
Abstract
Chronic low back pain (cLBP) is common and has a tremendous economic impact. With the prevalence and incidence of low back pain (LBP) on the rise, individuals often seek alternative treatments. Yoga is a widely used complementary and alternative medicine treatment for LBP. However, its efficacy as an intervention for LBP has not been thoroughly investigated. Therefore the purpose of this study was to systematically review the current literature for randomized controlled trials that assess the outcomes of Yoga as an intervention for individuals with cLBP. An electronic database search was performed for studies related to the efficacy of yoga in treatment for cLBP. Studies included were randomized control trials, published in English, from a peer-reviewed journal that identified yoga as the primary treatment focus for LBP in at least one group and included participants with at least a 12-week (3-month) history of symptoms. Our search revealed 185 articles. Of these, 10 met the inclusion criteria. We concluded Yoga intervention appears to be an efficacious intervention in alleviating cLBP. Yoga was demonstrated to significantly improve quality of life and reduce disability, stress, depression, and medication usage associated with cLBP in 8 of the 10 analyzed trials when compared with usual care, self-care book, or exercises. However, more research is necessary before recommendations can be made.
‘Yoga, which uses a more holistic approach when compared with conventional methods, has been shown to decrease symptoms with chronic low back pain.’
Introduction
Estimates suggest that 84% of people may experience low back pain (LBP) at some point in their lifetime. 1 A primary reason individuals seek medical care is for LBP, which can be costly to treat and manage. 2 Risk factors for long-term LBP include age, depression, previous history of back pain, pain distal to the knee, and dissatisfaction with job. 3 Many common treatments for LBP have been found to be ineffective, 1 thus, individuals suffering from LBP are turning to alternative treatment methods, such as yoga.1,4-8
A systematic review evaluating the prevalence of LBP found the point prevalence, and 1-year prevalence were estimated to range from 1.0% to 58.1% and 0.8% to 82.5%, respectively. 9
Low back pain typically affects individuals between 30 and 50 years of age with the prevalence increasing through adulthood up to 65 years of age. 2 Men and women are affected equally by LBP, and the cause can usually be traced to a work-related disability in adults younger than 45 years. 1 The prevalence of LBP is typically lower in persons with higher levels of income and education. 10 According to Hoy et al, 9 the 1-year incidence of a first time LBP episode ranges between 6.3% and 15.4%, and the 1-year incidence of any LBP episode ranges between 1.5% and 36%. Additionally, the incidence of LBP is twice as high for individuals with previous history of LBP when compared with those who have no history of LBP. 11
The incidence and prevalence of LBP results in rising medical costs and workers’ compensation claims, making LBP the most costly work-related disability. 2 It typically takes 2 months for an individual to return to work following a sick leave due to LBP.2,11 Thus, LBP leads to missed work, less productive workers, and rising health care costs estimated to be in the billions of dollars. 3
Complementary and alternative medicines (CAM) have long been used by individuals to help treat or manage illnesses. CAM treatments used in the treatment of LBP include acupuncture, manual medicine, mind–body therapy, and yoga. 5 Yoga, which uses a more holistic approach when compared with conventional methods,12,13 has been shown to decrease symptoms with chronic low back pain (cLBP). 5 It is believed that recurrences of debilitating LBP are particularly high in individuals with cLBP. 11 The estimated range for recurrence at 1 year is 24% to 80%. 9
There are 8 components of yoga on which the majority of styles are based: These are as follows (Sanskrit name with English translation in parentheses): yamas (moral restraints), niyamas (moral observations), asana (posture), pranayama (controlled breathing), pratyahara (sensory withdrawal), dharana (concentration), dhyana (meditation), and samadhi (self-actualization). 14
Styles practiced today and analyzed in research studies include hatha, Iyengar, Viniyoga, and integrated and specialized yoga. Hatha yoga is a branch of yoga from which many styles are rooted 15 and mainly focuses on asanas (postures), pranayama (breathing), and dhyana (meditation). Hatha yoga has been used by various studies because of its accessibility, popularity, and low intensity, making it appropriate for patients with cLBP. A pilot study by Galantino et al 16 found a 6-week intervention of hatha yoga to be effective in improving function in individuals with cLBP. This was further supported by another pilot study by Saper et al 17 who also found improved function and less pain medication use in individuals with LBP. Furthermore, a randomized trial by Tilbrook et al 18 found a 12-week yoga intervention program yielded improved function from 3 months to 12 months after completing a program. Iyengar yoga, which mainly focuses on asanas and the sequencing of asanas, is the most widely practiced style in the United States.4,15 Similar to outcomes of Hatha yoga, previously cited trials by Williams et al4,19 found that yoga interventions using the Iyenar approach were effective in reducing pain, disability, and medication use. Viniyoga is a therapeutic style that emphasizes postures and breathing with focus on relaxation, strength, flexibility, lateral bending, and asymmetric poses. 6 Sherman et al6,20 used this style in studies because of its ease on nonexperienced yoga participants. A trial by Cox et al 21 used a yoga intervention similar to the one used by Sherman et al 6 created by an Iyengar yoga instructor focusing on poses, movement, and simple breathing awareness. Finally, studies by Tekur et al8,22 used a specific module of an integrated approach to yoga therapy consisting of asanas, pranayamas, dhyana, didactics, and sessions about yoga’s philosophical concepts.
A recently published systematic review regarding yoga’s effectiveness as a treatment for cLBP concluded that although it has the potential to alleviate LBP a definitive claim about yoga’s effectiveness should be treated with caution. 23 Distinctions between the 2 reviews arise in the method of quality assessment (Jadad vs PEDro). Also, the present review includes recently published randomized controlled trials from Sherman et al 20 and Tilbrook et al. 18
Methods
Data Sources and Searches
An electronic database search was performed on SPORTDiscus, (1975 to December 2011), MEDLINE (1950 to December 2011), CINAHL (1981 to December 2011), AMED (1985 to December 2011), and PEDro (1929 to December 2011). The following key words were used independently and in combination: yoga and low back pain. One reviewer (AD) examined all titles and abstracts to determine initial study eligibility. Full-text articles were then reviewed to evaluate specific inclusion criteria. A second reviewer (WJH) independently reviewed all full-text articles for eligibility. A third reviewer (MJK) determined final eligibility if there was a discrepancy between the initial reviewers.
Study Selections
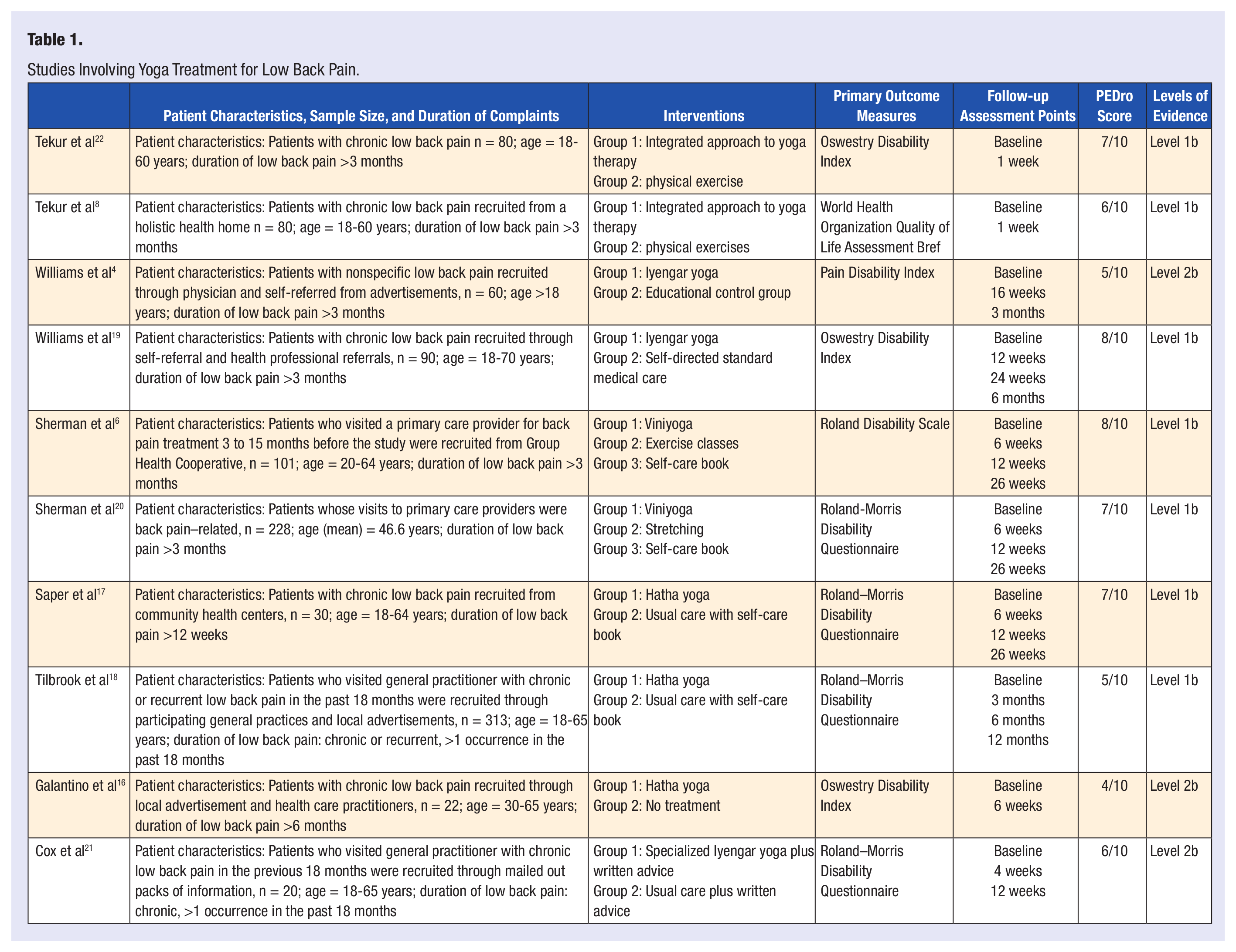
The inclusion criteria for studies in this review consist of the following requirements: a randomized controlled trial, published in the English language, published in a peer-reviewed journal, identified yoga as the primary treatment focus for LBP in at least one group, and included participants with at least a 12-week history of LBP. Also, a valid outcome measure such as pain or disability must have been used in the studies to be included in the review (Table 1).
