
Abstract
Intake of carbohydrates above the dietary guidelines to support performance of physical activity is common but may be unnecessary and counterproductive. Sports nutrition guidelines have not been designed to incorporate characteristics that may make high carbohydrate consumption a source of metabolic stress that may increase oxidative stress, inflammation, and lipogenesis. This metabolic stress is linked to the physiology underlying the development of insulin resistance, type 2 diabetes mellitus, and cardiovascular diseases. This review describes research-based evidence to aid in bridging the gap between dietary guidelines for overall health and those to support physical activity. Characteristics that increase the likelihood of metabolic stress resulting from carbohydrate intake include overweight and obesity, central/visceral adiposity, older age, sedentary lifestyle, and caloric state. Carbohydrate-based foods that provide the most health benefits are whole grains, beans and legumes, fruits, and vegetables. Carbohydrate-based foods that most readily elicit metabolic stress are those with added sugars and refined grains or that have a high glycemic index. A checklist that incorporates both the number of these characteristics and prevailing guidelines for nutrition and physical activity is presented. This may be useful in determining whether additional carbohydrates are needed to support the physical activity level of the individual.
Introduction
The aim of this review is to present research-based evidence to aid in bridging the gap between dietary guidelines for overall health and the carbohydrate intake guidelines to support physical activity. There are a limited number of situations in which addition of carbohydrate above the level suggested by dietary guidelines provide benefit for the performance of physical activity. Additionally, promotion of extra carbohydrate intake and or carbohydrate supplements as necessary for exercise and physical activity may be counterproductive and potentially harmful in many individuals exercising for health benefits. According to the Dietary Guidelines for Americans 2010 report, soda/energy/sports drinks as a category ranks as the third and fourth in the list of top 25 sources of calories for children and adolescents and for adults, respectively. 1 Although the extent to which these carbohydrate drinks are consumed for the perceived purpose of supporting physical activity and exercise is not known, these statistics highlight the urgency of being able to differentiate situations in which added carbohydrates provide benefit from those in which they are potentially harmful. The focus of this article will be on individuals without known metabolic or cardiovascular disease who need guidance regarding carbohydrate intake. In the absence of guidelines, using a checklist of both the situations in which carbohydrate intake above daily recommended intakes have demonstrated benefits (pluses) and the situations in which carbohydrate intake may elicit undesirable effects (minuses) may be a useful approach to guide carbohydrate recommendations for individuals performing physical activity to obtain health benefits.
There are a variety of situations in which consumption of carbohydrates can induce potentially harmful physiological effects such as oxidative stress, inflammation, or fatty acid synthesis.
Regular physical activity is associated with reduction in risk for many diseases, including cardiovascular diseases and type 2 diabetes mellitus (T2DM). Physical activity may reduce disease risk via several mechanisms, including, but not limited to, anti-inflammatory effects, antioxidant effects, obesity reduction, improved glycemic control, and improved lipid profiles.2,3 Inflammation interferes with insulin signaling and may promote insulin resistance (IR) and risk of T2DM.4,5 Inflammation also plays a role in the progression of atherosclerotic plaque formation as part of coronary artery disease.4,6,7 Oxidative stress enhances inflammation 8 and mediates the microvascular damage induced by hyperglycemia. 9 Excessive adipose storage, particularly ectopic lipid storage, or storage of lipids in unwanted locations, is an outcome of obesity that alters metabolism to increase inflammation, promote dyslipidemia, and promote IR. Lipid profiles characterized by high triglycerides (TGs) or LDL and low HDL levels are atherogenic and more likely to occur when IR is higher. 10 Thus, the potential impact of increasing physical activity on the lowering of many disease risk factors is tremendous.
There are a variety of situations in which consumption of carbohydrates can induce potentially harmful physiological effects such as oxidative stress, inflammation, or fatty acid synthesis. Given that many health benefits are gained from the opposing influence of physical activity on these physiological effects, it seems likely that the benefits of exercise may be lessened by carbohydrate ingestion in some situations. Criteria to be considered when evaluating the potential for adverse effects to occur with carbohydrate intake include type of carbohydrate to be consumed, BMI, adiposity deposition location, age, caloric state relative to caloric balance, and recent physical activity. Unfortunately, a great deal of additional research is needed to more accurately characterize the standards or cutoffs for each of these criteria relative to the potential benefits or harms of carbohydrate ingestion. Nevertheless, an attempt will be made to organize the available information as a starting point for further development in this area.
Dietary Guidelines for Carbohydrate Intake and Quality
There are several sources for general recommendations to guide individuals in developing a healthy and balanced diet. 11 The recommended dietary allowance (RDA) is the minimum amount of nutrient needed to prevent deficiency symptoms in 97% to 98% of people. Dietary reference intake (DRI) is the amount of a nutrient needed to maintain health. The RDA for carbohydrate (for all but infants or pregnant or lactating women) is 130 g/d, with a DRI of 45% to 65% of the energy in the diet from carbohydrate, and no more than 25% of total energy in the form of added sugars. It is important to note that 130 g/d for a 2000 calorie diet would be approximately 26% of energy from carbohydrates and fall well below the DRI as a percentage of energy intake. To achieve this DRI, the specific recommendations for food groups with substantial carbohydrate content in a 2000 calorie diet of 6 ounces of grains (at least half of these should be whole grains), 2.5 cups of vegetables, 2.0 cups of fruit, and 3.0 cups of low-fat dairy products are recommended by the USDA through the MyPlate recommendations (http://www.choosemyplate.gov/). 12 Acquiring carbohydrates across this recommended distribution of foods also aids in the intake of an appropriate balance of protein, fat, fiber, vitamins, phytonutrients, and minerals.
Nutrient density has to do with the amount of vitamins, phytochemicals, and minerals contained in a food relative to the number of calories. As sources of carbohydrate, whole grain products, legumes, fruits, and vegetables are examples of carbohydrate-rich foods with high nutrient density. Sugar-sweetened sodas and other soft drinks, many sports drinks, and many energy drinks are examples of high-carbohydrate foods with low nutrient density.
