
Abstract
Motor vehicle crashes during pregnancy are the leading cause of traumatic fetal mortality and serious maternal injury, morbidity, and mortality in the United States, injuring approximately 92 500 pregnant women each year. Little is known about the circumstances surrounding these crash events and the maternal characteristics that may increase women’s vulnerability to crash-related injuries during pregnancy. Even less is known about the effects of crashes on fetal outcomes. Crash simulation studies using female anthropomorphic test devices and computational models have been conducted to better understand the mechanisms of maternal and fetal injuries and death resulting from motor vehicle crashes. In addition, several case reports describing maternal and fetal outcomes following crashes have been published in the literature. Only a few population-based studies have explored the association between motor vehicle crashes and adverse maternal and/or fetal outcomes, and even fewer have examined the effectiveness of seat belts and/or airbags in reducing the risk of these outcomes. This article reviews what is presently known about motor vehicle crashes during pregnancy, their effects on maternal and fetal outcomes, and the role of vehicle safety devices and other safety approaches in mitigating the occurrence and severity of maternal crashes and subsequent injuries. In addition, this article suggests interventions targeted toward the prevention of crashes during pregnancy.
Injuries during pregnancy not only result in adverse maternal outcomes, but even minor maternal injuries can be life threatening to the fetus.
Epidemiology of Crashes During Pregnancy
Motor vehicle crashes during pregnancy are all too common. In the United States, the annual crash rate for pregnant women has been estimated as at least 13 per 1000 person-years as compared with 26 crashes per 1000 person-years among nonpregnant women. 1 Although most state-specific crash rates among pregnant women are unknown, there are 3 states that have conducted population-based studies to estimate their pregnancy crash rates: Pennsylvania, Utah, and Washington State. In Pennsylvania and Utah, the motor vehicle crash rates were 1.1% (between 2002 and 2005) and 2.8% (between 1992 and 1999), respectively, among pregnant drivers, with a fairly even distribution of crashes across trimesters.2,3 In Washington State, the motor vehicle crash rate for pregnant front seat occupants (ie, drivers and passengers) between 2002 and 2005 was 1.3%, with the majority of crashes occurring during the second trimester. 4 Weiss and Sauber-Schatz 3 suggest that the differences in these statewide motor vehicle crash rates during pregnancy may be a result of several state-specific factors, including birth rates, the mean maternal age during pregnancy, and the variation in age-specific crash risk for women of reproductive age.
Motor Vehicle Crashes and Maternal Outcomes
Motor vehicle crashes are the leading cause of hospitalized injury and injury-related death during pregnancy in the United States.5-10 Each year, approximately 1 million women in the United States, aged 15 to 44 years, are injured, and 6,130 women die as a result of motor vehicle crashes. 11 Although the number of pregnant women injured in motor vehicle crashes in the United States has been estimated to be more than 92 000 annually, this number is likely an underestimate because many crashes are unreported, and pregnancy status may be unknown, especially early in pregnancy. 12 In the United States, the rate of injury from motor vehicle crashes during pregnancy has risen over time. This is mainly a result of increases in exposure—that is, the increasing number of miles driven by pregnant women.1,13,14 Crashes result in many types of injuries. Minor injuries include dislocations, sprains, contusions, and open wounds. 15 However, more serious adverse outcomes are possible. Blunt and penetrating abdominal trauma from crashes during pregnancy can result in splenic rupture, uterine rupture, pelvic fractures, placental abruption, and maternal death.15-18 The severity of these outcomes depends on a variety of factors, including the gestational age at the time of injury, crash severity, and seat belt use.2,13,15,18,19
