
Abstract
Acute exercise prior to vaccine administration can improve the immune response. Animal data are now supported by human trials, which have shown that immune responses are enhanced by a bout of acute exercise before innoculation; this effect is particularly prominent in vaccines that normally produce weak immune responses. Although there remain many aspects of this phenomenon to be investigated, including task characteristics such as duration and form of exercise, it appears that even a moderate bout of exercise of the muscles into which vaccine will be administered can enhance the antibody response. In this review, the authors will summarize the animal and human literature and discuss the investigation of potential mechanisms of acute exercise–induced immunoenhancement.
It has been hypothesized that eccentric exercise, performed using the muscles located at the site of vaccine administration, improves the subsequent immune response by inducing a proinflammatory environment in the muscles.
Introduction
The introduction of vaccines against diseases has been one of the most successful public health interventions and, at present, is the most effective and cost-efficient method of disease prevention in humans. 1 Despite the remarkable success of vaccination, there is variation in the efficacy of some vaccines, and many are only capable of inducing relatively poor immunogenic responses. For example, the effectiveness of influenza vaccination at preventing disease can be as high as 71%, but research suggests that the efficacy may be as low as 53% in healthy adults. 2 Other vaccines such as hepatitis B induce even poorer immune responses, and further “booster” vaccinations are thus required. 3 Given the often poor immunogenicity of some common vaccines, there is a large body of research devoted to developing adjuvants to improve immune responses. 4
The acute-stress immunoenhancement hypothesis 5 has been developed based on a number of studies suggesting that acute stress, experienced at close temporal proximity to vaccine administration, may induce endogenous adjuvants and thus augment the subsequent immune response (Figure 1). For a number of years, researchers have suggested that, from an evolutionary standpoint, acute stress is an integral component of the fight or flight response. 6 This response initiates a series of immunological changes, presumably in anticipation of exposure to antigenic challenge, with the primary aim of maximizing immune responses against the antigen. The literature surrounding this area mainly comprises research conducted in animals, with a now increasing number of studies also conducted in humans. To assess the effectiveness of the immune responses to vaccination, researchers in this area have typically investigated either humoral immunity status (eg, antigen specific antibodies) or cellular responses (eg, delayed-type hypersensitivity reactions). In animals, a variety of behavioral stressors have been used, including restraint stress, inescapable footshock, and exercise. Human studies have primarily used exercise with either dynamic whole-body exercise (eg, cycling) or isolated muscle actions of isolated muscle groups (eg, eccentric movements). Psychological stress studies have used laboratory stress tasks, such as public speaking or mental arithmetic. The hypothesis is that the stressor, regardless of the mode chosen, temporarily primes the immune system and augments the response to any proximal pathogen exposure.
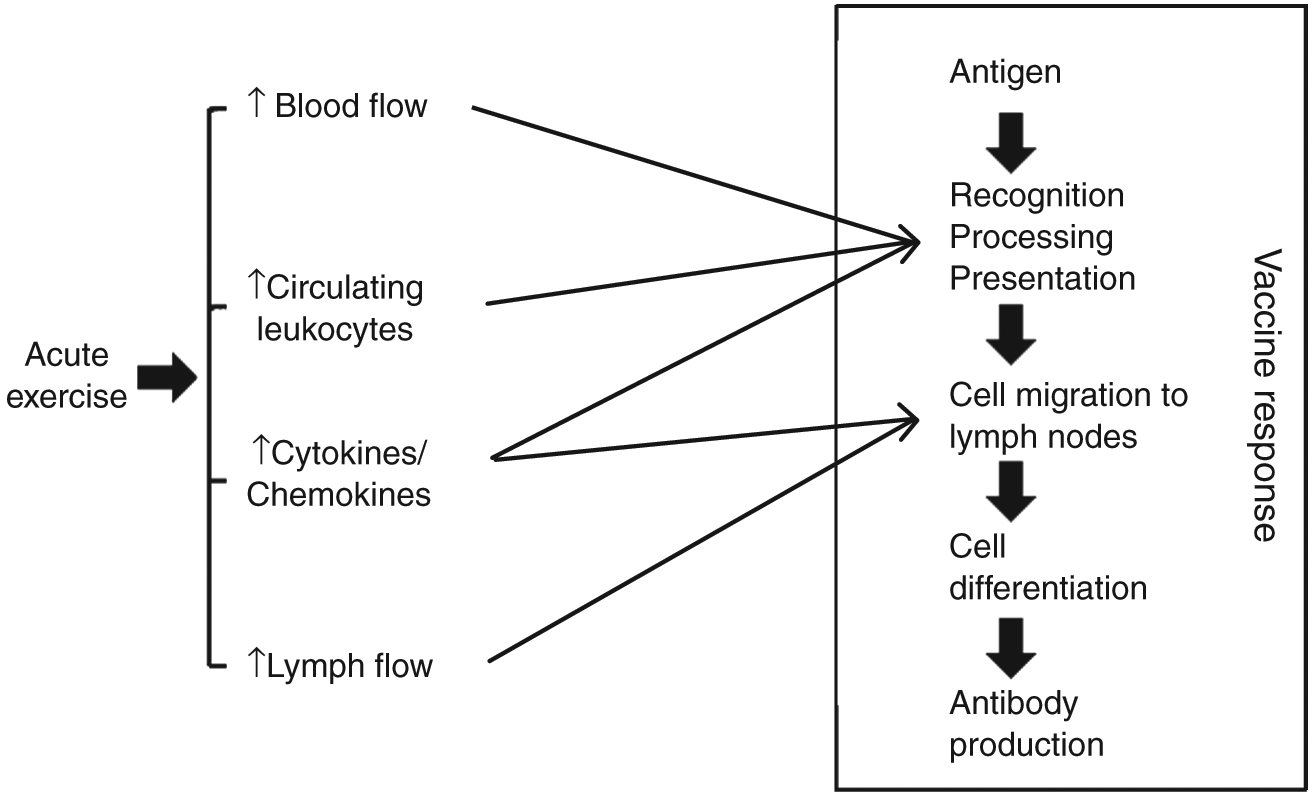
Responses to Acute Exercise and Potential Points of Interaction With Vaccine Response.
Acute Stress–Induced Enhancement of Vaccination Response in Animals
