
Abstract
Keywords
Introduction
The ability of ionizing radiations (IRs) to adversely affect the function of hemolymphopoietic system has been well known since the early 1900s.1-3 The damaging effects of IRs on hematopoiesis were demonstrated in studies conducted on survivors of the atomic bombs dropped on Nagasaki and Hiroshima in 1945. In this case, hematopoietic failure was the leading cause of death due to the exposure to moderate/high doses of IR. 4 At doses >2-3 Gy, absorbed in a short period of time, the hematopoietic sub-syndrome (HS) of the acute radiation syndrome (ARS) becomes clinically manifest.5,6 IRs induce damage and suppression of mitosis in hematopoietic stem cells (HSC) and their progeny and apoptosis in lymphocytes and other hematopoietic cells. 7 On the other side, also long-term repeated exposure to lower doses (from 0.7-1.5 Gy to 2-3 Gy) can damage the hemolymphopoietic system. 8 Such chronic radiation syndrome (CRS) can manifest with a moderate leukopenia sustained by neutropenia and, in some cases, by lymphopenia, up to a serious bone-marrow hypoplasia.9-11
However, it should be noted that, over the past 4 billion years, IR exposure from geologic materials decreased fom about 1.6 mGy y(-1) to 0.66 mGy y(-1), 12 and recent estimates reported an annual average individual effective dose of approximately 2.4 mSv for natural radiation exposure.12-14 On the other hand, it is also important to emphasize that IR occupational exposure is characterized by chronic exposure doses that are extremely lower than those capable for generating CRS. 15 For example, the European Atomic Energy Community Directive 2013/59/Euratom (but also the International Commission on Radiological Protection (ICRP) with its 2007 recommendations) establishes 20 mSv in a single year as the effective dose limit for occupational exposure (although a higher effective dose, up to 50 mSv in a single year, may be allowed under special circumstances or for certain exposure situations).16,17 Furthermore, it is widely acknowledged that low or very low-dose radiation exposure is defined as ≤100 mSv and the low-dose radiation rate is ≤ 6 mSv per hour. 17
The worldwide health protection from the adverse effects of IRs in general living and occupational settings, is based on the linear no-threshold (LNT) extrapolation model18,19 that considers IRs capable of causing harmful biological effects, e.g., cancers, in a manner proportional to the magnitude of the exposure dose, irrespective to its low- or very low-level.20,21 Nevertheless, the potential adverse effects associated with IR low-doses continues to remain an extremely controversial issue. This is also due to the somewhat conflicting results obtained in available epidemiological studies. Some of these, in fact, demonstrated an adverse impact on the hemolymphopoietic system,22,23 others supported the radiation hormetic phenomenon and the hypothesis of a radioadaptive response,24,25 whereas others failed to identify any effect, 26 thus preventing definite conclusions. Moreover, the dose-response relationship at low-levels of exposure, an essential aspect in the assessment and management of IR risks for workers, has not been still clarified. 15 An epidemiological study conducted on Chinese healthcare workers exposed to IRs reported a significant difference in platelet count among the cumulative radiation dose groups with a nonlinear dose-response relationship (U-inverted shaped association). 27 In this study, the cumulative radiation dose was 0.200-31.272 mSv, and doses were divided into 0.200-2.586, 2.586-3.754, and 3.75- 32.00 mSv by the inter-quartile range. The group with the 2.586-3.754 mSv cumulative dose showed the highest platelet level, 235.75 ± 55.15 (109/L). Overall, there was a correlation between platelets changing and the cumulative radiation dose after adjusting for gender, services at baseline, occupation, medical level, and smoking. Platelets in male showed an increase trend with the cumulative radiation dose (βa = 0.013 × 109/L, 95% CI = 0.007- 0.019 × 109/L). A comparable nonlinear dose-response relationship, with respect to the cumulative IR dose, was determined in industrial radiation workers, for red blood cells (RBCs), platelets, and hemoglobin (HB) levels. 28 Interestingly, also in a group of healthcare workers, RBC, HB, and glutathione levels showed a nonlinear trend with respect to the cumulative annual effective dose. 29
Therefore, the aim of the present study was to obtain further information on the potential adverse effects induced by IR low-dose exposure on the hematological parameters of occupationally exposed healthcare workers. Hematological parameters were compared with values obtained in a control group and also evaluated in relation to the cumulative dose of IRs over the past 5 years to study the dose-response relationship.
