
Abstract
Introduction. Women attain numerous benefits from physical activity during pregnancy. However, because of physical changes that occur during pregnancy, special precautions are also needed. This review summarizes current guidelines for physical activity among pregnant women worldwide. Methods. We searched PubMed (MedLINE) for country-specific governmental and clinical guidelines on physical activity during pregnancy through the year 2012. We cross-referenced with articles referring to guidelines, with only the most recent included. An abstraction form was used to extract key details and summarize. Results. In total, 11 guidelines were identified from 9 countries (Australia, Canada, Denmark, France, Japan, Norway, Spain, United Kingdom, United States). Most guidelines supported moderate-intensity physical activity during pregnancy (10/11) and indicated specific frequency (9/11) and duration/time (9/11) recommendations. Most guidelines provided advice on initiating an exercise program during pregnancy (10/11). Six guidelines included absolute and relative contraindications to exercise. All guidelines generally ruled-out sports with risks of falls, trauma, or collisions. Six guidelines included indications for stopping exercise during pregnancy. Conclusion. This review contrasted pregnancy-related physical activity guidelines from around the world, and can help inform new guidelines as they are created or updated and facilitate the development of a worldwide guideline.
‘Guidelines on physical activity during pregnancy provide recommendations for health professionals as to whether to prescribe physical activity and if so, in what manner.’
Introduction
Health benefits of physical activity during pregnancy include reduced risk of excessive gestational weight gain and conditions such as gestational diabetes, preeclampsia, preterm birth, varicose veins, and deep vein thrombosis.1-4 There is some evidence that physical activity during pregnancy is associated with a reduced length of labor and delivery complications. 4 However, vigorous leisure activity is associated with reduced birth weight. 5 Psychological benefits to physical activity during pregnancy include reduced fatigue, stress, anxiety, and depression, as well as improved well-being.1-4 From a public health perspective, women who are active during pregnancy are more likely to continue physical activity during postpartum. 4
Physiologic responses to exercise, such as changes in heart rate, cardiac output, ventilation, and energy expenditure, are all greater during pregnancy than prepregnancy, and may become more pronounced as pregnancy progresses.6,7 Hormonal changes increase joint laxity that may place a woman at increased risk for injury. 8 Adaptations to physical activity are needed to reduce the risk of injury for both the mother and baby.
Guidelines on physical activity during pregnancy provide recommendations for health professionals as to whether to prescribe physical activity and if so, in what manner. Guidelines from a variety of organizations help address questions about physical activity, such as how long, how far, how often, and at what intensity. The World Health Organization’s guideline on physical activity recommends that adults aged 18 to 64 years should engage in at least 150 minutes of moderate-intensity aerobic activity throughout the week (in bouts of at least 10 minutes), or at least 75 minutes of vigorous-intensity aerobic activity, or an equivalent combination of the two. 9 Muscle strengthening should be done 2 or more days per week. The guideline states that pregnant women may need extra precaution and should seek medical advice before striving to achieve the recommendations.
More detailed guidelines for physical activity during pregnancy are available from several countries, with some guidelines based on evidence and others based on expert consensus. These guidelines were produced by a range of professional bodies and government agencies, and were written for different target audiences, and at different times. The aim of this review was to summarize the different public health and clinical guidelines on physical activity during pregnancy from around the world. A summary of guidance across countries may stimulate national bodies to develop guidelines where they do not exist, share best practices, and update existing guidance. It could also facilitate the development of a global recommendation for physical activity during pregnancy.
Methods
For this review, we searched PubMed (MedLINE) for published guidelines on physical activity during pregnancy. The search was narrowed to peer-reviewed studies published between 1990 and 2012. We cross-referenced with articles that referred to country-specific guidelines and then identified an expert in that country to work with on the project. Thus, each country included in this review was represented by at least one scientist. To narrow the scope of the review, we included only the most recent country-specific or clinical guidelines. Layman-oriented guidelines and those from other societies (such as dietetics) were excluded. A single author reduced all extraction forms into tables that coauthors subsequently checked.
Results
Background
We identified 11 guidelines representing 9 countries, including Australia,10,11 Canada,3,12,13 Denmark,14,15 France, 16 Japan,17,18 Norway, 19 Spain, 20 the United Kingdom, 4 and the United States2,21 (Table 1). The guidelines represented or endorsed by obstetrics and gynecology (Australia, Canada, Denmark, Spain, United Kingdom, United States), public health (Canada, Denmark, France, Norway, United States), sports medicine (Australia, Japan), and exercise physiology (Canada). Since the 2 Danish guidelines were essentially identical in their recommendations, they were coded in the remaining tables as one guideline,14,15 The 2 US guidelines differed and thus coded separately: American College (now Congress) of Obstetricians and Gynecologists (ACOG) 21 and the US Department of Health and Human Services (USDHHS). 2
Development of Clinical and Public Health Guidelines for Physical Activity During Pregnancy.