Glycemic index (GI) and glycemic load (GL) are additional key properties when considering the quality of carbohydrate consumed relative to the amount of physical activity performed. The rate of digestion and appearance of glucose in the blood influences the GI. Specifically, GI is the relative proportion of the blood glucose area under the curve for ingestion of 50 g of available carbohydrate for a specific food as compared with a reference food of either white bread or glucose. Foods with less than 55% of the area under the reference curve have a GI of 55 or less and are generally low GI foods, whereas those with more than 70%, with a GI of 70 or greater, are at the higher end of the GI spectrum. The primary factors that influence GI are the type of carbohydrates within the food, the amount of fiber in the food, and the overall macronutrient content of the food. For example, the starch amylose is digested more slower than the starch amylopectin, so foods with higher amylose/ amylopectin ratios typically have lower GI. Fiber slows gastric emptying and digestion in the small intestine; thus, higher fiber content is often associated with a lower GI. Fat and protein slow gastric emptying, so foods with high content of these nutrients relative to carbohydrate often have lower GIs. The GI of a food has special reference to the amount of food consumed that contains 50 g of available carbohydrate (fiber is not available carbohydrate). The GL is used to account for the amount of carbohydrate in the amount of food actually consumed: that is, GL is the GI of the food times the amount of available carbohydrate consumed. For example, cooked carrots have a higher GI but a low amount of available carbohydrate; thus, the GL for carrots is low. Evaluation of the dose of carbohydrate and the impact of the foods consumed requires attention to GL as well as GI. 13
Cross-Sectional and Longitudinal Studies Relating to Carbohydrate Quantity and Quality
A number of prospective longitudinal studies of carbohydrate intake and cardiovascular diseases (CVDs) or diabetes risk have produced a mixture of findings. Variables to be considered when evaluating the epidemiological evidence relating to carbohydrate quality are GI and GL, nutrient density, amount of processing for grains, and the amount of fiber. In many studies, it is difficult to determine the independent effects of each of these variables. For example, GI and GL are associated with higher levels of TG, LDL, and C-reactive protein (CRP; a marker of systemic inflammation) and lower levels of HDL in the blood within the Nurse’s Health Study. 10 Incidence of diabetes also differed within this study with a 1.59-fold increase in risk for individuals in the highest compared with the lowest GI quintile. 14 Diets with higher proportions of low-GI, slow carbohydrate foods are associated with a lower risk for a number of conditions and diseases, including CVD, T2DM, age-related macular degeneration, and cataracts in the preponderance of prospective investigations. 13 For example, relative risk or odds ratios for the highest versus lowest quintiles of dietary GI ranged from 1.15 to 1.47 across 7 prospective studies (Chiu et al 13 ). Diets with lower GL are also associated with lower risk for T2DM. One of the physiological benefits of fiber is to lower the GI of many foods; however, a number of studies have been able to establish a lowering of T2DM risk for lower GI diets that is independent of fiber. 13
Foods with added sugar have an increased caloric density and a lowered nutrient density, as the addition of sucrose and other common sweeteners such as high fructose corn syrup add calories but not nutrients. With respect to added sugars and health risks, a scientific statement from the American Heart Association in 2002 concluded that longitudinal studies have produced equivocal findings owing to the many confounders, such as increase in body mass, but shorter-term studies have convincingly demonstrated that sugar consumption lowers HDL and raises TG levels. 15
Meeting Carbohydrate Needs to Support Physical Activity and Exercise
Relative to the dietary guidelines for average individuals, there are 3 broadly defined situations in which an increase in carbohydrate intake provides benefit to the physically active individual. Specifically, increased carbohydrate intake is beneficial when it (1) enhances exercise or physical activity performance, (2) enhances beneficial adaptations to exercise or physical activity, or (3) decreases the risk of overreaching or overtraining. For the purposes of this article, information will be presented to identify current sports nutrition recommendations most relevant to the majority of individuals. This is being presented to convey the criteria for recommending carbohydrates in excess of dietary guidelines. There are many position statements and extensive reviews that provide excellent guidelines for athletes and individuals with very high levels of physical activity, and there is also the research evidence supporting the key points presented in the present review.16-21
Individuals exercising or performing physical activity to improve health often are likely to have enough carbohydrate available to meet their performance needs simply by following dietary guidelines for average individuals. Three sources of glucose to working muscles during physical activity include (1) glycogen in muscles, (2) glucose synthesized or released from storage in the liver, and (3) glucose ingested and absorbed during the physical activity. The ability to perform exercise or physical activity decreases if glycogen levels become low. As muscle glycogen levels reach lower levels, glucose delivery to working muscles can be increased with carbohydrate ingestion. Thus, it is important to identify the situations in which (1) addition of carbohydrates above average recommended intake is needed to ensure adequate glycogen levels during exercise and (2) carbohydrate intake during physical activity will improve performance. Carbohydrate recommendations that are particularly relevant to individuals exercising for health benefits or recreational sports performance from a collection of expert sources and position statements are given in Table 1.
