
Abstract
The American College of Obstetricians and Gynecologists recommends that women exercise throughout pregnancy unless they have a condition-related contraindication. This study’s purpose was to determine if pregnant women perceive receiving exercise counseling by their providers with details of frequency, intensity, type, and time (FITT principle). Women in 2 postpartum care units of a large health care system were invited to complete a voluntary, anonymous survey regarding whether they received exercise counseling during their prenatal care. Survey results were descriptively reported, stratified by demographic variables, and analyzed using Fisher’s exact tests. Of 224 postpartum women surveyed, 130 (58.0%) perceived receiving exercise counseling during pregnancy; 119 (91.5%) did not recall receiving counseling on exercise frequency. Though 165 (73.6%) exercised before becoming pregnant, 64 (38.8%) ceased exercise during pregnancy. Eighty-eight (39.3%) received advice from other sources/non–health care professionals. Privately insured women reported receiving exercise counseling at a higher rate (70.1%) than those on Medicaid (44.8%) or uninsured (40.0%; P = .004). A disproportionate number of pregnant women perceived not receiving adequate prenatal exercise counseling or received incomplete counseling. Women at a socioeconomic disadvantage may be vulnerable. As social determinants of health, structural barriers, and socioeconomic status likely contribute, women may benefit from more targeted inclusive and equitable messaging.
‘. . . it is estimated that 60% of pregnant women do not perform any type of leisure-time physical activity (PA) during pregnancy.’
The Centers for Disease Control and Prevention (CDC) and Department of Public Health state that exercise in pregnancy reduces the risk of excessive weight gain, gestational diabetes, and postpartum depression, all comorbidities that have damaging impacts on morbidity and mortality for both the mother and baby. 1 Exercise during pregnancy also reduces risk of morbidity and mortality for the mother and baby according to the Department of Health and Human Services. 1 Nevertheless, it is estimated that 60% of pregnant women do not perform any type of leisure-time physical activity (PA) during pregnancy. 2 Common reasons for reduced levels of PA during pregnancy include physical discomfort, nausea or fatigue, insecurity with PA during pregnancy, fear of obstetric complications, and lack of time. 3 However, the American College of Obstetrics and Gynecology (ACOG) Committee Opinion Number 804 reports that PA does not increase risk of miscarriage, low birth weight, or early delivery throughout low-risk pregnancies. 4
Other reasons for reduced PA during pregnancy include environmental/lifestyle barriers, particularly among women with a lower socioeconomic status. A 2018 systematic literature review suggests that women with low socioeconomic status report fear of walking alone, difficulty accessing facilities, and low social support as barriers to leisure-time PA. 5 The absence of such infrastructure and community not only discourages PA for concerns of safety but also diminishes social support and interpersonal accountability. Furthermore, women report fatigue, lack of time, and domestic commitments including childcare as significant barriers, which were all shown to be inversely associated with PA. 6
Fortunately, women demonstrate receiving benefit from targeted health initiatives during pregnancy,7-9 particularly if they are young or have few educational qualifications. 10 Crozier et al reported reductions in smoking (12% reduction), caffeine (13% reduction), and alcoholic beverages (44% reduction) in 1490 women during pregnancy after receiving recommendations. 10 May et al reported that women who were “more careful about eating healthy (odds ratio [OR], 3.1; 95% confidence interval [CI], 1.2-8.0) and who discussed exercise with their obstetric provider (OR, 2.2; 95% CI, 1.1-4.3) were more likely to maintain or increase exercise” during pregnancy than those who were not conscientious about their diets and those who did not discuss exercise with their obstetric provider, respectively. The odds of obstetric providers discussing exercise with pregnant patients increased 7-fold (OR, 7.1; 95% CI, 1.4-37.3) for each health behavior the obstetric provider discussed with the patient. 11
While studies provide evidence that messaging from obstetric health care providers regarding lifestyle changes may be beneficial for improving health during and after pregnancy, little data exist regarding a person’s perception of receiving that information.12-16 Perception of counseling may significantly influence health outcome results in pregnant women. A previous study examining communication around weight gain management in socioeconomically disadvantaged, African American women demonstrated a potential gap in communication on exercise and weight gain during pregnancy, as although providers reported giving weight management advice, patients did not report receiving the same information. 17
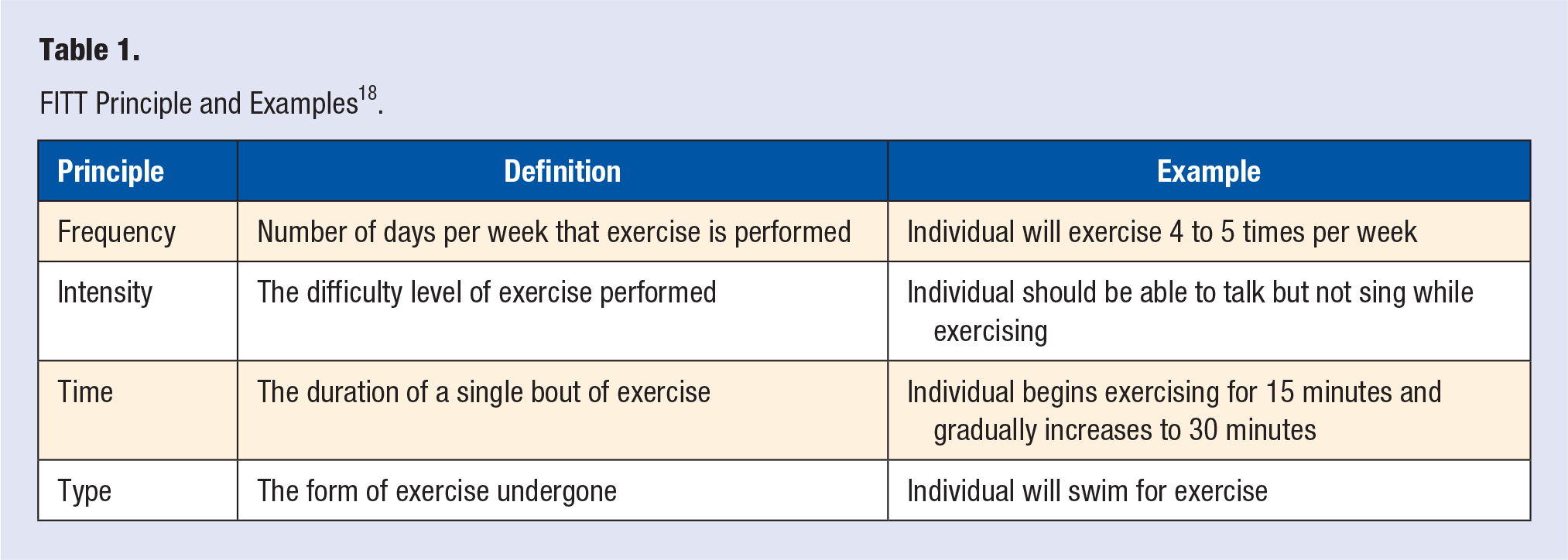
Patient reports of advice on PA are consistent with the previously stated CDC guidelines, but limited in scope and detail. 13 The FITT (frequency, intensity, type, and time) principle, for example, is recommended by the American College of Sports Medicine as well as experts in prenatal health as a foundational tool used for exercise prescription that is defined by specific instructions on frequency (ie, how often), intensity (ie, how hard), time (ie, how long), and type of exercise (ie, what kind; Table 1). 18 Limited data exist demonstrating whether or not the FITT principle is used in counseling pregnant women on exercise despite the recommendations for exercise, and specific exercise prescriptions, by ACOG.4,19 Notably, women are more likely to meet exercise goals if prescribed by their obstetric health care provider, representing an opportunity for providers to positively influence the actions of their patients. 13 Despite the existing evidence that women are more likely to make lifestyle changes when pregnant, and the evidence of the advantages of exercise throughout pregnancy, there remains a lack of literature on whether or not specific exercise prescriptions are given to patients throughout prenatal care, and more specifically, little data exist on whether or not women recall receiving this intervention throughout pregnancy.