Studies Involving Yoga Treatment for Low Back Pain.
Quality Assessment
The PEDro scale was used to assess the quality of trials selected. The scale is determined by counting the number of criterion present from 10 possible scale items. Internal validity was assessed through random allocation, concealment of allocation, if groups were similar at baseline, blinding of subjects, blinding of therapists, blinding of assessors, more than 85% follow-up for at least one outcome, and analysis by intention to treat. Interpretability is assessed through the reported between-group statistical comparisons and point measures and measures of variability for at least one outcome. An item on the PEDro scale not used in the method of scoring is eligibility criteria, as it relates to external validity (www.pedro.org.au). de Morton 24 found the PEDro scale to be a valid measure for assessing the methodological quality of clinical trials. The reliability of the total PEDro score is acceptable; however, individual scaled items varied from fair to substantial or from moderate to substantial. 25 The levels of evidence assigned to the randomized controlled trials was either a level 1b, with ≥80% follow-up or level 2b, with <80% follow-up.
Results
Study Selection
A total of 185 articles were retrieved from the electronic databases. Of the 185 articles, based on the title, abstract, and inclusion criteria, 10 full-text articles were included in this review as outlined in the PRISMA flow diagram (Figure 1). 26
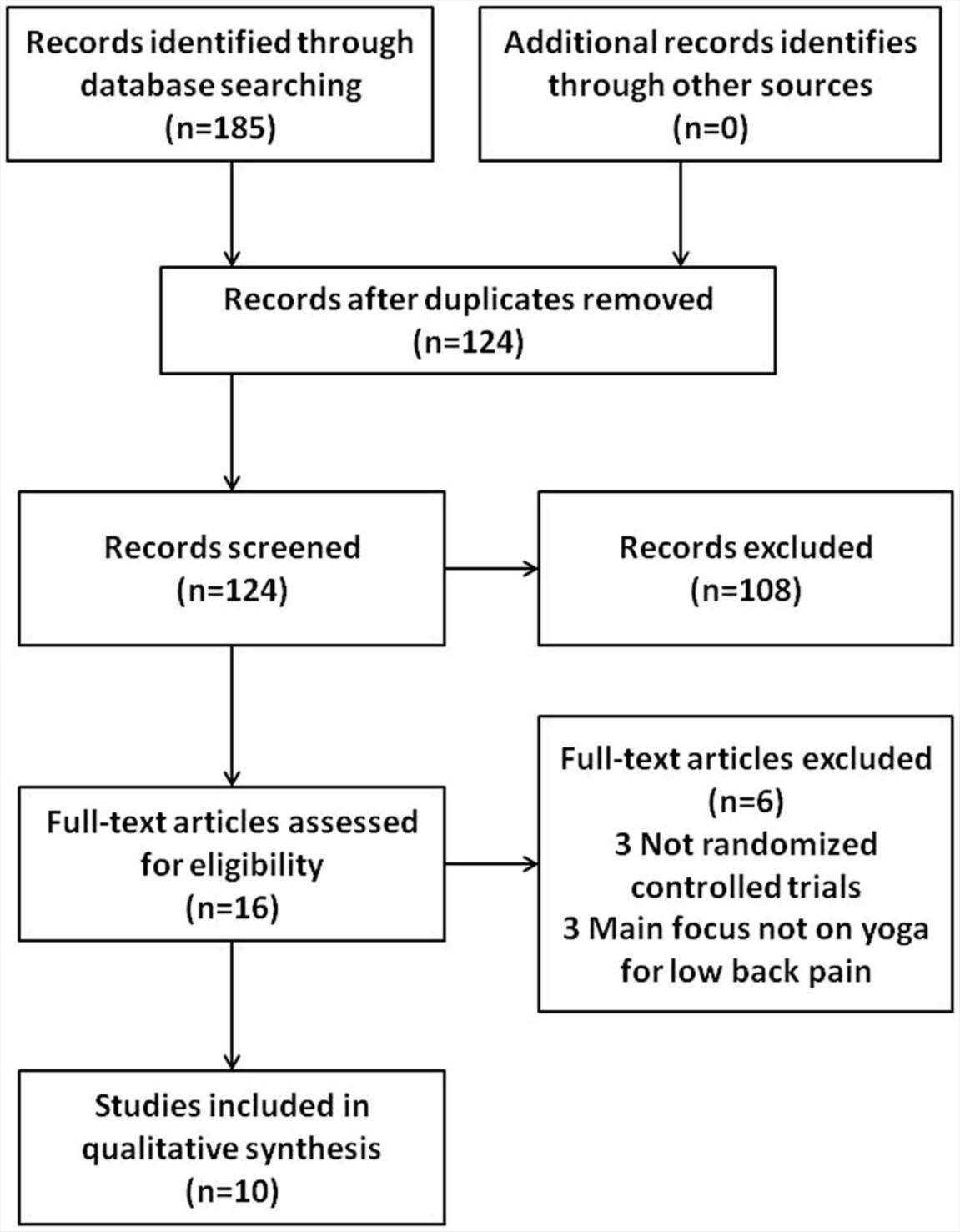
Search strategy for selected articles.
Methodological Quality
The mean score of the PEDro scale, used to assess the methodological quality of the trials, was 6.3 with a range of 4 to 8 out of 10. Subject and therapist blinding was not possible for any of the randomized controlled trials considering the yoga-based intervention. All the studies used random allocation and evaluation of between-group statistical comparisons. Galantino et al, 16 Williams et al, 4 and Tilbrook et al 18 did not have concealed allocation. Galantino et al 16 did not have baseline comparability, where at least one outcome measure and measure of severity described at baseline is needed. Galantino et al, 16 Saper et al, 17 Tekur et al, 8 Sherman et al, 20 and Cox et al 21 did not have blind assessors. Williams et al, 4 Tekur et al,8,22 and Tilbrook et al 18 did not analyze outcomes by intention to treat. Galantino et al, 16 Williams et al, 4 and Cox et al 21 did not have adequate follow-up, where the PEDro scale requires more than 85% follow-up for point allocation. Galantino et al 16 reported a 72% follow-up at the 6-week point, Williams et al 4 reported a 70% follow-up at the 3-month point, and Cox et al 21 reported a 78% follow-up at the 12-week point. The levels of evidence for the clinical trials are listed in Table 1.