Methods
Subjects and Recruitment Strategy
This retrospective observational study was performed using data and information retrieved from health surveillance medical examinations performed on healthcare workers employed in a hospital located in a large metropolitan city in Southern Italy during the period 2017-2021. The Italian legislative framework for health and safety in the workplace, regulated by Legislative Decree 81/08 (and its amendments and integrations), establishes the obligation to submit workers exposed to specific occupational risk factors (e.g., biological agents) to periodic health surveillance medical examinations. Since 2020, in Italy the radiological protection of workers exposed to IRs is ensured by the application of the Legislative Decree 101/20 (transposing the European Atomic Energy Community Directives on this topic) which, similarly to Decree 81/08, imposes the provision of periodic health surveillance to workers who experience occupational IR exposure. In detail, workers exposed to IRs are classified into two occupational exposure categories according to the presumed exposure dose: category A includes workers at the greatest risk of exposure, susceptible to be exposed to an annual effective dose between 6 and 20 mSv; category B refers to workers susceptible to be exposed to an effective annual dose higher than 1 mSv but lower than 6 mSv. Exposed workers were engaged in IR application both for diagnostic and therapeutic purposes consisting mainly in performing radiographs and computed tomography scans and using radioisotopes. 30 Consequently, the following inclusion criteria were applied for the workers’ enrollment: i) to have been hospital workers exposed to IRs and belonging to categories A and B, e.g., physicians, nurses, radiology technicians, social-health workers, residents and PhD students, equally divided between females and males, ii) to have been continuously exposed to IRs (in category A or B) during the reference period, iii) availability of dosimetry data in the period 2017-2021, iv) to have performed periodic health surveillance examinations in the investigated period, v) negative history of anemia or other diseases of the hemolymphopoietic system. Then, among the healthcare staff of the same hospital, IR unexposed control workers were individually selected to obtain a control group that had similar socio-demographic (especially age and gender) and occupational characteristics (occupational risk factors, with the exception of IR exposure) as the exposed group, accordingly with the last two above-mentioned inclusion criteria. Ethical issues were addressed as all the workers, during their health surveillance, were adequately informed on aims, methods and any other relevant aspects of the study and agreed about the possibility to use their data anonymously and collectively for research purposes. All medical procedures were performed, and all other information relevant to the study were obtained, in compliance with relevant national laws (Legislative Decree 81/08, 101/20 and 230/95) and respecting the privacy rights of recruited subjects.
Assessment of the Cumulative Radiation Dose
Dosimetric data on annual exposure to IRs (in terms of effective dose) were retrieved from the personal dosimetry record form provided by the radiation protection expert. The determination of the effective dose was carried out using the data provided by individual thermo-luminescent dosimeter (TLD) badges (Tecnorad, Verona, Italy). This dosimeter model, worn under the gown, uses thermoluminescence technology and is usually applied for personal monitoring of X and Gamma IRs, providing the worker’s individual dose, which is estimated by considering primary beam position, beam quality and source-skin distance. 30 For each worker, by adding the IR effective doses recorded over the period 2017-2021, we obtained a cumulative (5 years) effective dose and then calculated the relative mean over the reference period. In order to evaluate the dose-response relationship, we divided the exposed subjects into three different categories based on the inter-quartile range of the cumulative radiation dose.