A handful of population-based studies have been conducted that examined both national and state-specific pregnancy-associated hospitalizations and emergency department visits from trauma during pregnancy.5-7,9,10,20 Although these studies described maternal injuries and death from all causes during pregnancy, motor vehicle crashes were recognized as the leading cause of maternal injury. In the United States, approximately 26% of injury hospitalizations during pregnancy resulted from motor vehicle crashes. 6 This injury hospitalization rate is similar to the motor vehicle emergency department rates reported in Utah and Massachusetts (22.2% and 27%, respectively) for pregnant women.5,9 In Washington State, the incidence of pregnancy-associated injury hospitalization was 243.4 per 100 000 live births; motor vehicle crashes were responsible for 30.4% of these injuries. 20 Pennsylvania and California reported lower rates of motor vehicle–related injury hospitalizations among women during pregnancy, with rates of 227 injuries per 100 000 person-years in Pennsylvania and 67 prenatal injuries per 100 000 deliveries and 8 injuries to women at delivery per 100 000 deliveries in California.7,10
In addition to the studies that examined injury hospitalizations and hospital emergency department visits from all causes during pregnancy, a few population-based studies3,15,19,21 focused on adverse maternal outcomes from motor vehicle crashes. In New Mexico, Schiff et al 19 examined maternal death records between 1986 and 1995 and found that motor vehicle crashes accounted for 70% of all injury-related maternal deaths. Among the women who died, 77% were not wearing seat belts at the time of the crash. 19 A second study conducted by Schiff and Holt 15 in Washington State described the types of injuries sustained by pregnant women who were hospitalized following a motor vehicle crash. Among the 393 pregnant women who sustained crash-related injuries, those who were severely injured (ie, those with an Injury Severity Score ≥9) were more likely than non–severely injured women to be hospitalized for fractures, dislocations, sprains, intracranial injuries, open wounds, and internal chest injuries. 15 In contrast, a higher percentage of non–severely injured women were hospitalized for contusions. 15 The most recent epidemiological study of motor vehicle crashes during pregnancy found that one third of the 5929 crashes during pregnancy in Pennsylvania between 2002 and 2005 resulted in minor maternal injuries, 7.5% resulted in more serious injuries, and only 1 resulted in maternal death. 3
An international population-based study estimated the incidence of maternal injuries and fatalities from motor vehicle crashes in Sweden between 1991 and 2001. 21 Based on a sample of more than 1 million pregnancies, the incidence rates of maternal injury and death were estimated as 23 per 100 000 pregnancies and 1.4 per 100 000 pregnancies, respectively, which are lower than the overall US and state-specific rates previously reported. 21 However, it must be noted that the overall crash rate in Sweden is lower than the US rate, which may explain the differences observed for pregnant women between the US and Swedish studies. 22
Motor Vehicle Crashes and Fetal Outcomes
There is a paucity of information about the effects of crashes on fetal outcomes. Given that approximately 92 500 women are injured from motor vehicle crashes during pregnancy each year, 12 more research is needed to examine the effects of these crashes and subsequent maternal injuries on fetal morbidity and mortality. Injuries during pregnancy not only result in adverse maternal outcomes, but even minor maternal injuries can be life threatening to the fetus. Specifically, traumatic injury during pregnancy, most often as a result of motor vehicle crashes, is an important cause of adverse fetal outcomes. 23 Until birth, the fetus relies on maternal survival and placental circulation for its own survival. After the first trimester, the uterus enlarges while protecting the fetus and providing nutrients, blood, oxygen, and waste exchange. When a mother sustains a traumatic injury, these functions may become impaired and can result in fetal injury or death. By the third trimester, pregnant women are at the greatest risk of early labor, placental abruption, amniotic rupture, and fetal–maternal blood transfusion, which can lead to adverse fetal outcomes such as prematurity, low birth weight, fetal distress, and fetal death.2,15,16,18,20,21 Placental abruption from severe maternal trauma is a leading cause of fetal loss and accounts for a reported 60% to 70% of all fetal deaths.24,25 Even in minor or noncatastrophic trauma during pregnancy, the risk to the fetus may be significant. Preterm labor, placental abruption, and death can occur among fetuses exposed to minor trauma.