The animal literature offers strong evidence to suggest that acute stress administered at close temporal proximity to vaccination can enhance both the primary and secondary antibody responses. For example, Millan and colleagues 7 showed that rats exposed to short periods of restraint stress (2 hours over 2 consecutive days) prior to inoculation had higher primary antibody titers at 7 days postimmunization compared with control rats. Similarly, antibody responses to sheep red blood cell inoculation have been shown to be enhanced by restraint stress immediately prior to injection, 8 and responses to the primary antigen keyhole limpet hemocyanin are shown to be enhanced by footshock.9,10
As will be discussed in more detail in later sections, findings in human studies have shown that acute stress selectively enhances responses to the antigens that elicit weak responses; 2 studies from the animal literature also support this observation. Karp and colleagues 11 exposed mice to restraint stress immediately after (keyhole limpet hemocyanin) vaccination and found enhanced antibody responses at 3 time points postinnoculation (8, 14, and 21 days). In addition, the study included an immunodeficient group of mice, modeling the poorer immune system responses. The results indicated that mice administered an immunosuppressive drug, cyclophosphamide, prior to vaccination appeared to show the largest increase in antibody responses when exposed to restraint stress. These findings appear to illustrate that acute stress exposure may be more beneficial at augmenting immune responses in circumstances where poorer responses would otherwise be expected. In a similar model, which compared young and old mice, Kapasi and colleagues 12 found no effects of acute or chronic exercise on the antibody response to human serum albumin in young mice. However, older mice exposed to acute exercise had elevated antibody responses in comparison with other older mice in either a control group or a chronic exercise group. These findings lend further support to the notion that acute stress may have the potential to help return otherwise weak immune responses to more “normal” levels.
In summary, the majority of the literature illustrates that acute stress enhances responses to antigens in mice and rats and further suggests that poorer immune responses may be particularly enhanced by acute stress. Despite the majority of literature supporting this line of research, it should be noted that not all acute stress studies have found enhancements to vaccine responses. 13
Acute Stress–Induced Enhancement of Vaccination Response in Humans
There is accumulating evidence that acute stress may also enhance immunity in humans. However, historically, there seemed to be conflicting theories in this research area. The open window hypothesis suggested that after a single bout of acute strenuous and pro-longed exercise, the immune system becomes suppressed and vulnerable to infections such as upper-respiratory tract infections. 14 With this hypothesis, 2 early studies were conducted, but they bear remarkable similarity in design to the later studies examining acute stress–induced enhancement of vaccination responses. In contrast to the open window hypothesis, but in keeping with the acute stress–induced enhancement hypothesis, Eskola and colleagues 15 found that the antibody response to tetanus toxoid vaccination was higher in the group that had completed a marathon prior to innoculation compared with a nonrunner control group. However, in a similar study, Bruunsgaard and colleagues 16 did not find differences in the antibody responses to diphtheria, tetanus toxoid, and 6 pneumococcal serotypes between triathletes who had just completed a half-ironman competition prior to vaccination compared with either resting triathletes or sedentary controls. These studies both used extreme bouts of exercise to elicit an effect of exercise on vaccine responses; the sample sizes were relatively small and did not control the exact duration and relative intensity of the acute stress exposure in each participant. Despite the limitations of both investigations, it is important to note that neither study supported the hypothesis that exercise suppresses antibody response to vaccination.