Carbohydrate Recommendations for Individuals Exercising for Health Benefits or Recreational Sports Performance
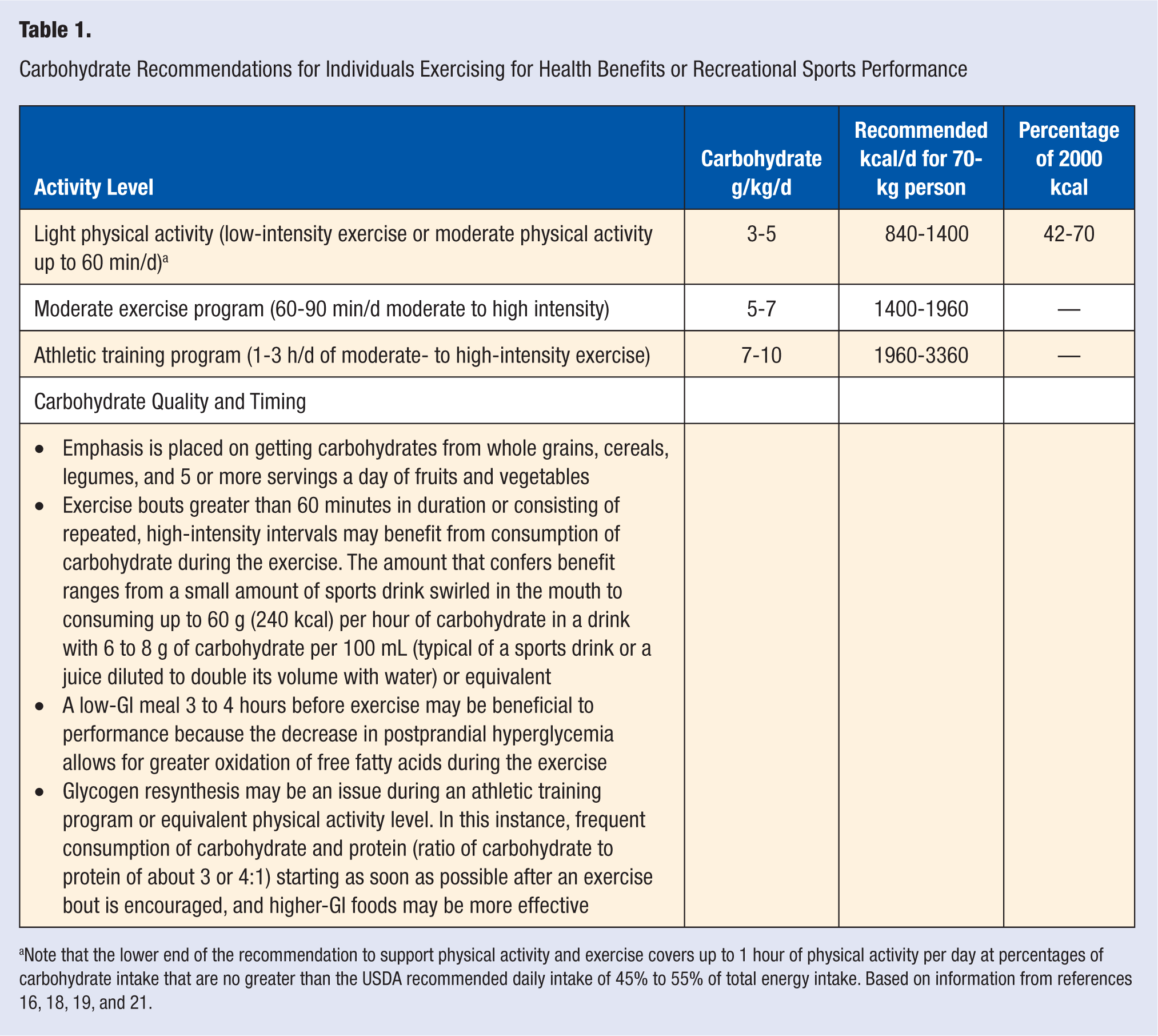
Note that the lower end of the recommendation to support physical activity and exercise covers up to 1 hour of physical activity per day at percentages of carbohydrate intake that are no greater than the USDA recommended daily intake of 45% to 55% of total energy intake. Based on information from references 16, 18, 19, and 21.
Potentially Harmful Effects of Carbohydrate Consumption
The primary focus of this article is to review the evidence relating to possible negative consequences of carbohydrate intake in adults without known disease. In many instances, these are the same situations that should be avoided by individuals with known metabolic pathology or CVD; however, the goal is to highlight potential pitfalls that apply to health maintenance and disease prevention. The criteria to be considered include type of carbohydrate to be consumed, BMI, adiposity deposition location, age, caloric intake relative to energy balance, and physical activity status. Generally speaking, the potentially negative consequences attributed to carbohydrate intake occur in situations when the glucose from carbohydrate elicits one of the following effects: (1) an increase in oxidative stress, (2) an increase in inflammation, and (3) an increase in fatty acid synthesis. The primary goal with respect to dietary carbohydrate intake is to supply energy, and the specific instances when carbohydrate intake above the DRI is needed have already been identified. Evidence will be presented in the following section to establish a list of situations in which individuals should be particularly careful to avoid excess carbohydrate.
Glucose-Induced Increases in Oxidative Stress and Inflammation
The capacity for glucose ingestion to increase oxidative stress and trigger proinflammatory pathways has been clearly established using the oral glucose tolerance test (OGTT) protocol of ingesting 75 g of glucose. 22 This equates to 300 kcal of glucose in 1 bolus, or 15% of a 2000 kcal/d diet, or about 1/4 to 1/3 of the DRI for carbohydrate in 1 bolus. In other words, the amount of glucose ingested via an OGTT is somewhat comparable to the ingestion of a high-GI food with 300 kcal of available carbohydrate.
