. However, despite an understanding of many of the causal factors relating to each, large-scale interventions have had minimal impact on either problem to date. Some behaviors associated with obesity (eg, processed food consumption, nonrenewable fuel use, etc) also affect greenhouse gas (GHG) emissions associated with climate change. This suggests that interventions aimed at curbing GHGs might also have public health benefits. Personal carbon trading is an emission reduction intervention that has been proposed to influence obesity-related behaviors. This article builds on the links between obesity and climate change and discusses some of the early findings of the Norfolk Island Carbon and Health Evaluation study designed to assess the impact of personal carbon trading on obesity and GHG emissions. Early results suggest that health and environmental scientists should be working more closely to develop cross-disciplinary initiatives and messages around health and environmental issues.
‘. . . the environmental impacts associated with increased adiposity, and obesity-related behaviors have started to emerge.’
Background
Worldwide, obesity rates have more than doubled since 1980. 1 With greenhouse gas (GHG) emissions trending in the same direction globally, 2 we are faced with 2 modern world dilemmas: obesity and environmental pollution, specifically linked with climate change. Although both health and environmental scientists continue to look for solutions for their respective problems—an increase in deaths from noncommunicable diseases by 30% in the past 20 years 3 and CO2 levels rapidly reaching a point of irreversible damage 4 —some researchers are now looking for a cross-disciplinary solution for dealing with both. 5
The implications of climate change for public health have long been recognized. Most of the early literature concerned the impacts of increasing severe weather events, 6 shifts in disease vectors to lower latitudes, 7 and expansion of tropical diseases. 8 More recently, the environmental impacts associated with increased adiposity and obesity-related behaviors have started to emerge.9,10 Physical activity replaced by carbon emitting, fossil fuel–powered transport, and sedentary-based leisure activities along with consumption of high-energy-dense processed foods traditionally associated with an increased risk of obesity are now being recognized in the context of their environmental impact.11,12
The consumption of food, for example, has long been shown to have impacts on human health. As food becomes increasingly processed there is an increase in energy density 13 and an associated risk of obesity and chronic disease. 14 The impacts of food on the environment have also been established where, in comparison with highly processed Westernized diets, more traditional plant-based diets are associated with lower GHG emissions. 15
A similar relationship exists between these diets and their impact on body weight, with lower rates of obesity demonstrated with plant-based diets. 16 In theory at least, a positive shift toward a healthy (more plant-based) diet should not only reduce body weight but also contribute to reducing an individual’s carbon footprint and hence, environmental impact.
Dietary interventions have the potential to reduce GHG emissions and improve health. The same can be said about physical activity in the form of active transport. Population-based interventions aimed at reducing CO2 emissions associated with passive, rather than active transport, could help reduce the 1.9 million annual global deaths from physical inactivity. Other public health benefits include reducing the 800 000 annual global deaths from outdoor air pollution and the 1.2 million annual deaths from traffic accidents. 17
Given that obesity-related health behaviors have demonstrated environmental impacts, obesity itself presents a climate change challenge. Compared with a “normal” distribution (~3% obese) an overweight population with 40% obesity (more consistent with the modern-day UK population) has a 19% increase in total energy expenditure associated with adiposity. As shown in a unique study carried out at the London School of Hygiene, if 1 billion people were to be represented by the overweight distribution this equates to between 0.4 and 1.0 gigatons of CO2 equivalents each year. 18
Changing Behavior to Improve Our Health and the Environment
As it stands, the impacts of obesity and obesity-related behaviors on rising GHG emissions are becoming increasingly clear. History has demonstrated, however, that public health campaigns designed to address these behaviors at the population level have largely been unsuccessful. 19 Previous interventions have predominantly focused on education and social responsibility where key public health massages around a healthy diet and regular exercise unfortunately have not translated into common practice. 16 It may be time to rethink our approach.