FITT Principle and Examples 18 .
Therefore, the purpose of this study was to determine (1) whether women are perceiving the receipt of information during pregnancy from their obstetric healthcare providers; (2) whether women perceive that providers are giving specifics of the FITT principle; (3) whether this perception varies by race/ethnicity, socioeconomic status, insurance type, and care clinic; and (4) whether women perceive receiving information from sources other than their obstetric provider.
Methods
Investigators invited postpartum women at 2 birthing units at Prisma Health–Upstate, Greenville, South Carolina, to complete anonymous surveys about their perception
The 20-item, predominately multiple-choice survey was developed and validated according to the process described by Zamanzadeh et al, according to previous research for assessing exercise behaviors in adults, and according to previous research on exercise prescription assessment using the established FITT principle and specified for pregnant women (Supplement 1).19,22-24 In brief, the survey development and validation process by Zamanzadeh et al involves domain determination, item/question generation, instrument formation, instrument revision and consolidation, and preliminary instrument version team consensus. 23 It also involves utilizing a team of content experts in the development of the survey from a wide variety of backgrounds on the proposed topic, with the goal of improving engagement of the patient taking the survey. 23 The survey development team included 1 PhD-trained exercise physiologist, 1 board-certified OBGYN clinician, 5 second-year medical students, and 1 senior biostatistician in order to maximize content importance of the survey questions. The questions were developed based on current literature for exercise prescriptions, the importance of the FITT principle in exercise prescriptions, and exercise recommendations in pregnancy, which ensured the survey questions engaged the participant in topics that were up to date and evidence based.19,22,24 Content validity of the survey, per the process outlined by Zamanzadeh et al, was established a priori via a stepwise process: Step 1—internal team members reviewed each item and proposed conceptual or grammatical revisions; Step 2—external panel members including 2 board-certified OBGYN clinicians and 1 full-time OBGYN research nurse reached consensus on proposed item revisions to maximize face and content validity; Step 3—preliminary and revised versions of the questionnaires, respectively, were pilot tested with pregnant women and obstetric providers to ensure that the questions were clear and concise. 23 Investigators designed the survey to be brief (average time to complete was <5 minutes) in effort to respect the participant’s time, keep the participant’s attention, and reduce chance of survey errors due to postpartum fatigue and infant care demands. This process is also recommended with the goal of establishing trust with the participant as well as maximizing patient activation. 23 The pilot tests with pregnant women who provided feedback helped provide external validation and improve the instrument for optimal patient engagement. Participants completed the survey on a HIPAA-secure, user-friendly, web-based online application that collects and stores data (REDCap, Vanderbilt University).
Investigators performed descriptive analyses, stratified by demographic variables, and analyzed using Fisher’s exact tests of independence to determine if there was a significant relationship between the 2 categorical variables. More specifically, investigators used 2-sided test of the Fisher’s exact test and calculated the P value. This method was preferred over the χ 2 test as the smaller sample may make the χ 2 test unreliable and therefore inappropriate for this particular study. Comparisons across demographics were examined using frequencies, associations, and substratification on associations using SPSS v21.0 (IBM Corporation). Analyses examined exercise counseling perception, prepregnancy exercise status, exercise information obtained by a source other than an obstetric provider, and demographics. A P value of <.05 was considered statistically significant.
This study was approved by the Prisma Health System Institutional Review Board for Human Subjects Protection (Pro00083011). Investigators also obtained a signed informed consent form from each participant prior to collecting data.