Crash Simulation Studies
Several simulation studies of automobile crashes during pregnancy have been conducted, primarily at the University of Michigan Transportation Research Institute and the Virginia Polytechnic Institute and State University (Virginia Tech) Center for Injury Biomechanics, with an additional study conducted in Japan. These studies have used female anthropomorphic test devices (ie, pregnant crash test dummies)26-30 and computational models31-37 to better understand the mechanisms of maternal and fetal injuries and death resulting from motor vehicle crashes. More recently, researchers in France have used postmortem human cadavers as an alternative to dummies for a more “realistic” pregnant model to further examine these injury mechanisms.38,39
Anthropomorphic devices
Beginning in 1996, Pearlman and Viano developed the first abdominal insert for a female anthropomorphic test device to measure the effect of restraints on abdominal force, fetal head acceleration, and fetal head injury risk across various levels of crash severity, crash speed, and restraint position.27,28 In 2001, modifications were made to improve the size and shape of the pregnant abdomen and to implement instrumentation to better quantify the effect of abdominal forces and fetal accelerations on fetal injury and death. 26 Initial studies using these devices found that high-speed crashes increased abdominal force and fetal head accelerations, primarily with improper seat belt use. 28 In addition, airbag deployment coupled with no restraint use increased the risk of fetal head injury. The combined effect of airbag deployment and shoulder and lap belt use (ie, 3-point belt) was the most protective for a woman and the fetus. A recent study of low-impact collisions measured the anterior and posterior abdominal pressure of pregnant dummy models and how it varied by seat belt use and location of impact. It was found that in frontal impact tests, seat belts reduced peak abdominal pressure when contact was made with the steering wheel. 30 In rear impact tests, seat belts reduced secondary contact with the steering wheel. 30 In France, a study by Delotte et al 38 examined injury mechanisms during crashes using a postmortem human cadaver. This study found that lap belt loading and backrest impact may result in fetal injury. Specifically, the impact of the lap belt on the pelvic bone may lead to fetal head compression and the impact of the backrest may result in increased fetal acceleration.
Computer simulations
Computational models of pregnant occupants in motor vehicle crashes derived from anthropomorphic test devices and human models have been used to investigate the biomechanics of crashes and to assess the effects of crash speed, restraint conditions, and airbag deployment on maternal and fetal outcomes. Computer simulation studies conducted between 2002 and 2008 by Duma et al,31-34 Moorcroft et al,35,36 and Manoogian et al 37 were used to predict the risk of adverse fetal outcomes from motor vehicle crashes during pregnancy. Duma et al31,32 and Moorcroft et al35,36 found that the risk of adverse fetal outcomes and uterine strain increased with crash speed, particularly among unrestrained occupants. Specifically, Duma et al 31 found that at a speed of 13 km/h, the estimated risk of fetal death ranged from 32% for restrained pregnant drivers to 44% for unrestrained pregnant drivers. At a higher speed of 35 km/h (approximately 22 mph), the risks of fetal death increased to 89% and 100%, respectively. 31 Similarly, Moorcroft et al 36 found that at speeds of 35 km/h, the risk of serious adverse fetal outcomes exceeded 75% among unrestrained pregnant drivers. Moorcroft et al 35 further noted that uterine strain was a strong predictor of fetal injury, most likely because of placental abruption, with peak uterine strain ranging from 33% among restrained pregnant drivers with airbag deployment to approximately 61% among unrestrained drivers. In regard to maternal outcomes, the risk of abdominal injury and head trauma was the highest among unbelted drivers and lowest among restrained drivers with airbag deployment.35,36 Overall, 3-point belts in conjunction with airbags were the most effective for preventing maternal injury from motor vehicle crashes during pregnancy.
Population-Based Studies
Only a few population-based studies have examined the association between motor vehicle crashes and fetal outcomes.2,4,15,21,40 Overall, findings from 5 epidemiological studies suggest that pregnant women are at increased risk of experiencing several adverse fetal outcomes after a motor vehicle crash, particularly low birth weight, preterm delivery, and fetal death (Table 1).