Study Characteristics
Yoga Versus Physical Exercises
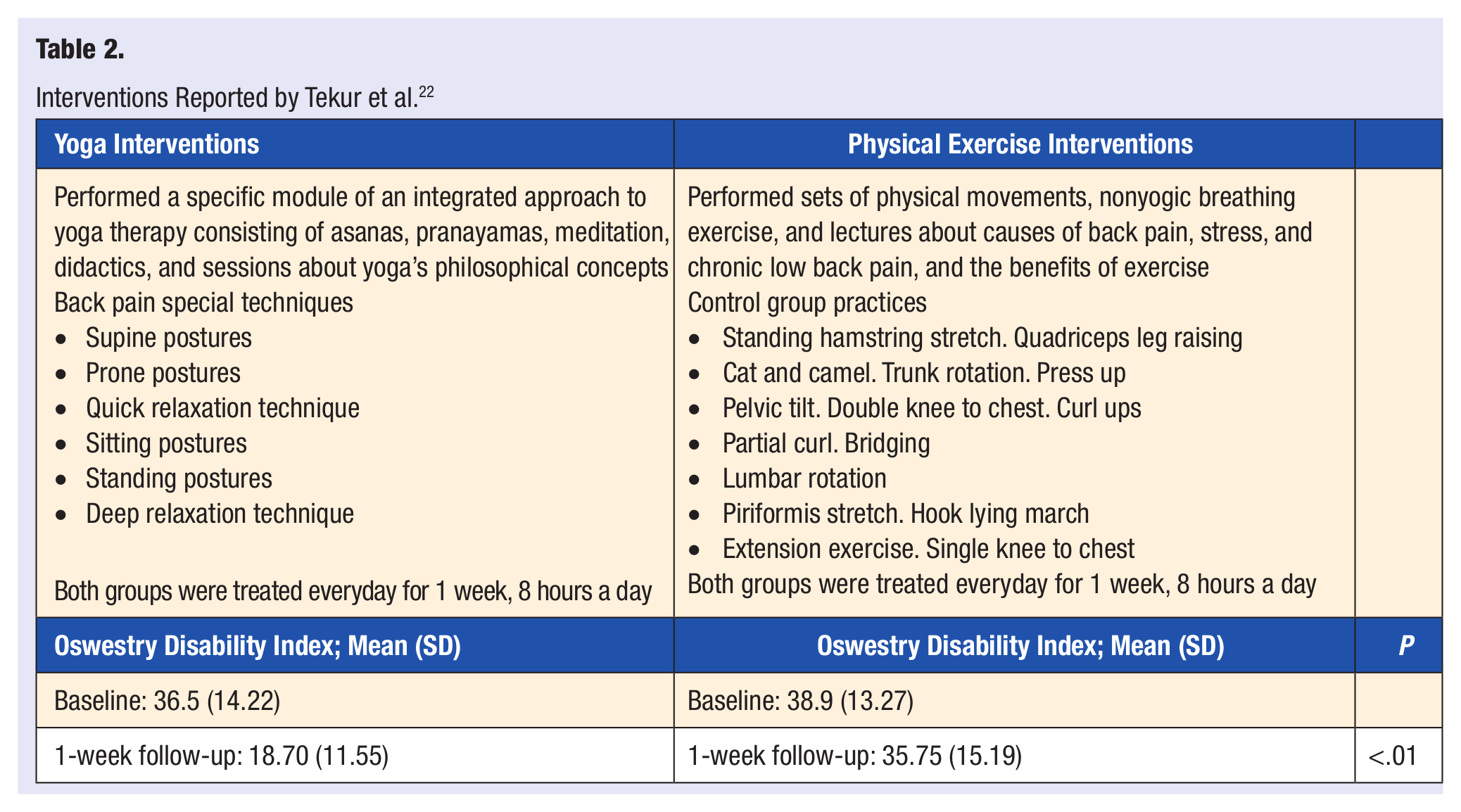
Tekur et al8,22 randomized 80 subjects with cLBP into an “integrated approach to yoga” therapy group or a physical exercise group. Treatment was 1-week long, consisting of a daily 8-hour schedule. The yoga group’s daily routine consisted of meditation, yogic hymns, lectures on yogic lifestyle, pranayama, deep relaxation technique, cyclic meditation, counseling, mind sound resonance technique, and yoga-based special techniques consisting of yoga postures to relax, stretch, and strengthen. The control group completed physical movements, nonyogic breathing exercises, and lectures on causes of back pain, stress, and cLBP, and the benefits of exercise. There was a 100% compliance rate for both groups with no adverse effects.
The primary outcome measure used by Tekur et al 22 was the Oswestry Disability Index (ODI), which is a measure of perceived disability due to LBP. There was a significant difference within groups (P < .001) in the yoga group. However, there was no significant reduction in ODI scores in the control group (P = .19). Spinal mobility was also measured with an increase in flexion and extension in both groups with a significant difference between groups, yoga having the higher improvements (P = .008 and P = .001, respectively). This study concluded that 1 week of a residential intensive yoga-based lifestyle program is more effective in reducing pain-related disability and improving spinal flexibility in patients with cLBP when compared with a physical exercise program (Table 2).
Interventions Reported by Tekur et al. 22
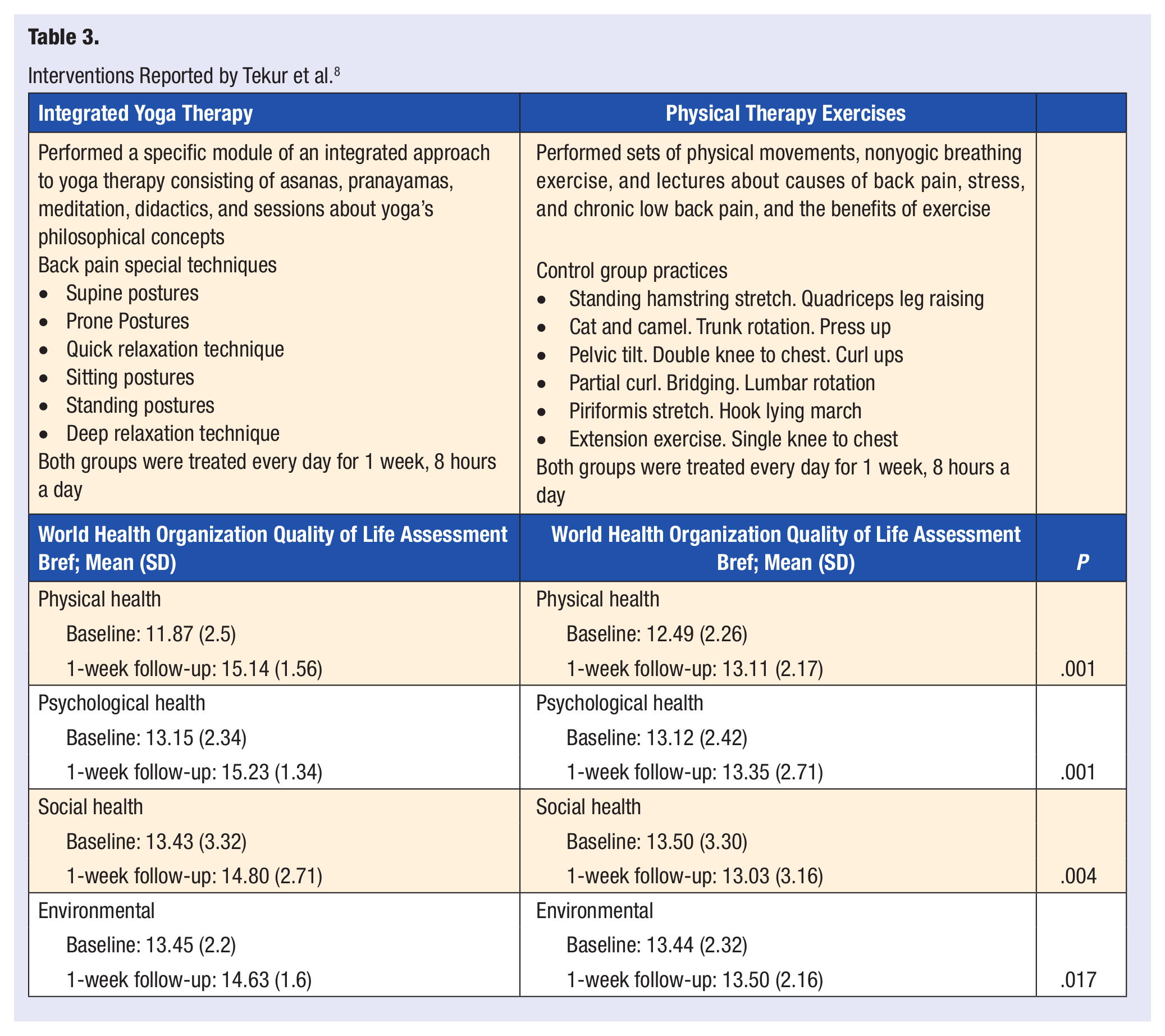
The primary outcome measure used in another study by Tekur et al 8 was the World Health Organization Quality of Life Assessment Bref. This study found a significant difference (P < .01) between groups on all domains (physical, psychological, social, environmental) and significant improvement in quality of life (P < .01) in the yoga group compared with the exercise group. Stress was also assessed through the perceived stress scale. Relating these 2 outcomes, this study found a negative correlation between the perceived stress and quality of life as measured in each of the World Health Organization Quality of Life domains: physical r = 0.31 (P = .005), psychological r = 0.48 (P < .001), social r = 0.46 (P < .001), and environmental r = 0.39 (P < .001; Table 3).