While knowledge might be necessary, it is not always sufficient to influence behavior. Despite knowing the health benefits of physical activity and a healthy diet, less than half of adults in Western advanced countries like the United States, the United Kingdom, and Australia do sufficient exercise to achieve a health benefit, and <15% consume the recommended daily amount of fruit and vegetables.20-22 Scale these types of behaviors up to a global level and this helps explain why 65% of the world’s population are living in countries where the mortality rates associated with being overweight or obese exceed those associated with being underweight or malnourished. 1
This has largely come about not through lack of education or guidance from governing bodies who have been following these trends for some time, 23 but from rapid changes to the macro- and microenvironments through economic development, which overwhelms these health messages.5,24 Despite global efforts emphasizing the importance of regular exercise, 25 advances in technology have largely removed the need to perform physical activity, which was once ingrained in activities of daily living. Easily accessible and affordable energy-dense foods also mean that healthy food options like fruit and vegetables are often replaced with tastier, cheaper, and more convenient processed alternatives, or those embellished with unhealthy nutrients (fat, sugar, salt) as part of their “value added” process for sale. 26
Despite the best efforts of public health experts, the “obesogenic” environment continues to hold the balance of power in the war against obesity. 27 Greater attention to diagnosing and modifying obesogenic environments is required if public health initiatives are going to successfully reverse these trends.5,10,28 Counteracting this knowledge, however, is the fact that obesity is still often seen as a “personal” problem. This is partly through its adverse effect on only certain individuals 29 and partly through political expediency. GHG emissions and environmental degradation on the other hand, have the potential to disastrously affect everyone.
The Big(ger) Picture
Reducing global GHG emissions, like reducing obesity, is no easy task. One thing that appears to be gathering momentum, however, is the amount of stakeholder engagement and level of commitment around the globe. The “Six America’s Study” carried out since 2008 by the Yale Project on Climate Change and Communication 30 shows a significant turnaround in concern about climate change since 2010. Such commitment forces governments to act and although action has been insufficient to date, changes in technology and incentives aimed at replacing carbon-intensive infrastructure are beginning to emerge.