Summary of Findings From 5 Population-Based Studies That Assessed the Effect of Motor Vehicle Crashes During Pregnancy on Fetal Outcomes, 1993 to 2008
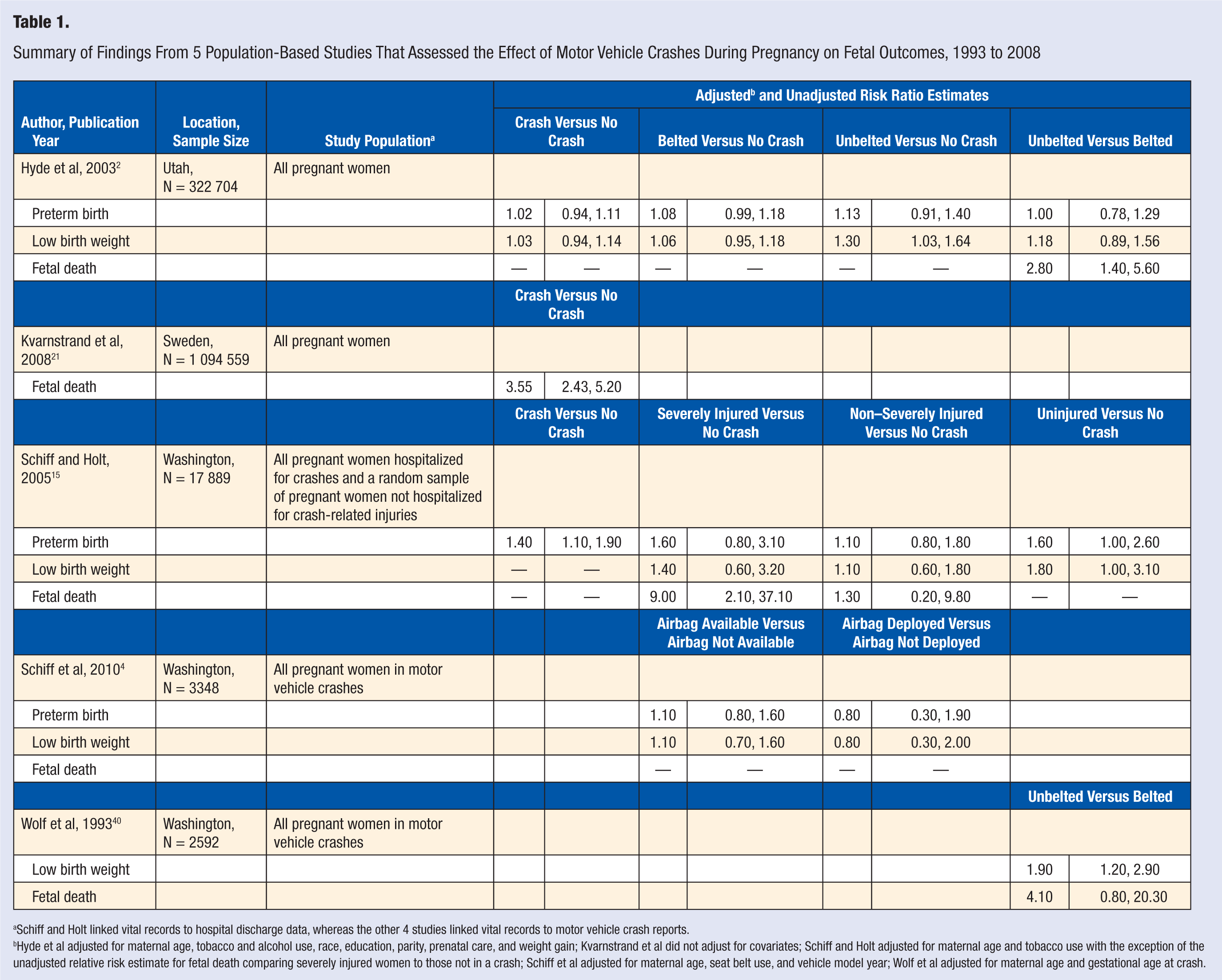
Schiff and Holt linked vital records to hospital discharge data, whereas the other 4 studies linked vital records to motor vehicle crash reports.
