
Abstract
Many young athletes train and compete under conditions that put their body fluid balance at risk, and hypohydration is usually the major concern. Another less frequent condition is hyperhydration that—if accompanied by other risk factors—may cause hyponatremia. Water and electrolyte losses during physical activities occur primarily from sweat. Such losses have been identified mostly in active (but nonathletic) young populations under laboratory settings. Studies have been trying to estimate fluid losses in the athletic population under field conditions, taking into account the sport modality and environmental conditions. Besides these external conditions, young athletes adopt different drinking attitudes, which may depend on knowledge, education, and the opportunities to drink during the break periods as well as fluid availability. Focusing on the young athlete, this review will discuss water and sodium losses from sweat, the effects of hypohydration on performance, and fluid intake attitudes within and during practices and competitions. Some considerations related to the methods of identifying hydration status and guidelines are also given, with the understanding that they should be individually adapted for the athlete and activity. The young athlete, parents, coaches, and athletic/health professionals should be aware of such information to prevent fluid imbalances and the consequent hazardous effects on performance and health.
Introduction
Sport performance and health maintenance can be affected by body fluid balance, which involves not only body water content within the different compartments but also body electrolyte concentration. Under certain conditions, young athletes may be at risk of fluid imbalances. Fluid loss from sweating can be substantial and not be fully compensated by fluid intake. Drinking attitudes and the amount of fluid intake of active children and adolescents is influenced by individual factors such as sport modality, 1 type of competition and practices, 2 circumstances between sporting events,3,4 sun exposure, 5 and the characteristics of the available beverage.6-9 Educational interventions10,11 and awareness of hydration status can also contribute to adequate fluid intake attitudes in young athletes. Among some fluid imbalance conditions, which will be defined in the next section, hypohydration is most prevalent compared with hyperhydration and/or hyponatremia.
Unlike in adults, we still do not know how much hypohydration is required to adversely affect athletic performance and health in young athletes.
In the adult literature, it has been consistently documented that hypohydration accelerates the rate of core temperature increase and adds stress to the cardiovascular system during exercise, especially in the heat. As a consequence, hypohydration impairs physical performance (mostly endurance activities), increases fatigue and perception of effort, and decreases motivation.12,15,16 In addition, there is an increase in the risk of injuries and heat illness. Unlike in adults, we still do not know how much hypohydration is required to adversely affect athletic performance and health in young athletes. It was observed that children, compared to adults, experience a greater increase in core temperature as they become dehydrated. 16 Despite their lower sweating rate and higher metabolic cost of locomotion, there are other physical and physiological characteristics that have traditionally explained thermoregulatory disadvantages in children. 17 Their higher surface area to body mass ratio could potentially induce a higher heat gain in conditions in which air temperature is higher than the skin temperature 18 ; however, a small number of studies that showed similar thermoregulatory responses between boys and males 19 and between girls and women 20 led to a recent change in this interpretation. 21 Therefore, more studies are needed to clarify thermoregulatory differences between maturational groups while they exercise in the heat.
The heat acclimatization process, as a result of repeated heat exposure, may be delayed in children when compared with adults.22,23 Particularly at the start of the season, it is possible that young athletes are at risk for hypohydration and associated heat-related problems because of lack of acclimatization to the hot conditions and sudden increases in activity/training levels.24,25 It is alarming that the number of American high school and college deaths in football players caused by exertional heat stroke in the past 10 years has nearly doubled from 15 to 29, 26 and heat-related illness among young athletes is a major concern.27-31
On the other hand, hyperhydration is also undesirable, particularly when accompanied by excessive ingestion of low-sodium or sodium-free drinks and large sweat sodium losses. 32 In such scenarios and combined with other risk factors, an abnormally low serum sodium concentration (ie, hyponatremia) may occur, and its adverse effects are severe for health. However, we are not aware of any reported cases of symptomatic hyponatremia in young athletes during competitions or training.
Active or athletic youngsters, as do adults, appear to start their physical activities already hypohydrated13,11,33-35 and/or dehydrate during competitions 36 or practices.2,37 Given the potential for performance impairment and clinical problems, body fluid imbalance should be prevented. Suitable in-field tests, including body mass and urine marker measurements, are available to evaluate hydration status.
Some assumptions derived from the adult population or nonathletic youngsters have been made to complement our understanding in this growing population of athletes. Also, much information is derived from laboratory settings, instead of in-field conditions, because the former has been the focus of previous research. The majority of young athletes participate in team sports in which opportunities for fluid ingestion occur during break periods or during accidental stoppages in the game. Our goal is to synthesize the available knowledge, so that athletes, coaches, parents, and professionals can help recognize body hydration status and establish individual hydration recommendations to optimize performance and the well-being of the young athlete. The purpose of this review is to focus on the characteristics of sweat loss and fluid intake during physical activities of young athletes, their risk of fluid imbalance, methods to assess hydration status applicable to the pediatric population, and general hydration advice for the young athlete.