Recently, a more detailed program of studies began to examine the acute stress–induced immunoenhancement hypothesis in humans. Our group has completed a number of studies, which have demonstrated that both acute exercise and psychological stress experienced at close temporal proximity to vaccination have a beneficial effect on the subsequent antibody response. In the first of these studies, 2 vaccines were administered—influenza and meningococcal A + C—after either resting control, acute dynamic (cycling) exercise. or psychological stress.17,18 Given the apparent differences in mechanism of responses between thymus-dependent (influenza) and thymus-independent (meningococcal) vaccines, we used both to assess any difference in susceptibility to alteration by acute stress and thus discern the importance of the role played by T-cells in altering the response. Participants in the exercise group completed a moderate-intensity cycling task, those in the psychological stress group completed a time-pressured mental arithmetic test, and a nonstress control group rested quietly. Following their allotted 45-minute task, participants received an influenza vaccine. Results indicated that women in both the exercise group and psychological stress groups showed enhanced antibody responses to the A/Panama influenza strain at 4 and 20 weeks postvaccination in comparison to the resting control group. 18 This strain elicited particularly poor antibody responses in the female control group, suggesting that the interventions successfully augmented the antibody response to an otherwise weakly immunogenic strain. In contrast, men displayed robust responses to all strains, and no effects of exercise or stress were observed. In the same study, participants were also administered a meningococcal A + C vaccine into the contralateral arm. 17 Results indicated that in men, both exercise and psychological stress improved the antibody response to meningococcal A compared with control men. In agreement with the previous study, augmentation was observed where the control group response was poor; on this occasion, men, rather than women, in the control group had weaker responses to this particular strain. These results confirmed that the adjuvant effects of exercise and psychological stress are not limited to thymus-dependent (eg, influenza) or thymus-independent (eg, meningococcal) vaccines and thus do not seem to be dependent on T-cell interactions.
In the second study in this series, a resistance-based, eccentric exercise protocol was developed. 19 An eccentric exercise task was designed to initiate a local inflammatory response in the biceps brachialis and deltoid muscles of the arm in which the influenza vaccine was administered. It was hypothesized that this inflamed local environment would provide an efficient way of augmenting the antibody response to influenza vaccination. Sixty healthy young adults were randomly allocated to either an eccentric exercise group or a control group. The exercise group performed 50 repetitions of the eccentric portion of the bicep curl and lateral raise exercises in the nondominant arm using a weight that was 85% of the single repetition maximum; the task lasted approximately 25 minutes. The control group rested quietly for the same time. Then, 6 hours after task completion (to allow for the inflammatory response to the exercise to develop), participants received an influenza vaccine into the nondominant arm. Results indicated that women in the exercise group showed enhanced antibody responses to the A/Wyoming and B/Jiangsu strains of influenza at 6 and 20 weeks postvaccination. Again, these strains had produced relatively weak antibody responses in women in the control group; again, however, men showed more robust responses against these strains, and no effects of exercise were found. In line with these findings, the other strain in the vaccine, A/New Caledonia, produced robust responses in both men and women in the control group, and no effect of exercise was observed.
These 2 initial studies were followed by 2 larger studies conducted by our group. These recent articles provide somewhat mixed findings, but taken together, extend the evidence for the acute stress–induced immunoenhancement hypothesis. These 2 studies investigated the effects of exercise timing and intensity and were again in a population of young, healthy adults. Interestingly, that in the timing study, 20 a full-dose influenza vaccine was used, whereas in the intensity study, 21 a reduced dose (0.5 times the recommended dose) influenza vaccine was used.