Hyde et al adjusted for maternal age, tobacco and alcohol use, race, education, parity, prenatal care, and weight gain; Kvarnstrand et al did not adjust for covariates; Schiff and Holt adjusted for maternal age and tobacco use with the exception of the unadjusted relative risk estimate for fetal death comparing severely injured women to those not in a crash; Schiff et al adjusted for maternal age, seat belt use, and vehicle model year; Wolf et al adjusted for maternal age and gestational age at crash.
In Washington State, Wolf et al 40 examined the effect of motor vehicle crashes and seat belt use on pregnancy outcomes and found that unbelted pregnant women in a crash had almost twice the risk of having a low-birth-weight baby and 4 times the risk of losing their fetus than belted women. A more recent study in Washington by Schiff and Holt 15 found that pregnant women hospitalized following a crash had a 40% higher risk of having a preterm baby than those not in a crash. This risk increased to 60% for women who were severely injured in the crash. 15 A third study conducted in Washington State, between 2002 and 2005, examined the subset of pregnant women who were drivers or occupants in the front seat in a crash. 4 This study found that pregnant women in a crash with an airbag available had a 10% higher risk of having a preterm or low-birth-weight baby than pregnant women whose car did not have an airbag. 4 These findings differed when assessing airbag deployment. Pregnant women who were in a crash with a deployed airbag had a 20% lower risk of having a preterm or low-birth-weight baby compared with those in a crash without a deployed airbag. 4 In Sweden, pregnant women in a crash had almost 4 times the risk of losing their fetus compared with women not in a crash during pregnancy. 21 Although these 4 studies provide important information regarding the risk of fetal outcomes from motor vehicle crashes, 1 study 15 focused on women assessed after the crash using hospital discharge data and only captured the most severe crashes, and 2 studies4,40 only focused on pregnant women who were in a crash without including a noncrash comparison group.
Given that minor injuries can significantly affect the well-being and survival of a fetus, it is important to examine the effect of all reported motor vehicle crashes on fetal outcomes, including those that did not result in hospitalization. Data regarding the impact of nonhospitalized crashes on fetal outcomes are lacking. Only 1 published US study has examined the effect of motor vehicle crashes using nonhospitalized crash data while also including a noncrash comparison group by linking police-reported motor vehicle crashes and vital records in Utah between 1992 and 1999. 2 This study found that, overall, pregnant women in a crash were not at higher risk of adverse birth outcomes than pregnant women not in a crash. However, when examined by belt status, unbelted pregnant women in a crash had a 30% higher risk of having a low birth weight baby compared with pregnant women not in a crash and almost 3 times the risk of a fetal death as belted pregnant women. 2 Although this is the only study that has linked statewide databases to explore fetal outcomes resulting from hospitalized and nonhospitalized crash victims, there are several limitations that must be addressed in future research to better assess this important public health issue. Specifically, there was no vehicle deformity information to adequately assess crash severity; there were not enough outcomes to assess interactions with gestational age; the study population was relatively small and predominantly white; and the study did not account for gestational age at the time of crash in relation to delivery or death. More research is needed to build on the Utah study to quantify the impact of motor vehicle crashes on fetal outcomes.