Definitions of Terms and Classification Issues
The notion of water balance is generally expressed by a sinusoidal line that slightly fluctuates from a “normal” or “euhydrated state.” Under thermoneutral ambient conditions, body water content of a healthy adult should vary around ±0.25% and perhaps not more than ~0.5% under heat conditions. The term hyperhydration is used when the hydration state is above this range. Conversely, when the hydration state falls below this range, it is referred to as hypohydration. The terms dehydration and hypohydration are often used interchangeably; however, dehydration refers to the active process of losing water from a euhydrated state, whereas hypohydration refers to a state of body water deficit. Hypohydration has been classified into categories according to the amount of water loss, expressed as a percentage of the initial body weight. The World Health Organization 38 and the American Academy of Pediatrics 39 have developed assessment guidelines for the pediatric population based on percentage body mass loss and clinical manifestations and classified hypohydration as mild (4%-5%), moderate (6%-9%), and severe (>10%). This classification was established from conditions in which hypohydration was caused by illness such as gastroenteritis, and therefore, it is not applicable when dehydration is caused by exercising in the heat. In a person who is exercising, the metabolic body heat produced from muscle contraction, in combination with the heat gained from the environment, aggravates the clinical manifestations at a given level of hypohydration, independent of age. In addition, lower hypohydration levels (1%-2%) have been shown to cause adverse cardiovascular, thermoregulatory, and cognitive responses and impair performance before the appearance of any clinical sign or symptom. Greenleaf 40 advised in a review that under exercise/heat situations, hypohydration of 1% to 2% increases body temperature; at 3%, important decrements in performance time can occur; at 4% to 6%, cramps and heat exhaustion may occur; and above 6%, the risk of heat stroke increases. It is not easy to determine whether these thresholds can be generalized and applied to young athletes. Because of ethical constraints, research has not dehydrated children and adolescents to levels higher than 2%.
Another consideration when classifying hydration status is that a given volume of water loss may differ when expressed relative to body mass as opposed to body water content. Water is the largest component of the human body. As the proportion of water is greater in infants and children and decreases with age, by the end of adolescence, it likely reaches the adult proportion of about 60%. Total body water is also affected by factors such as training and gender because they are influenced by the individual’s body composition. For example, muscle tissue is approximately 85% water, whereas adipose tissue constitutes ~10%. In addition, trained athletes have greater relative body water because of larger muscle mass and muscle glycogen levels, which increase water transport into the muscle, 41 and by fluid-regulating hormone adaptations (ie, aldosterone and sensitivity). 42 There is no reason to believe that adolescent athletes, especially those involved in endurance training, do not experience some of these same adaptations, although there is no direct scientific evidence to support this issue. Novak 43 showed that a significant increase in body water content during the growth spurt years was only experienced in boys and that water content in adolescent boys is higher than in girls of the same age group. The extent to which training status, maturation, and gender interact to influence total body water content and the performance and health impact of body water deficits are unknown.
The term hyponatremia is defined as a serum sodium level <135 mEq L−1, and a level <130 mEq L−1 is considered to be severe hyponatremia. Clinically, hyponatremia is also referred to as a fast lowering of blood sodium, for which symptoms may appear.
Fluid Loss During Exercise
Water Loss
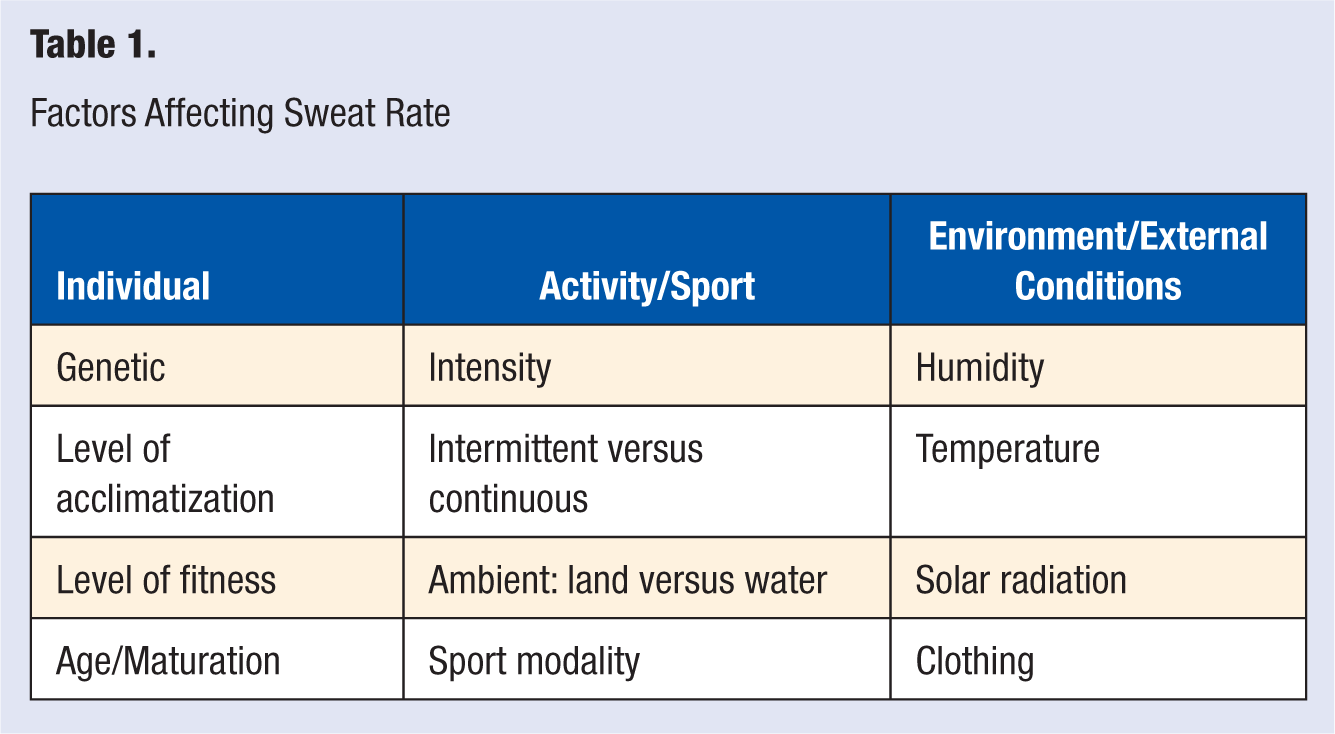
Sweat volume and composition primarily determine the extent of exercise-induced fluid losses. It is, therefore, helpful to have an estimate of an individual’s sweating characteristics because these can vary considerably depending on the athletes and exercise conditions. A number of factors influence sweating rate (see Table 1), making it difficult to establish a common estimate with general applicability for all young athletes.