Results
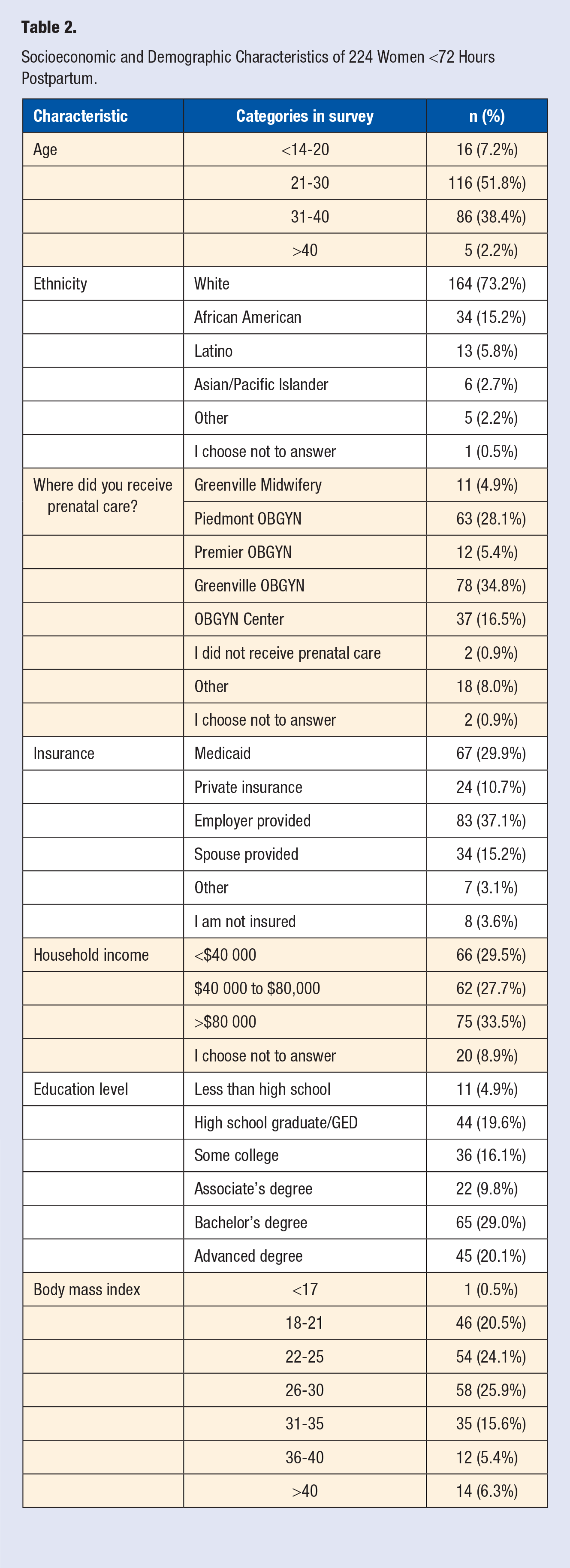
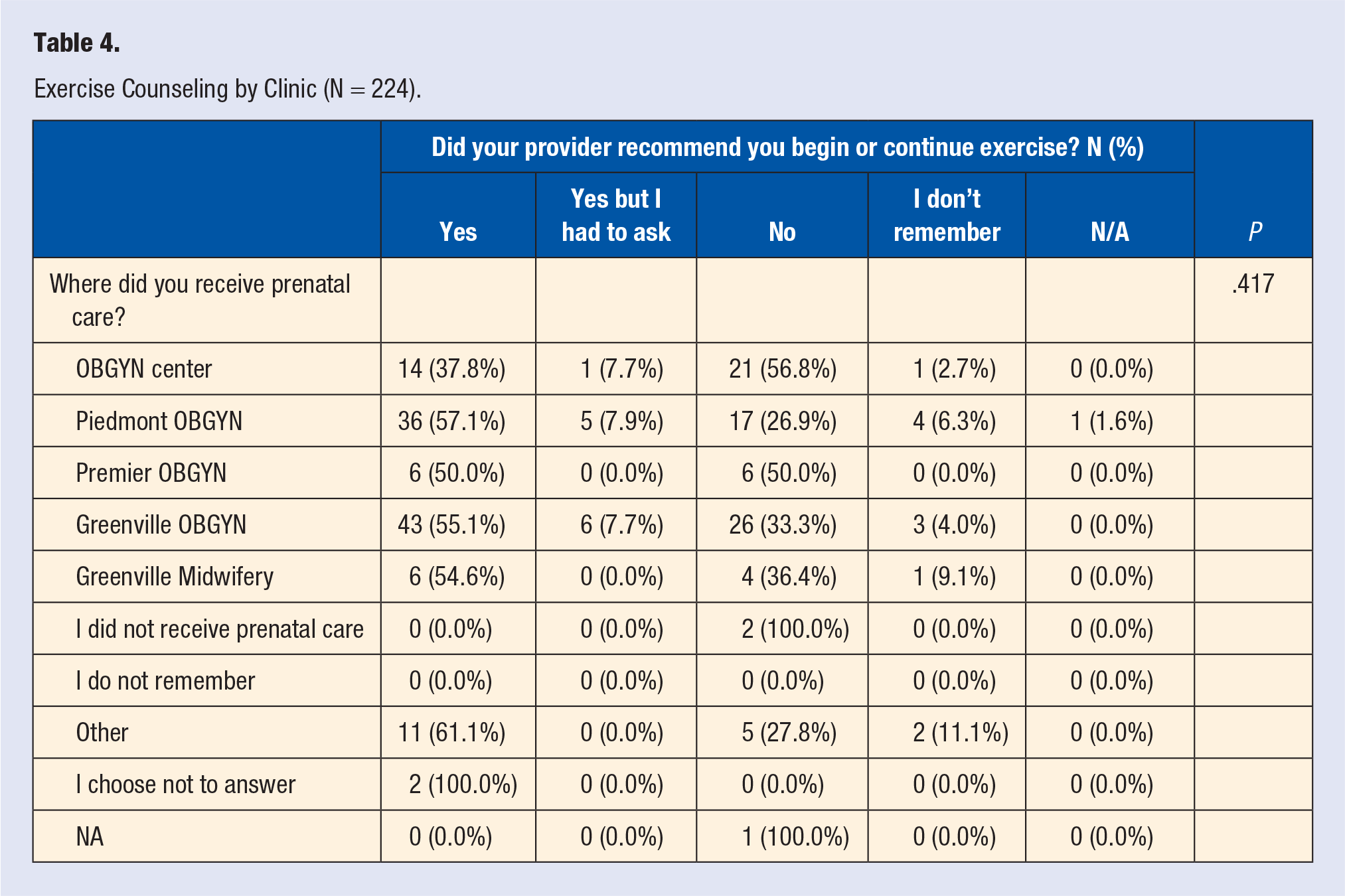
Two hundred and twenty-four women consented to complete the survey out of 227 requests (98.7% response rate). One person declined completed demographic questions but completed the exercise survey. Of the women surveyed, 164 (73.2%) were White, 141 (62.9%) were covered by private/employer/spouse insurance, and 110 (49.3%) had at least a 4-year college degree (Table 2). Of the 224 women who completed the exercise survey, 118 (52.7%) recalled that the obstetric provider recommended they begin or continue exercising, and 12 (5.4%) recalled that they received recommendations only after asking their health care provider, meaning 130 (58.0%) recalled receiving any exercise counselling (Figure 1). Eighty-two (36.6%) women reported that the provider “did not specify” and 11 (4.9%) did not remember, meaning 93 (41.5%) did not recall being counselled (Figure 1). Of the 130 women who perceived receiving specified counseling using components of FITT (Table 3), the majority (n = 102, 45.5%) of women reporting being counseled to walk, while 29 (12.9%) stated that the provider did not specify. The majority of women (n = 119, 53.1%) reported that the provider “did not specify” how many days per week to exercise, and 63 (28.1%) reported that the provider “did not specify” how long to exercise. No statistically significant differences were found for perceived recommendations by clinic (P = .417, Table 4).
