
Abstract
Physical activity during pregnancy has been associated with significant health benefits; however, most women in the United States do not meet the current guidelines. This systematic review evaluates evidence for interventions to improve physical activity during pregnancy in order to identify best practices and inform future research. Electronic databases (PubMed, CINAHL, SportDISCUS, Embase, ERIC, Psych Info, and ISI Web of Science) were searched in July 2011 for peer-reviewed journal articles. Studies were included if they were English-language randomized control trials that measured the efficacy of an intervention targeted at pregnant women and were designed to change physical activity as a primary or secondary outcome. Out of 777 studies identified through the systematic search, 9 interventions were selected for inclusion by multiple reviewers. Data were abstracted using an abstraction form modeled after the “Guide to Community Preventive Services.” Of the 9 interventions included in the review, 3 reported statistically significant positive results for physical activity. Although the interventions included a variety of strategies and techniques, none were uniquely associated with positive outcomes. Overall, this review suggests that little is known about the efficacy of interventions for physical activity during pregnancy. This study provides several recommendations for future research and intervention design.
Introduction
Lack of physical activity (PA) is a problem for women across all age-groups,1,2 but it is of particular concern for women during pregnancy.3-6 Moderate to vigorous PA during pregnancy has been linked to better health outcomes for mothers and their children7-12 and can be protective against the development of chronic illness.13-15 In recognition of the importance of PA during pregnancy, the American College of Obstetricians and Gynecologists (ACOG) released guidelines in 2002 advising pregnant women to engage in at least 150 minutes of moderate-intensity PA each week. 16 These guidelines were supported in 2008 by the US Department of Health and Human Services’ Physical Activity Guidelines for Americans. 17 However, despite the significant health benefits of PA during pregnancy, only 15% of pregnant women meet the minimum national recommendation of 150 minutes of moderate-intensity aerobic activity per week. 3
Moderate to vigorous PA [physical activity] during pregnancy has been linked to better health outcomes for mothers and their children and can be protective against the development of chronic illness.
In light of evidence for the benefits of PA during pregnancy and the low percentage of women attaining the recommended levels of PA, medical practitioners and public health professionals have been working to promote PA behavior change using a variety of strategies. Several systematic reviews have focused on PA during pregnancy as a strategy to influence other health outcomes, such as gestational weight gain, preeclampsia, gestational diabetes, and birth weight.8,9,18-23 However, we located no published systematic reviews of behavioral interventions targeting PA during pregnancy as the primary outcome. The aim of this article was to conduct a systematic review of the literature on behavioral interventions designed to improve PA among pregnant women. The primary goals of this review were to identify effective PA promotion intervention strategies for pregnant women, help guide future intervention design, and build a common literature for professionals who work with women to promote PA during pregnancy.
Methods
Selecting Articles for Review
Electronic databases (PubMed, CINAHL, SportDISCUS, Embase, ERIC, Psych Info, and ISI Web of Science) were searched in July 2011 for peer-reviewed articles. Given that many relevant articles have been published recently, no limit terms were used in the search that could omit articles not yet indexed in PubMed. Four search filters were combined to search each database: (a) one for interventions with pregnant populations, (b) one for interventions focused on PA, (c) one for interventions focused on health beliefs, and (d) one to specify a randomized control trial design (Figure 1). Reference lists of 3 previous reviews of intervention literature related to PA during pregnancy were searched manually for additional references and used to test the search strategy.8,24,25
Search Terms and Strategy.
Inclusion criteria
Studies were included if they were English-language randomized control trials that measured the efficacy of an intervention designed to change PA behavior in pregnant women. PA behavior could be measured as a primary or secondary outcome. Articles that were not randomized control trials and/or were specifically designed only for postpartum women were excluded, as were articles where PA behavior or intention was not measured at baseline and follow-up. Exercise training studies in which PA performance was required as the intervention strategy were also excluded, as the intention of this review was to provide an overview of strategies that encourage elective, nonmandatory PA.