Factors Affecting Sweat Rate
The volume of sweat lost during training or competition can be obtained by calculating the change in body mass from before and after the task while correcting for fluid intake and, if the bladder has not been emptied, correcting for urine output. If possible, the measurement of body mass should be made with the athlete naked or with minimal dry clothing designated for preexercise and postexercise body weight because clothing that is wet from sweat can overestimate the final body mass value. Fluid intake is most often assessed by calculating the change in mass of a standard drinking container offered to the athlete, and thus, care should be taken to individualize and label bottles and avoid discharging bottles or drinking from external sources (eg, water fountains). It is considered that each liter of sweat loss corresponds to 1 kg of body mass loss. This estimation is not quite precise because it does not account for water losses from respiration or water produced from substrate (glycogen and fat) use. Children and adolescents appear to oxidize relatively more fat than carbohydrate, compared with adults, at a given relative intensity of exercise, 44 and oxidation may also be affected by the carbohydrate intake during exercise.45,46 For practical reasons, such potential errors in calculating sweat rate have been ignored because the respective volumes are minimal compared with the considerable volume of water lost as sweat.
Under a given physical activity and/or environmental condition, sweating rates are usually lower in children than in adults (for reviews see Falk and Dotan 47 and Meyer and Bar-Or 48 ). There is evidence that sweating rate increases with the maturational process, with pubescent children sweating more than prepubescent children but less than young adults.49,50 This difference seems to be more apparent in boys as opposed to girls exercising in a warm and humid climate.19,51 The majority of studies, however, have been conducted in an active and nonathletic population, and there are few studies involving young athletes.
Overall, endurance athletes have a greater sweating rate compared with untrained individuals, 52 but the modality of exercise still affects sweating. For example, endurance swimmers and runners may not have the same degree of sweating adaptations because training and competing in the water helps dissipate body heat production through convection and conduction. Young adult swimmers did not sweat as much as runners (0.45 vs 0.75 L or 6 vs 10 mL kg−1) when they cycled on land for 30 minutes at similar intensity and heat (32°C, 40% relative humidity) conditions. 53 Heat exposure while living under heat stress or moving from cold to warm conditions also produces an increase in sweating rate. 54 Therefore, adjustments in volumes of fluid intake should be done taking into account not only the sport modality and fitness level but also the training season or timing of heat exposure.
Sodium Loss
The electrolytes lost in sweat are mainly sodium and chloride, but smaller quantities of potassium, calcium, magnesium, and other minerals are also present. Their amounts are related to the volume and rate of sweat produced and, therefore, vary according to individual factors already presented in Table 1. Endurance training and/or heat acclimatization appear to lower sweat sodium and chloride concentrations.55,56 For the purpose of this review, we will focus on sodium as it is the major ion in sweat and in the extracellular space. In the body, sodium determines water shifts within compartments and, therefore, fluid balance and the maintenance of plasma volume and other fluid compartments as well. As a consequence, sodium has been more frequently reported than other electrolytes.
In some situations, it may be helpful to identify those young athletes who present with a high sodium loss. Recent studies4,11 in the young population have used the method of adhesive gauzes (known as sweat patches), as described by Patterson et al. 57 The usual sites for sweat collection are the scapula, chest, forearm, thigh (all on the right side of the body), and the forehead. Other sweat collection techniques include direct pipetting from the skin, use of capsules, and the total body wash-down technique, which is not feasible to perform in field conditions and is probably less acceptable to children. The use of impermeable bags described by Boysen et al 58 has been adapted in previous studies with children and adolescents during exercise49,50 and was shown to be reliable. 59
