
Abstract
HIV/AIDS is a serious, but preventable disease that can have improved outcomes with early diagnosis and treatment. Primary care providers are experts in prevention and early treatment. The Centers for Disease Control and Prevention has recommended that HIV testing be routinely incorporated into health care settings for patients aged 13 to 64 years. There has been much confusion and noncompliance with these recommendations. Primary care providers should understand the rationale behind these latest guidelines as well as their own states’/territories’ regulations and laws around HIV testing to embrace these latest recommendations in order to provide their patients with the best possible care.
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is a preventable disease that can easily be diagnosed and treated in primary care settings. Due to the introduction and widespread use of antiretroviral agents beginning in 1996, survival has increased and hence more people are living with HIV/AIDS as a chronic disease. The Centers for Disease Control and Prevention (CDC) estimates that more than 1 178 350 people in the United States are living with HIV. 1 Unprotected sexual intercourse, both heterosexual and homosexual, remains the leading risk factor for HIV transmission. Initially, HIV testing and diagnosis was limited to a few high-risk groups (men who had sex with men and injection drug users); however, now it is increasingly found among people without identifiable risk factors.2-6 HIV should be recognized as both an acute and chronic disease affecting both genders, occurring in both rural and urban settings, and, in addition, disproportionately affecting underrepresented minorities.
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is a preventable disease that can easily be diagnosed and treated in primary care settings.
Routine testing for HIV may help reduce the impact of the current HIV/AIDS epidemic. Routine HIV testing is defined as the offering of HIV tests to all sexually active patients, without an initial risk history and without pretest counseling. Routine testing also adheres to the general rule that anyone who is, or has been, sexually active is presumed to be at risk for HIV and should be tested at least once in their adult lifetime. Importantly, it is offered irrespective of the race, ethnicity, or sexual orientation of the patient. The goal of routine testing is to identify HIV early in the course of the disease and link those who have been diagnosed to effective medical care. The benefits of HIV testing have been shown even in lower prevalence settings.7,8 Several studies have demonstrated that knowledge of one’s HIV infection status can reduce subsequent high-risk behaviors and hence secondary transmission.9-11 Thus, routine HIV testing in primary care practices can lead to (a) enhanced personal health of patients through earlier diagnosis and/or improved awareness of protection strategies, (b) improved public health by reducing transmission, and (c) increased economic productivity of patients by reducing medical expenses through providing earlier, more cost-effective preventive care.
HIV is a prevalent, preventable, and treatable chronic disease. As such the impetus is on primary care providers (PCPs) to “normalize” HIV testing, making it a routine part of preventive care. The role of PCPs includes promoting the awareness, education, diagnosis, management, and treatment of disease. 12 This article aims to guide PCPs in the current epidemiology, diagnosis, and early management of HIV/AIDS. It also addresses routine HIV testing and methods to better incorporate CDC recommendations into primary care practices. Specific regimens of medication therapy are beyond the scope of this article but can easily be accessed at http://www.aidsinfo.nih.gov.
Epidemiology
Although the first case of HIV was diagnosed in 1982, there still remains significant stigma among the general public and a knowledge gap among many PCPs about HIV diagnosis, prognosis, and management. Both patients and their doctors frequently underestimate their risk for HIV.13-15 Nationally from 1996 to 2005, HIV incidence was stable at 40 000 cases/year, but in 2006, improved surveillance documented incidence closer to 56 300 new HIV infections annually.16,17 HIV/AIDS is also becoming more prevalent in rural areas and among younger individuals.
HIV is an infectious disease that can be transmitted to others, but it can also be easily identified and treated in the early stages of the disease. However, despite previous testing recommendations by the CDC, a little more than half of the adults in the United States have been tested for HIV.18,19 Current standards of most practicing physicians do not include routine HIV testing.14,20-23 This low compliance is due to several factors. The diagnosis of HIV or AIDS continues to evoke anxiety among patients and their loved ones. In addition, because of the nature of the risk factors (ie, sexual and illicit drugs) associated with HIV transmission, many PCPs are also uncomfortable with, or hesitant to, spontaneously introduce the subject of HIV testing with their patients.24-27 To address this screening gap, in 2006 the CDC advocated routine HIV testing in all health care settings for adolescents and adults 13 to 64 years of age. 28 This testing policy change served to reduce both the real and perceived barriers associated with HIV testing. These barriers include the lack of perception of risks by both the PCP and the patient, the lack of time allotted for the risk-based counseling and to complete additional paperwork, as well as the lack of training addressing the diagnosis and management of HIV/AIDS.