Socio-Demographic, Occupational, and Biochemical Data
The socio-demographic data (e.g., age and gender), occupational features (e.g., professional category, job task, working area, years of exposure, exposure to occupational risk factors, use of personal protective equipment), anamnestic data (especially with regard to the possible presence of hematological disorders) and information about recreational habits/lifestyle (i.e., smoking) of all workers were obtained from the health record hold by the hospital occupational physician. The health surveillance protocol performed in healthcare workers, according to the provisions of Legislative Decree 101/20 and 81/08, included the collection of blood samples to perform hemogram and other biochemical analysis (e.g., blood glucose, lipid profile, thyroid hormones, and so on). Blood sampling was carried out by nursing staff of the hospital’s Occupational Medicine department under fasting conditions and collecting 5 mL and 3 mL of peripheral blood in appropriate vacuum tubes for the determination of biochemical parameters (BD Vacutainer, SSTTM II Advance Plus Bloob collection Tubes, Becton, Dickinson and Company, Belliver Industrial Estate, Plymouth, UK) and hemogram (BD Vacutainer K3E Plus Blood Collection Tubes, Becton, Dickinson and Company, Belliver Industrial Estate, Plymouth, UK), respectively. The analysis were conducted according to standard clinical laboratory methods and in greater detail, following the manufacturer’s instruction, the XN-3100 Automated Hematology Analyzer system (Sysmex Corporation, Kobe, Japan) was used for hemogram testing, whereas the Cobas® Pro (F. Hoffmann-La Roche Ltd, Basel, Suisse) was used for biochemical analysis.
The occupational physician assembled an electronic dataset in which all the information needed to conduct the study was reported completely anonymously (by associating the data with a unique code). All statistical analysis (specified in the next section) were performed on the anonymous dataset and the information was processed collectively so that the data could not be traced back to the individual worker. Thus, in this study, all information was processed and handled with respect for worker privacy and no additional sensitive data were collected, used, or analyzed in addition to those that are usually evaluated in the mandatory health surveillance activity established by the Italian regulatory framework for the protection of the health and safety in the workplace.
Statistical Analysis
Data are summarized with mean and standard deviation for continuous variables and with absolute frequency and percentage for categorical variables. Student’s t test or Mann-Whitney U test, as appropriate, was used to investigate the difference between means for continuous variables. Difference between cumulative dose groups is additionally expressed as rate of change compared to the control group and standard error. ANOVA or Kruskal-Wallis, as appropriate, were used to investigate the difference between more than 2 groups for continuous variables. Chi-square test or Fisher’s exact test, as appropriate, was used to investigate difference between groups for categorical variables. Bonferroni correction was used to adjust the P-values for multiple comparisons. Crude and adjusted linear regression models were used to investigate the association between all the considered predictors and the outcomes RBCs, HB and HCT. Adjusted regressions included all and only variables which were significant (P < .05) at the crude model. In particular, all the available socio-demographic and clinical variables were considered as covariates. To investigate the non-linearity of the association between the cumulative dose of radiation and each of the three continuous outcomes, natural cubic spline term was added to the models. Non-linearity was hypothesized first inspecting the residuals plot. Then, models with and without cubic spline term were compared using ANOVA, while Bayesian Information Criterion (BIC) ad Akaike Information Criterion (AIC) were used to check model performances. Additionally, for all analyses, the value of P < .05 was considered as the threshold for statistical significance. R software version 4.4.0 was used for the analyses.
Results
Socio-Demographic and Occupational Characteristics of Studied Subjects
A total of 180 IR exposed workers and 180 unexposed controls was enrolled in the study. The mean ± SD age of healthcare workers was 49.32 ± 11.29 years (52.38 ± 11.35 and 46.04 ± 10.44 for male and female workers, respectively). Unexposed controls had a mean ± SD age of 50.20 ± 13.75 years (53 ± 14.01 and 47.28 ± 12.92 for male and female workers, respectively), without significant difference with exposed ones (P > .999). The vast majority of the sample, both among the controls (86%) and the exposed workers (88%), were nonsmokers. Comparably, also with respect to the dietary habits and alcohol consumption, the characteristics of the sample were completely overlapping with an absolute prevalence of Mediterranean diet and occasional alcohol consumption in both groups.