Once we know the sweat electrolyte concentration, the amount of electrolytes lost is calculated by multiplying the concentration by the sweat volume. If we want to express the loss in grams, we multiply the resultant amount in mmol (or mEq) by the respective molecular weight of the electrolyte (see Table 2). To estimate the total body electrolyte loss, we should add the electrolyte lost from urine, which is more influenced by dietary intake. Relative to urine, the volume of sweat was shown to be about 3 times greater in active/ competitive children who exercised and remained euhydrated during 50 minutes of intermittent cycling in the heat; however, the resultant electrolyte lost from sweat was comparable to that lost in urine. 60
Estimated Sodium Sweat Losses From Exercise, Under Different Conditions, in the Young Population
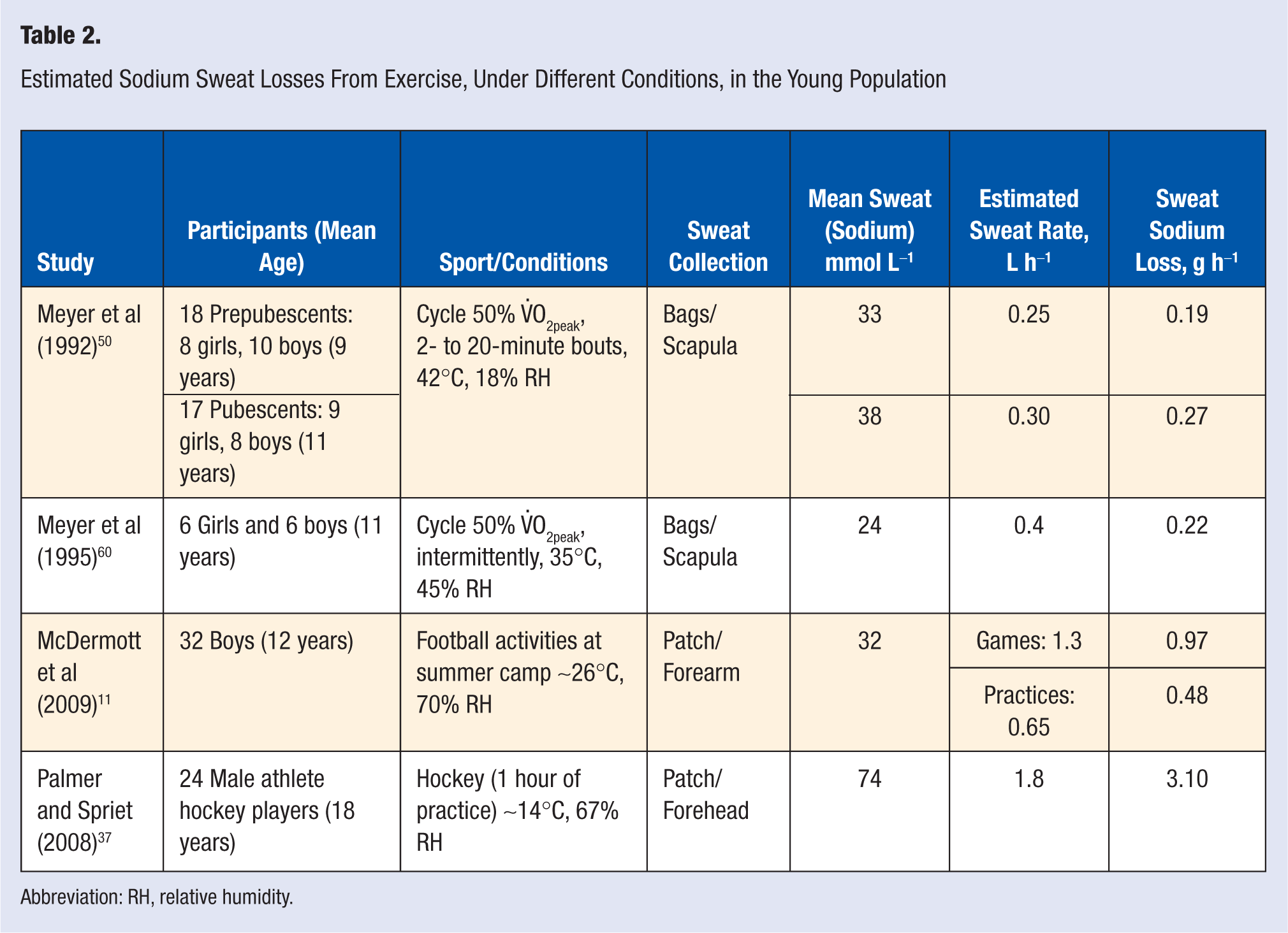
Abbreviation: RH, relative humidity.
Studies that analyzed sweat electrolyte concentration from children and adolescents (up to the age of 18 years old) during exercise have shown some variability, which is expected, as in adult studies. Table 2 lists the studies, the respective exercise/conditions, and the amount of sodium loss estimated.
Despite the lower sweat sodium concentration and losses in children and adolescents compared with those of adults, the resulting sodium balance in response to exercise is expected to be negative, even when rehydration is achieved with a typical sports drink, because these beverages usually contain a lower sodium concentration (about 20 mmol L−1 or less) than sweat. The effect of sodium ingestion on total body sodium balance (including urine) was examined 60 in 9 active children (11 years old) who cycled intermittently in the heat in 3 separate sessions during which they were kept euhydrated with solutions that only differed in sodium content: 0, ~10, or ~20 mmol L−1. Independent of the session, a sodium deficit occurred. Not surprisingly, this deficit per hour was greatest when the sodium-free solution (~0.2 g) was consumed compared with situations when sodium was replaced with the sodium solutions of 10 (0.16 g) and 20 mmol L−1 (~0.10 g). Such deficits, however, did not affect plasma concentrations of sodium because plasma volume is expected to decrease with exercise, and thus, sodium concentration in plasma is expected to be maintained or even be higher.
Based on the calculated sodium loss from sweat per hour (Table 2), a range from 0.2 g in prepubescents to 3.1 g or higher in young adults can be observed. Such sodium losses are minor compared with the overall body sodium content, and they could easily be compensated afterward, except when long bouts are repeated and no sufficient rest time exists between matches, as in tournament scenarios. Current information alerts that the pediatric population—probably including young athletes—is ingesting more salty foods and snacks,61-63 exceeding the desirable upper intake of 2.2 g per day.64,65 However, taking the study of McDermott et al 11 as an example, the sodium loss from sweat of a 12-year-old boy who practices American football for 2 hours may exceed his adequate daily intake of 1.5 g. 64 In the recent study by Logan-Sprenger et al 66 involving elite, male junior hockey players (18 years old), a higher mean sodium deficit of 2.3 g was experienced during an ice hockey game, even when they ingested sodium by either drinking a carbohydrate–electrolyte solution (CES, 270 mg per 591 mL) or by adding an extra 770 mg of sodium to the CES. These “in-field” studies suggest that sweat sodium losses from sweat may become relevant and gradually aggravate body sodium deficits when combined with an unusually low sodium intake and other risk factors, such as those described in the later subsection “Risk of hyperhydration and/or hyponatremia.”