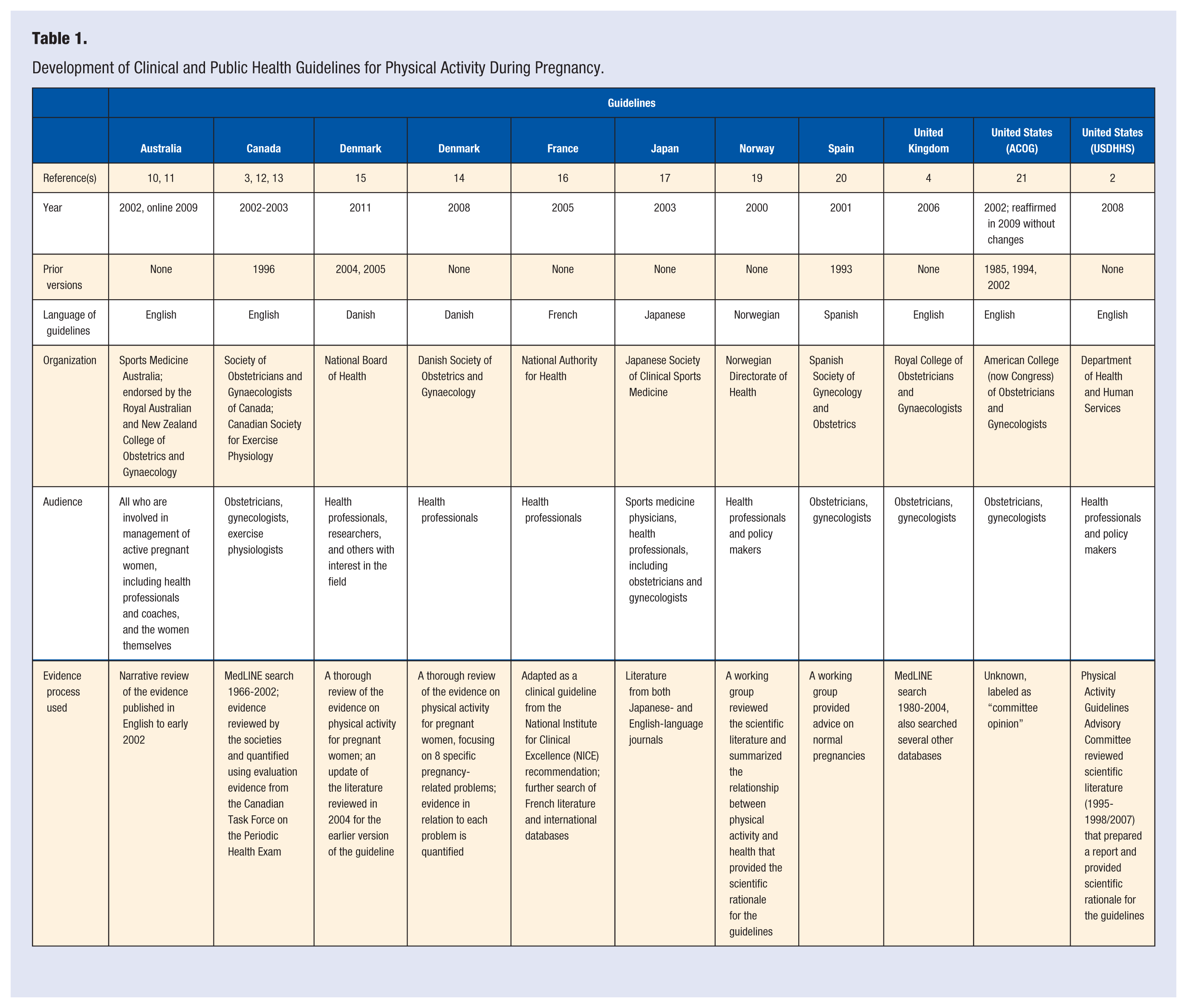
Most guidelines included a comprehensive literature review, but not a quality assessment. However, Canada had a comprehensive rating of scientific evidence contributing to its guidelines, which included a quality assessment of the evidence (considering the study design in this process) to support each recommendation. The Danish Society of Obstetrics and Gynecologists guideline also rated the evidence for each issued recommendation.
Contraindications to Exercise During Pregnancy
Absolute contraindications refer to conditions where exercise is not recommended. Relative contraindications refer to conditions where the risks of exercise may exceed the benefits. Guidelines from Canada, Japan, Spain, and the US ACOG described contraindications to exercise in absolute and relative terms; however, guidelines from Norway and the United Kingdom did not make these distinctions (Table 2). The guidelines from Australia, Denmark, France, and the USDHHS did not address contraindications, because they were intended for healthy women with normal pregnancies. Generally, where 2 or more countries identified contraindications, they agreed on whether it was an absolute or relative contraindication.