Interventions Reported by Tekur et al. 8
Iyengar Yoga Versus Educational Group
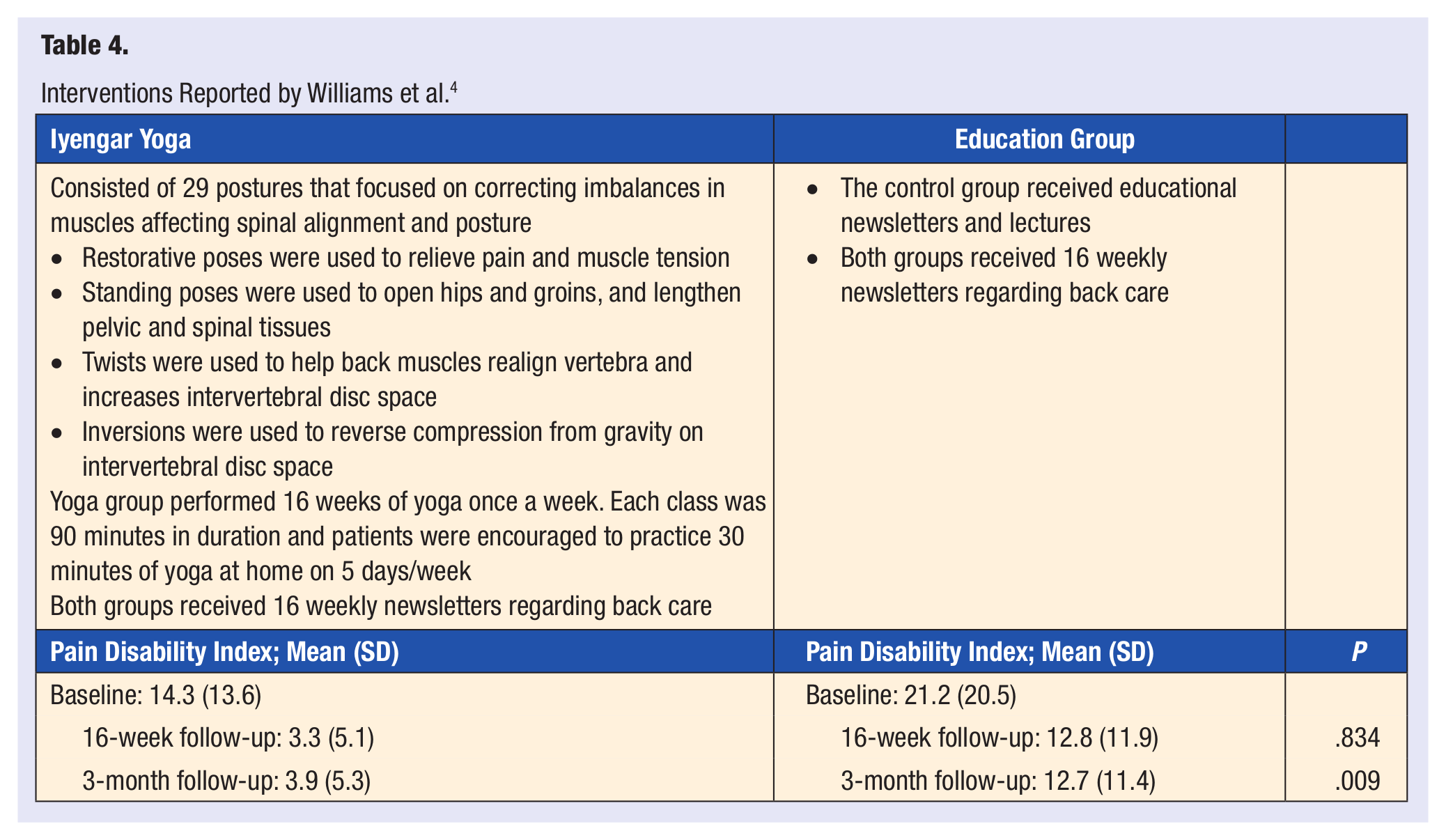
Williams et al 4 studied the effects of Iyengar yoga on patients with nonspecific cLBP by comparing the outcomes of a group receiving Iyengar yoga intervention with an educational control group. Sixty subjects were randomized into one of the programs for 16 weeks: 30 received yoga intervention and 30 served as the control group. A follow-up was conducted in 20 subjects from the yoga group and 22 from the control group, resulting in a 70% completion rate. Of the 10 subjects from the yoga group who were excluded, one subject was diagnosed with a herniated disc during the study, which was determined to be unrelated to the yoga postures performed. Both groups received 16 weekly newsletters regarding back care written by physical therapy students. Before beginning the program, both groups attended two 1-hour lectures of occupational/physical therapy education about cLBP. The yoga group attended a 1.5-hour class once a week and was encouraged to practice yoga at home 5 days a week for half an hour. Sessions consisted of 29 postures that focused on correcting imbalances in muscles affecting spinal alignment and posture. The primary outcome assessed was functional disability measured by the Pain Disability Index. Directly after the intervention, the yoga group had a significantly lower functional disability when compared with the control group (P = .005). At a 3-month follow up, the yoga group was found to have a significant improvement in functional disability (P = .009). The study concluded that the yoga group demonstrated a significant reduction in self-reported disability (77%), pain intensity (64%), decreased use of pain medication (88%), and longer lasting results than the educational intervention group (Table 4).
Interventions Reported by Williams et al. 4
Iyengar Yoga Versus Self-Directed Standard Medical Care
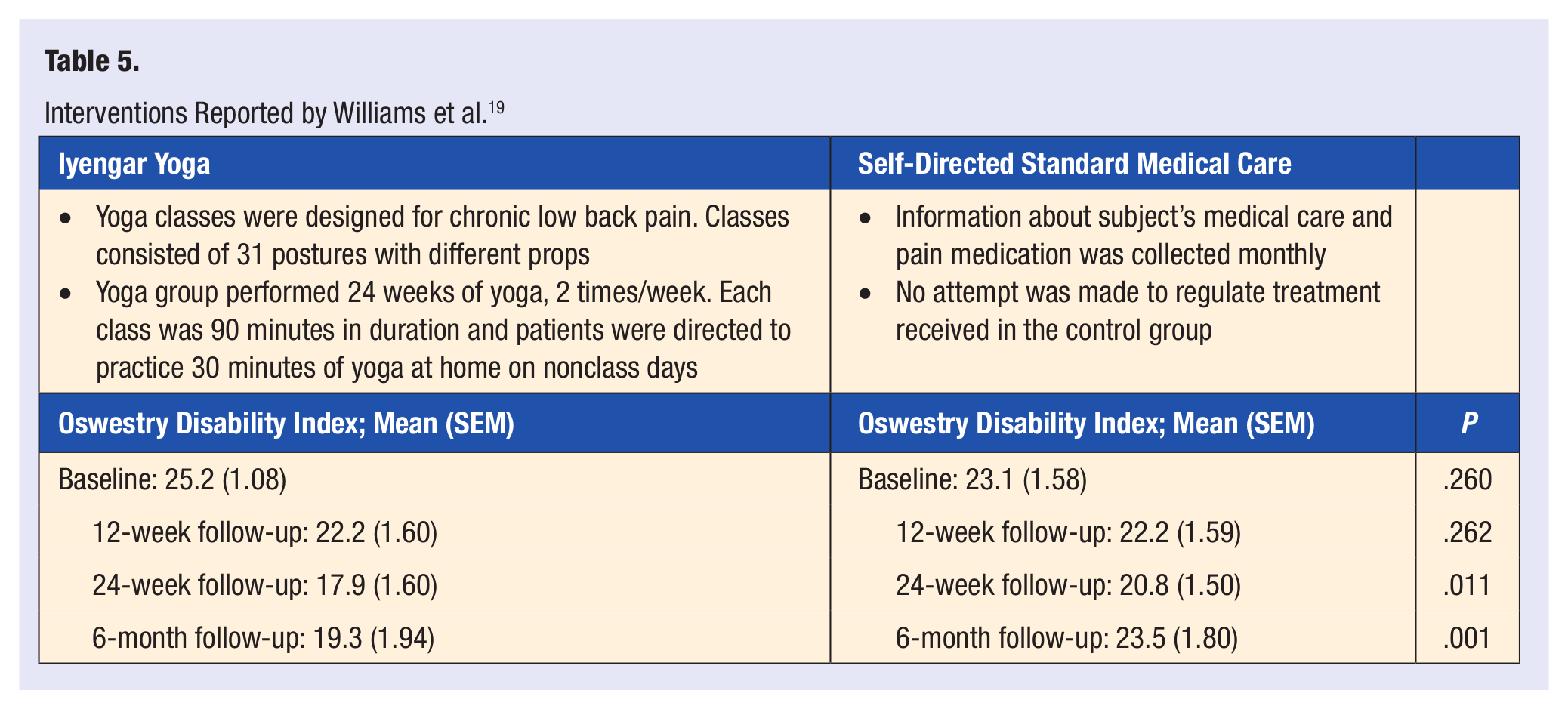
To evaluate the effectiveness and efficacy of Iyengar yoga for cLBP, Williams et al 19 randomized 90 subjects to either a yoga group (n = 43) or a control group (n = 47) consisting of standard medical care. The yoga participants attended yoga twice a week for 24 weeks with each session lasting 90 minutes. Classes consisted of 31 postures with different props, and patients were directed to practice 30 minutes of yoga at home on nonclass days. A significant reduction in functional disability, assessed using the Oswestry Disability Questionnaire, pain intensity, using the Visual Analog Scale, and medication usage was observed in the yoga group compared with the standard medical care group. Improvements in functional disability were 11.9% at a 12-week follow up and 29.0% at a 24-week follow-up for the yoga group. Depression, using the Beck Depression Inventory, was significantly lower in the yoga group. There was an 82% retention rate of participants in the yoga intervention. Attempts to regulate treatments in the control group were not reported. The results of the study suggest that yoga improves functional disability, pain intensity, and depression in adults with cLBP (Table 5).