Effects of Fluid Imbalances
Hypohydration and Aerobic Performance Activities
Hypohydration has consistently been shown to impair aerobic performance and cause fatigue to occur earlier in the adult population, even at mild levels (as low as 1%-2% body weight loss). The mechanisms underlying premature fatigue in sustained aerobic exercise may be explained by thermoregulatory, cardiovascular, and metabolic factors. Gradual dehydration causes an increase in the magnitude of core temperature and heart rate elevation at the same time that blood flow, stroke volume, cardiac output, and skin blood flow become relatively lower compared with a euhydrated state, especially in the heat (for reviews see Cheuvront et al, 12 González-Alonso et al, 67 Murray, 68 and Sawka 41 ). Hypohydration also affects muscle metabolism by accelerating the rate of glycogen depletion and central nervous system functioning by reducing motivation and effort.
These aforementioned detrimental responses shown in adults were mainly observed in prolonged and, therefore, submaximal exercise (~65%-70% V.O2peak). It is also likely that children’s performance is impaired by hypohydration, even at shorter and more intense efforts. Wilk et al 69 have examined this question in physically active boys (10 to 12 years old); 9 boys cycled at ~90% V.O2peak to exhaustion after a 45-minute rest period following a 2-hour intermittent cycling protocol in the heat. In 3 separate sessions, the boys dehydrated by 0%, 1%, or 2%. Mean time to exhaustion was ~2 minutes earlier at 2% hypohydration (5.38 minutes) compared with when the boys were euhydrated (7.35 minutes). Time to exhaustion at 1% hypohydration (6.20 minutes) did not differ from that in the other sessions, and the calculated total work to exhaustion followed a similar pattern. Because this was a high-intensity performance test, we suppose that such impairment could be extrapolated to effort patterns required in many team sports, as discussed below. However, because this was a single study, a gap in our knowledge remains with respect to the impact of hypohydration on the aerobic performance in children and adolescents, whether they are athletic or not.
Hypohydration and Team Sports: High-Intensity and Intermittent Efforts, Strength, and Power
Most young athletes are involved in sport modalities such as basketball, soccer, tennis, and gymnastics, which are characterized by high-intensity and intermittent bouts of exercise, yet still demand specific skills that may extend for a few hours. Occurrence of hypohydration (1%-3% of body mass) has been described in young athletes practicing or competing,2,70 but the degree to which it affects specific performance skills is not clearly understood.
Basketball seems to be the sport modality on which the majority of research has been focusing in the young athlete population, but results are still inconsistent. An early study by Hoffman et al 71 in 10 basketball players (mean age 17 years) found no difference in shooting performance, anaerobic power, vertical jumping height, or counter movement jump during a simulated game when no fluid was given (causing a progressive hypohydration of ~2%) versus a game in which ingestion of pure water maintained players euhydrated. Conversely, Dougherty et al 72 showed that 2% dehydration before a simulated game impaired basketball shooting, sprinting, and lateral movement times in younger boys (12 to 15 years old). A study by Baker et al 73 in older adolescent and young adult (17 to 28 years old) athletes showed a progressive impairment in basketball skills as the percentage dehydration increased from 1% to 4%. Recently Carvalho et al 74 showed an increase in the rate of perceived exertion but no impairment in a set of basketball drills (2-point, 3-point, and free-throw shootout, suicide sprints, and defensive zigzags) in 12 adolescent athletes (14 to 15 years old) who were dehydrated by 2.4% from a previous 90-minute training session. These studies reveal limitations when transferring in-field settings from laboratory models, and inconsistent findings may be a result of different study protocols and testing performance models (reflecting the complexity of field research) and/or age-maturational factors.
Studies examining the effect of hypohydration in soccer, which is a worldwide sport played by most children and adolescents, have been restricted to the adult population. One study 75 showed that dribbling performance was impaired in male players (mean age 20 years) after a simulated soccer practice where players were hypohydrated (2.4%) compared with when they were euhydrated. The performance of a specific intermittent shuttle run test was also impaired when soccer players (mean age = 24.4 years old) dehydrated by ~2%. 76 Nevertheless, a study 70 and abstract publications77,78 have reported the occurrence of hypohydration during youth soccer camps, but no relationship to performance was reported. Whether we can assume that hypohydration impairs the performance of young soccer players as much as that of adults remains to be clarified.
Another consideration is the carryover effect of successive strenuous competition events on a single day, which may not allow sufficient time for the young athlete to recover from a previous hypohydration state. For example, in a field study 79 during junior tennis championships that occurred in the heat, players were not as well hydrated prior to the doubles (in the afternoon) as in the morning singles matches (see Table 3). As a relationship was found between prematch hydration status and increase in core body temperature (ingestible sensor), players who were less hydrated might have been at a greater risk of exertional heat illness. Besides tennis, basketball, and soccer, other examples of youth sports tournaments that may pose a risk to a supposed “unrecovered” body fluid balance in warm environments are softball, baseball, and track and field hockey (for reviews see Bergeron33,80).