Absolute and Relative Contraindications to Exercise During Pregnancy. a
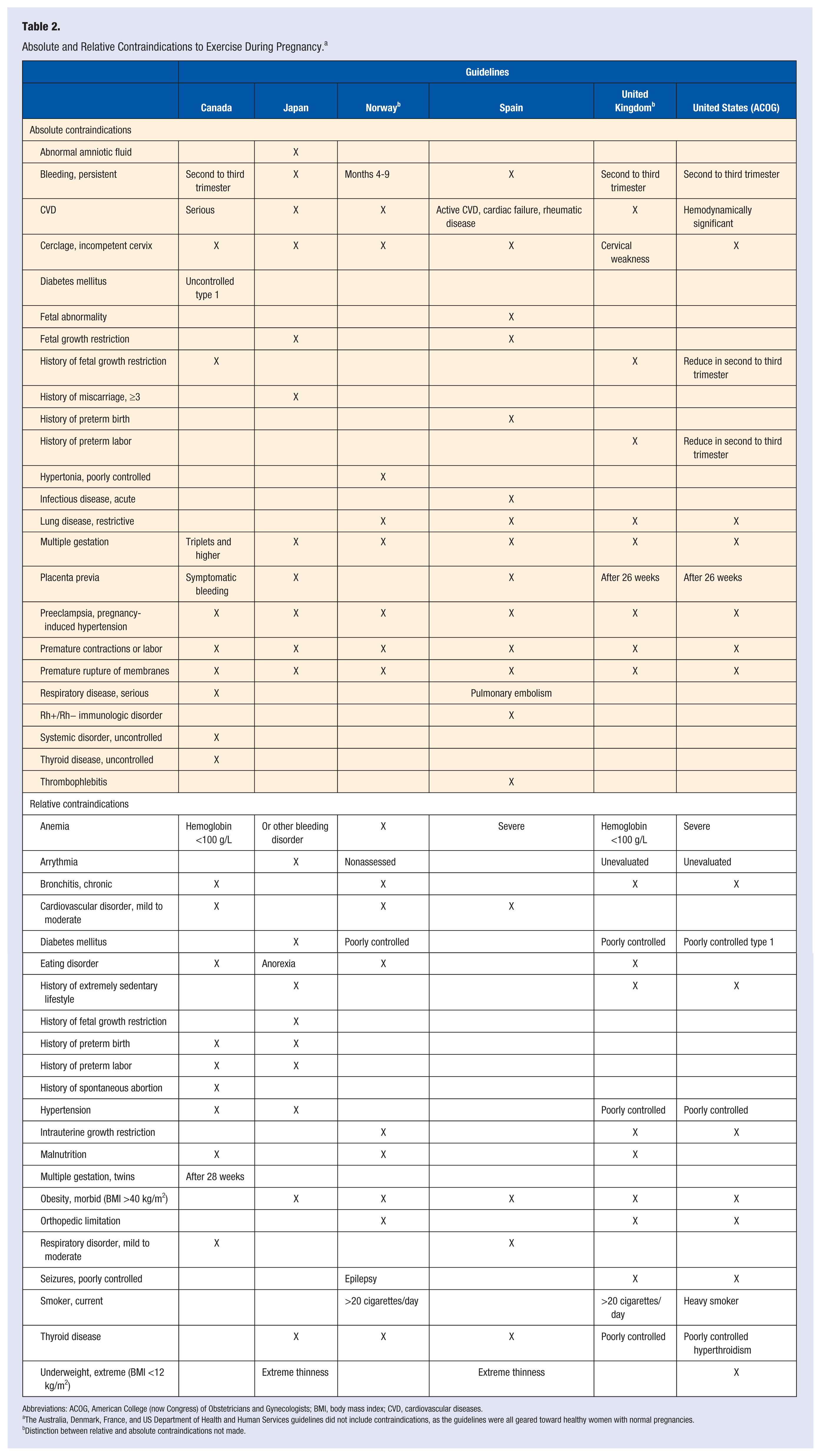
Abbreviations: ACOG, American College (now Congress) of Obstetricians and Gynecologists; BMI, body mass index; CVD, cardiovascular diseases.
The Australia, Denmark, France, and US Department of Health and Human Services guidelines did not include contraindications, as the guidelines were all geared toward healthy women with normal pregnancies.
Distinction between relative and absolute contraindications not made.
The 6 countries (Canada, Japan, Norway, Spain, United Kingdom, US ACOG) agreed on several contraindications to exercise, including anemia, persistent bleeding, cardiovascular disease, cerclage or incompetent cervix, multiple gestation, preeclampsia or pregnancy-induced hypertension, premature contractions or labor, premature rupture of membranes and thyroid disease. Four or five of the 6 guidelines identified contraindications for diabetes mellitus, eating disorder, morbid obesity, and placenta previa.
Activities to Avoid During Pregnancy
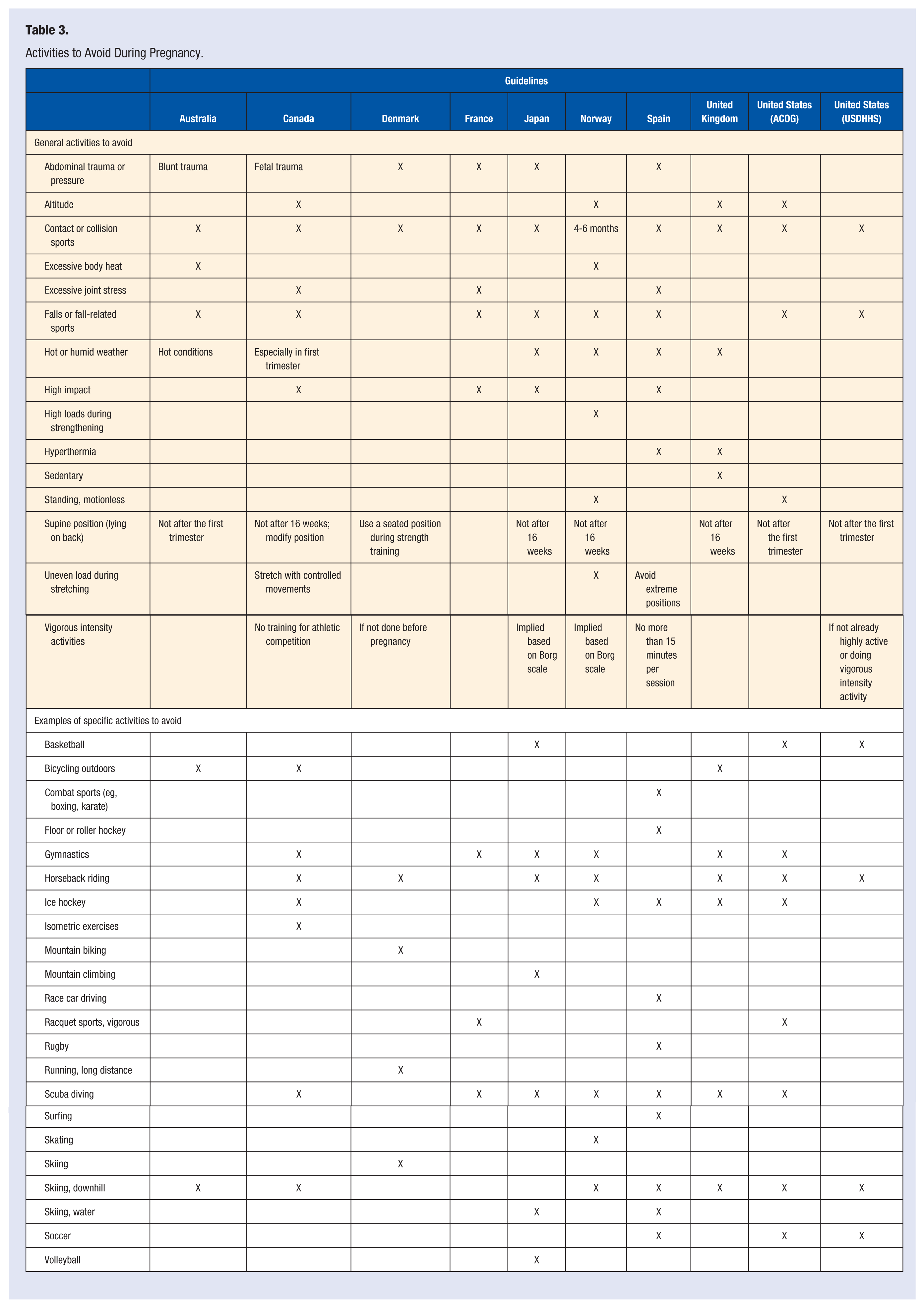
For women who received physician clearance to exercise during pregnancy, all reviewed guidelines described specific characteristics of activities to avoid and specific sports to avoid (Table 3).
Activities to Avoid During Pregnancy.
Falls or Trauma
All guidelines generally ruled out sports involving risks of falls, trauma, or collisions. A sport’s safety was determined based on the movements required to participate in it. One concern was that the ligaments become relaxed because of increasing hormone levels, making joints more prone to injury (Australia, Canada). The Norwegian guideline was the only one to warn against high loads during strengthening exercises because of the risk of pressure reflex.
Position
All but 2 guidelines (France, Spain) warned against activities in the supine position (lying on one’s back) because of the chance of decreased cardiac output and orthostatic hypotension caused by the enlarged uterus, which may obstruct venous return or blood flow from the abdominal aorta. As a result, these guidelines recommended avoiding the supine position during physical activity after the first trimester or 16 weeks’ gestation. Canada’s guideline suggested modifying the position of the exercise to instead be on one’s side, sitting, or standing. Denmark’s guidelines recommended a seated position during strength training.
Altitude and Depth