Oxidative stress results from the high oxidation rate of glucose in the mitochondria of cells exposed to high blood glucose concentrations. The reactive oxygen species (ROS) linked to a high flux of electrons through the mitochondrial electron transport system when glucose is high is the superoxide radical. 8 This increase in ROS is a common trigger for several consequences, including (1) activation of proinflammatory transcription factors (nuclear factor [NF]-kB, activator protein–1), (2) decreased bioavailability of nitric oxide (NO), which promotes vasoconstriction/increased blood pressure and prothrombotic effects, (3) increased advanced glycation end products (AGE) such as glycosylated hemoglobin (HbA1c), (4) increased polyol formation, and (5) increased hexosamine.8,9,23 The latter 3 (AGE, polyols, and hexosamine) are associated with diabetic hyperglycemia. However, the increase in ROS and inflammation has been demonstrated in a variety of nondiabetic situations, including in normal-weight, healthy, young adult individuals.23-25 Furthermore, a common property of a wide group of drugs that lower progression from impaired glucose tolerance to T2DM is an antioxidant effect, and given the fact that oxidative stress plays a role in the development of IR with overfeeding, dysfunction of β-cells, endothelial cell dysfunction, and other components of T2DM pathology, some researchers suggest that oxidative stress is the “common soil” underlying promotion of T2DM and CVD. 26
A number of inflammatory mediators participate directly in the pathological development of CVD, T2DM, and other conditions and diseases ranging from macular degeneration, to Alzheimer’s disease, to cancer.4,27,28 An increase in oxidative stress induces activation of NF-kB, which promotes gene expression of a wide range of inflammatory proteins, including TNF (tumor necrosis factor)-a and IL (interleukin)-1β. These 2 cytokines have direct effects on and interfere with insulin signaling5,29,30 and have positive feedback effects to amplify production of themselves and other proinflammatory molecules that attract and activate inflammatory leukocytes (adhesion molecules, chemokines, and enzymes). 31
Postprandial hyperglycemia is a risk factor for the development of CVD that should be considered in the discussion of combining diet and physical activity to have the greatest impact on disease risk reduction. The term postprandial dysmetabolism refers to large elevations in either glucose or TGs in the blood following a meal. Whereas fasting glucose depends on insulin sensitivity of the liver and insulin secretion by the pancreas, glucose tolerance following ingestion of glucose depends on both suppression of hepatic glucose output and insulin action on peripheral tissues—predominantly skeletal muscle but also adipose. 32 The prevalence of impaired fasting glucose is 1.5- to 3-fold greater in men compared with women. The prevalence of impaired glucose tolerance is greater in men than in women and increases with age. 32 There is an association between 2-hour post–glucose challenge glycemia levels and risk of cardiovascular disease events in individuals with normal glucose tolerance.33-36 In a study of postmenopausal women with coronary artery disease and normal glucose tolerance, 2-hour postchallenge glucose levels (<87 to 140 mg/dL) correlated with the progression of changes in coronary artery lumen diameter. 37 Elevations in blood glucose, even when artificially induced in healthy individuals with no underlying metabolic limitations, elicits atherogenic responses such as oxidative stress, decreased prostacyclin, glycosylation of proteins, increased coagulability, and other effects. 38
One interpretation of these research findings may be that potential negative health consequences stemming from consumption of carbohydrates extends beyond individuals who are known to have impaired fasting glucose levels and includes many people who are likely to be unaware of their postprandial dysmetabolism. An alternative explanation simply may be that the metabolic changes that underlie the postprandial dysmetabolism correlate with disease progression. More research is needed in this area; however, evidence is accumulating to elicit caution regarding, and perhaps to discourage, consumption of extra carbohydrates unless individual needs to support high physical activity levels are clearly demonstrated.
Carbohydrates and Lipogenesis
There are multiple routes for stimulation of fatty acid synthesis by the liver. The end result of high levels of hepatic fatty acid synthesis is hepatosteatosis, hypertriglyceridemia, and hepatic IR. 39 Overnutrition in the form of excess energy is one means of activating a key step for fatty acid synthesis—induction of the sterol regulatory element–binding protein (SREBP). 39 Insulin is capable of activating fatty acid synthesis through this same pathway. 40 Diets rich in carbohydrate, sugars, and saturated fatty acids are strong inducers of SREBP-1c, the isoform of the binding protein that stimulates gene expression of enzymes (acetyl-CoA carboxylase, [ACC], fatty acid synthase, and others). 39 Hepatic fatty acid synthesis may be stimulated by glucose via a carbohydrate responsive promoter region in the genes for ACC and fatty acid synthase. 41 At the lowest carbohydrate end of the dietary spectrum, Volek et al 42 showed that compared with a low-fat diet with a similar caloric deficit, 12 weeks of a very low carbohydrate, ketogenic diet resulted in a greater decrease in body mass, TG, and insulin levels. Although there is some disagreement about the ideal level of carbohydrate in the diet, it is generally accepted that the combination of higher carbohydrate intake with caloric excess can lead to hepatic lipogenesis, which can lead to elevations in blood TGs, ectopic accumulation of fat in the liver, and hepatic IR.
Factors to Consider When Determining Likelihood of Harmful Effects
Carbohydrate Quality
The inflammatory effects of carbohydrate occur primarily when high-GI carbohydrate is ingested. In the absence of attention to carbohydrate quality, carbohydrate intake of 25% compared with 45% of total energy controlled for 6 months in overweight women did not influence inflammation, as evidenced by CRP levels. 43 The proposed mechanism for activation of inflammation by carbohydrate intake, particularly high-GI carbohydrate intake, is that a surge in glucose elicits production of superoxide radicals by mitochondria. The mean amplitude of glycemic excursions is associated with measures of oxidative stress, for example, 8-iso-prostaglandin F2a. 44 Consumption of high-GI diets is associated with plasma indicators of oxidative stress in healthy adults (n = 292). 45 Demonstrated consequences of large postprandial increases in glucose eliciting oxidative stress and inflammation include endothelial dysfunction, hypercoagulability, and sympathetic hyperactivity. 38 Many people with normal fasting glucose levels have postprandial hyperglycemia. 38
Surges in blood glucose can be avoided by decreasing the overall GI of the diet, and there is evidence that lower-GI carbohydrate diets effectively eliminate the proinflammatory consequences of glycemia. Particularly relevant to the argument that high-GI carbohydrates are not needed unless physical activity levels are high is the study by Dickinson et al. 24 They measured increased mononuclear cell NF-kB protein levels, the key transcription factor to induce transcription of proinflammatory cytokines, in mononuclear cells collected from young, healthy, lean men after ingestion of 50 g of carbohydrate either as glucose, white bread, or pasta. Furthermore, the GI of the glucose and white bread was greater than that of a low-GI pasta, and the researchers reported 3-fold greater NF-kB levels with the high-GI foods. Kelly et al 46 found that production of proinflammatory cytokines in older, obese adults after 12 weeks of endurance training with a diet of 55% to 58% carbohydrate was enhanced for those with a high GI intake and decreased for those with a low GI intake. In support of this relationship, Liu et al 47 measured a positive association between dietary GL and plasma CRP concentrations in healthy, middle-aged women. Additionally, Fleischman et al 48 demonstrated that anti-inflammatory treatment with salsalate improved postprandial glycemia in obese, young adults.