Differences in the Main Socio-Demographic and Occupational Characteristics of Controls and IR Exposed Workers Groups (Subdivided According to Cumulative Doses).

Socio-demographic, lifestyle and occupational features have been explored in IR exposed and unexposed workers in order to identify possible differences between groups that may influence the functionality of the hematopoietic system. *P-value of the difference between the 4 groups (controls, 1st interval, 2nd interval, 3rd interval) computed with ANOVA/Kruskal Wallis or with Chi-square/Fisher’s test as appropriate. Adjusted P-value obtained using Bonferroni correction for multiple comparisons. Significant values are marked in bold.
Levels of Hematological and Biochemical Parameters
Differences in the Main Hematological and Biochemical Parameters of Controls and IR Exposed Workers Groups (Subdivided According to Cumulative Doses).

Differences in hematological and biochemical parameters were investigated to deeply understand the effect of low-dose IR exposure and possible non-linear dose-response relationship. Significant values are marked in bold.
CHO, cholesterol; GLU, glucose; HB, hemoglobin; HCT, hematocrit; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PLT, platelets; RBCs, red blood cells; TRIG, triglycerides; WBC, white blood cells.
*P-value of the difference between the 4 groups (controls, 1st interval, 2nd interval, 3rd interval) computed with ANOVA/Kruskal Wallis or with Chi-square/Fisher’s test as appropriate. Adjusted P-value obtained using Bonferroni correction for multiple comparisons.
Association of RBC Levels With Socio-Demographic and Occupational Variables
Association Between Individual and Occupational Factors and RBC Changes in Healthcare Workers Assessed Through the Univariate Linear Regression Model. Significant values are marked in bold.

Findings obtained with this model showed significantly lower RBC values in subjects included in the first cumulative radiation dose group than in controls (β: −0.18; 95% CI: −0.32, −0.04; P-value: .013). With regard to socio-demographic and individual variables, we observed statistically significant differences for gender (β: 0.50; 95% CI: 0.43, 0.57; P-value: <.001), age (β: 0.13; 95% CI: 0.03, 0.23; P = .010) and hypertension (β: 0.17; 95% CI: 0.06, 0.28; P = .002), observing higher RBC levels in male workers, in the 45-64 age group and in subjects with hypertension.
Association of HB Levels With Socio-Demographic and Occupational Variables
Association Between Individual and Occupational Factors and HB Changes in Healthcare Workers Assessed Through the Univariate Linear Regression Model. Significant values are marked in bold.