Four guidelines included recommendations about physical activity or exercise at altitude. Canada’s guideline accepted moderate exercise at altitudes up to 6000 to 8250 feet (1800-2500 meters). The US ACOG guideline stated that exercise up to 6000 feet (1800 meters) appeared safe, but exercise at higher altitudes carried risk. It also stated that women should be informed of the signs of altitude sickness and advised that if it develops, to stop exercising and descend from altitude to seek medical attention. Norway and the United Kingdom guideline suggested women at altitudes above 8250 feet (2500 meters) obtain 4 to 5 days of exposure at that altitude to avoid exertion and to regulate uterine blood flow. Seven guidelines specifically warned against scuba diving during pregnancy, because the fetus is not protected from decompression sickness and the fetal pulmonary circulation cannot filter bubble formation in the maternal bloodstream.
Heat and Cold
The Australian and Norwegian guideline warned of excessive body heat during exercise for pregnant women. Several other guidelines (Canada, Japan, Spain, United Kingdom) warned of exercising in hot or humid weather.
Sedentary Behavior and Motionless Standing
The United Kingdom guideline specifically mentioned avoiding a sedentary lifestyle, stating that “women and care providers should consider the effects of a sedentary lifestyle during pregnancy . . .”4(p3) because it can contribute to a number of adverse maternal outcomes. The Norwegian and US ACOG guidelines were the only ones to advise against motionless standing due to its association with decreased cardiac output.
Avoidance of Vigorous-Intensity Activity
Regarding vigorous activity, the Canadian and Norwegian guidelines cautioned against athletic competition, whereas the Australian guideline advised close monitoring by a physician. For both Japan and Norway, the recommended rating of perceived exertion categories did not include the vigorous intensity range. The USDHHS guideline stated that women not already highly active or engaged in vigorous activity should focus on moderate-intensity activity. The Denmark guidelines cautioned against vigorous activity for women not engaged in it prior to pregnancy. These guidelines also advised that pregnant women accustomed to high-intensity physical activity during prepregnancy could continue this activity as long as they felt well. The Spanish guideline recommended no more than 15 minutes of vigorous activity and to decrease intensity by 20% to 30% for pregnant athletes. The French guideline mentioned that women engaged in jobs that involved hard or strenuous aspects or long travel time should refer to her occupational or family physician and consider specific adjustments to job tasks.