Hydration Status in the Young Population According to Urinary Markers Before Practices and/or Competitions in Different Sport Modalities
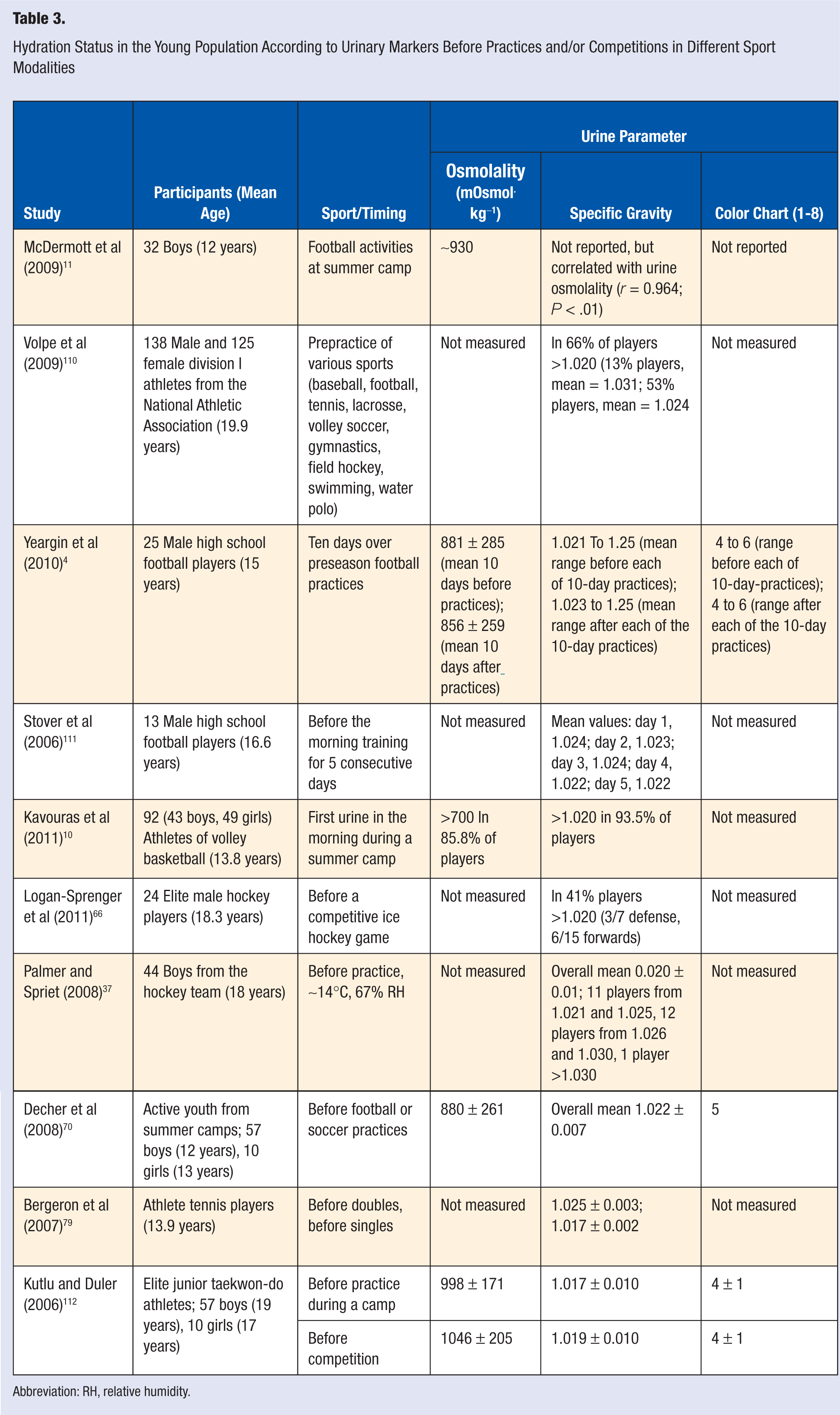
Abbreviation: RH, relative humidity.
A complete rehydration between same-day competitions/practices likely helps decrease the physiological strain and increase performance for the following exercise event. A study by Bergeron et al 3 tested this hypothesis in 24 young athletes (boys and girls from 12 to 13 and from 16 to 17 years old) during 2 identical 80-minute intermittent exercise bouts (treadmill and cycle at 60% and 40%V.O2peak, respectively, in the heat separated by a 1-hour recovery in a thermoneutral room where athletes were fully rehydrated). Overall, no “remaining” effect was observed according to core temperature (measured by ingestible sensor), heart rate, and the calculated physiological strain index parameters. However, in some of the older athletes (16 and 17 years old), a greater physiological strain and rating of perceived exertion were observed in the second bout, suggesting an incomplete recovery. This is an interesting finding, suggesting that recovery from exercise may be related to maturational differences (such as substrate use) rather than hydration level. Younger prepubescent boys (8 to 12 years old) recovered faster than young adults (18 to 23 years old) following consecutive and shorter high-intensity efforts. 81 Therefore, information regarding the effect of hydration level on high-intensity efforts of young athletes should be based on studies of this specific group.
Hypohydration and Cognitive Function
In many games and sports situations, young athletes will require cognitive and reaction abilities, in addition to physical conditioning. Some studies in the adult population73,82-84 already indicate that a variety of cognitive functions such as vigilance, attention, short-term memory, perceptual discrimination, arithmetic ability, visuomotor tracking, and psychomotor skills are affected by a moderate hypohydration of ~2%. In contrast, exercise-induced dehydration (up to 2% body weight) did not affect cognitive functions (choice reaction time, choice movement time, selective attention, goal-directed aiming, and short-term memory) in 10- to 12-year-old nonathletic boys. 85
From the sport or athletic angle, the effect of hypohydration on cognitive function in the pediatric population has not been documented as extensively as in adults. 86 Bar-David et al 87 observed children (10 to 12 years old) who were divided into a euhydrated or a dehydrated group. In the morning, groups were similar in cognitive tasks. At noon, the hydrated group performed better on tasks such as short-term memory, verbal analogy, and making groups. Two studies88,89 indicated that some visual attention tasks are improved in children as young as 6 to 9 years old once they drank water and their thirst levels decreased.