Routine testing does not mean that the HIV testing is coercive or mandatory. It encompasses general medical consent (ie, patients are told they will be tested for HIV unless they decline) as adequate consent for HIV testing. Oral or written information should include an explanation of HIV infection and the meaning of a positive or negative test result. Patients should be provided an opportunity to ask questions and to decline testing for HIV. With such notification, consent for HIV screening should be incorporated through the patient’s general informed consent for medical care on the same basis as other screening or diagnostic tests; a separate consent form for HIV testing is therefore not required. The CDC continues to recommend offering pretest information to patients. 29 CDC no longer recommends that specific or interactive counseling about personal risks and risk reduction except in the case of high risk patients, who should continue to receive, or be referred for, pretest counseling.
Several studies have shown that patients are more likely to be HIV tested when their health care providers offer the test.14,21-23 Therefore, when PCPs do not offer HIV testing to their patients, it likely results in a loss of access to early and appropriate lifesaving treatment. Follow-up for HIV care may also occur more readily when obtained in primary care settings.
The natural history of HIV is that it takes 10 years, on average, to develop AIDS if no medical intervention is undertaken. Many persons are asymptomatic and may appear physically well during this decade. During this interval the CD4 count, which is a measure of the integrity of the immune system, can drop from a normal value of around 500 to an immunocompromised value of less than 200. Current recommendations suggest initiating antiretroviral treatment (ART) for HIV at or below a CD4 count of 350. 30 Patients who drop below the cutoff value of 200 require antimicrobial intervention in addition to ART to prevent the development of opportunistic infections (OIs). The lower the CD4 count drops below the 200 value, the worse the prognosis and the longer it takes for the immune system to recover.
HIV testing is an important prerequisite to identify the patient’s HIV status as positive. HIV testing is performed by identifying antibodies to HIV. Antibodies develop in most cases within 2 to 6 weeks after exposure to the virus but may occasionally require as long as 6 months to manifest. Testing by laboratories are done using ELISA technology and, if positive, repeated twice prior to confirming the result with Western blot analysis. The tests are highly sensitive and specific and, in addition, have been shown to be cost effective. Tests can be performed on saliva, urine, whole blood, and/or serum. Many practices are now increasingly adopting the rapid test for the detection of HIV antibodies. When using the rapid test, results can be processed in 20 minutes. However, if reactive, a confirmatory Western blot test will need to be done. All screening for HIV should be done using tests that detect antibodies to HIV; viral load testing and T cell counts should not to be employed for making the diagnosis of HIV but rather for managing the patients once in treatment.
If the results of the HIV test are negative, patients should be encouraged to start employing or continue to employ safe sex behaviors and avoid illicit substances. If the patient does engage in high-risk activities, risk reduction for these specific activities should be reviewed and the patient should be retested for HIV infection in 3 to 6 months. The possibility of a false negative and the window period, or the length of time that the virus takes to mount an antibody response that will be detected by the HIV test, should also be explained to the patient. This is especially important for patients who are tested when they have flulike symptoms, which may be associated with initial acquisition of HIV infection.
If the results of the HIV test are positive, patients should be evaluated to assess their current and past mental and psychological health status. The evaluation for the newly diagnosed or new-to-care HIV-positive patient is relatively straightforward and can be effectively performed by the PCP, even if she or he does not plan to continue to manage the patient, prior to referral for specialty care. HIV primary care is very similar to the level of care primary care doctors offer their non-HIV-infected patients (see Table 1). The initial evaluation includes assessing the patients’ signs and symptoms with increased attention devoted to weight loss, diarrhea, fever, night sweats, fatigue, dyspnea, and rash. The patient’s emotional health as well as their social support systems and networks should also be assessed at the first and each subsequent visit.