Activities to Perform During Pregnancy
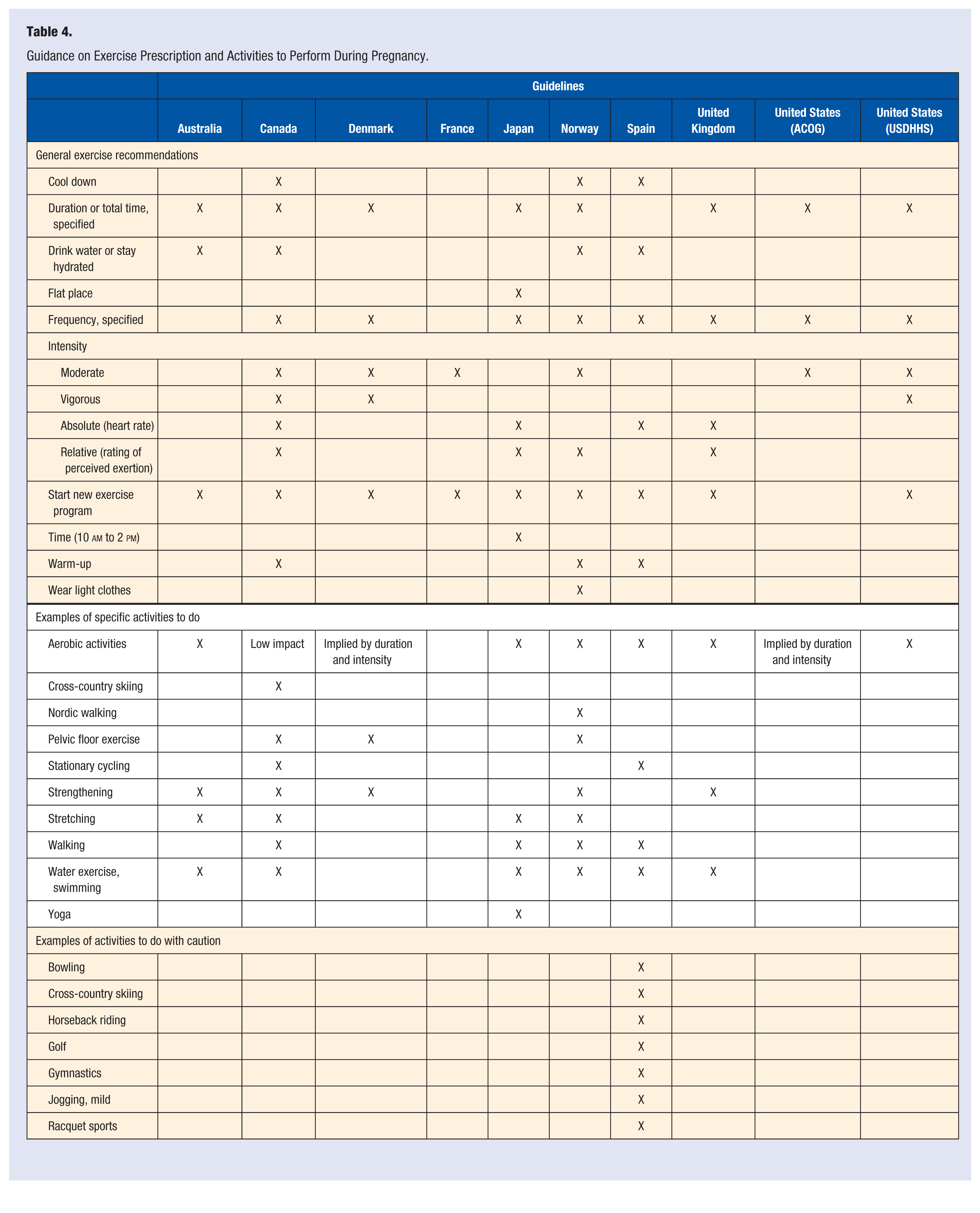
Most guidelines recommended activities to engage in during pregnancy (Table 4). All but the French and Spanish guidelines indicated duration or total time and all but the Australian and French guidelines indicated frequency of physical activity. For most all guidelines, intensity was indicated as moderate or vigorous, or in absolute (eg, heart rate) or relative (eg, rating of perceived exertion) indicators.
Guidance on Exercise Prescription and Activities to Perform During Pregnancy.
Type
All but the French guidelines specified aerobic activities as an acceptable modality. Guidelines from Australia, Canada, Denmark, Norway, and the United Kingdom also recommended strengthening exercises. Other specific activities that were recommended are summarized in Table 4. Only Spain provided a list of activities to perform with caution.