Socioeconomic and Demographic Characteristics of 224 Women <72 Hours Postpartum.
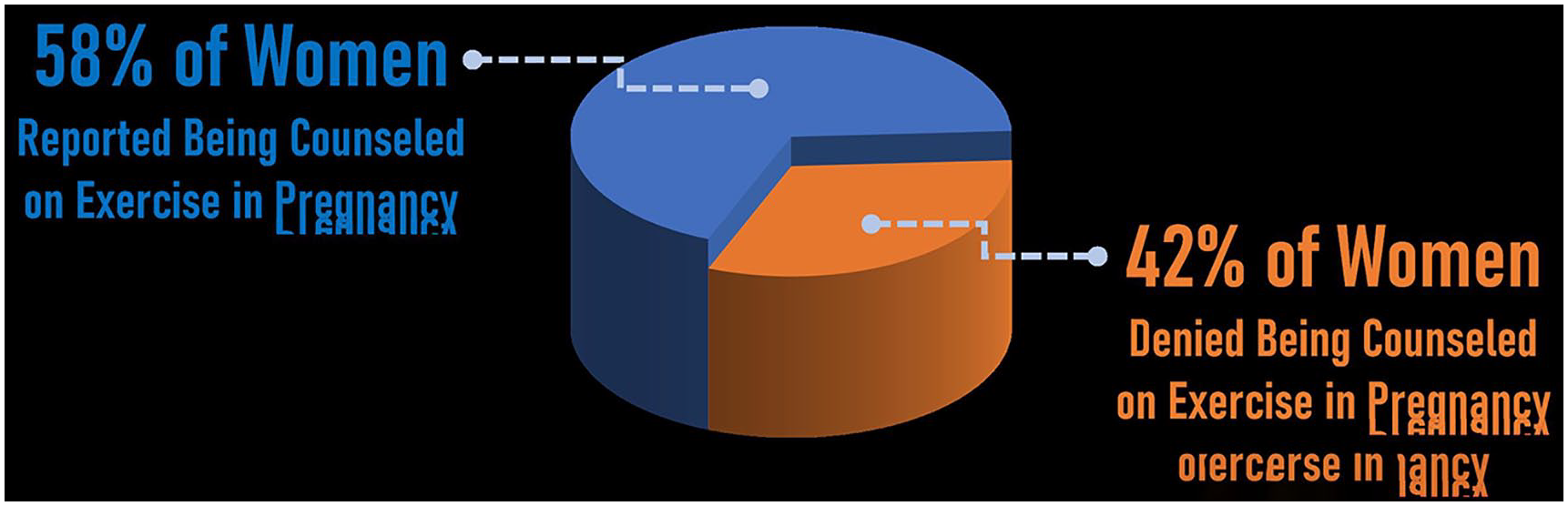
Percentage of women who perceived receiving exercise counseling during pregnancy versus those who did not.
Number (Percentage) of Women Whose Provider Recommended to Begin or Continue Exercise Using Components of FITT Principle.
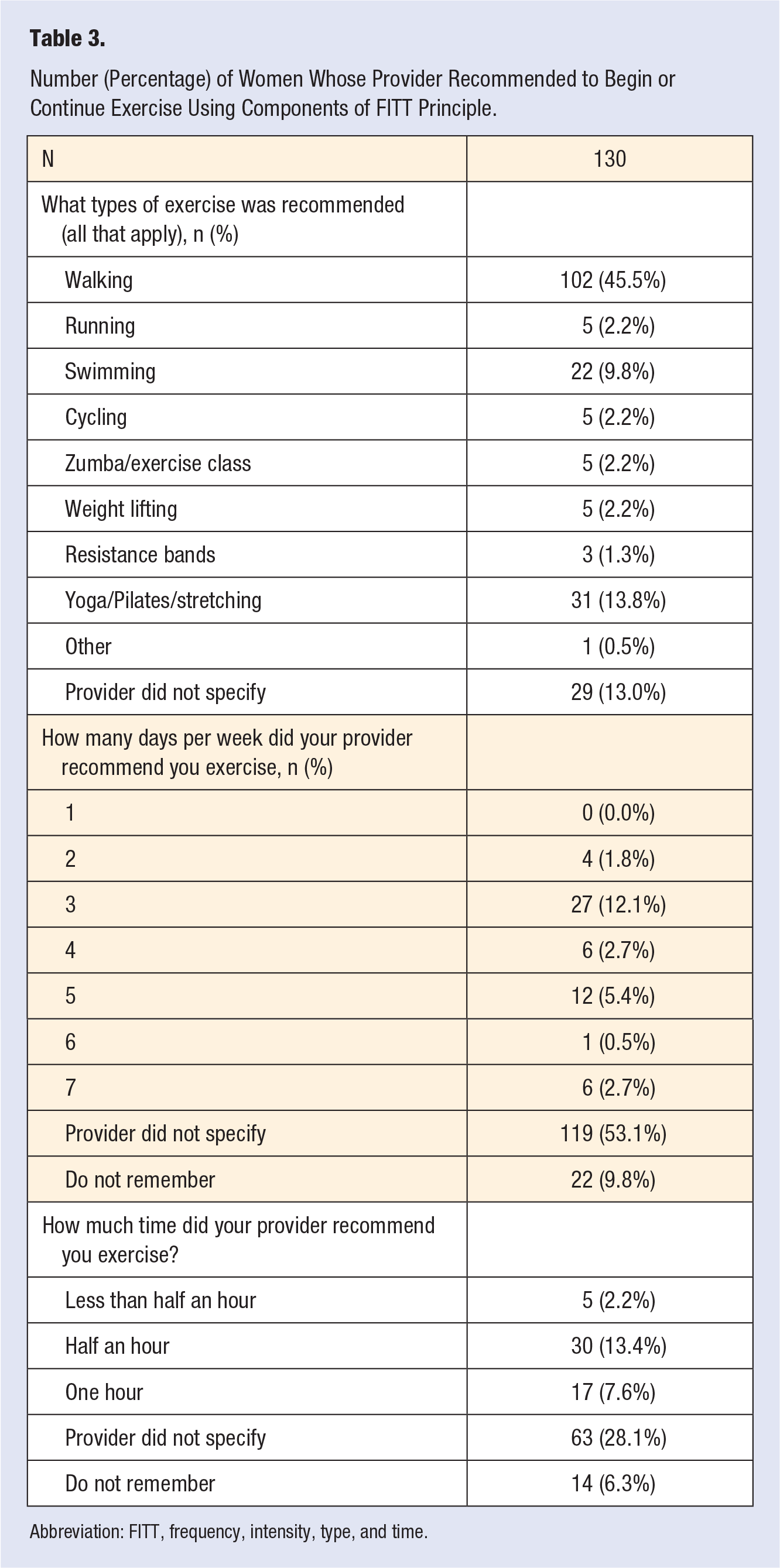
Abbreviation: FITT, frequency, intensity, type, and time.