Interventions Reported by Williams et al. 19
Viniyoga Versus Exercise Versus Self-Care Book
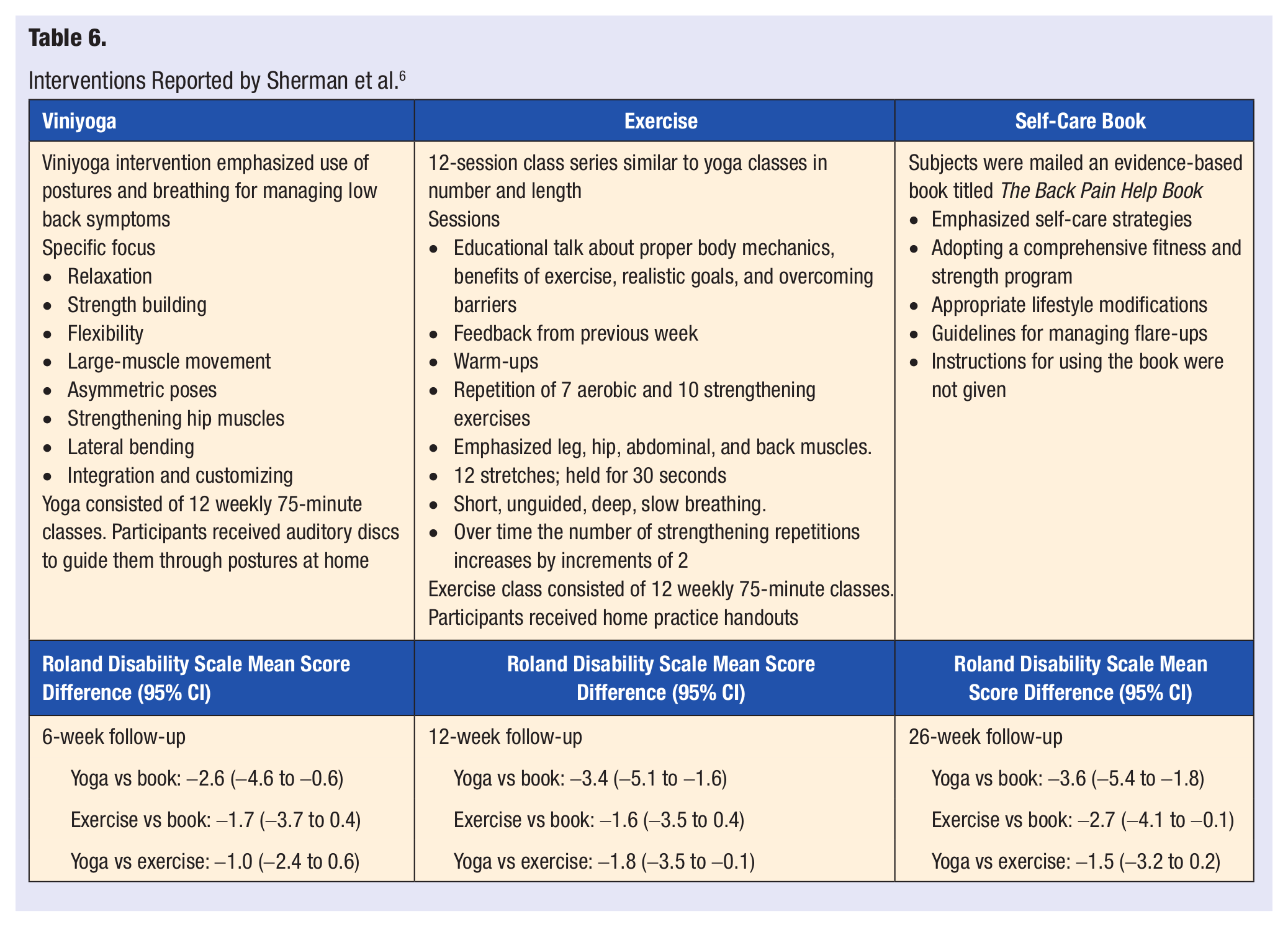
In the randomized control trial conducted by Sherman et al, 6 101 adults with cLBP participated in 12 weeks of either a Viniyoga class (n = 36), exercise class (n = 35), or a self-care book (n = 30). The participants in the yoga and exercise group attended 12 weekly, 75-minute classes. Viniyoga emphasized use of postures and breathing for managing low back symptoms with focus on relaxation, strength, flexibility, asymmetric poses, and bending. The exercise intervention consisted of an educational session, warm-ups, aerobic exercise, and strengthening exercises that focused on the hip, leg, abdominal, and back muscles. The group randomized to the self-care book group, received an evidence-based book that focused on self-care strategies such as fitness and strength programs, lifestyle modifications, and management of back pain. Outcomes were assessed through a modified 24-point Roland Disability Scale and an 11-point pain scale. The yoga group, when compared with the self-care book group, showed clinically important and statistically significant improvements in functional status at each of the follow-ups. There was significantly greater improvement in Roland scores for the yoga group than the exercise group at 12 weeks. In the yoga group, 69% reduced their Roland score to at least 50% compared with 50% from the exercise group and 30% from the self-care book group. Medication used to manage LBP after the 26 weeks decreased the most with yoga participants, and yoga was better than exercise for reducing pain at the 26-week mark. Class attendance in the yoga group was similar to the exercise group, and more than 75% reported in their compliance logs that they practiced for an average of 3 or more days a week. There were no serious adverse events reported. At 26 weeks, outcomes for yoga and exercise were both deemed statistically and clinically significant. The authors concluded that yoga and exercise was more effective than a self-care book for improving function and reducing cLBP (Table 6).
Interventions Reported by Sherman et al. 6
Viniyoga Versus Stretching Versus Self-Care Book
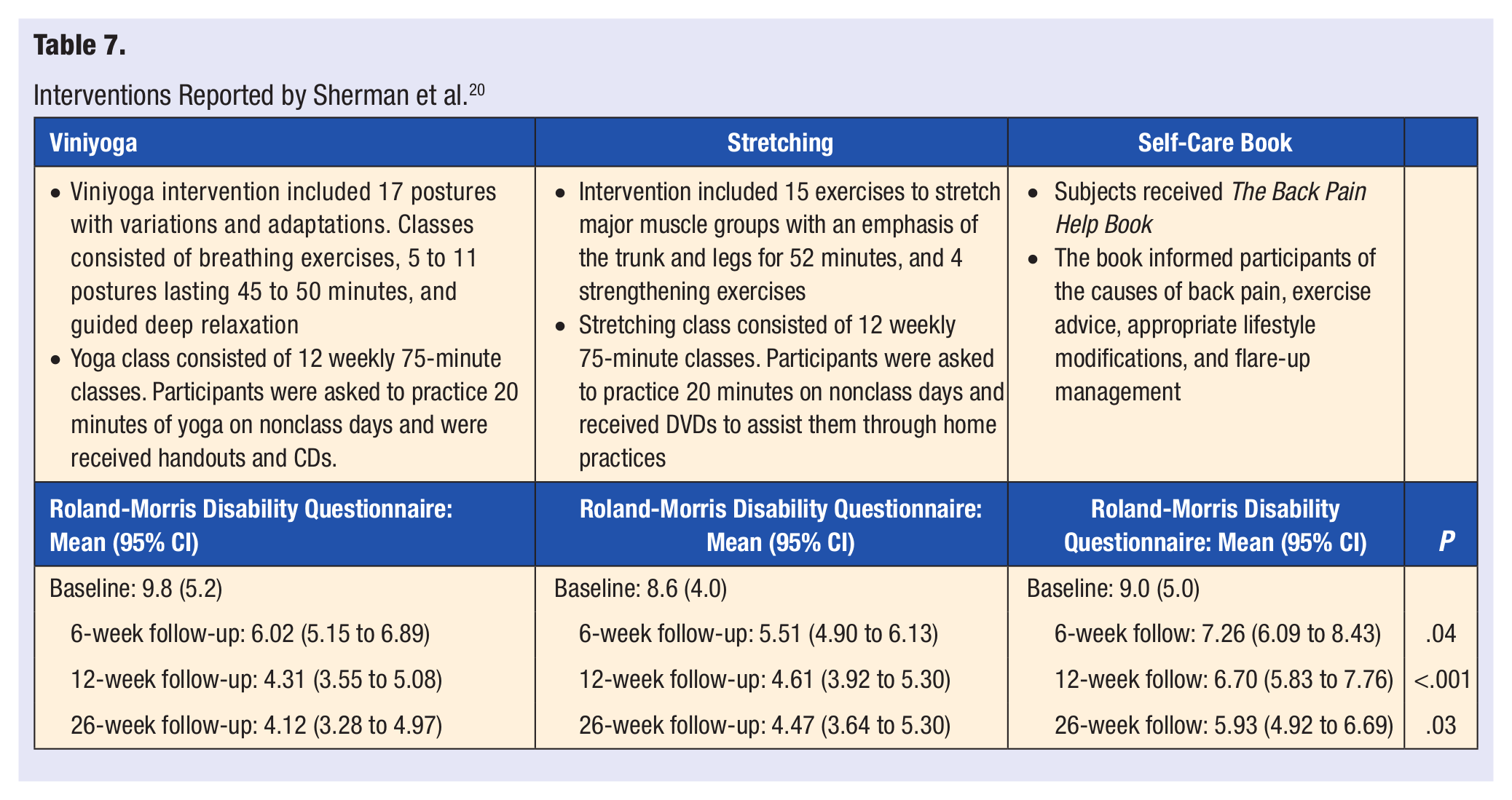
Sherman et al 20 randomized 228 adults with cLBP to 12 weeks of Viniyoga (n = 92), conventional stretching exercises (n = 91), or a self-care book (n = 45). The participants in the yoga and stretching group attended 12 weekly, 75-minute classes. Viniyoga intervention included 17 postures with variations and adaptations. Classes consisted of breathing exercises, 5 to 11 postures lasting 45 to 50 minutes, and guided deep relaxation. Stretching intervention included 15 exercises to stretch major muscle groups with an emphasis of the trunk and legs for 52 minutes, and 4 strengthening exercises. Participants of both groups were asked to practice 20 minutes on nonclass days and received either a DVD (stretching) or a CD (yoga) to assist them through home practices. Of the 228 subjects, 90%, 88%, and 100% were included in the 26-week follow-up analysis of the yoga, stretching, and self-care book groups, respectively. Attendance of at least one class was higher for yoga (95%) compared with stretching (82%), and attendance of at least 3 of the first 6 classes and 3 of the last 6 classes for yoga (67%) and stretching (66%) were similar. The reported home practicing of yoga and stretching for at least 3 days in the previous week of the 26-week follow-up was 59% and 40%, within each respective group. Twenty-eight subjects reported adverse events: 1 subject from the self-care book group reported increased pain after performing recommended exercises, 1 subject from the yoga group herniated a disc, and 13 subjects from the yoga and 13 from the stretching group reported increased back pain. Compared with baseline, medication use in the yoga and stretching groups were reported to be one fourth to one third less. Back-related functional status was assessed using the modified 23-point Roland–Morris Disability Questionnaire. The study reports that the Roland–Morris Disability Questionnaire score declined over the weeks in all groups, where there was a significant difference in adjusted values in the 3 groups. There were no statistically or clinically significant differences between yoga and stretching groups; 6 weeks (95% confidence interval [CI] = −0.57 to 1.58), 12 weeks (95% CI = −1.33 to 0.74), 26 weeks (95% CI = −1.52 to 0.83). The yoga and stretching participants were significantly more likely to rate their back pain as better, much better, or completely gone at all follow-ups when compared to the self-care book participants (Table 7).