Frequency and Duration
Most guidelines (with the exception of those from France) included information on frequency and/or duration of exercise. Specifically, Canada and United Kingdom indicated a minimum of 15-minute sessions for 3 times per week, progressing to 30 minutes, 4 times per week even if intensity was reduced. Denmark recommended at least 30 minutes of moderate intensity activity daily. Japan recommended aerobic exercise for up to 60 minutes, 2 to 3 times per week. Norway recommended 30 minutes per day of aerobic activity. Spain recommended a frequency of 3 times per week with no duration specified. The US ACOG recommended accumulating 30 minutes or more of moderate exercise on most if not all days of the week. The USDHHS indicated that
healthy women who are not already highly active or doing vigorous-intensity activity should get at least 150 minutes (2 hours and 30 minutes) of moderate-intensity aerobic activity per week during pregnancy and the postpartum period. Preferably this activity should be spread throughout the week.2(p42)
Intensity
For absolute intensity, heart rate guidance was the provided by Canada, Japan, Spain, and the United Kingdom. Guidelines from Canada and the United Kingdom specified heart rates accounting for age; however, Japan and Spain recommended heart rates less than 150 and 140 beats per minute, respectively. The Canadian guideline advised working in the lower ends of the heart rate zone if starting a new exercise program or in late pregnancy. The target heart rate zones provided by Canada represented 60% to 80% of maximal aerobic capacity. The United Kingdom guideline advocated for an “upper range of 60% to 90% maximal heart rate for women wishing to maintain fitness during pregnancy,”4(p4) and 60% to 70% of maximal heart rate for women who were sedentary prior to pregnancy. The Norwegian guideline recommended that aerobic exercise intensity should not exceed 70% to 75% of maximal oxygen uptake, instead advising use of a talk test (being able to talk while exercising) or the Borg’s rating of perceived exertion scale. 22 Canada and the United Kingdom also mentioned the usefulness of the “talk test.” The lowest guidance on intensity was from Spain, which recommended not exceeding 50% of maximal oxygen consumption.
For relative intensity, Canada, Norway, and the United Kingdom recommended perceived exertion of 12 to 14, just above or below “somewhat hard,” which generally coincided with moderate intensity. Japan recommended a perceived exertion less than 13 (somewhat hard) or 14, and for continuous exercise to be less than 11 (fairly light) or 12.
The French guideline recommended that beginning or continuing moderately intense sport physical activity during pregnancy was possible. The USDHHS guideline indicated that
pregnant women who habitually engage in vigorous-intensity aerobic activity or are highly active can continue physical activity during pregnancy and the postpartum period, provided that they remain healthy and discuss with their health-care provider how and when activity should be adjusted over time.2(p42)
The Australian guideline condoned this: for healthy women not highly active or engaging in vigorous activity, then moderate intensity was recommended. The US ACOG stated that pregnant women should engage in regular, moderate intensity physical activity in the absence of contraindications.
Starting a New Exercise Program
All but the US ACOG guidelines included guidance for women starting a new exercise program during pregnancy. The Australian guideline suggested that women could begin a light to moderate exercise program in consultation with their doctor, and the Canadian guideline stated that for uncomplicated pregnancies “women with or without a previously sedentary lifestyle should be encouraged to participate in aerobic and strength-conditioning exercises as part of a healthy lifestyle.”3(p334) It indicated this generally was “in the second trimester, when the nausea, vomiting, and profound fatigue of the first trimester have passed and before the physical limitations of the third trimester begin.”3(p335) In Japan, the guideline indicated that if a pregnant woman started a sport during pregnancy, she should initiate it after 12 weeks’ gestation and confirm a normal pregnancy.
In Norway and the United Kingdom, women engaging in new exercise programs during pregnancy were encouraged to begin gradually with shorter sessions of 15 minutes for 3 times per week, then increase gradually to 30-minute sessions 4 times a week, and eventually to daily sessions. Spain recommended only initiating exercise slowly for previously sedentary women, but did not provide specifics. The US ACOG guideline indicated that previously inactive women should be evaluated before physical activity recommendations are made and to increase the amount of physical activity gradually over time. The USDHHS guideline also indicated that
when beginning physical activity during pregnancy, women should increase the amount gradually over time. The effects of vigorous-intensity aerobic activity during pregnancy have not been studied carefully, so there is no basis for recommending that women should begin vigorous-intensity activity during pregnancy.2(p42)
Other Exercise Guidance
The guidelines from Canada, Norway, and Spain suggested warming up and cooling down before and after exercise, respectively. Australia, Canada, Norway, and Spain also mentioned hydration during exercise. Norway’s guideline also suggested wearing light clothes during exercise. Japan’s guideline described environmental characteristics of the exercise, such as choosing a flat place and exercising between 10
Signs and Symptoms to Stop Exercise
Six guidelines included indications for stopping exercise during pregnancy (Table 5), whereas Denmark, France, and the USDHHS did not. All 6 guidelines indicated ceasing exercise with dizziness or presyncope, dyspnea before exertion, or vaginal bleeding. Five of the 6 guidelines recommended ceasing exercise if there was indication of abdominal or back pain, amniotic fluid leakage, or excessive shortness of breath. The remaining signs or symptoms in Table 5 were only indicated in 1, 2, 3, or 4 of the guidelines.