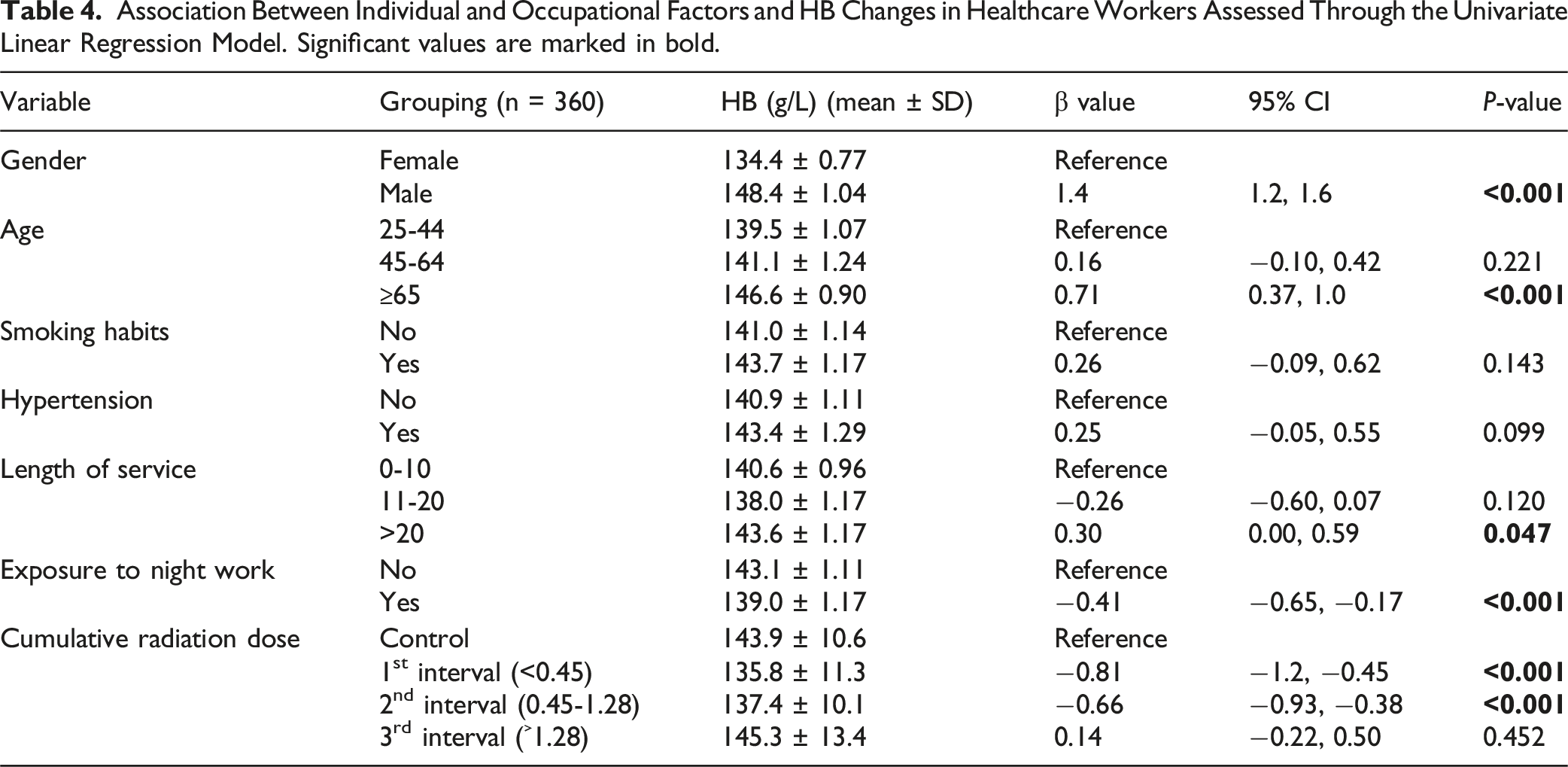
Concerning this hematological parameter and with regard to occupational variables, we observed several statistically significant differences. First of all, healthcare workers exposed to IRs and belonging to the first two cumulative dose ranges had significantly lower HB levels compared with those in the control group (β: −0.81; 95% CI: −1.2, −0.45; P =<.001 and β: −0.66; 95% CI: −0.93, −0.38; P = <.001 for the first and second cumulative dose group, respectively) and considerably lower HB values were also found in workers who performed night shifts (β: −0.41; 95% CI: −0.65, −0.17; P = <.001), whereas, in contrast, workers with greater length of service showed significantly higher levels of HB (β: 0.30; 95% CI: 0.00, 0.59; P = .047). Similarly, with regard to socio-demographic variables, average HB values were found to be significantly higher in male workers (β: 1.4; 95% CI: 1.2, 1.6; P = <.001) and in those aged 65 years and older (β: 0.71; 95% CI: 0.37, 1.0; P = <.001).