Interventions Reported by Sherman et al. 20
Hatha Yoga Versus Usual Care With Self-Care Book
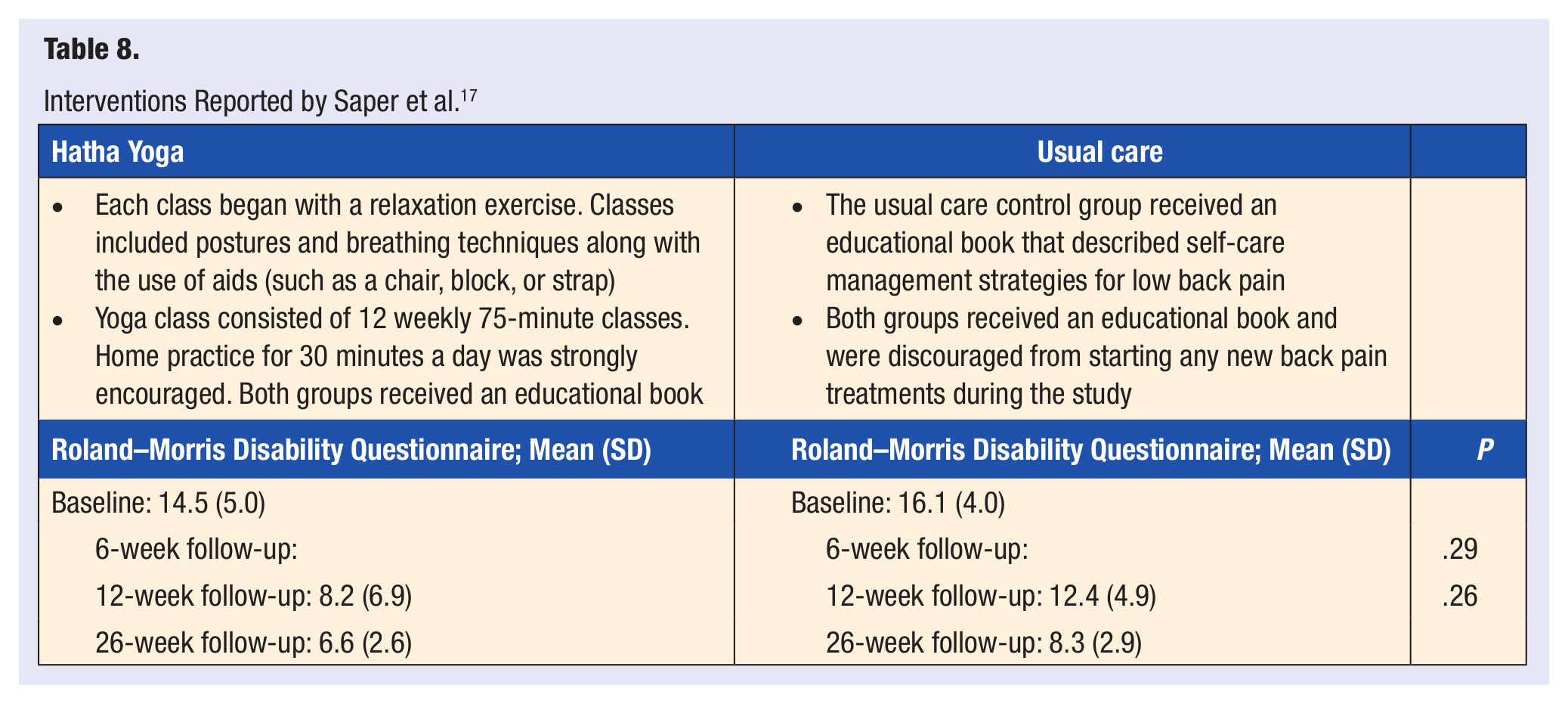
Saper et al 17 randomized 30 subjects with nonspecific cLBP into 2 groups: 15 allocated to yoga and 15 to a usual care group. There were weekly Hatha yoga classes lasting for 12 weeks, with each session lasting 75 minutes. The hatha yoga intervention was developed for subjects with little to no yoga experience. Each class began with a relaxation exercise and was given a theme, such as “Listening to the Wisdom of the Body,” with segments built on previous ones. The protocol provided aids, such as a chair, block, or strap, to accommodate different abilities. The usual care group received an educational book that described self-care management strategies for LBP. Both groups continued to receive routine medical care, medication, and a self-care book; and during the intervention they were discouraged from beginning any new back pain treatments. One adverse event was reported in a yoga participant whose LBP became worse and improved after discontinuing treatment. Subject retention was 97% at 12 weeks and 77% at 26 weeks. No statistically significant difference between the groups was identified at baseline. The Roland–Morris Disability Questionnaire was the primary outcome measure. It found that the mean scores decreased from baseline to 12 weeks by 6.3 points (SD = 6.9) in the yoga group and by 3.7 points (SD = 4.9, P = .28) in the usual care group. The mean pain scores decreased from baseline to 12 weeks by 2.3 points (SD = 2.1) in the yoga group and by 0.4 points (SD = 1.8, P = .02) in the usual care group. Pain medicine usage by the yoga group decreased from 67% to 13% whereas no change was noted in the control group (P = .003). The pilot study suggests yoga may be more effective than usual care for reducing pain and medication use in those with cLBP (Table 8).