Signs and Symptoms to End Exercise During Pregnancy. a
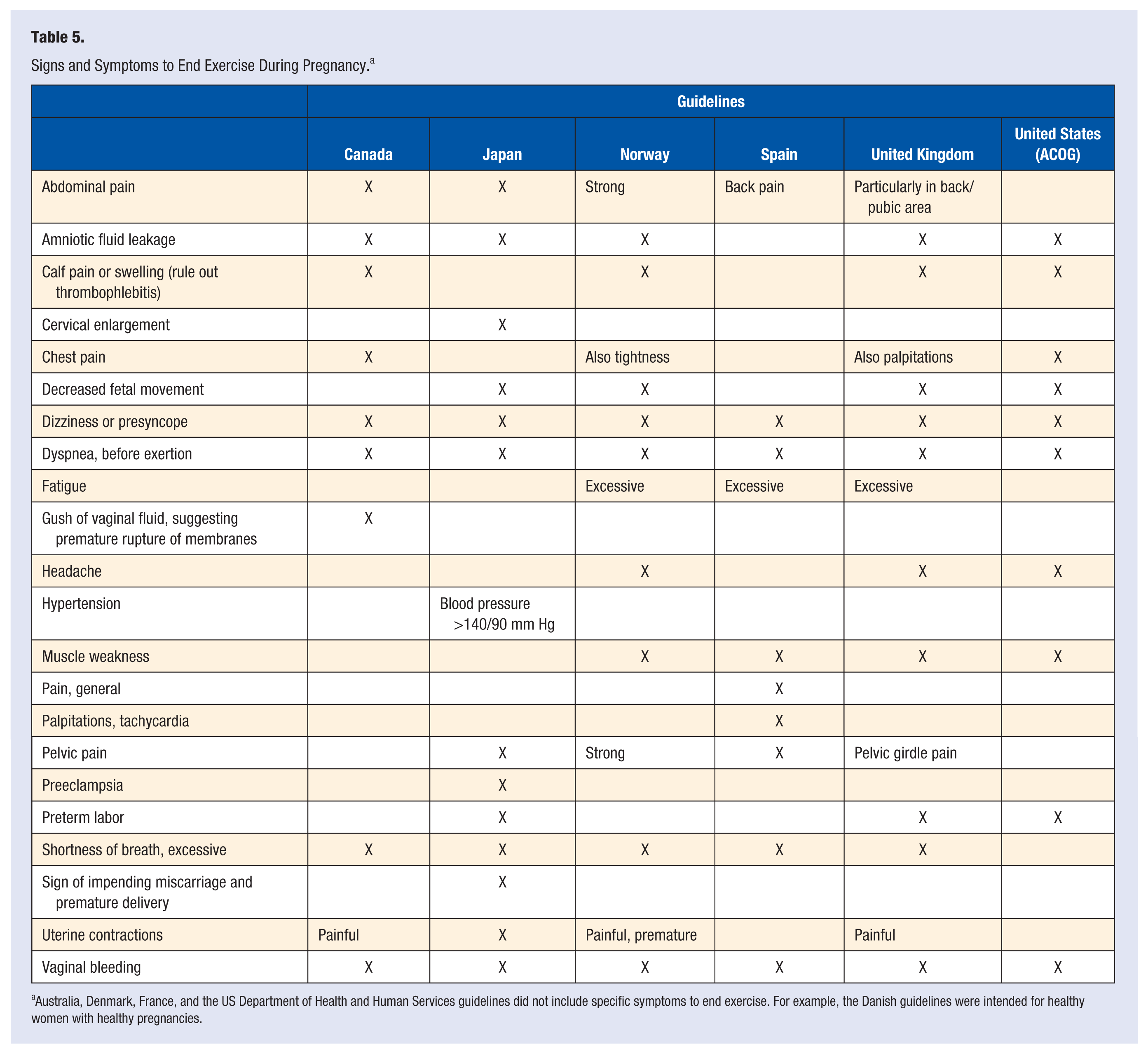
Australia, Denmark, France, and the US Department of Health and Human Services guidelines did not include specific symptoms to end exercise. For example, the Danish guidelines were intended for healthy women with healthy pregnancies.
Discussion
The earliest formal recommendations for physical activity during pregnancy can be documented from the 18th century, which largely reflected the cultural and social norms of the times, rather than scientific evaluation.25,26 The earliest studies on maternal physical activity and birth outcomes were conducted in the late 19th and early 20th centuries.26,27 Corresponding with the developing science, recommendations on physical activity during pregnancy continue to be created and updated to provide guidance to health professionals. In this review, we identified, summarized, and contrasted 11 clinical or public health guidelines for physical activity during pregnancy from around the world.
Generally, we found that the content of the guidelines varied depending on the date of publication and target audience (ie, clinicians vs public health professionals). There were commonalities as well. For example, almost all guidelines supported moderate-intensity physical activity during pregnancy (Spain implied it through heart rate recommendations but not through oxygen consumption). Most guidelines also suggested that women should seek advice from their health care provider before starting or continuing an exercise program. All ruled out sports involving either risks of falls, trauma, or collisions during pregnancy. The 6 more clinically focused guidelines included contraindications to exercise, including signs and symptoms that should indicate stopping. In terms of exercise prescription, most of the guidelines included specific type, frequency, and duration or time for physical activity or exercise during pregnancy.
A difference across guidelines was the use of relative and absolute intensity to guide the exercise. Canada, Japan, and the United Kingdom all provided guidance for intensity using both heart rate (absolute intensity) and ratings of perceived exertion (relative intensity). In contrast, Denmark, France, US ACOG, and USDHHS indicated neither. However, the US ACOG prior guidelines from 1985 statement did include heart rate guidance 28 that was removed in 1994. 29
Only guidelines from Canada, Denmark, and USDHHS provided any recommendation on vigorous-intensity physical activity. This reflects the lack of accumulated evidence from well-designed studies on vigorous activity and pregnancy outcomes. 30 To date, most studies on vigorous-intensity physical activity during pregnancy are laboratory based or observational, often with insufficient statistical power to detect findings on relatively rare outcomes. In addition, lack of recommendations about vigorous activity could be due to discrepancies in the definition for this level of intensity.
While most guidelines focused on aerobic exercise, 5 countries indicated strengthening exercises. Only a few studies have investigated the safety and efficacy of strength training during pregnancy.31,32 Given the potential health-related benefits of strength training during pregnancy, more work is needed to clarify the safest prescription in terms of volume and intensity. The Canadian guideline suggest using lighter weights and more repetition, not lifting while lying flat on one’s back, and avoiding the Valsalva maneuver.