Association of HCT Levels With Socio-Demographic and Occupational Variables
Association Between Individual and Occupational Factors and HCT Changes in Healthcare Workers Assessed Through the Univariate Linear Regression Model. Significant values are marked in bold.

Dose-Response Relationship Between Cumulative Radiation Dose and Hematological Parameters
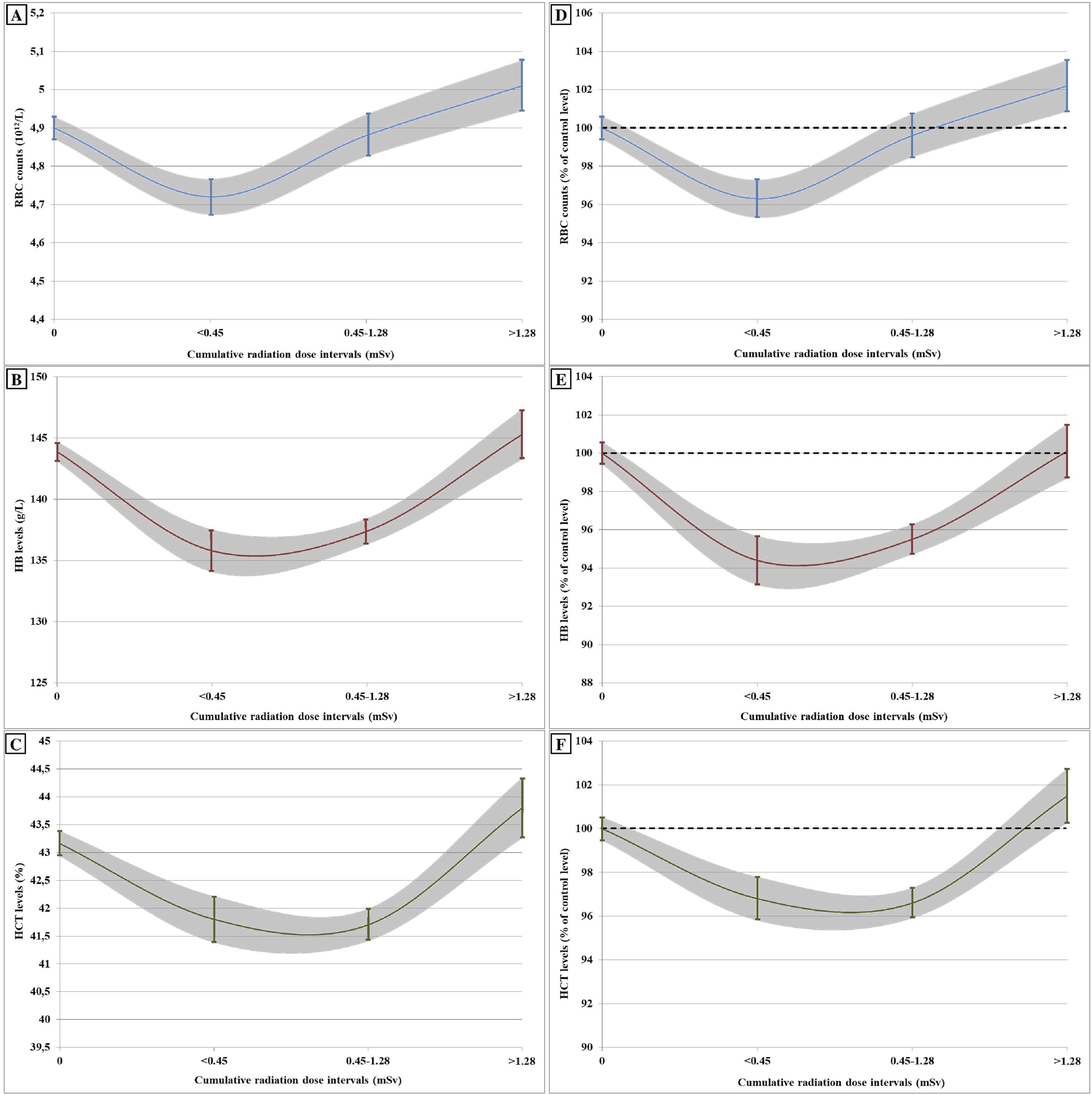
After adjusting for univariate variables that were meaningful at the crude model (P < .05), a natural cubic spline model was used to investigate the non-linearity of the association between the cumulative radiation dose and RBC, HB and HCT outcomes. These data demonstrated a significant (P < .001) nonlinear relationship between the IR cumulative dose with both RBCs (Figure 2A) and HB (Figure 2B) levels. As can be seen in Figure 2A, the RBC values (adj. model estimate at cumulative dose = 0, RBC = 5.20, pred. interval 5.11-5.28) initially decrease (reaching a minimum adj. estimated value of RBC = 5.08, pred. interval 4.99-5.17 for cumulative dose = 4.04) until the first cumulative radiation dose range and then begin to rise to levels even higher than those of controls (reaching a maximum adj. estimated value of RBCs = 5.40, pred. interval 5.23-5.58 for cumulative dose = 0.39). The same significant nonlinear relationship is also observed for HB and HCT values although in this case the pattern is less evident than for RBCs, with a similar decrease up to the first cumulative radiation dose interval and a subsequent increase (with increasing cumulative effective dose) that is, however, less pronounced, as shown in Figure 2B (adj. model estimate at cumulative dose = 0, HB = 151.3, pred. interval 149.1-153.4; minimum at cumulative dose = 0.51, HB = 144.5, pred. interval 141.9-147.0; maximum at cumulative dose = 5.70, HB = 153.2, pred. interval 149.0-157.4) and Figure 2C (adj. model estimate at cumulative dose = 0, HCT = 45.49, pred. interval 44.89-46.10; minimum at cumulative dose = 0.48, HCT = 44.10, pred. interval 43.40-44.80; maximum at cumulative dose = 4.9, HCT = 46.29, pred. interval 45.13-47.46).
Discussion