Fructose is a monosaccharide with a low GI, and has been considered as a possible alternative to glucose as a means of lowering dietary GI. However, this may be counterproductive because fructose is rapidly taken up by the liver for conversion to glucose, fatty acid, or lactate. This has a net effect of increasing esterification of fatty acids at the expense of oxidation, thereby promoting TG formation and an increase in hepatic VLDL production. For this reason, it is recommended that fructose intake does not exceed 20% of dietary energy. 49 Segal et al 50 proposed the need for a “fructose index” and limiting the amount of fructose in the diet as a means of preventing atherogenic dyslipidemia. The main sources of fructose in the diet are table sugar (half glucose half fructose); high fructose corn syrup, ranging from 42% to 55% fructose; fruits; and honey. Additionally, sports drinks typically are a mix of carbohydrates that include fructose.
High dietary fructose has been shown to elicit IR at doses of 250 g/d for 1 week and about 216 g/d for 28 days, but not 100 g/d for 28 days.51-53 Phosphorylation of fructose by the enzyme fructokinase in hepatocytes lowers and may deplete adenosine triphosphate (ATP) levels and result in increased production of uric acid. 50
Body Mass Index (BMI)
The association between inflammation and body mass index has been consistently measured across many studies.54,55 Reduction in BMI reduces basal levels of many inflammatory markers, including CRP.43,56 Healthy, obese individuals have higher levels of inflammation (IL-6 and CRP), free fatty acids, and TGs compared with nonobese individuals. 57 This is true for overweight compared with normal-weight children and adolescents also. 58 Thus, the relationship between obesity and inflammation is independent of age.
Stimulation of oxidative stress and inflammation by carbohydrate ingestion is lower in people with a lean BMI, but it can occur with higher-GI carbohydrates. Gonzalez et al 22 measured suppression of lipopolysaccharide (LPS)-induced inflammation by mononuclear cells in lean but not obese women. There is evidence that normal-weight individuals who are physically active are able to increase insulin sensitivity in response to a high-GI challenge, whereas sedentary, obese individuals (based on pretraining data) increase insulin secretion to bring glucose levels back to homeostasis levels.59-61 Normal-weight individuals with a BMI ≤ 25 kg/m2 typically do not respond to glucose intake with increases in oxidative stress or inflammation.62,63 However, Dickinson et al 24 demonstrated that the inflammatory transcription factor NF-kB increased in mononuclear cells of young, healthy, lean men in response to consumption of 50 g of high-GI carbohydrates.
Visceral Versus Subcutaneous Adiposity
Adipose tissue is considered an endocrine, proinflammatory tissue that, in proportion to the amount of adipose in the body, releases several proteins that decrease insulin sensitivity in animal models; these are elevated in people with T2DM also and include adipsin/ acylation stimulatory protein, resistin, TNF-a, IL-6, macrophage and monocyte chemoattractant protein 1, plasminogen activator inhibitor 1, and angiotensinogen. 64 Also, many of these proinflammatory proteins are produced by macrophages, and an additional component of inflammation related to adipose tissue is that inflammatory macrophages infiltrate adipose tissue to increase the adipose-derived level of inflammation. 64 Adipose tissue in the abdominal cavity with the viscera is a determinant of reduced insulin sensitivity and has a higher level of inflammatory activity compared with subcutaneous adipose tissue.65,66 Stimulated production of inflammatory cytokines from mononuclear cells during hyperglycemia was associated positively with the percentage of truncal adipose in both men and women.67,68 Loss of visceral adipose tissue in obese and overweight women resulting from a diet and exercise intervention was an independent predictor of improvements in glucose use and insulin sensitivity. 69 Conversely, accretion of visceral adiposity with increasing age has been implicated in the development of IR. 70
Age
There are changes associated with increasing age that increase the likelihood of postprandial hyperglycemia and or IR. A decrease in pancreatic β-cell function is associated with aging. 71 Furthermore, an increase in IR has been measured in association with the increase in visceral adiposity that occurs with aging. 70 There is some debate as to the influence of the loss of muscle mass on the decrease in glucose tolerance that occurs with aging, but the accumulation of visceral adipose tissue appears to have a significant role in the development of age-associated decreases in glucose tolerance. 70 In a large cross-sectional investigation, Abbatecola et al 72 found that inflammation and IR increased with age, independent of central adiposity and BMI. Thus, a decrease in glucose tolerance with increasing age is well established, whereas the underlying mechanism is less clear.
Exercise that results in muscle damage elicits an inflammatory response. Experimentally induced hyperglycemia following muscle damaging exercise increased glucose oxidation in younger but not older men who were normal weight and had normal glucose tolerance. 71 This decrease in oxidation, coupled with the acute increase in IR and decrease in glycogen resynthesis, 73 might increase the likelihood of a greater glycemic response after carbohydrate ingestion in older men after strenuous or eccentrically biased exercise.