Sedentary behavior is modifiable and comprises time spent in periods of little or no movement while awake, such as sitting, ranging from 1.0 to 1.5 metabolic equivalents.33 -35 The concept that sedentary behavior is not equivalent to lack of physical activity has only recently emerged in the health literature, since one can be physically active and accumulate large amounts of sedentary time. Only the United Kingdom guideline mentioned sedentary behavior in the context of reducing it. Future pregnancy guidelines could consider more specific recommendations on sedentary behavior, particularly as research evidence is accumulated around this topic for pregnant women. In addition, none of the guidelines discussed indications for bed rest, despite its prescription to many women. 36 However, indication of bed rest implies a higher risk pregnancy, and these guidelines were usually geared toward women with normal pregnancies.
A challenge across several guidelines was a lack of clarity in terminology used to describe exercise. For example, several guidelines (Denmark, Norway, United Kingdom, US ACOG) interchanged the terms “exercise” with “physical activity.” Physical activity is a broad term that is defined as any bodily movement produced by contraction of skeletal muscles that results in increased energy expenditure above a basal level. 37 Exercise is a subcategory of physical activity that is planned, structured, and purposive to maintain or improve one or more components of physical fitness. Some of the terminology issues arise from cultural differences. For example, in the Danish guidelines “physical activity” and “exercise” are interchanged, and other terms are used as well (physical training, motion, fitness training), which are difficult to translate directly. Other terminology discrepancies reflect the differing target groups, for example athletes and sportswomen, who usually “exercise” and the general population, who are encouraged to “be active.”
Despite variations in the specific amount of physical activity recommended during pregnancy, pregnant women worldwide often do not meet the recommendations. Studies in each country represented in this review have shown that many pregnant women do not obtain as much physical activity or exercise as recommended in their country (examples of studies follow but are not exhaustive):
Australia (Australian Longitudinal Study on Women’s Health 38 )
Canada (surveillance study of Ontario 39 )
Denmark (Danish birth cohort study 40 )
France 41
Japan (convenience sample of pregnant women from 5 facilities in Kanto, Tokyo 42 )
Norway (pregnant women participating in a birth cohort study near Oslo 43 )
Spain 44
United Kingdom (cohort study in southwest England 45 )
United States (surveillance studies of the entire country46 -49)
Data from these countries indicate that a higher priority should be placed on promoting physical activity during pregnancy, including both education and addressing barriers to physical activity. More work is needed to understand the advice offered to pregnant women by their health care providers and how that advice is received and used. 50 Future studies across countries can elucidate the reasons behind the differences in beliefs, explore whether cultural reasons contribute to these differences, and determine whether tailored messages are more effective than general educational approaches.
Further work is also needed to enhance our understanding and use of pregnancy-related physical activity guidelines by health care providers. To facilitate the use of guidelines in practice, the Physical Activity Readiness Medical Examination (PARmed-X) for Pregnancy tool was developed to open communication between the health care provider, fitness professional, and the pregnant woman.12 The 4-page form includes a pre-exercise checklist the woman can fill out, contraindications to exercise the health care provider completes, and a health evaluation form that can be used by the prenatal fitness professional. It also includes information on prescribing aerobic activity, muscular conditioning, and active living. This screening tool facilitates implementation of the guidelines by providing a convenient checklist and prescription for health care providers to use in evaluating pregnant women who want to start a prenatal fitness program. Use of this tool may increase adherence to the physical activity guidelines by both providers and their patients.51,52
Limitations
Several limitations of this review should be acknowledged. The review was narrowed in scope and not all inclusive; we hypothesize that there are other guidelines that met our review criteria were not captured with our search efforts, particularly those not found in PubMed. For example, the review did not include guidelines from lower income nations, indicating either the recommendations were not captured by our search procedures or do not exist. Another limitation was that one person was unable to review all the original guidelines because of language differences. This problem was diminished by using a standardized extraction form. It should also be noted that while the abstraction was based on the published guideline, many countries created supplemental documents geared toward laypersons and often available in print or on the Internet. Although these materials may contain additional information, they were not reviewed herein. Despite these limitations, to our knowledge, this review is the first to summarize and compare current guidelines for physical activity during pregnancy from 9 different countries around the world. This review can be expanded as guidelines are developed, updated, and better accessed.
Conclusion
This review contrasted pregnancy-related physical activity guidelines from around the world and may help to inform the creation of new guidelines, or updates of older ones. It could also facilitate the development of a worldwide guideline. The guidelines we reviewed were important sources of information at the national level for promoting physical activity and exercise during pregnancy. Recognizing contraindications to physical activity, the guidelines can be used to advise and encourage pregnant women to take part in physical activity either by maintaining their prepregnancy levels of activity or, for previously sedentary women, by starting a new exercise program during pregnancy.
Footnotes
Acknowledgements
The authors thank Margeaux Kiyoko Akazawa (Emory University) for assisting with translation between English and Japanese, and Sara Satinsky for review of earlier drafts of the article.
Funding
Kelly R. Evenson acknowledges support by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health (NIH, #UL1TR000083), and the University Research Council at the University of North Carolina at Chapel Hill. Ruben Barakat acknowledges funding from the Spanish Ministry of Science and Innovation (DEP2009-08990) and Technical University of Madrid, Spain (UPM AL12-P-I+D-14). Michelle F. Mottola acknowledges funding from the Canadian Institutes of Health Research, and endorsement from Health Canada and the Canadian Society of Exercise Physiologists. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.