Exercise Counseling by Clinic (N = 224).
One hundred sixty-five (73.7%) women reported exercising prior to becoming pregnant (Figure 2), with 138 (83.6%) reporting walking as their form of exercise, followed equally by running (n = 42, 25.5%) and yoga/Pilates/stretching (n = 42, 25.5%). However, of those who exercised prior to pregnancy, 64 (38.8%) reported that they did not continue to exercise while pregnant (Figure 2). Forty-eight (36.9%) women who were recommended to begin or continue exercise during pregnancy reported receiving no counseling on warning signs of when to stop exercise. For those who perceived being counseled on warning signs, the 5 most common warning signs counseled on were “feeling weak or dizzy” (n = 55, 67.1%), “difficulty breathing” (n = 53, 64.6%), “vaginal bleeding” (n = 44, 53.7%), “preterm labor” (n = 35, 42.7%), and “decreased fetal movement” (n = 32, 39.0%).
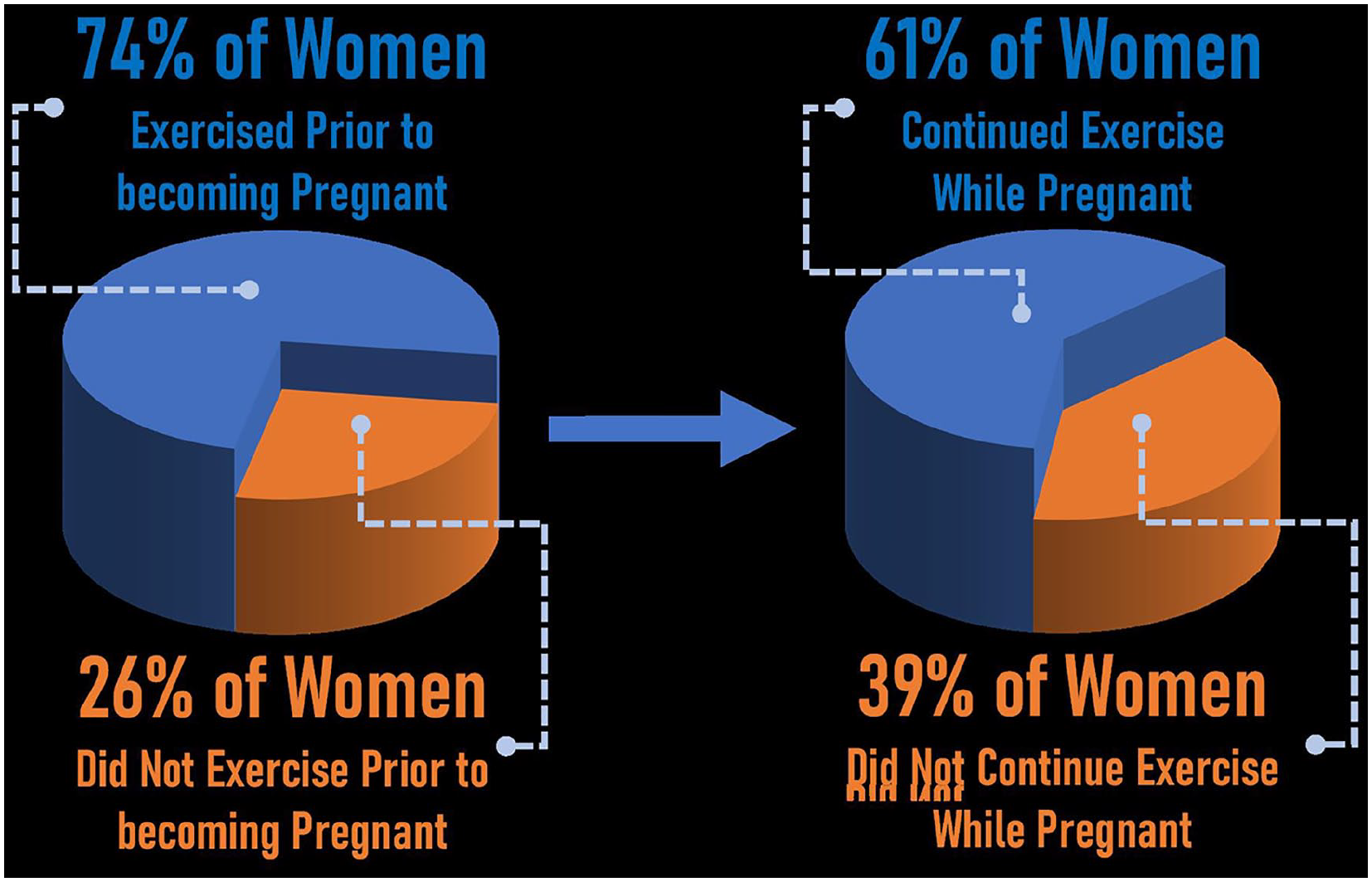
Percentage of women who exercised prior to pregnancy versus women who continued to exercise during pregnancy.