In the timing of exercise study, 20 we randomized 156 healthy young adults into 1 of 3 exercise groups or a control group. The 3 exercise groups all completed the same eccentric exercise task as previously described 19 but at different intervals prior to vaccination. A time point 6 hours prior to vaccination was used based on reported kinetics of the cytokine interleukin-6 (IL-6) response to eccentric exercise.19,22 Many of the exercise-induced physiological and immunological changes are returned to baseline within a short period of recovery, including increased circulating lymphocytes, 23 increased lymphatic drainage,24,25 and increased blood flow. 26 Given this and that from a pragmatic perspective a task closely associated with the vaccine might have most clinical applicability as well as replicating the timing used in the first in this series of studies, a group that exercised immediately prior to receiving the vaccine was also included. Finally, there was a group that performed the task 48 hours prior to vaccination. This time point was included to capture the peak of the muscle damage response, which at 48 hours postexercise is shown to include a peak in accumulated inflammatory infiltrate, including neutrophils, mononuclear cells, cytokines, and heat shock proteins.27,28 A full-dose influenza vaccine was administered, and all 3 strains produced robust responses in both men and women (23-, 10-, and 14-fold changes from baseline to 28 days), which were neither different between exercise and control groups nor among exercise groups. Physiological indices demonstrated that exercise timing did alter the profiles of muscle damage (pain and plasma creatine kinase) among the groups at the time of vaccination, but contrary to expectation, IL-6 was highest in the 48-hour and immediately prior exercise groups, indicating that the kinetics did not follow the same inflammatory response as previously reported.22,29 Although this null finding was unexpected, it was not entirely surprising, given the strong responses to all strains of virus contained in the seasonal influenza vaccine.
The intensity of exercise study followed a similar design, comparing the effects of 3 different exercise intensities with a resting control group. 21 This, the largest of the studies in the literature, included 160 healthy adults randomized to 1 of 4 groups. Exercise intensities of 60%, 85% (as had been used in prior studies), and 110% of the single repetition maximum were used. The importance of intensity on the adjuvant effect is of particular interest, not only to determine a task with maximum efficacy but also for clinical application—that is, if intensity shows no effect, a modest bout of exercise could still be prescribed for a beneficial effect on protection afforded by vaccination. Given the previous finding that in a similar cohort, a full-dose seasonal influenza vaccine produced robust responses in all 3 strains, this experiment used a reduced (50% of recommended dose) dose influenza vaccination. Administering a reduced dose allowed us to investigate whether poorer responses, elicited by a less immunogenic antigen exposure, were enhanced by exercise. Indeed, smaller fold changes were seen, with 2 strains showing responses of 5- and 6-fold changes; the final strain showed a robust 19-fold response. As hypothesized, exercise enhanced the antibody response in both the strains, which demonstrated a weaker response in the control group. The B/Florida strain, which showed an overall 5-fold increase, was enhanced by exercise in both men and women, whereas the A/Uruguay strain (6-fold response) was enhanced by exercise in men. There were no differences among the exercise groups in antibody responses, despite physiological differences such as dose-dependent changes in arm circumference and reported pain and the creatine kinase response. Furthermore, in contrast to the previous finding by Edwards et al 18 of an association between IL-6 and enhanced antibody responses, in this report, IL-6 measured 24 hours after task and vaccination did not show any association with antibody response. Although these null findings do not show support for any mechanistic pathways, it should be remembered that all current published studies have limited methodologies, for example only measuring IL-6 at baseline and a single follow-up. Thus, more detailed kinetics and a broader set of markers are needed to advance our mechanistic understanding.