Search results and screening
After removing duplicate articles, this search identified 777 unique publications. Titles, abstracts, and full texts of articles were then screened sequentially against inclusion criteria by EEP. Articles remaining in the full-text stage (n = 19) were dual-reviewed for inclusion by EEP and KRE. Eleven articles were found eligible for inclusion in the review (Figure 2). Two sets of articles, Luoto et al 26 (2010) and Luoto et al 27 (2011), and Yeo et al 28 (2008) and Yeo 29 (2009), reported on the same data set and were combined in the abstraction process. For simplicity, subsequent references to these interventions include only the most recent article.
Article Selection Process.
Data Abstraction
Fifty-three components were abstracted from each article using a data abstraction form modeled after the “Guide to Community Preventive Services: Systematic Reviews and Evidence-Based Recommendations,” developed by the Task Force on Community Preventive Services. 30 Data were extracted by EEP and were independently checked by KRE and DSD. Intercoder agreement was high, and disagreements were resolved through consensus.
Population characteristics
Population characteristics abstracted included information on sample size, population demographics, socioeconomic status, age, parity, stage of pregnancy, and country context.
Intervention strategy characteristics
Intervention strategy characteristics abstracted included overall description of intervention techniques designed to affect PA behavior. Intervention types were first broadly categorized within one or more of the following groups: provision of information only, behavioral intervention, environmental intervention, legislation/regulation, clinical, public health or medical care system intervention, high-risk target population, general target population, physical environment focus, and social environment focus. More detailed information about the intervention, including the setting, particular techniques used, incentives, and timing, was then described qualitatively. Using information from the qualitative description of the intervention, techniques were further subcategorized, following Gardner et al 25 and Mitchie et al, 31 into one or more of the following 8 groups: information, instruction, feedback, problem solving, reward, self-monitoring, goal setting, and modeling (Table 1).
Definition of Intervention Techniques, Adapted From Mitchie et al 31 .
In addition to a basic intervention description, 10 additional items in the abstraction form coded information on eligibility criteria, mode and setting of delivery, duration of intervention, data collection methods, setting and schedule, feasibility and implementation, intervention components, and the theoretical basis for intervention design.
Methodological characteristics
Methodological characteristics abstracted included information on study design, power analysis, measurement of PA and other outcomes, data collection schedule, statistical analyses, and process evaluation. Presence of a power analysis was coded as either “yes” or “no”; measurement of PA was coded as one or more of the following: self-administered questionnaire, laboratory test, record review, attendance, and other, and it was also assessed qualitatively. The qualitative assessment included more detailed information on the measurement tools, including evidence of the validity and reliability of the research instrument. The data collection schedule was assessed qualitatively. Presence of appropriate statistical analyses was coded as “yes,” “no,” or “unknown/did not report” and then further assessed qualitatively. Presence or absence of process evaluation and other implementation information was indicated by both coded and qualitative responses to a question about feasibility issues addressed in the article.
Outcome data
The outcome of interest was PA performance or intention. Outcome data abstracted included information on effect size, statistical significance, sample size, and attrition. The majority of outcome information was coded to indicate presence or absence and then described qualitatively to assess possible threats to validity. We considered an intervention to have an effect if there was a statistically significant (P < .05) difference between the intervention and control groups and a statistically significant positive effect size reported for the intervention group between baseline and follow-up PA measurements.
Validity measures
Validity measures abstracted included information on internal validity, external validity, and statistical conclusion validity. 32 Specifically, the abstraction form contained 23 items that coded components relevant to validity, including selection bias, study design, sample size, inclusion criteria, power analysis, success of randomization, attrition, baseline comparisons of intervention and control groups, validity and reliability of measures, and use and reporting of statistical analyses. Measurement instruments were considered valid if the study reported having validated the measure or cited other evidence for validity.
Results
Nine unique interventions were reported in the 11 studies that were included in the analysis (Table 2). All studies were randomized controlled trials where participants were randomly assigned to intervention or control groups.
Interventions Included in the Review, N = 9.
Abbreviations: PA, physical activity; TTM, transtheoretical model; SCT, social cognitive theory; PMT, protection motivation theory; TPB, theory of planned behavior; MET, metabolic equivalent.