When asked if the person would have liked to receive information about exercise while pregnant, 90 (40.2%) stated “yes.” When asked if they received information about exercise while pregnant from a source other than a health care professional, 88 (39.3%) stated “yes.” Sixty-eight (77.3%) of those women reported receiving information from the internet, 32 (36.4%) reported receiving information from a friend, and 19 (21.6%) of women received information from a family member.
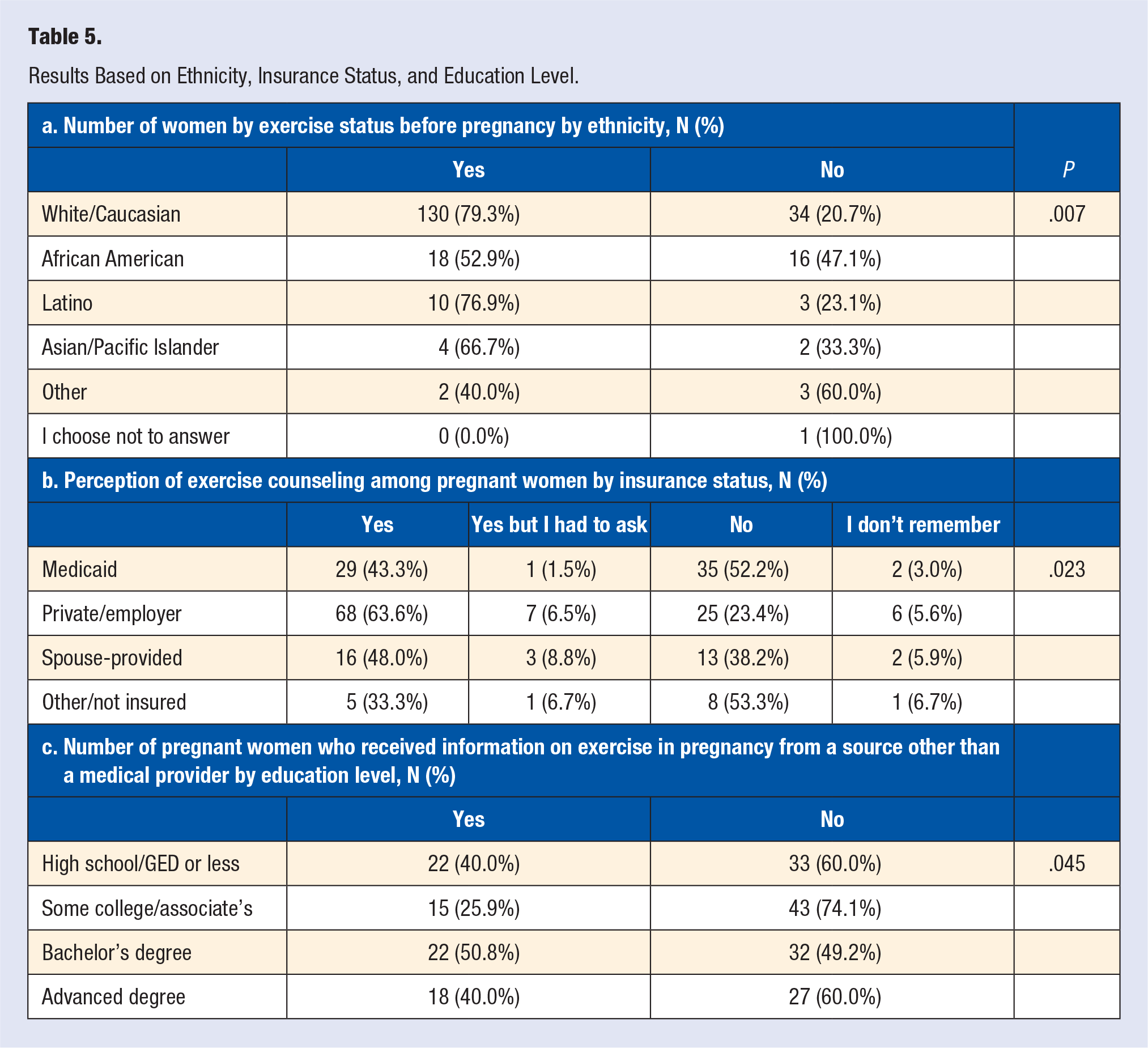
Statistically significant differences were found based on race/ethnicity, insurance status, and education level (Table 5). Women who reported exercising prior to becoming pregnant had statistically significant demographic differences (Table 5a, P = .007); however, there was no statistically significant difference between race/ethnicities with respect to the perceived receipt of recommendations to begin or continue exercise (P = .928). Regardless of ethnicity or race (P = .75), many women indicated a desire to have received information about exercise while pregnant: Whites = 63 (38.4%), African Americans = 15 (44.1%) Asian/Pacific Islander = 5 (83.3%), Latinx = 5 (38.5%), and Other = 1 (20.0%). A greater number of women also reported exercising prior to pregnancy if their annual household income was more than $40 000 compared to women whose annual household income was less than $40 000 (P = .006). More private/employer-insured women perceived receiving exercise counseling compared to other insurance types (P = .023, Table 5b). When asked if the individual had received information about exercise while pregnant from any source besides their obstetric health care provider, those with some college/associate’s degree received significantly less information from outside sources compared to other groups (P = .045, Table 5c).
Results Based on Ethnicity, Insurance Status, and Education Level.