A recent randomized, crossover study 90 examined the brain function and structure of 10 healthy adolescents (mean age 16.8 years old) by using magnetic resonance imaging after they dehydrated an average of 1.64% from 90-minute intermittent cycling and wearing extra clothing. Because hypohydration showed a greater increase in the response of blood oxygen level in the frontoparietal region of the brain that was not accompanied by changes in cognitive tests (physical/mental sedation and visual analog rating scales), the authors suggested that adolescents had to apply greater neuronal activity to achieve similar performance. This novel finding in adolescents indicates that overall central fatigue may be preceded by cognitive or skill impairments during exercise.
Risk of Hyperhydration and/or Hyponatremia
Although hyperhydration is not likely to happen in young athletes, concerns about overdrinking—particularly during prolonged exercise events—exist because of the associated risks of hyponatremia and health-related problems. In adults, hyponatremia is mainly reported in long events (>2 hours) in which excessive volumes of low-sodium or sodium-free drinks are ingested and sweating is intense. 32 Many athletes may be asymptomatic as serum sodium concentrations are at a lower level of ~135 mmol L−1. However, detrimental adverse effects can appear in adult athletes as serum sodium concentrations keep falling to 130 to 125 mmol L−1.32,91-93 Some of the signs and symptoms of hyponatremia include cramps, nausea, vomit, headache, lethargy, mental confusion, and edema of feet and hands. Further decrease in serum sodium concentrations, especially at a rapid rate, can result in cerebral edema, seizures, and coma. 32
Hyponatremia, induced by exercise or sports events, has not been investigated systematically in young athletes. It is possible, for example, that the cause of muscle cramp episodes in a young athlete could be hyponatremia; however, the diagnosis may remain unconfirmed if serum sodium analysis is not performed. Apart from the hyperhydration factor, the presence of particular characteristics may increase the susceptibility of a few young athletes to hyponatremia during exercise. The American Academy of Pediatrics 93 and the National Athletic Trainer’s Association 94 have pointed to the risk of electrolyte imbalances, including hyponatremia, in young athletes with eating disorders (anorexia and bulimia with binge–purge behavior). Two other conditions that may predispose young athletes to hyponatremia caused by excessive losses of sodium from sweat and kidneys are the presence of certain mutations of the cystic fibrosis gene 32 or a renal disorder. 95 These conditions do not necessarily prevent a child or adolescent from training and becoming an athlete.
Fluid Intake Between and During Practices and Competitions: Attitudes and Knowledge
The first studies5,16,96 showed that when active children or adolescents exercise in the heat—under controlled laboratory conditions—and water is available to drink as desired, they do not fully replace their fluid losses from sweat. This behavior has been called “involuntary” dehydration. It has been suggested that involuntary dehydration occurs because of a delay in thirst perception because it is usually not triggered until a certain degree of body water deficit (1%-2%) is achieved. 40 For the pediatric population, other factors, besides thirst delay may be responsible for volume intake during exercise. When 29 children (9-13 years old) were dehydrated by cycling (three 15-minute bouts at 50% V.O2peak in the heat; 35°C, 20% relative humidity), thirst perception increased within a minimal water deficit of 100 mL and continued to gradually increase as hypohydration reached a mere 0.8%. 6 During the recovery period, these children recovered from hypohydration by drinking as desired, but the volume of fluid intake was greater with flavored beverages (grape and orange) compared with water. Another study 9 involving adolescent athletes and young adults evaluated voluntary drinking while running at similar relative exercise intensities (80%-85% of predicted maximal heart rate) at 26.5°C and 27% relative humidity. During the 1 hour of exercise to simulate aerobic conditioning, participants had access to a lemon-lime flavored sport drink (6% CHO with electrolytes). No voluntary dehydration occurred in either group, possibly because of the flavoring characteristic of the drink.
In addition to flavoring, the presence of electrolytes (mainly sodium) and CHO should also help prevent involuntary dehydration by stimulating thirst. Wilk and Bar-Or 7 studied 12 boys who cycled intermittently for 3 hours in the heat (35°C, 43% relative humidity). In 3 separate sessions, boys could drink as desired one of the following drinks: pure water, flavored water, or a flavored CHO–NaCl solution with the same taste as the flavored water. Compared with pure water, voluntary fluid intake was 45% greater when flavor was added. The addition of CHO (2% glucose and 4% fructose) and electrolytes (18 mmol L−1 of NaCl) induced a further increase in voluntary drinking, which was sufficient to avoid dehydration. A later study 97 from the same laboratory, using a similar protocol, showed the consistency of flavored CHO-NaCl beverages in preventing voluntary dehydration in boys.
In the above study, 7 boys were not acclimatized to the heat. However, heat-acclimatized children also experienced voluntary dehydration during exercise when water was provided ad libitum. 5 Rivera-Brown et al 8 examined voluntary fluid intake in trained, heat-acclimatized boys who cycled and rested intermittently for 180 minutes in the outdoor conditions of Puerto Rico (Wet Bulb Globe Temperature 30.4°C). In separate sessions, the boys drank ad libitum unflavored water or flavored water plus 6% CHO and 18 mmol L−1 of sodium. Voluntary fluid intake was 32% higher with the flavored CHO-electrolyte drink, and unlike the water session, dehydration was prevented despite the high sweat rates of the boys (~570 mL h−1). This finding has not been confirmed in “real field conditions.” When adolescent tennis players (15 years-old) trained for 2 sessions of tennis, lasting 120 minutes each, in the heat, intake of a flavored 6% CHO-electrolyte drink (~1890 mL) was not significantly greater than that of water (~1740 mL). 35 Nevertheless, the resultant dehydration level was significantly lower in the CHO-electrolyte training session (0.5%) compared with that of water (0.9%) most likely because of greater fluid retention.