Initial Evaluation of the HIV-Positive Patient for Primary Care Providers
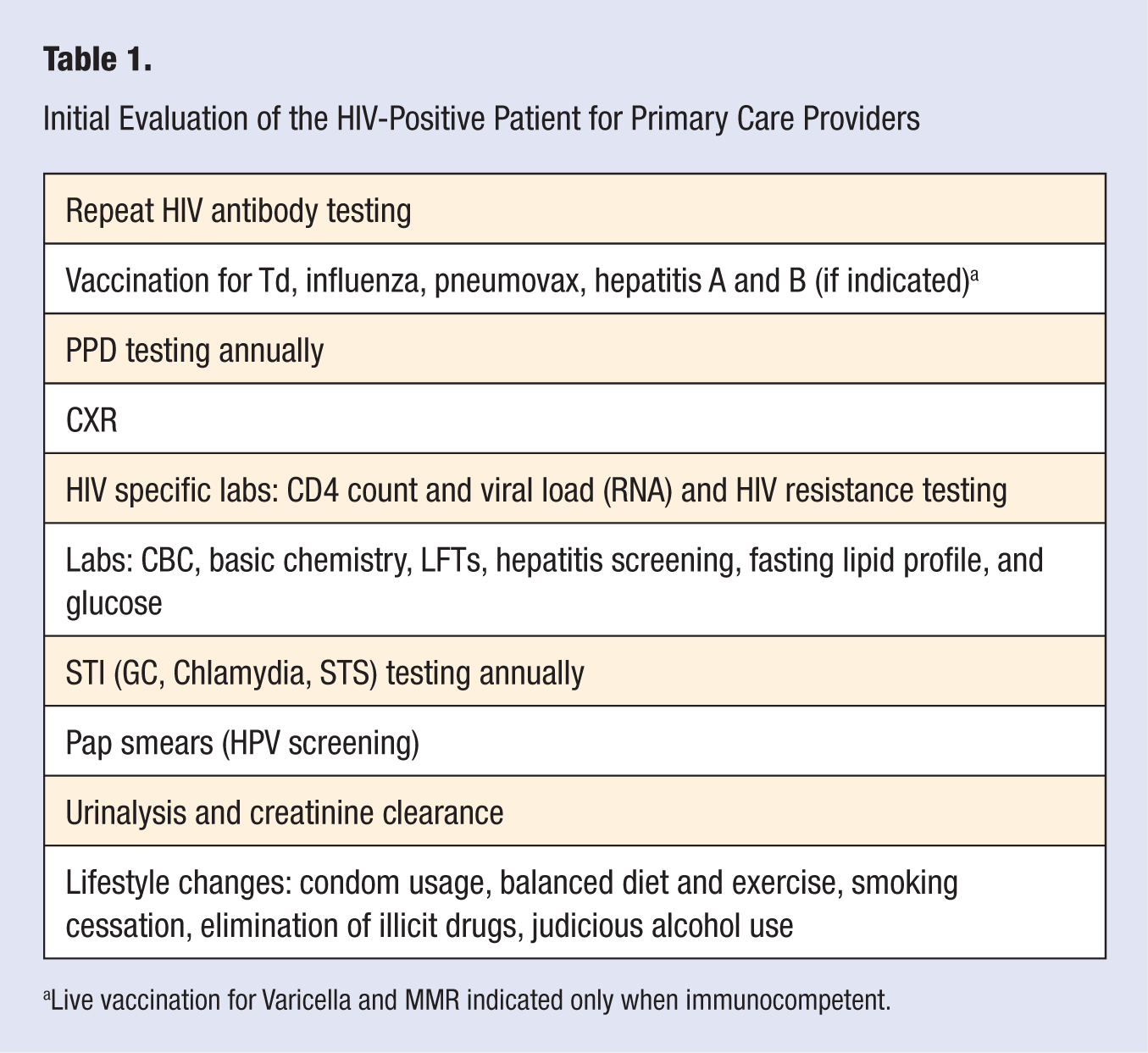
Live vaccination for Varicella and MMR indicated only when immunocompetent.