Interventions Reported by Saper et al. 17
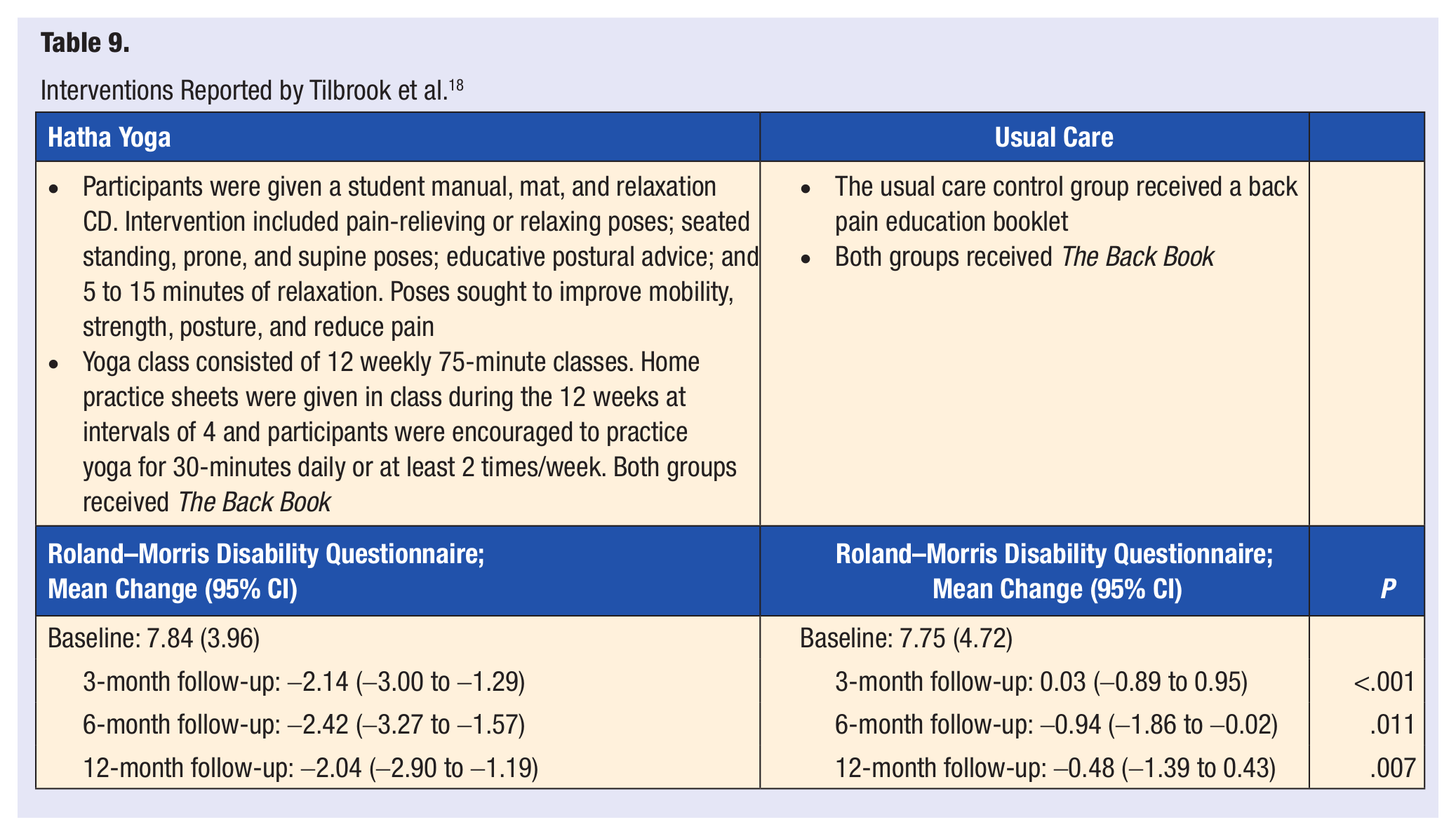
Tilbrook et al 18 randomly assigned 313 adults with chronic or recurrent LBP in 1 of 2 groups: yoga (n = 156) or usual care (n = 157). The participants in the yoga group attended 12 weekly, 75-minute classes. Yoga intervention consisted of asana, pranayama, relaxation techniques, mental focus, and philosophy with each class building on postures from previous weeks. All the subjects received a back pain educational booklet and usual care. Of the 313 participants, 272 were included in the analysis in the last 12 months (25 lost to follow-up, 13 withdrew, and 3 had a change from baseline that could not be calculated). Fourteen adverse events were reported, 2 from usual care and 12 from yoga, related to increased pain. Of the yoga participants, 60% adhered to the program, attending a minimum of 3 of the first 6 classes and at least any other 3 classes, 26% attended at least 1 class, and 15% did not attend any of the classes. The frequency of yoga practiced at home was 82%, 65%, and 60%, during the first 3, 6, and 12 months, respectively. Thirteen percent of participants did not provide any follow-up information for home practice. At months 3, 6, and 12, both groups had similar health scores and back pain. With the adjusted mean score of the Roland–Morris Disability Questionnaire 2.17 points, 1.48 points, and 1.57 points lower in the yoga group compared with the usual care group at months 3, 6, and 12, respectively, the yoga group demonstrated better back function. Based on the Self-Efficacy Questionnaire, the yoga group reported higher pain self-efficacy at 3 months (P = .027) and 6 months (P = .014), but not at 12 months (P = .190). The study suggests that yoga leads to greater improvements in back function when compared with usual care (Table 9).
Interventions Reported by Tilbrook et al. 18
Hatha Yoga Versus No Treatment
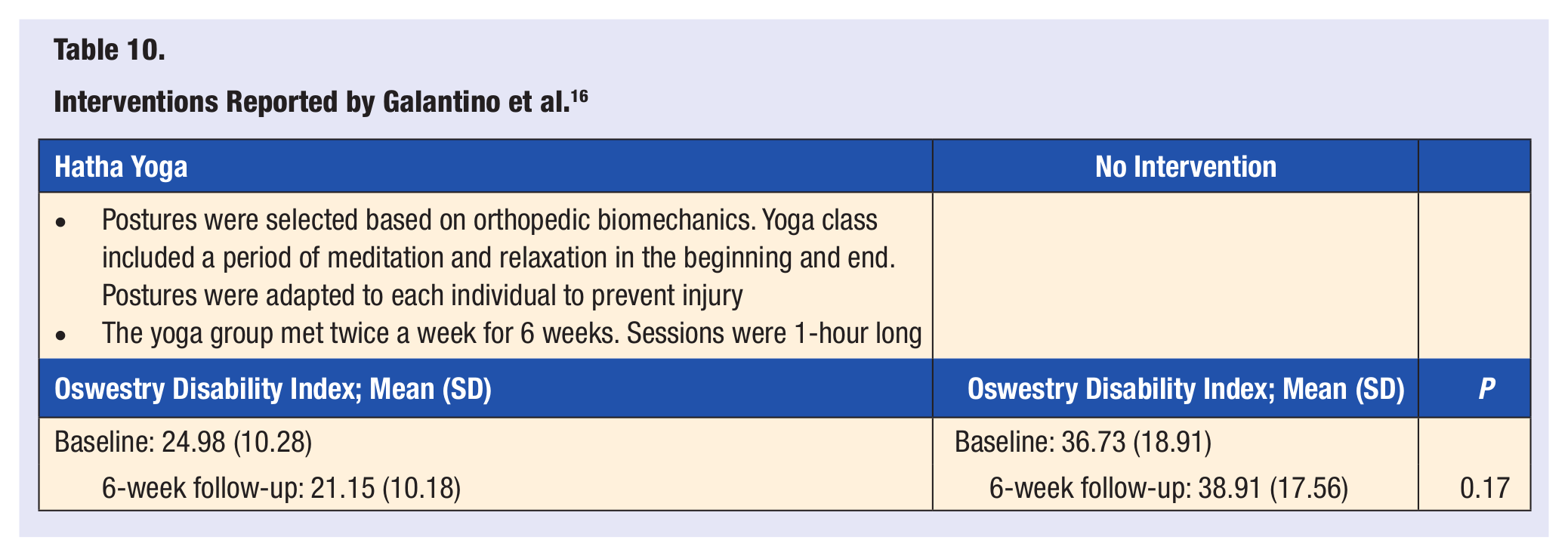
Galantino et al 16 performed the randomized pilot study to examine the effects of a 1-hour, twice a week, 6-week long modified hatha yoga protocol on individuals with cLBP. There were 22 randomized subjects, 11 to the yoga group and 11 to the control group. The trial retained 72% of participants. There were no reports of any adverse events. The yoga intervention consisted of postures that were able to be adapted to the subjects’ capabilities in order to prevent injury; a period of meditation and relaxation occurred at the start and finish of class. Feedback was given to the participants to assist them in maintaining positions with proper body mechanics and proper breathing techniques. There was no statistically significant difference between groups for the ODI (P = .17). The authors stated that this study was not intended for an efficacy analysis but rather to obtain an estimate of the effect size and variance to plan a definitive study. The study was not powered to reach statistical significance, but it did discover functional changes and improvement in quality of life from the yoga intervention when compared with the control group (Table 10).