Ionizing radiations are widely employed in medical diagnostics, and the increased use of imaging and interventional radiology raises concerns about the potential risks for healthcare professionals. 23 The healthcare workers can experience a chronic and generally low-dose IR exposure despite the use of personal protective equipment and the adoption of suitable work practices.22,31 Unfortunately, there is limited information about the possible changes in hematological parameters of IR exposed healthcare workers, and particularly on the dose-response relationship at their levels of exposure. Understanding such issues is crucial for a better risk assessment and to tailor targeted preventive and protective measures. In our study, among all the investigated hematological parameters, only the RBCs, HB and the HCT showed some significant differences compared to the control group. Not suitable comparison of these results can be performed with the available literature data, as extremely conflicting findings have been reported in the last decade on blood parameters in IR exposed healthcare workers. 26 In fact, while some studies22,32-34 reported increased levels of lymphocytes, monocytes, RBCs, HB, HCT, Mean Corpuscular Volume (MCV), Platelet Large Cell Ratio, and Platelets (PLT); other showed decreased levels of neuthrophils, leucocytes, monocytes, basophils, lymphocytes, eosinophils, MCV, HCT, red cell distribution width, HB, PLT, Mean Corpuscular Hemoglobin Concentration (MCHC) and white blood cells (WBCs).23,32,35-38
When hematological changes were analyzed according to the gender of X-ray hospital technicians, the amounts of RBCs, HB, HCT, MCHC and lymphocytes were significantly higher in the male compared to female employees, while males showed decreased WBC and PLT counts. 33 Comparably, RBCs, HB, HCT were significantly higher in male radiation workers employed in the departments of radiology, computed tomography, nuclear medicine and radiotherapy, compared to female ones. 39 More recently, also Tian et al 29 showed significantly higher levels of RBCs and HB in healthcare IR exposed workers. In line with these previous findings, our study could determine significantly higher levels of RBCs, HB and HCT in male and older (≥45 years) workers compared to female and younger ones (25-44 years), respectively.