Caloric Intake Relative to Caloric Balance
Overnutrition in the form of a positive caloric balance promotes oxidative stress and inflammation, 62 liver fatty acid synthesis, 39 and accumulation of lipid inside muscle cells, a factor contributing to IR in nonathletes. 74 Increased insulin and IR were measured in young, healthy, lean men who overate, having a high-calorie, high-fat diet and reduced physical activity for 4 weeks. 75 Caloric restriction to promote a caloric deficit for 1 to 7 days decreases ROS generation and related oxidative stress markers in both normal-weight and obese individuals.76,77
Physical Activity Status
Compared with physically active individuals, sedentary individuals have a greater postprandial increase in glucose, insulin, and TGs. 78 There are several physiological effects of physical activity that promote healthy glucose homeostasis or offer protection from hyperglycemia or its consequences. For example, there is an insulin-independent increase in glucose uptake during exercise. 79 Endurance training, independent of fat loss, decreases oxidative stress, increases endogenous antioxidant defenses, decreases TNF-a, and increases insulin sensitivity.80,81 Thus, there are physiological benefits of regular physical activity that reduce the likelihood of carbohydrate-induced metabolic stress.
Physical activity and exercise have anti-inflammatory effects. Severe exercise can induce inflammation either from tissue damage or from increased gut permeability to endotoxin.82,83 However, these effects are acute and not typical of most physical activity and exercise bouts. There is a substantial anti-inflammatory effect of physical activity and exercise derived from the release of IL-6, a cytokine and myokine that has anti-inflammatory actions, from contracting skeletal muscle. 27 Although associations of IL-6 with IR have been reported, infusion of IL-6 does not directly influence glucose disposal. 30 Based on the findings of several studies of overweight and obese children or adolescents, Rubin and Hackney 84 concluded that increasing levels of physical activity are associated with lower levels of inflammation in the presence of obesity. This is consistent with the research findings for obese adults.81,85
Influence of Carbohydrate and Physical Activity on Glucose Homeostasis and Inflammation
Research relating to carbohydrate intake and exercise training to improve glucose homeostasis and reduce inflammation is limited, but there is growing evidence that attention to carbohydrate quantity and quality influences the benefits of physical activity. It is important to note that there has been little if any research to determine the efficacy of carbohydrate intake strategies to optimize exercise or sports performance in overweight or obese individuals.
One of the research models used to study acute interactions between physical activity and inflammation or IR is exercise-induced muscle damage. Muscle damage, typically elicited with either high-force eccentric (resistance to muscle lengthening) exercise or downhill running, causes a transient increase in inflammation and IR that lasts for about 2 days postexercise.71,86-90 Thus, high-force eccentric exercise and downhill running may be used as research models to induce muscle inflammation and IR, so that nutritional mediators of these events can be studied. Using this model to study the effects of high carbohydrate intake during recovery from eccentric exercise, researchers measured increases in plasma IL-1β and IL-6 in response to high carbohydrate intake: 75% carbohydrate, 15% fat, and 10% protein at a carbohydrate level of 1.45 g/kg at each of 3 meals during the first 8 hours following high-force eccentric exercise. 87 This intake equated to an intake of approximately 0.54 g of carbohydrate per kilogram per hour. However, carbohydrate-induced inflammation increases were not measured in a previous study with a lower postexercise carbohydrate intake of 0.25 g of high-GI carbohydrate (sports drink) per kilogram of body weight per hour over and above a calorically balanced background diet of 50% carbohydrate, 30% protein, and 20% fat. 86 Thus, the level of high-GI carbohydrate needed to augment exercise-induced inflammation in young, healthy individuals may be between 0.25 and 0.54 g/kg/h, or 70 to 151 kcal of high-GI carbohydrate per hour for a 70-kg person. At 3 g carbohydrate per kilogram of body mass during the first 3 hours following high-force eccentric exercise, Ross et al 91 measured increases in intramuscular mRNA for IL-6, IL-18, and monocyte chemotactic protein-1 to further these findings by demonstrating that inflammatory cytokine production is linked to muscle tissue.
There is an interaction between BMI and the inflammation and insulin responses to carbohydrate and fat during recovery from eccentric exercise. In a comparison of high-carbohydrate to high-fat diets following eccentric exercise, Miles et al 92 found that there was a positive association with the magnitude of increase in inflammation, insulin, and the homeostatic model assessment of IR (HOMA-IR) with BMI and waist to hip ratio in the high-carbohydrate condition. These relationships were inverted for the high-fat condition, although not as strong. In this study, and in a more recent study using downhill running (Miller et al, unpublished data 2011), there were decreases in HOMA-IR in low-BMI and increases in HOMA-IR in higher-BMI individuals, such that the line of best fit crossed 0 at a BMI of roughly 25 to 26 kg/m2. We infer from this that inflammation and IR increase in response to ingestion of high-GI carbohydrate roughly at the lower end of the overweight BMI classification—that is, well below the level for obesity. These findings are consistent with previous findings by Gonzalez et al 22 and Kirwan et al 67 that lean but not obese men and women were able to suppress glucose-induced increases in LPS-stimulated inflammation and IR. These findings are also consistent with those of Adochio et al 93 who showed that a high-fat diet increased and a high-carbohydrate diet decreased IR in lean individuals.
Research to determine how carbohydrate influences the beneficial effects of exercise training in apparently healthy individuals is limited; however, benefits of low-GI compared with high-GI diets have been demonstrated. Isocaloric and fiber- and macronutrient-matched diets differing only in high versus low GI over 12 weeks of aerobic training, having similar weight loss and gains in aerobic fitness, had different effects on glucose homeostasis in obese, prediabetic individuals. 94 Exercise training and weight loss elicited improvements in insulin sensitivity that were independent of GI of the diet. This was also true in a separate study of the same design but with only 7 days of diet and exercise. 61 However, only the low-GI diet condition elicited improvements in hyperinsulinemia, an effect that was mediated by the gut-derived hormone glucose-dependent insulinotropic polypeptide. That is, the low-GI diet resulted in a measurable reduction in β-cell stress, an important effect to prevent the development of T2DM. Conversely, exercise training with a high-GI diet resulted in impaired β-cell function, apparently mediated by gut production of glucose-dependent insulinotropic polypeptide. Further research using this same research model determined that the glycemic and inflammation responses to an OGTT were attenuated in the low- versus high-GI condition. 46 Thus, the pattern identified from these studies is that loss of body mass and improvements in IR are somewhat independent of the GI of the background diet; however, improvements in β-cell function and lowering of inflammatory responses occur only when the exercise training is combined with a low-GI diet. Although these studies focused on individuals with compromised glucose metabolism, they provide a reasonable basis for recommending caution regarding consumption of high-GI carbohydrate supplements to aid in exercise training, particularly in older and obese individuals. That is, in the absence of additional research to determine age and BMI cutoffs for which dietary GI may be safely ignored, the safest approach may be to err on the side of the low-GI diet.