Study Characteristics
A total of 1506 pregnant participants were included in the 9 interventions. Four of the 9 interventions were conducted in the United States.28,33,37,38 Five interventions focused on high-risk groups, which included women with gestational diabetes,26,33 obese or sedentary women,28,35 and women in need of substance abuse treatment. 38 Of the studies reporting participant race (n = 7), 3 had majority white populations,28,34,35 2 had majority Asian populations,33,36 1 had majority African American populations, 37 and 1 had majority Canadian Aboriginal populations. 39
Of all the studies reviewed, only 2 focused on PA as the primary intervention target.34,39 Other primary targets included gestational weight gain,33,35-37 gestational diabetes mellitus,26,39 and preeclampsia. 28 All studies measured PA using self-report questionnaires. Four studies included additional measures of PA, including pedometers,28,39 heart rate monitors, 28 and daily exercise logs or diaries.26,33,36,39
All studies randomized participants into at least 2 groups. Most control groups were usual care controls.26,34-39 In one study, the control group received printed materials about gestational diabetes mellitus and newsletters about health and infant safety. 33 Another study had 2 control groups, one usual care and one that received a brochure about diet. 34 In one study, the control group received the same number of counseling sessions as the intervention group but did not receive PA content in the sessions. 38 One study had 2 intervention groups in addition to a control group, one that received counseling and a brochure, and one that received a brochure only. 35 Finally, one study compared the effects of 2 different interventions, randomizing participants into either walking or stretching programs. 28
Intervention Strategies and Techniques
The majority of the interventions were delivered primarily or entirely in a clinical setting.26,33-37 Other settings included a university exercise lab, 28 home,28,33,39 gym, 39 and a community-based substance abuse treatment facility. 38 Four interventions were delivered in more than one setting.26,28,33,39 Interventions were delivered by exercise specialists,26,28,39 trained nutritionists,33,35 trained nurses,26,36 computers, 37 motivational interviewing specialists, 38 and academic researchers. 34 Duration of interventions ranged from 1 week 34 to 1 year. 36
Four of the interventions were based on one or more health behavior theories or models, including the transtheoretical model or “stages of change,”26,33,37 social cognitive theory, 33 protection motivation theory, 34 and social support. 26 All interventions citing the transtheoretical model used the theory to tailor content to an individual participant’s readiness to change. For all other theories, constructs were used as a basis for general intervention content.
The interventions offered a variety of strategies and techniques intended to promote PA. General strategies included PA counseling by telephone, 33 via computer-based Video Doctor,” 37 and/or in person;26,33,35,36,38 brochures;26,34,35 PA self-monitoring diaries;26,33,36 VHS or DVD exercise instruction; 38 and individual 28 or group28,39 exercise instruction. Specific techniques included information,26,28,33-39 goal setting,26,33,34,36 feedback,26,28,33,36-39 instruction,26,28,39 modeling,28,39 rewards, 28 problem solving,33,35,36 and self-monitoring.26,33,36,39
Validity of Findings
Although 3 of the 9 interventions indicated positive, statistically significant effects on PA outcomes, studies varied in the degree to which the validity of their findings could be established.
Of the 6 studies showing no effect, only 3 presented evidence for most items assessing validity criteria,27,28,35 and none met the full criteria. Specifically, none of the 6 studies were powered on PA behavior; 2 had no power calculation included in the article;33,38 1 had a small sample size (n < 100); 28 2 reported high attrition during the intervention (20% and 35%);33,35 2 reported evidence of differential attrition between the intervention and control groups;33,37 2 did not report a test for significant differences between groups at baseline;37,38 1 found significant differences between groups on smoking and income at baseline but did not control for them in the analysis; 37 and all but one 28 used self-report questionnaires to measure PA, with only 3 reporting that the measure had been validated with pregnant populations.26,33,35
Of the 3 studies showing significant effects, all presented stronger evidence for validity than studies showing no effect, but none met the full criteria. Specifically, none of the studies were powered on PA behavior; 2 had small samples sizes (n < 100);34,39 2 reported high attrition (29% and 24%);34,36 and all used self-report questionnaires to measure PA, with only one reporting that the measure had been validated with pregnant populations. 39
Overall Effectiveness
Of the 10 interventions included in the review, only 3 reported statistically significant differences between the intervention and control groups.34,36,39 One additional study reported a statistically significant difference between baseline and follow-up for the intervention group but did not find significant differences between the intervention and control groups, both of which improved in PA performance. 37 This suggests that improvements in PA were due to a secular trend that affected both groups and should not be attributed to the intervention.