Labs
The first lab to be drawn when a patient tests positive for HIV is a repeat HIV test (ELISA and Western blot) in order to confirm the diagnosis. Other HIV-specific labs include CD4 count to assess the patient’s immune status, plasma viral load to assess the amount of viral replication, and resistance panel or genotype assay to detect mutations in the virus. Other recommended labs for the workup of HIV infection assist in the diagnosis and evaluation of anemia, thrombocytopenia, hepatitis, syphilis, hepatic and renal function, metabolic status, and sexually transmitted infection screening. A chest radiograph, PPD testing, and, if female, with or without a uterus, a pap smear are indicated. Inactivated vaccinations (ie, influenza and pneumovax) may be administered to the patient without regard to CD4 count; however, live immunizations, such as the Varicella and MMR vaccines, should be timed to coincide with the recovery of the immune system.
Initiating ART medications is never an emergency. Patients who are pregnant, have HIV-associated neuropathy or nephropathy, hepatitis B, a history of an AIDS-defining illness such as chronic diarrhea, Candida, or unexplained fever and weight loss should be started as soon as possible. Patients must be assessed for their mental readiness and willingness to start antiretroviral medications to control progression of HIV. Once started, ART compliance is a lifetime commitment. Many of the parallels of initiating insulin therapy are invoked, as there are frequently many myths and anecdotes that need to be addressed with the patient, even prior to addressing the benefits and the side effects of both these important medications. The most important message to stress is that the patient must be compliant and that ART needs to be taken as directed. Resistance is more likely to develop if multiple doses of the medication are missed or taken incorrectly. Resistance can also develop if even 1 or 2 drugs from the 3 or 4 drug regimen are not taken. This requires close monitoring of the side effects and the timing of the medications by the prescriber. Current medication guidelines, complete with side effects, can be found from the Department of Health and Human Services or the International AIDS Society–USA Web sites.30,31 In general, 2 nucleoside analogue reverse transcriptases combined with either a protease inhibitor or a nonnucleoside analogue reverse transcriptase inhibitor is recommended. A new class of antiretroviral therapy, integrase inhibitors, is becoming more popular among HIV specialists. In addition to discussing dosage, timing, and side effects of the medications, it is important to have a conversation with the patient about the role of ARTs in reducing the transmission of the virus when used in conjunction with latex condoms. If allergic to latex, polyurethane condoms can be substituted.
PCPs should be familiar with the class side effects of ART medications. The nucleoside/nucleotide reverse transcriptase inhibitors can cause lactic acidosis, lipodystropy (loss of subcutaneous fat or abnormal fat accumulation), and hyperlipidemia. The nonnucleoside reverse transcriptase inhibitors are responsible for neuropsychiatric symptoms, rash, liver toxicity, and lipid abnormalities. The protease inhibitors can cause gastrointestinal symptoms, as well as glucose and lipid abnormalities. In addition, since many of the drugs are metabolized by the cytochrome P450 system, drug interactions are to be expected. Caution should be exercised with concomitant use of ART with anticonvulsants, cardiac medications, contraceptives, proton pump inhibitors and phosphodiesterase type 5 inhibitors, and herbal and hormonal medications. Common medications used to treat HIV and their specific side effects are shown in Table 2.