Discussion
The study results suggest that a disproportionate number—nearly 50%—of pregnant women perceive that they either did not receive counseling on exercise in the prenatal period, or they received incomplete counseling if measured by the FITT principle. In addition, perception of receipt of counseling was insurance-type dependent. Many women looking for advice on exercising while pregnant reported receiving advice from non–health care professionals and sources. Compared to before the participants were pregnant, pregnant women in this study did not exercise as frequently. This is on par with the literature which demonstrates that less women exercise while pregnant, while many who exercised before conception cease to exercise afterwards.25,26 Finally, women traditionally identified as a demographic minority or at a socioeconomic disadvantage demonstrated a lower perception rate of exercise counseling during pregnancy, and therefore may be vulnerable. These novel multiple findings on the patient perception of obstetric provider level of exercise counseling add valuable insight to the literature on a patient’s “take home message,” suggesting a disconnect exists between the messaging and the receipt. In addition, these findings are clinically relevant given the CDC and ACOG exercise recommendations for reducing risk of maternal and fetal comorbidities 1 and that the prenatal period is a suggested time where women are more motivated to initiate positive lifestyle behavior changes.10,12 Since providers have significant access to this patient population for additional counseling, these results suggest that improving patient perception around exercise counseling in the prenatal period by obstetric health care providers could have lasting impact on the health and well-being of women and their children.
Previous studies demonstrate that prenatal patients are unsure about exercise recommendations received from obstetric health care providers, with some women reporting receiving incorrect guidance.17,27 Results from the current and previous studies align with McGee et al, who demonstrated that despite obstetric health care providers believing exercise benefits pregnant women, consistent counseling of pregnant women on exercise does not occur, and that advice on resistance training, maximum heart rate or exertion during exercise, and third-trimester exercise are often discordant with CDC and ACOG guidelines. 28 While these ACOG guidelines readily suggest further research is needed in the field to ascertain optimal exercise standards, they fully endorse a FITT prescription of 150 minutes per week of moderate intensity aerobic exercise per week throughout the pregnancy with the use of weights or resistance bands for 30 minutes at least twice per week. 4 ACOG also fully endorses continuation of high-intensity exercise practices in women who were well conditioned and trained prior to pregnancy. 4 Specific contraindications to exercise should be discussed by the provider and include vaginal bleeding, abdominal pain, dizziness or syncope, headache, painful contractions during exertion, prolonged muscle cramping, or development of fever. 4 ACOG does not have a recommended maximum heart rate due to physiologic cardiac output changes during pregnancy; they recommend moderate intensity be measured with the “talk test,” meaning if the patient can carry on a conversation, they are likely not over exerting themselves. 4 Therefore, if the patient meets any of the contraindications or fails the talk test, they should speak with their provider about ceasing exercise (if contraindicated) or adjusting their exercise prescription accordingly. 4 These current results stated above suggest that women who perceived receiving exercise recommendations did not receive a specific FITT prescription, and therefore are not properly educated on the recommendations and contraindications stated above. Possible reasons why women did not, in general, perceive receiving complete FITT counseling may include common barriers (similar to obesity counseling) cited by obstetric health care providers such as lack of time, referral services, and patient tools/information. 29 Additionally, most obstetric health care providers as well as primary care providers may not receive adequate training, educational resources, or even reimbursement codes to counsel patients.29,30 It is reasonable then to believe that this lack of training may extend to the FITT principle. Results from the current study may inform future studies as well as providers through offering education on the application of the FITT principle for exercise prescriptions as recommended by the American College of Sports Medicine and experts in prenatal health.18,19
While the authors found no statistically significant difference between ethnicities and races and perception of receiving exercise counseling, there was a significant difference between race/ethnicity regarding the number of women who participated in exercise prior to becoming pregnant. These results are consistent with other studies which demonstrate that racial and ethnic minorities, on average, exercise at lower rates. 31 However, over 80% of the racial/ethnic minority women surveyed stated that they would have liked to receive information about exercise while pregnant. Obstetric health care providers may be able to better support all patients by realizing the presence of numerous existing structural barriers to exercise among vulnerable populations. An integrative review of barriers to PA among African American women found many different barriers, including gender roles as the primary caregiver, cultural views of exercise as “selfish” or “self-indulgent,” lack of social support, lack of a partner with whom to exercise, lack of physically active role models, community safety concerns, lack of sidewalks, and lack of local facilities to engage in exercise. 32 In addition, an environment such as one’s neighborhood can either promote or deter PA. Neighborhood sidewalks or footpaths can increase recreational walking and cycling by creating smooth surfaces with less fall risk, can improve pedestrian walkability by separating sidewalks from roads, and can connect neighborhoods to facilitate community and positively impact social norms. 33 Personal safety measures can be further improved by adequate lighting and increased line of sight, which may not only allow for increased flexibility in the timing of leisure PA but may aid in reducing neighborhood crime. By being inclusive of all groups of pregnant women, understanding structural barriers, and helping provide equity in access to information and resources, obstetric health care providers may improve exercise counseling–based patient and infant outcomes.
The number of private/employer insured women who perceived being counseled versus not counseled was significantly different than the other groups. These results were unanticipated with regard to a difference between this group and the spouse-provided insured women, but not as compared to the Medicaid and other/not insured. While we lack previous study support to reflect on possible reasons for this insurance-based difference regarding perceived exercise counseling, we cautiously speculate that women with private/employer provided insurance may be at an advantage due to perhaps occupationally provided knowledge around benefits of PA through their work or occupation, or seek obstetric providers who understand similar associations. Supporting studies comparing similar socioeconomic status variables demonstrate that women of a lower socioeconomic status are more likely to have a Caesarean delivery, preeclampsia, preterm delivery, and obstetrical hemorrhage than those of a higher socioeconomic status. 34 Other studies support our findings as they found that patients who were uninsured or who had Medicaid insurance were counseled less often, 35 and that uninsured adults are less likely than adults with any kind of health coverage to receive preventive and screening services, concluding that health insurance that provides more extensive coverage of preventive and screening services is likely to result in greater and more appropriate use of these services. 36 While lack of health insurance presents a challenge regarding access to care, insurance status should not preclude established patients from receiving adequate counseling as increased PA may decrease rates of preeclampsia, Caesarean delivery, and preterm delivery.37,38 Therefore, results from this study may inform others on how to effectively target pregnant women specifically of low socioeconomic status for exercise-associated benefits, as this population is simultaneously at a higher obstetric risk and therefore may gain benefits from the increased exercise knowledge. 17 We also recommend further in-depth studies to learn more about this difference.