The 3 studies reporting significant intervention effects had a variety of methods of PA measurement and a range of effect sizes for intervention groups between baseline and follow-up. Gaston and Prapavessis 34 and Hui 39 measured PA in minutes per week and reported relatively small effect sizes: 8.6 metabolic equivalent (MET) min/wk and 0.77 min/wk, respectively. Huang 36 measured PA on a 4-point scale (1 = never, 2 = sometimes, 3 = often, 4 = rarely) and reported a 2.45-point increase in average PA scores.
The duration of effective interventions ranged from 1 week 34 to 1 year 36 and varied in dose from one session lasting less than 1 hour 34 to six 30-minute sessions. 36 Only one intervention was theory based, using protection motivation theory. 34 Intervention strategies included brochures,34,36 PA counseling as part of regular prenatal care visits, 36 and group exercise instruction in person and on VHS or DVD. 39 Specific intervention techniques in the studies demonstrating positive effects included information,34,36,39 goal setting,34,36 problem solving, 36 feedback,36,39 self-monitoring,36,39 instruction, 39 and modeling. 39
Discussion
The purpose of this systematic review was to report evidence from randomized controlled trials for behavioral intervention strategies to encourage PA behavior during pregnancy. Nine unique interventions were assessed. Overall, our findings suggest that little is known about the efficacy of interventions for PA during pregnancy. Three interventions reported having a positive effect on PA during pregnancy, and interventions employed a variety of strategies and specific program techniques for behavior change (Figures 3 and 4).
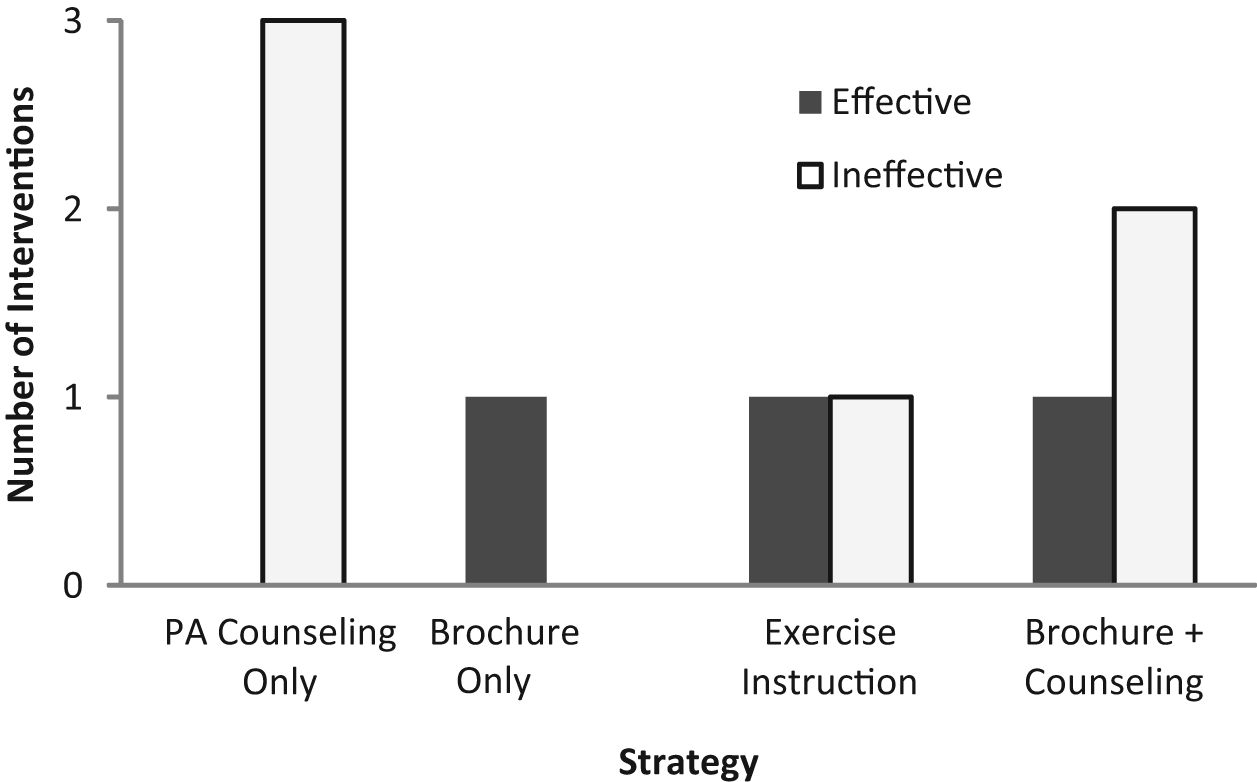
Effective and Ineffective Intervention Strategies.