Seat Belt Studies
Seat belts are known to reduce occupant injury and death during crashes. Among pregnant women, studies have shown that seat belts are effective at reducing the risk of adverse maternal and fetal outcomes.2,40,41 However, these studies did not have data regarding how seat belts were worn and how proper or improper use may affect the risk of these outcomes. Police-reported crash records across all states lack information on proper seat belt use during pregnancy. The American College of Obstetricians and Gynecologists recommends that during pregnancy, women should wear seat belts properly by wearing a 3-point restraint, with the lap belt placed below the abdomen and the shoulder belt placed diagonally above the abdomen. 42 Lap or shoulder restraints alone are not suitable. As suggested in the computational models and case reports, improper restraints can result in increased risk of uterine rupture or abdominal injuries that may further result in excessive maternal bleeding and/or fetal death. A recent case series of 57 pregnant women found that improperly restrained occupants had a higher risk of adverse fetal outcomes than properly restrained occupants. 41 Using a risk curve estimated from crashes at a speed of 30 km/h, this study further estimated that there would be an 84% reduction in the risk of adverse fetal outcomes if women were properly restrained. 41
Airbag Studies
Similar to seat belts, airbags were first developed as safety devices to reduce injury and death among occupants of motor vehicles during crashes. Although the benefits of airbags have been shown among nonpregnant populations, not much is known about the beneficial effect of airbags during pregnancy. In addition, it is unknown if airbags cause injuries during pregnancy because pregnant women may be unable to maintain the National Highway Traffic Safety Administration’s recommended 10-in. distance between themselves and the airbag, particularly during the later stages of pregnancy. A review of 3 case reports in Pennsylvania suggested that airbags in combination with seat belts do not increase the risk of injuries. 43 In contrast, the findings from several other case reports have suggested that airbag deployment without seatbelt use may result in maternal and/or fetal injury or death.44-48 However, population-based studies are lacking. Only 1 state-based study has examined the effect of airbags on maternal and fetal outcomes. 4 This study found that airbag deployment did not increase the risk of several adverse fetal outcomes in crashes during pregnancy in Washington State. Given the mixed findings from the published case reports and the population-based study, more research is needed to quantify the effect of airbags on maternal and fetal morbidity and mortality. As a passive vehicle safety device, airbags require no behavioral adherence from drivers and passengers, and if effective, they can be important safety devices for preventing adverse outcomes from motor vehicle crashes during pregnancy, particularly in conjunction with 3-point restraints.
Motor Vehicle Safety Interventions
Seat Belt Practices
Given the evidence suggesting the benefits of seat belt use during pregnancy, it is important that all pregnant women wear belts and wear them properly while in a motor vehicle. In the United States, an estimated 84.1% of pregnant women (compared with 83.8% of all reproductive-age women) report wearing seat belts. 49 Several state-specific studies have been conducted to assess pregnant women’s beliefs and practices regarding seat belt use.12,49-55 Most studies found that although pregnant women report wearing belts, very few wear them properly. Women who refrain from wearing seat belts during pregnancy report that they find them uncomfortable or fear that they will cause injury to themselves or their fetus. For example, a study conducted in the early 1990s found that among 298 pregnant women in Michigan, 78% reported belt use during pregnancy. 50 Among those who reported that they rarely or never use a seat belt, almost half reported that the belt was uncomfortable, 29% never used seat belts by habit, and 16% feared hurting their fetus. 50 In regard to proper belt use, at the first prenatal visit, only 53% reported proper belt use, whereas 68% reported proper placement when asked at the third trimester visit. 50 Another study conducted in the late 1990s assessed restraint use among 807 pregnant women in California. 54 This study found that although most women (86%) reported restraint use during pregnancy, only half wore them properly. In addition, 9% believed that seat belts were harmful to their fetus. 54 A third study conducted in 2001 among pregnant patients receiving care from 1 of 8 health centers in Jefferson County, Alabama, estimated a higher prevalence of reported belt use than was estimated in other studies. 52 Approximately 96% of pregnant women reported that they wore seat belts, and 72% reported that they used belts properly. 52 Among the women who did not always wear their seat belt, the most common reasons for underuse included discomfort (53%), forgetting to wear belts (43%), or belief that belt use was not necessary (19%). 52 Other explanations for lack of belt use included inconvenience (12%), fear of injury to the fetus (12%), and fear of injury to themselves (4%). 52 A second phase of this study assessed differences in restraint use and knowledge between county clinic patients and private practice patients. 53 The authors found that a higher proportion of private practice patients used belts before and during pregnancy and used them correctly as compared with county clinic patients.