Select Medication and Side Effects
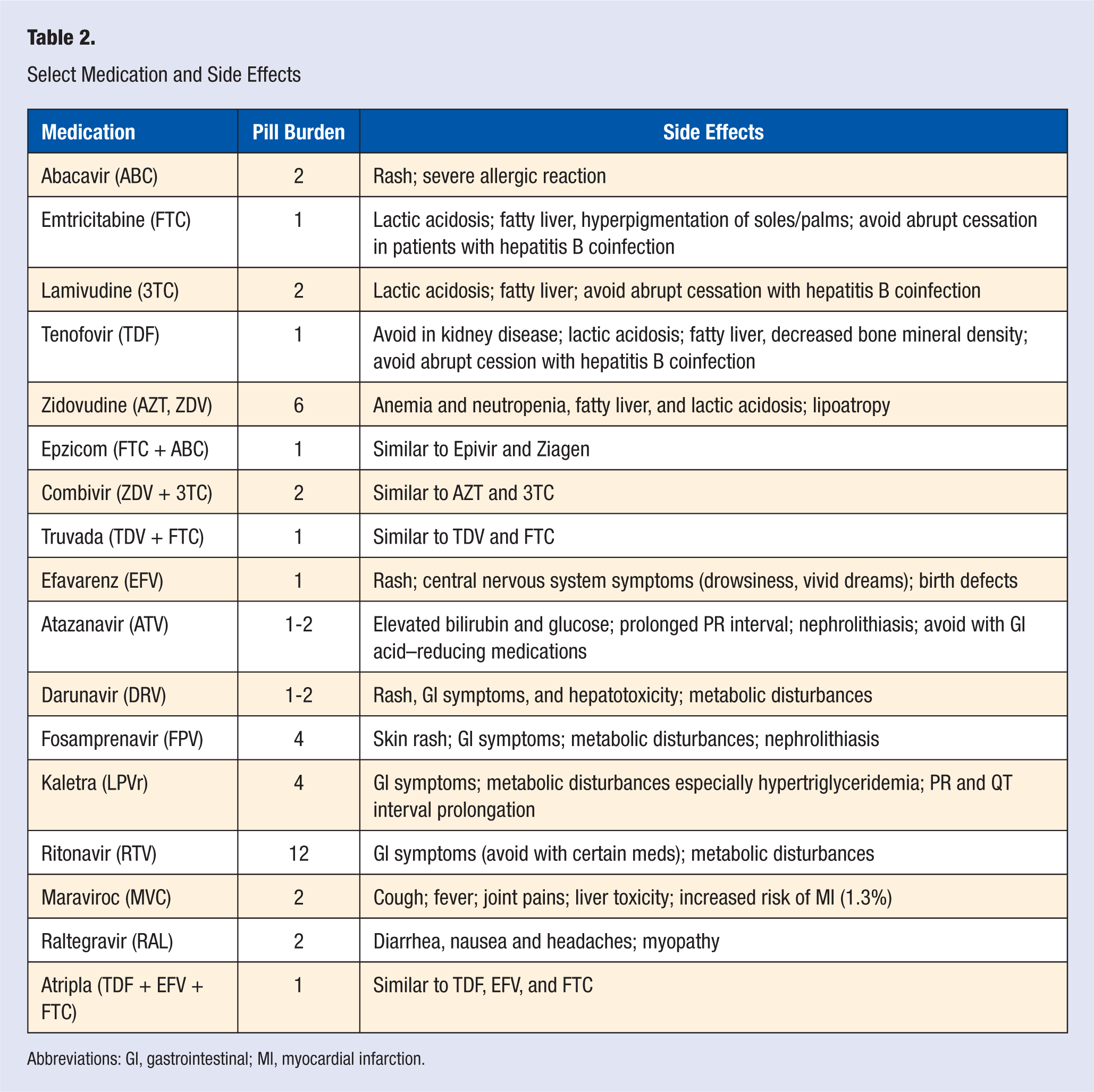
Abbreviations: GI, gastrointestinal; MI, myocardial infarction.
When the CD4 count drops below 200, initiating appropriate prophylaxis for opportunistic infections is crucial. At this CD4 level, daily or thrice weekly trimethoprim-sulfa or a suitable alternative to prevent Pneumocystis jirovecii should be initiated. The patient should also be evaluated for other opportunistic infections. At CD4 levels below 100, toxoplasmosis is more likely to occur and Mycobacterium avium complex can occur below a CD4 count of 50 (Table 3).