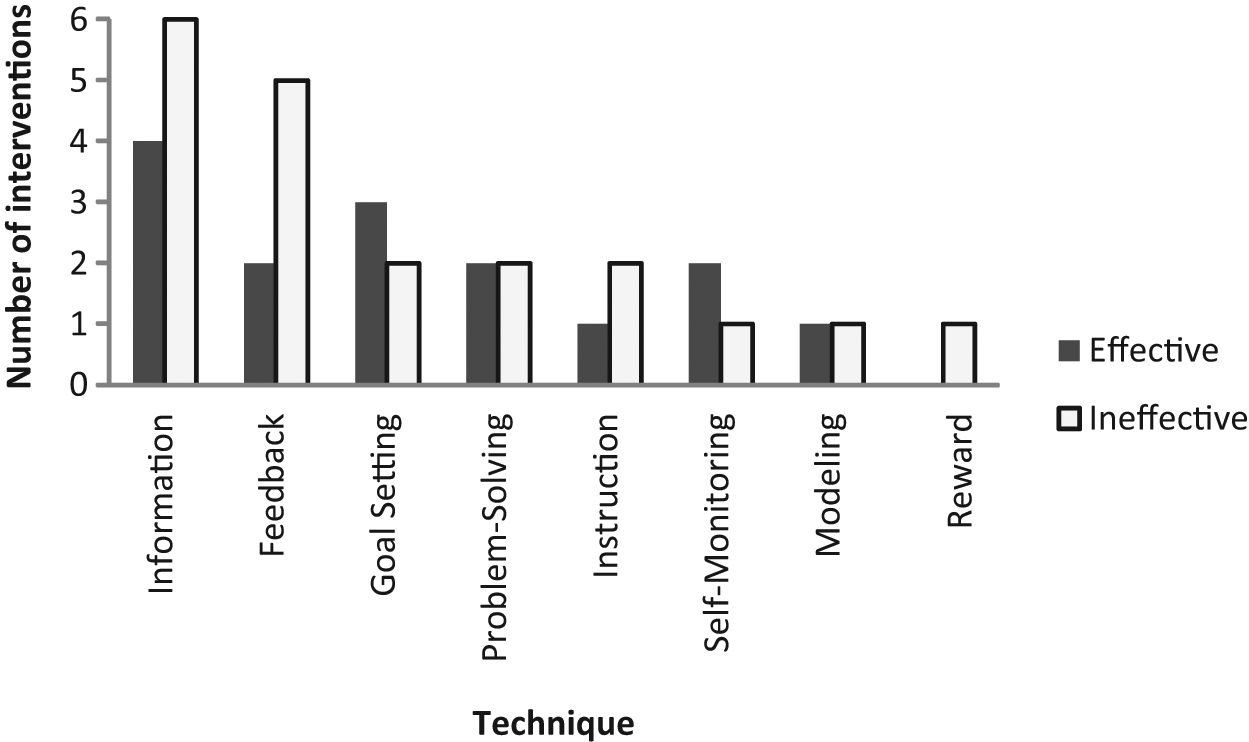
Effective and Ineffective Intervention Techniques.