An Irish study assessed frequency and awareness of proper belt use among pregnant women in Northern Ireland between 2003 and 2004. 51 Similar to the results from the US-based studies, approximately 75% of the 154 respondents reported belt use during pregnancy while driving, and 47% reported proper belt use. 51 One third of the women reported concerns about wearing a seat belt during pregnancy, and only 22% reported that they received belt use advice during pregnancy. 51
Although the reported prevalence estimates of seat belt use across several studies indicate that most pregnant women (ie, 75% to 96%) wear seat belts during pregnancy, it should be noted that not all these women (ie, 47% to 76%) wear belts properly. In addition, among the pregnant women who reported that they rarely or never used a seat belt, a small percentage had misconceptions about the effects of belt use on themselves and their fetus. Proper education about the importance of belts and correct placement can minimize concerns and correct misconceptions that prevent women from wearing belts and can increase proper belt use. An evaluation of an educational intervention disseminated in prenatal care clinics in Alabama found that providing women with educational materials that address the importance and proper use of seat belts resulted in increased knowledge of belt effectiveness for pregnant women and fetuses, increased belt use, and increased proper placement of lap and shoulder belts. 56 Earlier studies evaluating the effectiveness of educational interventions in childbirth classes and in obstetric clinics had similar findings.54,57 One intervention resulted in increased frequency of seat belt use, 57 and the other resulted in improved belt placement. 54
As recommended by the American College of Obstetricians and Gynecologists, all pregnant women should receive prenatal seat belt counseling. 42 However, this is usually not the case. Very few pregnant women report that they receive prenatal counseling about belt use.12,49,50,52,54 A multistate study conducted across 22 states found that the prevalence of reported prenatal counseling about belt use ranged from 38% (Arkansas) to 59% (Washington State). 12 This range is consistent with the findings from several prenatal clinic-based studies. For example, in Michigan, approximately 55% of women who completed a survey at 2 prenatal visits (n = 298) reported that they received information about belt use from their health care provider. 50 In Alabama, only 37% of the 450 women who completed surveys at their prenatal visits reported that they received information on belt use during pregnancy. 52 In California, even fewer women (21%) reported that they received information on proper belt use from their health care provider. 54
Additional Safety Interventions
Although existing motor vehicle safety devices, such as seat belts and airbags, probably provide increased protection for pregnant women and their fetuses in regard to adverse outcomes compared with no devices, more safety interventions are needed, particularly those targeted toward vehicle design, legislation development, and behavior modification.
Vehicle design
Existing vehicle crash protection systems can be improved for pregnant women and fetuses. The performance standards for vehicle safety designs are based on the stature and anatomy of average male drivers. As such, pregnant women may be uncomfortable with the positioning of certain vehicle devices (eg, belts and steering wheels) and may subsequently adjust these devices, thus putting themselves and their fetus at risk of injury. Therefore, automobile manufacturers should consider pregnant women when designing and testing vehicles and their safety devices in order to better accommodate the size and shape of these women. In addition to changes in vehicle design, protective devices worn in the vehicle may theoretically prevent injuries to pregnant women in crashes. For example, developers in Columbus, Ohio, recently designed nonmetal pregnancy “shields” of various sizes that could be fit over a pregnant woman’s abdomen while sitting in the vehicle. 58 The purpose of the shield is to redistribute forces, prevent seat belt intrusion, and reduce placental abruption in a crash during pregnancy. However, this and other related devices have not been studied for effectiveness.