Sytematic Approach to Link Dietary Guidelines for Health to Guidelines for Carbohydrates to Support Physical Activity
Evidence has been presented to indicate that caution is warranted when adding extra carbohydrate to the diet to support physical activity. Specifically, evidence has been presented to support the following key points:
In most instances, low-GI diets support physical activity as well as or better than high-GI diets and are less likely to induce oxidative stress and inflammation and increase blood lipids.
The following characteristics increase the likelihood of response to carbohydrate intake with surges in blood glucose, oxidative stress, or inflammation: overweight and obesity, central/visceral adiposity, older age, physical inactivity, and caloric excess.
More research is needed to establish nutrition guidelines to support physical activity and sports performance for individuals who are overweight or obese, have central/visceral adiposity, or are older.
There are 2 very important points to emphasize to keep this information in proper perspective. The first point is that carbohydrate-based foods with fiber, whole grains, and high nutrient density are healthy carbohydrate sources to be eaten according to dietary guidelines. Carbohydrates with low nutrient density and or high GI are less desirable and not necessary to support physical activity in most instances. For example, consumption of whole grains, legumes, fruits, and vegetables with lower GI, and avoidance of highly processed foods containing extra sugar or high-fructose corn syrup is recommended. 95 The second key point is that the overarching principle for optimal nutrition is that carbohydrate is 1 of 3 macronutrients, and there are many micronutrients to be considered. Fat types and sources are equally important. For example, diets favoring monounsaturated, polyunsaturated, and n-3 polyunsaturated fatty acids over saturated and trans fatty acids confer health benefits related to obesity, IR and T2DM, and CVD. 95
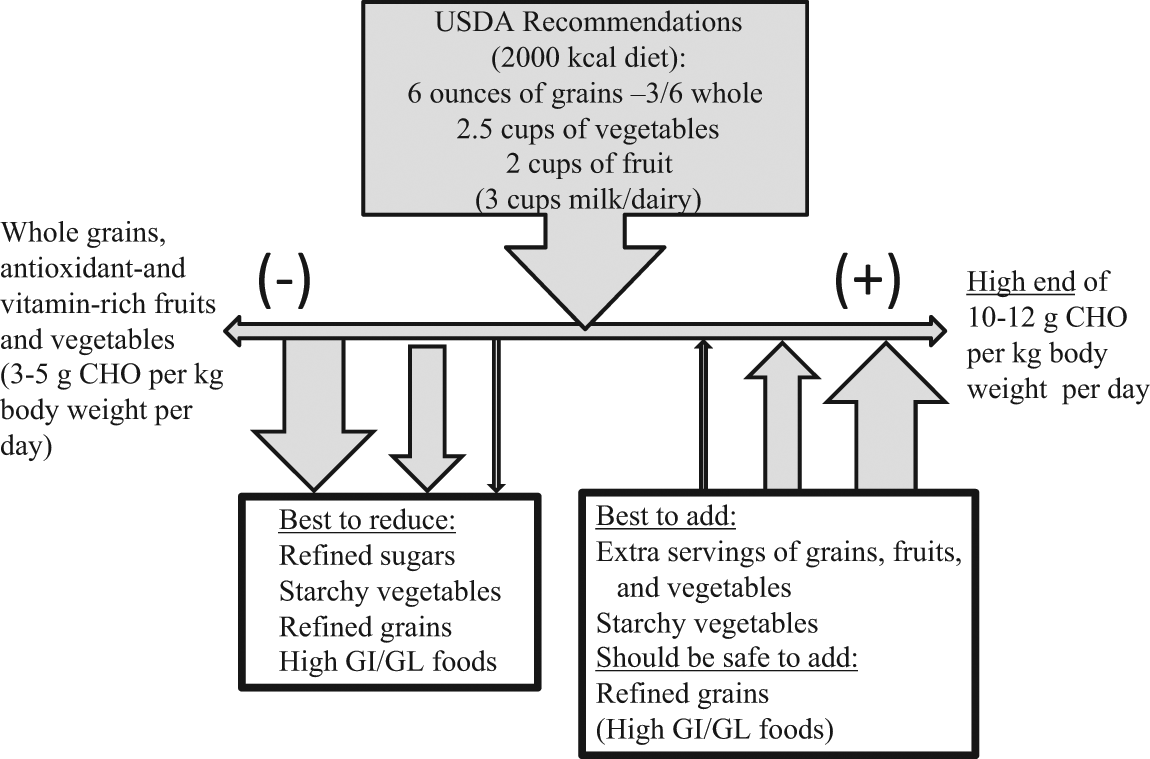
As a means of converting the findings of existing research into a practical tool that may be useful in conceptualizing and informing personal decisions or professional recommendations regarding carbohydrate intake to support physical activity without being counterproductive to health outcomes of that activity, a checklist has been developed (Table 2). As a starting point, add the checkmarks for the positives and subtract the checkmarks for the negatives. The net score is used to guide decision making regarding the amount and type of carbohydrate that most appropriately matches the chronic physiological state of the individual to the amount of physical activity performed, as further described in Figure 1. If the net score is 0, then it is suggested that no deviation from recommended levels for each food group is needed. If the net score is negative, then it is suggested that intake of carbohydrate-containing foods be restricted to only the nutrient dense, low-GI foods, particularly whole grains, low-GI fruits, and vegetables. The more negative the net score is, the greater the likelihood is that intake of refined sugars, starchy vegetables, refined grains, and other low-nutrient-density, high-GI foods will have a negative health impact. If the score is positive, then addition of carbohydrate may be warranted to support physical activity without jeopardizing health benefits. The more positive the net score is, the lesser the likelihood that high-GI carbohydrates and carbohydrate-rich foods with low nutrient density will be counterproductive to health benefits. Although these latter foods might be beneficial to support high-level athletic performances and other extremely demanding physical activities, it is still prudent for most individuals to choose the nutrient-dense, lower-GI carbohydrate foods to the greatest extent possible.