The most commonly used strategy was PA counseling, with and without take-home brochures (featured in 6 interventions). The most common intervention techniques were provision of information on PA during pregnancy (9 interventions) and feedback on PA performance (7 interventions). However, we found no unique strategies or techniques consistently associated with positive outcomes.
In addition to the similarity of intervention strategies in effective and ineffective interventions, elements of study design limited our ability to assess the validity of findings. Interventions that did not report an effect either had no power calculation33,38 or were not powered on PA outcomes,26,28,36,37 suggesting that they might not have adequate statistical power to detect changes in PA. This could have contributed to type II error, or failing to find an effect when it was present. Of the 3 studies reporting significant results, only 1 study 36 achieved the required sample size, as indicated by a power calculation. The small sample sizes may have decreased the effectiveness of the randomization process. Ineffective randomization could contribute to type I error, or finding an effect that was actually due to bias. Possible types of bias in terms of threats to internal validity included differential attrition and selection, which could be assessed if differences between groups were measured at baseline. One study 38 did not report testing for baseline differences between the intervention and control groups, but all other studies tested for and did not find significant differences between the 2 groups. This suggests that threats to internal validity were minimized in most studies by effective randomization. Only 3 studies26,33,39 reported using a PA measurement questionnaire that had evidence for validity among pregnant women. This suggests that the measures pose a threat to statistical conclusion validity. 32
In terms of external validity, although the interventions overall included diverse samples, none of the 3 effective studies focused on high-risk populations. Of the interventions in this review, only 4 were delivered in the United States.28,33,37,38 Because policies affecting access to prenatal care, usual care procedures, and norms of PA vary between countries, it is not possible to generalize most studies to the US context.
Recommendations
Because of the limitations of study designs, the outcomes of several intervention trials included in this review are uncertain. Absence of major differences in the content and delivery of effective interventions compared with ineffective interventions further underscores a lack of understanding of “what works”. Below we offer some suggestions for future research.
Design interventions to include strategies suggested by formative research with pregnant women.40-43
Expand intervention targets beyond pregnant women to include other “key players,” such as medical providers, family members, and social networks.44-46
Consider the social ecological framework by expanding the intervention focus beyond the individual level to target interpersonal, community, and population/policy levels. 47
Design interventions using health behavior theories and models demonstrated to be relevant to pregnant populations, such as the transtheoretical model,48-51 social cognitive theory,48,51-53 social support,48,54 theory of planned behavior,4,55,56 social ecological model,4,44,51 the life course framework,1,57,58 and the health belief model. 44
Strengthen study designs by using power calculations based on PA effect size estimates, inflating sample size requirements to take into account attrition rates and measuring and accounting for baseline differences between groups.
Increase the generalizability of evidence to minority and high-risk populations by including these groups in the intervention.
Improve retention rates during the study by limiting participant burden in data collection and by providing incentives of interest to pregnant women. 59
Improve assessment of PA by using a combination of self-report and objective assessments that have evidence for validity and reliability among pregnant women.
Conduct studies that are replicable.
Consider partnerships with local businesses, insurance providers, or nonprofits to provide vouchers, prizes, or other types of compensation and widen the sphere of community involvement.
Conclusion
Despite the significant health benefits of PA during pregnancy, most women in the United States do not meet the PA minimums set by current guidelines. 3 In recognition of the public health importance of PA behavior during pregnancy,3,5,6 interventions to improve PA in this population have been designed and evaluated. In our review of those interventions, few were found to have had a significant impact on PA behavior or intention, and methodological weaknesses decreased the validity of the study results. The findings of this systematic review underscore the need for further research to effectively design and evaluate interventions to promote PA during pregnancy. The recommendations provided here are intended to help guide practitioners and researchers considering intervention strategies to address this important public health issue.
Footnotes
Acknowledgements
The authors wish to thank Kathleen A. McGraw at the University of North Carolina at Chapel Hill Health Sciences Library for her helpful assistance in assembling the search terms for this review and the anonymous reviewers for their feedback. Kelly Evenson was funded by the National Institutes of Health (NIH)/National Cancer Institute (#CA109804-01). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.