Legislation
Although prior studies indicate that an estimated 75% to 96% of pregnant women report wearing seat belts, there are pregnant women who rarely or never wear belts. Legislative efforts to improve motor vehicle safety during pregnancy, such as primary seat belt laws, can help ensure that pregnant women, like all occupants, are wearing their seat belts during pregnancy. In the general population, evidence from the 2009 National Occupant Protection Usage Survey shows that belt use in states with primary belt enforcement laws (88%) is higher than belt use in states without primary belt enforcement laws (77%). 59 Therefore, enforcement of mandatory belt laws and adoption of primary seat belt laws may encourage pregnant women to wear seat belts at all times.
Behavior modification
There are several behavioral interventions that can be implemented to improve motor vehicle safety during pregnancy. For example, effective programs are needed to improve proper seat belt use. Educational interventions that emphasize the importance of correct belt placement can increase the use and proper placement of seat belts during pregnancy.54,56,57 In addition, pregnant women can be encouraged to decrease their crash risk by modifying their driving behaviors and driving use. Although not much is known about the circumstances surrounding crash events among pregnant women, ambient light, weather conditions, types of roadways, and vehicle speed are known to contribute to motor vehicle crash risks in the general population.60,61 As such, pregnant women could consider doing most of their driving when safer conditions prevail—that is, during the day, in good weather conditions, on well-maintained roads, and at average speeds in order to minimize their crash risk. Alternatively, some women may choose to reduce their driving frequency and distances during pregnancy (ie, lowering exposure) to avoid the potential for crash involvement.
Conclusion
Although many pregnant women and their fetuses are injured in motor vehicle crashes each year in the United States, population-based research pertaining to the effect of crashes on maternal and fetal outcomes and interventions aimed toward the reduction of crashes and improved safety during pregnancy are limited. To date, only 5 population-based studies have examined the association between motor vehicle crashes and maternal and fetal outcomes2,4,15,21,40; none of these studies described the circumstances surrounding the crash events. In addition, only 2 population-based studies2,40 have assessed the effect of seat belts, and 1 population-based study 4 examined the effect of airbags on maternal and fetal outcomes from crashes during pregnancy. More research is needed to better understand the circumstances surrounding crash events and the factors that contribute to crash-related maternal and fetal injuries. To facilitate this research, states should adapt pregnancy-related crash surveillance systems by using probabilistic record linkage methodology of existing records (ie, vital records and motor vehicle crash records) to track and monitor motor vehicle crashes during pregnancy. Currently, this information is not routinely collected in most states, yet all states collect vital records and crash data. To date, only 4 states (North Carolina, Pennsylvania, Utah, and Washington) have used probabilistic record linkage to examine crashes during pregnancy. Collective efforts to improve surveillance systems and conduct epidemiological research can help identify pregnancy-related risk factors for maternal and fetal injuries from crashes, which will aid in developing and implementing the most effective interventions.
Evidence-based interventions are needed to reduce the frequency of crashes and to minimize the risk and severity of crash-related injuries through increased seat belt use and proper placement of belts among pregnant women and the development of novel vehicle safety devices. Although there are no published studies pertaining to interventions to reduce driving frequency or modify high-risk driving behaviors among pregnant women, there are evidence-based studies regarding the effectiveness of educational interventions to increase belt use and proper placement of belts.54,56,57 Evaluations of these interventions have shown that providing pregnant women with prenatal seat belt counseling and/or educational materials is effective at increasing their knowledge of the effectiveness, use, and placement of belts. Therefore, existing interventions for belt use should be more widely implemented, and new interventions focused on other high-risk driving behaviors should be developed and evaluated. In addition, the development and evaluation of personal safety devices, such as the pregnancy shield, 58 may provide another avenue for the prevention of adverse maternal and fetal outcomes from crashes during pregnancy.
Footnotes
Acknowledgements
Catherine J. Vladutiu received partial support from Grant Number