Knowing attitudes about fluid intake between and during sports events may help adjust individual recommendations. The young athlete may be aware of the importance of being euhydrated and about general recommendations, but he or she may not follow such recommendations or may not know about proper amounts of fluids to be consumed.11,70,98 Recently, Kavouras et al 10 examined the effect of an educational intervention on hydration status and performance in 92 young volleyball and basketball athletes (mean age = 13.8 years) during a summer training camp in Greece. In the first week of the study, 31 children served as the controls, and in the second week, the other 61 children received an educational intervention, which consisted of: a 1-hour lecture on hydration benefits and recommendations; explanation of the urine color chart, 99 as discussed below, with copies placed at locker facilities; improvement of water accessibility; and body weight measurements before and after practices. Over a 2-day period, improvements in hydration status and in a 600-m run performance were observed. Therefore, educational programs for young athletes to comprehend hydration strategies and methods of assessing and monitoring their hydration status seem to be effective.
Practical Considerations
Methods to Identify Hydration Status
Considering the above-mentioned symptoms and deleterious effects, we do not wait for the clinical manifestations to diagnose a potential hydration imbalance. Some methods, such as a change in body mass and laboratory markers, have been useful to identify hydration status. Comprehensive and detailed reviews have described the various methods to assess hydration status in the adult population,99-102 most of which are commonly used with, and acceptable to, young athletes as well.
Change in body mass is probably the most practical method to identify acute changes in hydration status. Laboratory markers can also be used in combination with change in body mass to identify a baseline hydration status. This is particularly useful for those young athletes who participate in weight-related sports such as judo and wrestling in which the category is determined by body mass. 103 In this case, young athletes may hypohydrate intentionally. Manipulations to force hypohydration may cause adverse consequences that affect physical and cognitive performance and health.104-106 Although urinary markers, such as osmolality, specific gravity, and color, are not as sensitive to acute changes in hydration status as are blood markers, 107 they are feasible and inexpensive when compared with collecting and analyzing blood samples. Urine samples from the first void in the morning (or following 12 hours fasting) when analyzed over a sequence of days, rather than a single time before exercise, may better indicate an individual’s overall daily hydration status. The American College of Sports Medicine position stand 108 indicated as euhydration a urine osmolality ≤700 mOsmol kg−1. The specific gravity of urine can be determined using a handheld pocket refractometer. No specific reference values are known for children or adolescents, so adult values are applied, whereby values >1.020 indicate hypohydration and those >1.030 indicate significant hypohydration.99,109 The 1- to 8-level color chart is used to classify individuals as well (1 to 2) hydrated and having minimal (3-4), significant (5-6), and serious (>6) dehydration. This chart seems to be easily explained and available for self-assessment and follow-up of hydration status of an adult athlete, although the feasibility and reproducibility of children self-reporting hydration status using a urine color chart have not been investigated, at least to our knowledge. As summarized in Table 3, a number of studies4,10,11,37,66,70,79,110-112 have indicated that young and college athletes of different modalities arrive hypohydrated to their practices/competitions according to urinary markers.
Hemoglobin and hematocrit changes can also be used as indicators of hydration status, but they are more representative of plasma volume change, which can be affected by factors such as posture, use of tourniquet, and tissue osmolality. A more sensitive blood marker of body hydration changes is plasma osmolality because of its role in overall body fluid homeostasis. It has been demonstrated that once young adult athletes dehydrate to as low as 1% from exercising in the heat, plasma osmolality increases by 7 mOsm·kg−1 and keeps increasing by about 5 mOsm·kg−1 for every 2% loss of body mass. 107 Plasma osmolality is generally analyzed using the freezing point or vapor pressure depression osmometer, but such evaluations have been used mostly for research purposes rather than during practical in-field evaluation.
General Guidelines and Concluding Remarks
Given the above-mentioned factors that influence body fluid balance between and during practices and competitions, it is difficult to formulate a single hydration guideline for all young athletes. Hydration guidelines for active and athletic pediatric populations have already been published.113-115 The latest 2011 AAP Policy Statement 31 on climatic heat stress and exercising children and adolescents updates the previous APP Policy Statement 113 and reinforces that children, not specifically athletes, should have sufficient and appropriate fluid available to be consumed at regular intervals before, during, and after all sports participation. It was further advised that safety and performance could be improved if sufficient rehydration is achieved between the rest periods of same-day matches. Another recent document by the AAP 116 formulated by the Committee on Nutrition and The Council on Sports Medicine and Fitness advised that ingestion of sports drinks that contain electrolytes (also carbohydrates or protein) may benefit pediatric athletes, but only water may be necessary for the average active child. In agreement to what was discussed above, this committee further pointed to the risk of electrolyte abnormalities in those young athletes who are restricting their dietary sodium or who drink excessive amounts of water.
The consistent finding that young athletes start practices and competitions mildly hypohydrated suggests that recovery of body water losses has not been optimal. It seems that more emphasis should be given to the recovery period or between exercise bouts or games, especially under warm environmental conditions. Programs in which young athletes can learn how to recognize their hydration status combined with a favorable assessment of proper beverages should be encouraged to avoid body fluid imbalances.