One well-recognized incentive for reducing emissions is carbon trading. 31 To date, most of the attention has focused on Corporate Carbon Trading or a Carbon Tax, to provide “upstream” reductions in emissions. As an economic incentive, industries responsible for the largest GHG emissions are encouraged to change their current ways of working to a “greener” more environmentally sustainable alternative.
While upstream interventions are beginning (albeit with some problems associated with carbon pricing) around the globe, 32 and while these may have some impact on obesity-related behaviors, around 40% to 50% of GHG emissions come from individuals and households. 33 This has led to proposals for a more “downstream” system such as Personal Carbon Trading (PCT), 34 which might engage individuals more in both reducing emissions and, almost incidentally, reducing obesity through a change in obesity-related behaviors.
Personal Carbon Trading, unlike a carbon tax, is designed to entice individuals to have more responsibility for their own carbon-related (and by stealth, health-related) behavior. Under this system, a national carbon emissions target is set at a declining level for each year, which is then divided equitably within the population. All adults are given a personal carbon allowance with the same number of carbon units. When buying carbon intensive products such as fuel, electricity (and possibly food), units come off that person’s carbon allocation. As an incentive, those left with carbon units at the end of a set period can trade these into the marketplace for financial rewards. As a disincentive, those that exceed their allowance are then required to purchase more. 11
One advantage of allocating personal carbon allowances is that it introduces an element of mental accountability and responsibility, which otherwise would only be recognized through price signals. 35 This is best highlighted in Figure 1, which compares downstream methods such as personal carbon allowances to the more upstream carbon tax. 35
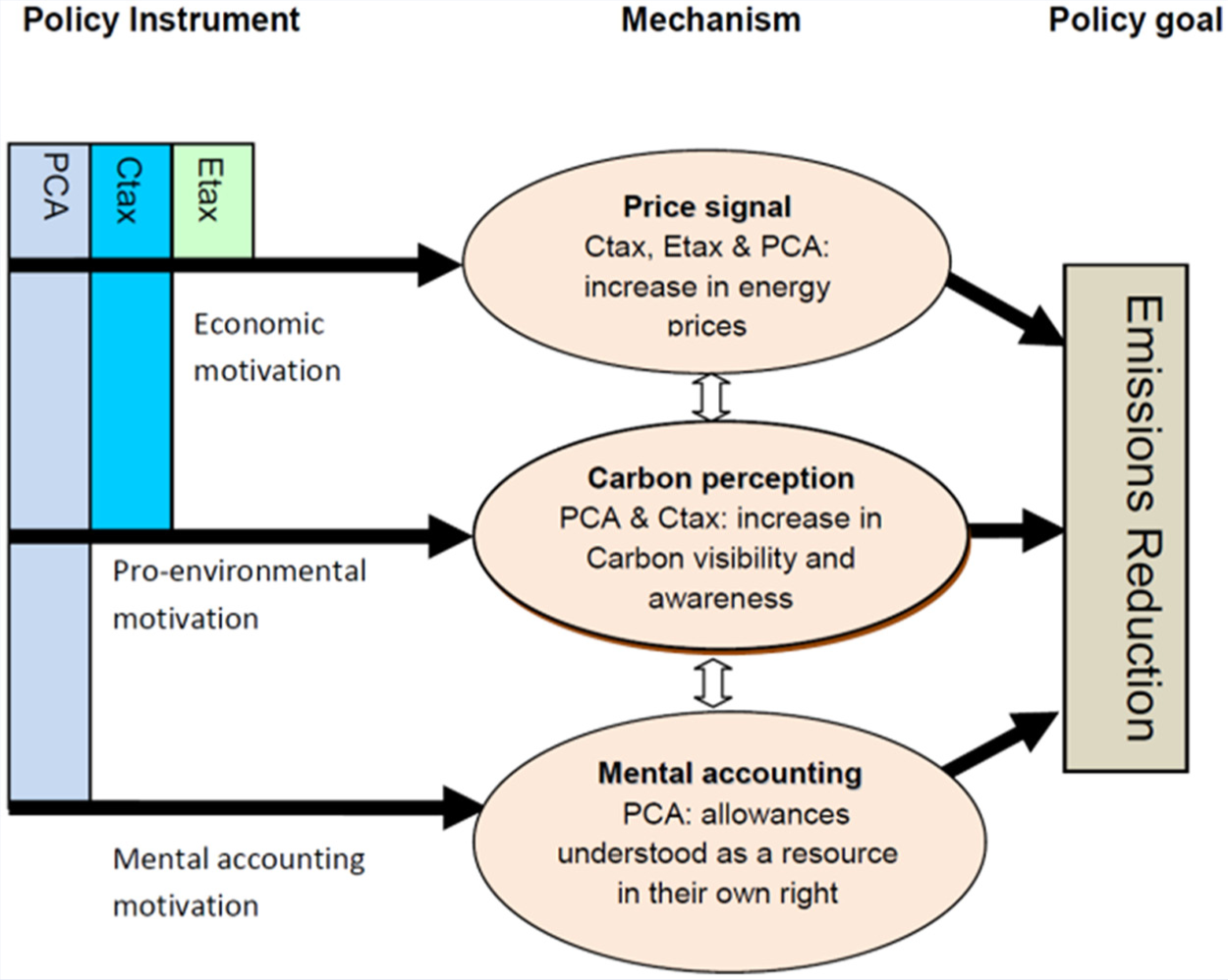
Motivations for energy-related behaviour provided by an energy tax (Etax), carbon tax (Ctax), and personal carbon allowancces (PCA). 35
Given the aforementioned links between GHG emissions and health, PCT has also been suggested as an environmental strategy to improve population health, in particular obesity, through the adoption of improved health behaviors (ie, diet and active transport) associated with a low carbon lifestyle. 10
In essence, PCT is an emissions reduction strategy that has the potential to positively influence obesity-related behaviors. Through the introduction of policy and financial incentives, a strategy designed to reduce GHG emissions has the potential to double as a (macro) environmental strategy to improve health behaviors and reduce obesity. The theoretical basis of such an approach was first proposed some time ago. 10 However, difficulties in testing such an approach in a large population and the political acceptability of such a trial to date have prevented this from happening.