Timing of Initiation of Medications to Prevent Opportunistic Infections
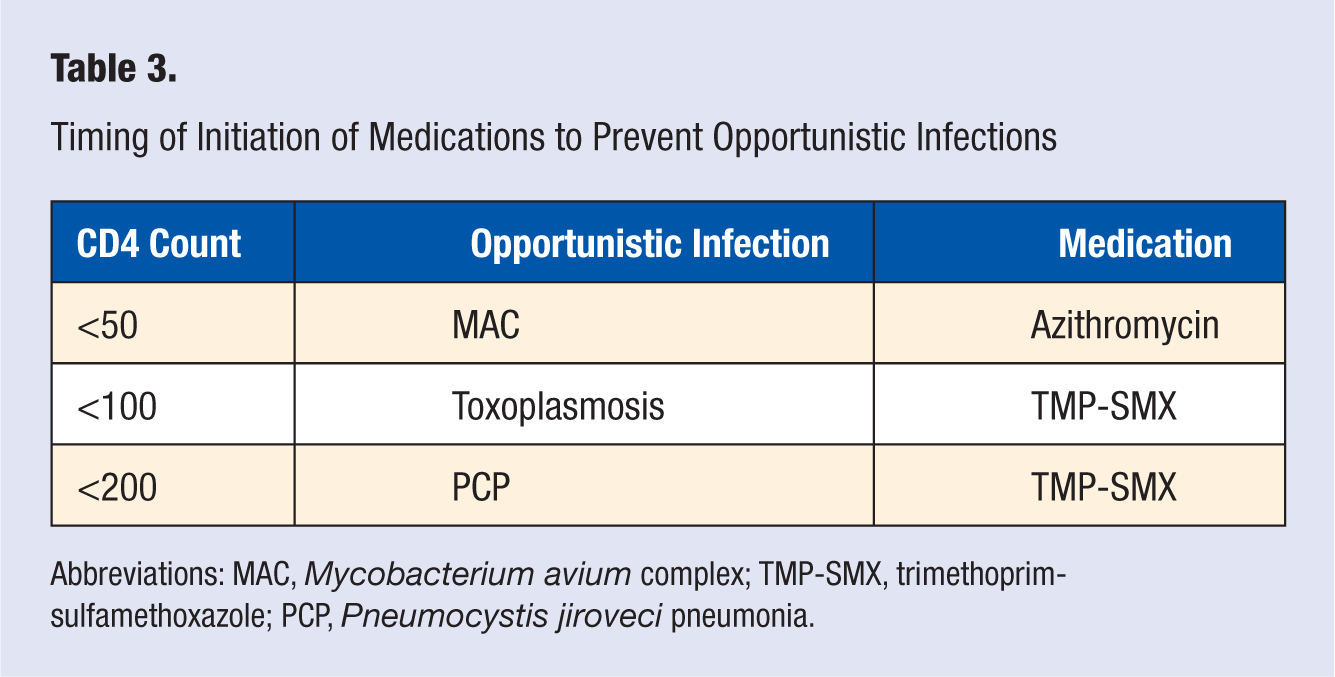
Abbreviations: MAC, Mycobacterium avium complex; TMP-SMX, trimethoprim-sulfamethoxazole; PCP, Pneumocystis jiroveci pneumonia.
Primary care doctors are in an optimal position to care effectively for patients with HIV. Many of the same diseases need to be followed in those patients living with HIV/AIDS as in noninfected individuals. Metabolic complications such as lipodystrophy, lipid abnormalities, insulin resistance or impairment, avascular necrosis, and premature osteoporosis have been associated with HIV disease. Patients should be assessed and monitored for osteoporosis and cardiovascular disease as well as diabetes. Alcohol, smoking, and substance use, if present, should be addressed with the patient and strategies for reduction and/or elimination should be suggested. Continued reminders about the importance of adherence and protection of their sexual and needle sharing partners is required.
Conclusion
For PCPs to optimally do their jobs of health promotion and disease prevention, routine HIV testing must be incorporated into their practice at least once for all our sexually active patients. The testing of and education of patients about their risks for HIV infection is important for prevention of further infection and longer healthier lives of those living with HIV. Because the primary care setting is a point-of-care testing site, HIV screening and diagnosis in this setting should seamlessly increase the number of HIV infected people who are linked to appropriate medical and social services.