Checklist of Characteristics to Guide Carbohydrate Intake
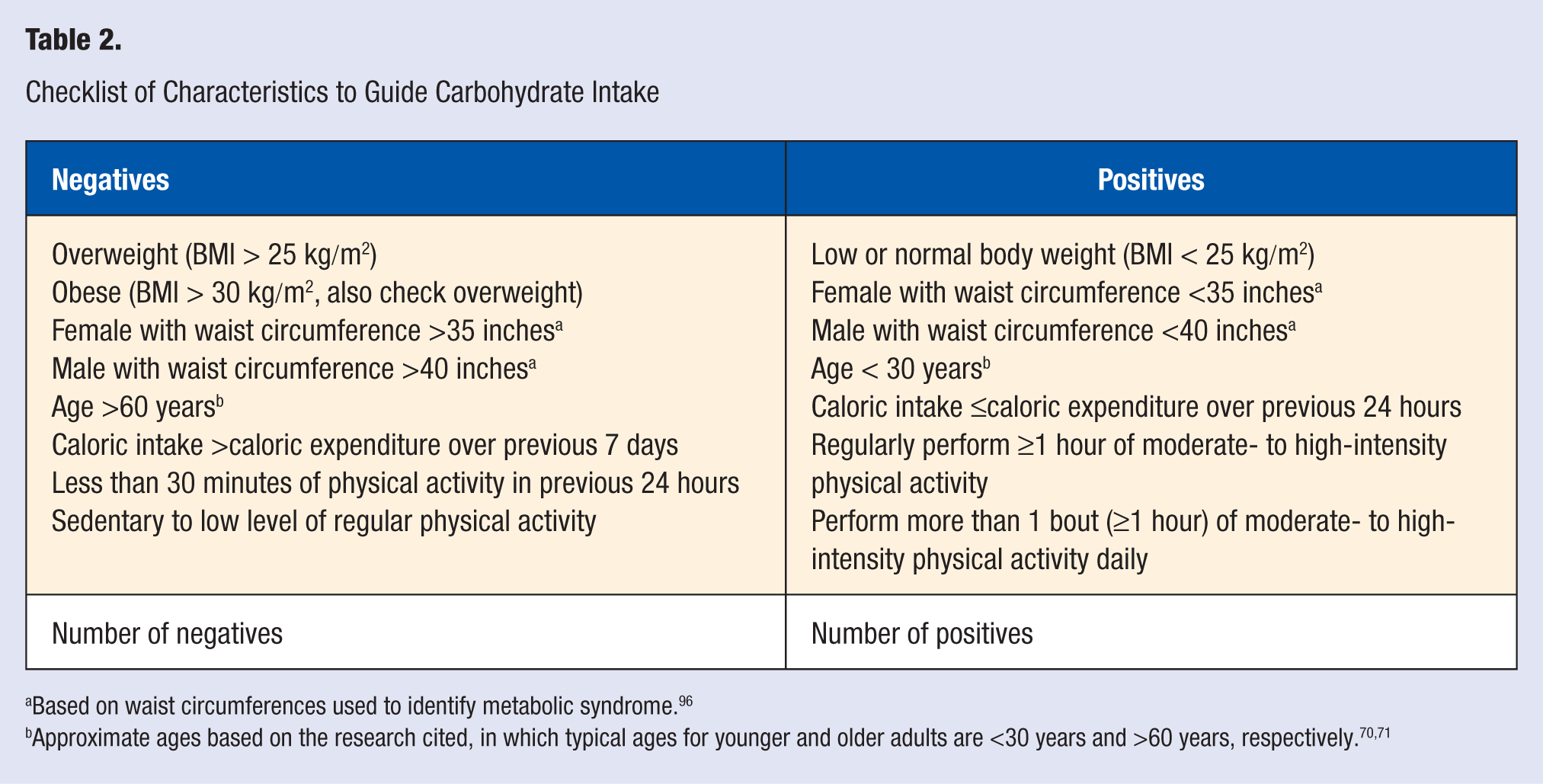
Based on waist circumferences used to identify metabolic syndrome. 96
The Net Score of the Positives (+1 for Each Positive Characteristic) and Negatives (−1 for Each Negative Characteristic) May Be Useful to Determine Whether There Are More Factors Favoring or Discouraging the Need for Addition of Carbohydrates to the Base Diet to Support Physical Activity. People With Net Scores Near 0 (±1) May Do Best at the Dietary Recommendations; Those With Large Negative Scores Should Be Cautious With Carbohydrate Intake and Focus Primarily on the Healthiest of Sources, and Those With Large Positive Scores Are Not Likely To Experience Negative Health Consequences From Adding Carbohydrates to Their Diets to Support Higher Levels of Physical Activity. Research Is Needed to Test This Model. However, the Model Is Based on Available Research to Date and May Serve as a Starting Point to Guide Healthy Individuals Make Decisions Regarding Carbohydrate Intake.
Footnotes
Acknowledgements
This work was supported by grants from the American Heart Association, ADVANCE, and the Helyn McGown Endowment at Montana State University. A portion of this work was presented as a tutorial lecture at the American College of Sports Medicine 2011 Annual Meeting and the Second World Congress on Exercise is Medicine, Denver, June 3, 2011.