Potential Mechanisms
It has been hypothesized that eccentric exercise, performed using the muscles located at the site of vaccine administration, improves the subsequent immune response by inducing a proinflammatory environment in the muscles. During an active eccentric muscle action, the exercising muscle applies force as it lengthens, causing damage to the internal structure of the muscle fibers. 30 This damage is greater than that observed with concentric (shortening) muscle contractions 31 and, in untrained individuals when substantial damage is caused, leads to an inflammatory response in the muscle. 32 Characterized by edema, muscle pain, muscle weakness, leakage of muscle and cellular proteins (eg, creatine kinase), and cellular infiltration, this response occurs early postinjury and may last from 2 up to 7 days. 28 For example, exercise elevates the levels of inflammatory mediators released from stressed cells within the damaged muscle tissue. 33 These stressed cells release a range of danger signals, such as IL-6, uric acid, HSP60, HSP70, and are thought to play a role in orchestrating inflammation and repair of the surrounding tissues.34,35 These markers of inflammation may result in increased leukocyte homing to the site of vaccine administration and/or enhanced antigen uptake and processing, making the initial phase of the immune response more efficient and subsequently enhancing the antibody response. In support of this theory, the extent of the self-reported pain and the change in upper-arm limb circumference following eccentric exercise, both indirect indicators of muscle damage, have been significantly positively correlated with the subsequent cell-mediated immune response to the vaccination. 19
Elevated concentrations of proinflammatory cytokines, such as IL-6, have been implicated in enhancing vaccine responses.36,37 For example, higher mean levels of circulating IL-6 were found in the sera of vaccinees with good antibody responses than in sera from nonresponders, from 7 days prior to vaccination through to 63 days postvaccination. In addition, preimmunization levels of IL-6 in serum were also higher in responders than in nonresponders. 36 In another study, the coadministration of IL-6 gene with vaccine completely protected mice from a lethal challenge with influenza virus; coadministration of other cytokine genes was less successful. 37 Given these findings, it has been hypothesized that increased levels of IL-6 in the systemic circulation, stemming from eccentric exercise–induced muscle damage, may play a role in augmenting the immune response to vaccination. Indeed, the extent of the IL-6 response was also associated with the antibody response at 6 weeks’ postvaccination. 18 However, no associations were found between the IL-6 response to exercise at 24 hours’postexercise and the antibody response to vaccination in either the timing or intensity studies.20,21 It is possible that this discrepancy is a result of the mode of exercise used. The previous study used a concentric cycling exercise, rather than an eccentric exercise intervention, which is known to induce more localized muscle damage. In whole body exercise, the circulating levels of IL-6 are likely to be crucial to any adjuvant effect. There is evidence that plasma levels of IL-6 do not always accurately represent actual intramuscular damage and inflammatory status following eccentric exercise; 38 thus, it remains possible that IL-6 levels in the muscular tissue, rather than plasma, are more closely related to the extent of the antibody response to the vaccination.
Alternatively, it is possible that the degree of inflammation is not the main mechanism underlying this effect. Indeed, one of the most commonly observed immune effects of acute stress is leukocytosis. 23 This rapid increase in cell numbers observed in the circulation includes increases in monocytes and dendritic cells,39,40 which are responsible for antigen recognition, uptake, and presentation. Thus, acute exercise initiates leukocyte mobilization and subsequent extravasion into tissues, guided by chemoattractants of the transient inflammatory response in the exercised muscles. In this way, acute exercise would induce leukocyte mobilization and localization of leukocyte accumulation in exercised muscles, the intramuscular administration of antigen further attracts leukocytes, and the immune response develops, enhanced by the exercise-induced magnification of accumulation of leukocytes.
A final mechanistic pathway to be mentioned is the enhancement of lymph drainage. There is evidence to suggest that muscular contractions are associated with a temporary increase in lymph drainage around the site of exercised muscle tissue. 25 Therefore, exercise could subsequently lead to enhanced immune cell transport from the site of antigen administration via this altered lymph fluid dynamics. In this case, it would be hypothesized that performing some degree of exercise is sufficient to enhance antigenic transport to the lymph nodes where recognition by lymphocytes takes place. It would be interesting to measure this more directly in future studies.
Future Directions
It is clear from the issues raised in this review that further investigation into the exercise-induced augmentation of vaccine responses is warranted. For example, it appears that exercise has an adjuvant effect on vaccines containing poorly immunogenic strains. Given this, it would be interesting to test this hypothesis directly by measuring the efficacy of an exercise intervention on the antibody responses to different doses of a vaccine. If the intervention could increase the response to a reduced dose vaccine to the levels observed with a standard dose, then this would be beneficial in circumstances where vaccine availability is reduced. Alternatively, the adjuvant effect of exercise on poor immune response could be investigated by measuring the effects of exercise on the immune response to vaccination in immunologically compromised individuals. There is a host of different populations that may benefit from this approach. For example, HIV patients are known to respond poorly to vaccination. 41 Similarly, there is now a wide body of research implicating immunological senescence (ageing) as an important factor in the efficacy of vaccination; 42 thus, it would be of pertinent interest to investigate whether these poorer responses can be enhanced by acute exercise, as has been shown in elderly mice. 12 It should be noted, however, that there is evidence that older adults also have reduced inflammatory responses to exercise, 43 and this may affect the efficacy of this intervention. It is conceivable that similar deficiencies may be observed in the responses of HIV patients, although to our knowledge, this has never been directly tested.
Footnotes
Acknowledgements
The authors wish to thank Dr Victoria Burns and Prof Christopher Ring for the many discussions on this topic and Ms Lianne Tomfohr for her critical reading of the manuscript.