Several women surveyed in this study perceived receiving counseling and/or information from sources other than their obstetric health care providers such as the internet, a friend, or a family member. This suggests that a key opportunity may exist in the obstetrics field to actively provide women in-person, reliable, evidence-based information in messaging that is appropriate to the patient’s understanding, with special attention to cultural competency, socioeconomic status, and level of education to satisfy this information seeking behavior. Similarly, one pilot study (N = 7) reported that 30% of women who reported counseling stated that the advice from their provider changed their PA habits. 39 Another pilot study found that remote health coaching in pregnant women led to lower rates of excessive gestational weight gain, was financially feasible, and had high patient satisfaction. 40 A subsequent possible research opportunity based on the current findings would be to conduct an intervention study and provide a facilitated (ie, virtual or in-person) education intervention to the obstetric providers on knowledge and behavior change skills, and then determine if women increase understanding (ie, about the importance of exercise, how to implement the FITT principle in their daily lives, and how to overcome barriers) and subsequently increase rates of exercise participation.
One of the strengths of this study compared to the existing literature is the larger sample size (N = 224). This improves upon and validates previous studies showing gaps in communication regarding exercise between pregnant women and their health care providers, all of which had smaller sample sizes than this study.13,17,27,41 Another strength was that the data collection sites are 2 hospitals that serve a population estimated at 514 213. This was a strength because it allowed us to get a large sample size from a diverse population, but also the vast majority of the population in this cohort received care at 1 of the 5 largest OBGYN provider groups in this small region. Therefore, if one provider group was counselling on exercise at a higher rate, we could isolate their process and study it in further detail. However, we found no such difference in rate of exercise counselling per provider group, indicating all 5 major provider groups in the area that serve over 500 000 people are likely not adequately counselling on exercise in pregnancy and recognizing this as a systemic problem in this region. Finally, little is known with respect to rates of perceived FITT principle–based counseling among pregnant individuals. This is the first study to our knowledge that examined the specificity of exercise counseling perception in pregnant women based on the FITT principle. Similarly, some limitations exist in this study. One potential limitation is the racial demographic distribution of 73.5% White, 15.0% Black, 5.8% Latinx, 2.7% Asian/Pacific Islander, and 2.2% Other; however, the studied population demographics were consistent with the Greenville County 2018 report, which was 76.4% White, 18.5% Black or African American, and 5.1% Other, 20 as well as the estimated 2018 US demographic of 76.5% White, 13.4% Black or African American, and 10.1% Other. 42 While the perceived lack of racial or cultural heterogeneity can be seen as a limitation in many studies as it may not be representative of a larger group with unique cultural preferences on exercise, pregnancy, or health care in general, this study used a randomized sample of the existing population demographics which were on par with the local county population and very close with the demographics reported in the United States. A second potential limitation was that women’s reports of exercise prior to pregnancy may not be generalizable to other exercise behavior patterns in regions across the United States. Greenville, South Carolina, is considered to have a rate of 82.3% for “Access to Exercise Opportunities,” and “Physical Inactivity Rate” of 23.7%. 43 A third limitation is potential recall bias due to interviewing women in the immediate postpartum period (ie, within 48 hours) and asking them to recall exercise counselling throughout the entire pregnancy period. Many studies have shown patient recall, in multiple settings of health care, is not completely reliable.21,44 This lack of accurate recall is only further pronounced with longer time periods from the intervention, and is best ameliorated with repetition from the provider. 44 However, the advantage of this design was to reduce confounders such as various practice models and timelines established by different obstetric health care providers regarding prenatal exercise counseling. We also designed this study so if the provider was repeating this exercise counseling (per studies which state repetitive interventions improve recall), the total number of provider contacts would be maximized which would minimize recall bias as the provider would have maximum number of opportunities to reinforce exercise prescriptions. 44 Furthermore, by delivering the survey as close the provider contacts as possible (directly after the delivery as opposed to 3-week follow-up), our design minimized recall bias exacerbated by long time periods from the intervention prescription. 21 A fourth perceived limitation may be that providers were not cross-surveyed to determine if they believed they were providing exercise counseling; however, this was an intentional choice. The purpose of this study was to ascertain women’s perspectives, with a goal of informing further interventional research focused on patient-centered outcomes as well as disseminating this information to obstetric providers. If women are going to begin or continue exercise in pregnancy at the recommendation of their provider, they need to not only receive the intervention but be able to recall the specifics of the conversation. Thus, the relevance of this study is health care’s understanding of what patients perceived that they received regarding exercise counseling, not whether or not the providers are providing this information.
Conclusion
In conclusion, information from this study suggests that at approximately one-half of pregnant women do not perceive receiving counseling on exercise in the prenatal period; and if they are counseled, lack of specificity exists of how to safely exercise as well as heed warning signs to stop exercising. Women also perceive not always receiving appropriate information about exercise from their obstetric providers, even though they indicate a desire to receive it, and instead reach out to other sources such as family members, friends, and the internet, which may be inaccurate resources. Of utmost importance to consider, women identified as a minority demographic or at a socioeconomic disadvantage may be especially vulnerable with respect to preventative care counseling, as evidenced by lower rates of perceived exercise counseling among these groups. While there are likely multiple factors, including various social determinants of health, including structural barriers, and socioeconomic status that contribute, women would benefit from additional counseling efforts as well as more targeted messaging from an inclusive and equitable perspective. Although other preliminary interventions show positive results, further studies are needed to inform on the most effective style of counseling and communication between obstetric health care providers and patients in order for women to be able to translate information received into action for the health of mother and child during pregnancy.
Supplemental Material
sj-pdf-1-ajl-10.1177_1559827621991851 – Supplemental material for Exercise Counseling in Pregnancy: Do Women Perceive Receiving the Information They Need?
Supplemental material, sj-pdf-1-ajl-10.1177_1559827621991851 for Exercise Counseling in Pregnancy: Do Women Perceive Receiving the Information They Need? by Connor Evins, Jasmine Dennis, Karson Mostert, Shiv Patel, David Enyart, Kacey Eichelberger, Joseph Ewing, Xiyan Tan and Jennifer L. Trilk in American Journal of Lifestyle Medicine
Footnotes
Acknowledgements
We would like to thank Prisma Health in Greenville, South Carolina for allowing us to perform this study at their facility.
Authors’ Note
This study was presented in part at the American College of Lifestyle Medicine Conference in Orlando, Florida, from October 27 to 30, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Prisma Health System Institutional Review Board for Human Subjects Protection (Pro00083011).
Informed Consent
Investigators obtained a signed informed consent form from each participant prior to collecting data.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.