Interventions Reported by Galantino et al. 16
Specialized Yoga Versus Usual Care and Advice
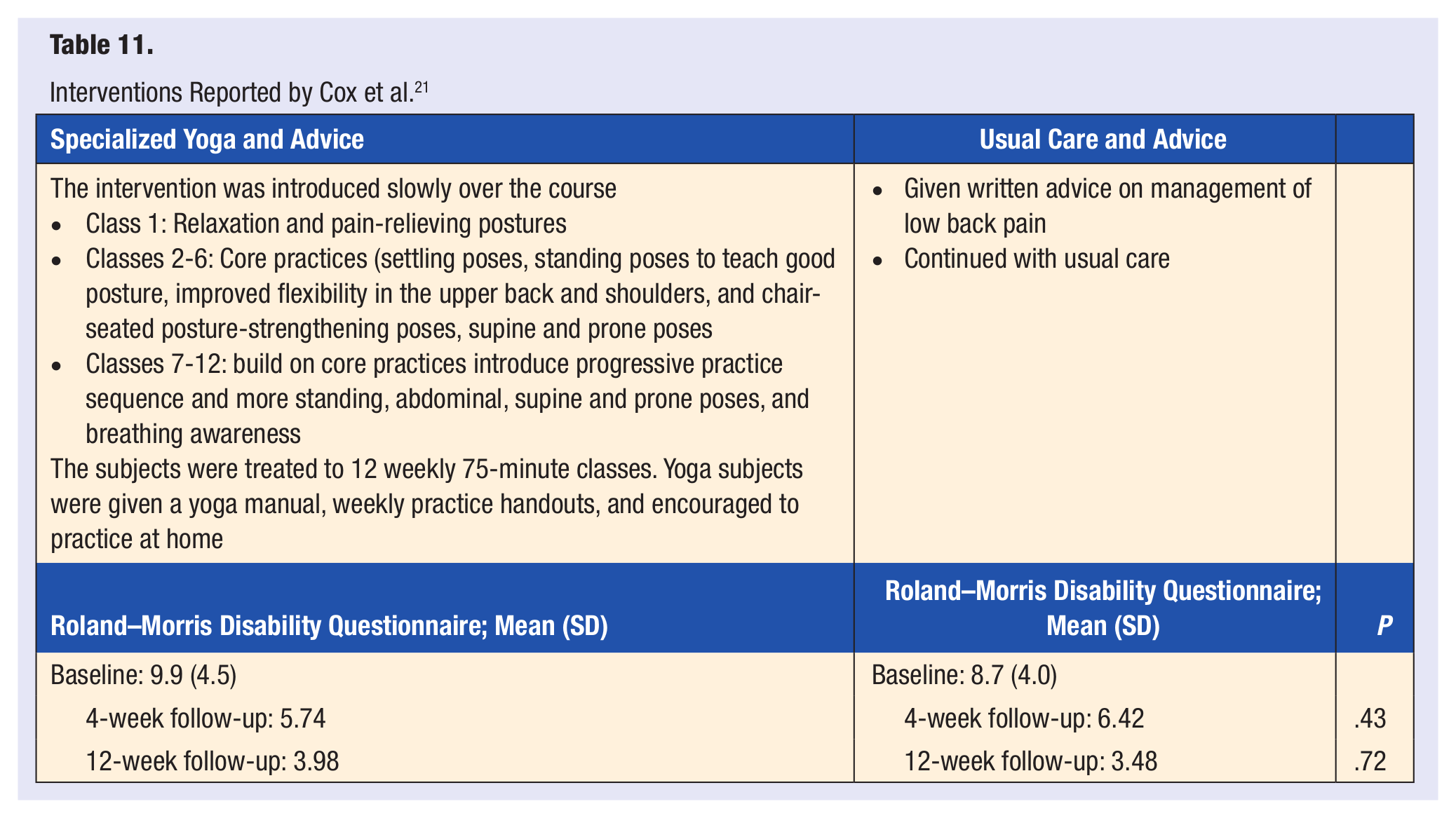
Cox et al 21 performed a pilot study and randomized 20 cLBP participants, 10 to the yoga group and 10 to the usual care and advice group. The participants in the yoga and exercise groups attended 12 weekly, 75-minute classes. Yoga was introduced slowly over the course with the first class focusing on relaxation and pain relieving postures. The 2nd to 6th classes taught core practices, which included poses to teach good posture, exercise to improve flexibility in the upper back and shoulders, and chair-seated posture-strengthening poses. The 7th to 12th classes built on previous poses with more standing, abdominal, supine and prone poses, and breathing awareness. Yoga subjects were given a yoga manual, weekly practice handouts, and were encouraged to practice at home. The follow-up data received from the yoga group at baseline was 60%, 50% at 4 weeks, and 60% at 12 weeks; the usual care group at baseline was 90%, 80% at 4 weeks, and 90% at the 12-week follow-up. There were no reports of any adverse events. The primary outcome assessed was functional limitations as measured by the Roland–Morris Disability Questionnaire, which did not yield significant results at 4-week (P = .43) and 12-week (P = .72) follow-up. The 12-week follow-up reported 66.6% of the yoga group improved by at least 2 points on the disability questionnaire compared with the 55.6% of the usually care group. At both follow-up points in the trial, a nonsignificant trend in the yoga group showed a substantial improvement in pain self-efficacy over usual care (Table 11).
Interventions Reported by Cox et al. 21
Discussion
This systematic review suggests that yoga may benefit individuals when prescribed as an intervention for LBP. Studies have shown that yoga is superior to physical exercises,8,22 education, 4 standard medical care, 19 and usual care with a self-care book.6,17,18,20 However, no statistical difference existed when comparing yoga with stretching, 20 no treatment, 16 and usual care with advice. 21
With the many different styles of yoga available, the randomized controlled trials differed in their choice for treatment of LBP: hatha (Galantino et al, 16 Saper et al, 17 Tilbrook et al 18 ), Iyengar yoga (Williams et al4,19), Viniyoga (Sherman et al6,20), integrated yoga (Tekur et al8,22), and specialized yoga (Cox et al 21 ). However, every yoga style used in the studies centered largely on asanas. Though other inconsistencies identified in the studies included specific details of the interventions, such as class duration and frequency, either 1 week for 8 hours a day,8,22 6 weeks for 1 hour twice a week, 16 16 weeks for 90 minutes a week, 4 24 weeks for 90 minutes twice a week, 19 or 12 weeks for 75 minutes a week; 6,17,18,20,21 number of subjects, ranging from 20 to 313; and follow-up periods, either 1 week,8,22 6 weeks, 16 12 weeks 4 (3 months), 21 6 months, 19 26 weeks,6,20 or 12 months. 18 These inconsistencies in the yoga interventions do not allow for an absolute summary of the results. Each study involved participants with nonspecific cLBP, where the duration of low back pain was at least 12 weeks or as described. The specific inclusion criteria was important for the studies considering the natural course that LBP takes, where 90% of nonspecific acute LBP conditions resolve within 2 weeks and 40% are affected with recurrences within 6 months. 1
The average PEDro score for the trials analyzed was 6.3 and the methodological quality varied with a range of 4 to 8 out of 10 where all studies had limitations. Despite the discrepancies identified in the included studies, the efficacy of yoga as an intervention for LBP is positive. The 2 randomized controlled trials conducted by Tekur et al8,22 found significant differences between the yoga and control groups, concluding that yoga can improve quality of life and reduce disability as reported by scores on the ODI. Williams et al4,19 determined that yoga improved functional disability and reduced pain intensity and pain medication usage. Sherman et al6,20 concluded that yoga was more effective than a self-care book in reducing symptoms and improving function in subjects with cLBP, but not more effective than stretching. 20 Saper et al 17 found yoga to be more effective in reducing pain and medicine use than usual care, specifically in the short term. Tilbrook et al 18 suggested that yoga leads to greater improvements in back function when compared with usual care. Galantino et al 16 did not find significant differences between groups for disability, but did find functional changes and improvement in quality of life in the yoga group when compared with the control group. Finally, Cox et al 21 found the yoga intervention group to have substantial improvement in pain self-efficacy over usual care.
In a related, nonrandomized longitudinal study by Evans et al, 5 53 adults participated in a 6-week treatment for cLBP. Through the use of a modified integral yoga class, 2-hour weekly classes, and twice per week physical therapy, the researchers found a strong correlation between a positive outcome of cLBP treatment and high self-efficacy. At 6 weeks, regression analysis of the Rand Short Form 36 Health Survey 1.0 demonstrated predictive characteristics for social function (R2 = .568, P = .001) and physical function (R2 = .778, P = .00). The Roland–Morris Disability Questionnaire showed significant correlation as well (R2 = .777, P = .001). There were significant between-group differences for pain interaction (P = .026) and pain bothersomeness (R2 = .372, P < .05). The study concluded that yoga participants with low pain self-efficacy (Roland–Morris Disability Questionnaire x = 2.679 ± 1.525) compared with participants with high pain self-efficacy (Roland–Morris Disability Questionnaire x = 3.85 ± 1.706) showed small differences in disability; whereas, the physical therapy participants with low pain self-efficacy at baseline had twice the disability (Roland–Morris Disability Questionnaire x = 8.359 ± 1.706) compared with participants with high pain self-efficacy (Roland–Morris Disability Questionnaire x = 4.045 ± 1.854). However, Evans et al 5 discussed how the social factor in yoga may have presented subjects with a positive influence through social interactions, which the control group did not have. Also, the study suggests the possibility of bias, since participants were allowed to choose between yoga and physical therapy as their treatment. This may explain the different disability outcomes between the groups. The American College of Physicians and the American Pain Society have recommended yoga as an alternative treatment option for managing patients with cLBP. 27
Conclusion
With the advancement of evidence-based care and the noted prevalence of patients with LBP patients, healthcare practitioners should consider yoga as an efficacious intervention in addition to standard education or no care. With the complexities involved in formulating an effective treatment for LBP, yoga is a viable option. Research demonstrated that yoga reduces functional disability, has a positive effect on QOL, and a negative effect on stress, depression and pain intensity. Whether yoga is the most effective treatment for LBP or which style is most effective cannot be determined; however, its overall effect on the subjects in all trials was positive.
Key Points
Evidence demonstrates moderate support for yoga as an effective treatment for LBP.
Yoga was shown to be more effective than no treatment, usual care, a self-care book, but no more effective than stretching or other forms of exercise.
Yoga can improve quality of life, reduce perceived disability, and decrease use of pain medications.