The Norfolk Island Carbon and Health Evaluation Project
Norfolk Island is a self-governing Australian protectorate, currently inhabited by around 1600 permanent residents. It is a relatively small volcanic island (5 × 8 km2), situated 1500 km from the east coast of Australia and approximately 1200 km from the northern tip of New Zealand.
Norfolk Island was selected to study the possible impact of a PCT system on obesity-related behaviors because demographically it is similar to much of Australia, it is a relatively closed system where all inputs and outputs to the Island can easily be measured and the project can be run as a community based initiative. Additionally, given that the population is already electricity conscious and reuses a lot of household items it will help identify what other behaviors may be influenced by a GHG emission reduction intervention that might otherwise not be recognized in other populations.
The Norfolk Island Carbon Health Evaluation (NICHE) study (http://www.niche.nlk.nf) is the first population study of its kind designed to evaluate whether a PCT intervention could positively influence environmental and health behaviors concurrently. The voluntary study began in 2011 with a comprehensive audit of the island and involvement with local residents through an elected NICHE committee. A voluntary household baseline survey was completed in 2012 and carbon cards were distributed to islanders that voluntarily agreed to participate in the intervention stage of the study in March 2013. The first phase of the project is designed to study fuel, power, and electricity use. A second phase, looking at food purchasing behavior will commence later in 2013. During the study, participants will be able to track their individual and household carbon footprint against the population norm and national target (personal carbon allowance) using the electronically based carbon card and account system.
Carbon-related behaviors are measured in real time through transactions recorded by the carbon card at the point of sale and matched with obesity-related behaviors measured pre- and postintervention.
Given the political nature of introducing a mandatory PCT into a population, a modified voluntary version of PCT was created with hypothetical financial incentives/disincentives being evaluated at follow up. Baseline surveys were delivered personally to households in support of 6 community groups incentivized to increase questionnaire completion in a census region through a small donation given based on completed questionnaires. More than 50% (n = 423) of all Norfolk Island households took part in the baseline survey.
Despite the voluntary nature of the survey, demographics (age, residential status, number of people per household) along with other variables such as the percentage of households using gas cooking and water tanks of the sample population when compared with census data 36 for the entire population were shown to be an accurate representation of the entire island community.
As part of the baseline survey, respondents were asked attitudinal questions relating to both the environment and health to see if there is a link between such attitudes and the strength of this link. If the 2 are related this would expand the options for interventions aimed at improving either obesity-related or emissions related behaviors. Initial results from the survey suggest that the link is real and significant. (These data are currently being prepared for publication.) The factors associated with attitudes to health were also shown to be correlated with attitudes about PCT. These results justify the need for further research exploring the links between environmental and health behaviors.
The NICHE study will continue to evaluate if there is a relationship between positive health and pro-environmental behaviors within an island-based population. It will measure the impacts of a simulated PCT on these behaviors to see whether both problems can reasonably be dealt with together and whether this is likely to be politically acceptability if scaled up into a tool for reducing emission and or as a public health strategy in larger national populations.
Where to Next?
Given that there is now an established link between environmental and health-related behaviors, there is a growing case for carbon reduction interventions aimed at changing environmental behaviors. These have the additional potential of being able to positively influence public health problems such as obesity.
Will a PCT intervention solve population obesity? Unlikely by itself, however, it does have the potential to positively influence the macro environment, a key construct of the epidemiological triad, 37 which to date has largely been lacking in obesity management. It is also hoped evidence will be forthcoming as to why health and environmental scientists should be working together to communicate and support cross disciplinary initiatives and messages around climate change and obesity management.
Footnotes
Acknowledgements
The Norfolk Island Carbon Health Evaluation project is funded by an Australia Research Council (ARC) Linkage Grant. Project No. LP110100452 conducted through Southern Cross University.