Concerning occupational factors, significantly higher levels of HB and HCT were demonstrated in those with the longest length of service (>20 years). As previously detailed for other parameters, conflicting results are available in literature in this regard. The recent study by Güngördü et al 23 on healthcare workers showed decreased HB levels only in workers exposed for more than 10 years. Qian et al 40 also found a significant decrease in the levels of RBCs and HB in IR exposed workers, including both medical workers as well as industrial and enterprise personnel, as the years of seniority in the profession increased. Tian et al 29 demonstrated that, in female medical radiation workers, the RBC count was significantly lower in those employed for at least 10 years compared to those in 5-10 years length of service. Conversely, in 2019, Sabagh and Chaperian, 39 determined a significant positive association between work experience and age and the RBC and HB levels. This overall suggests that the effects of IR on the hematopoietic system can be related to the frequency and duration of the exposure, although deep research is necessary to better define these issues.
Several factors need to be considered to explain the differences in the above-mentioned retrieved findings. These include the different study design, study sites, sample size, and the characteristics of the participants (e.g., our study was a retrospective analysis while Liu et al 27 performed a prospective investigation on healthcare workers, enrolling more than 1200 subjects). In most studies no unexposed subjects were enrolled as controls, and the lowest exposure groups was used as reference. Moreover, time of blood sampling, and other covariates such as time and duration of exposure, type of work (e.g., different devices employed: X-ray machine, computed tomography scan, fluoroscopy, for a variable number of patients a day, 5 to 35), including the methodology applied to determine the levels of IR exposure could differ among studies. In this latter regard, not all the studies addressing the hematological variability in healthcare workers due to IR exposure, reported dose values. This makes understanding the relationship between the low-dose IR exposure and hematological parameters a quite challenging issue. In fact, a median exposure of 0.68 ± 1.58 mSv/year by film badge and an average equivalent dose of 1.37 ± 1.12 mSv/year have been reported by Heidari et al, 32 and Surniyantoro et al, 36 respectively. In Tian et al 29 an annual effective dose was 0.58 ± 1.18 mSv was determined. Higher doses were reported by Ryu et al 37 with mean cumulative dose levels in males of 9.65 ± 15.2 mSv/year and 4.82 ± 5.55 mSv/year in females. In some cases, due to the loss of several personal doses monitoring data, a notional dose was employed, which was the average dose of the same occupation in the same year to supplement the missing data, and calculated the cumulative radiation dose by the job exposure matrix. 27
Concerning the dose-response relationship, our research demonstrated a significant non-linear relationship between RBCs, HB, HCT and the cumulative radiation dose. The RBC count showed a decrease at the first radiation dose, with an evident rise, compared to the control levels, at the highest doses. Such trend was also observed for HB and HCT levels, that decreased at the two first doses, and increased at the highest one, although in a less evident manner. Comparably, Tian et al 29 found that in male medical radiation workers, the RBC and HB levels were significantly higher in the 0.5 mSv group compared to those with an annual effective dose in the 0.3-0.4 and 0.4-0.5 mSv range. Overall, these results suggest that low-dose IR exposure can affect the hematopoietic system causing early changes in hematological parameters that can differ according to the cumulative dose experienced. Although the mechanisms underlying such effects have not been fully elucidated, a direct damage to the hematopoietic stem cells that can affect the capacity of the bone-marrow stromal elements to support and/or maintain hematopoiesis, but also the impact of the IR exposure on the redistribution and apoptosis of mature elements of the blood can be involved. In this perspective, the authors argued that lower IR doses may induce hemolysis, and that at higher levels of exposure erythropoiesis can be enhanced, thus determining an increase in the hematological parameters RBCs, HB and HCT. 29
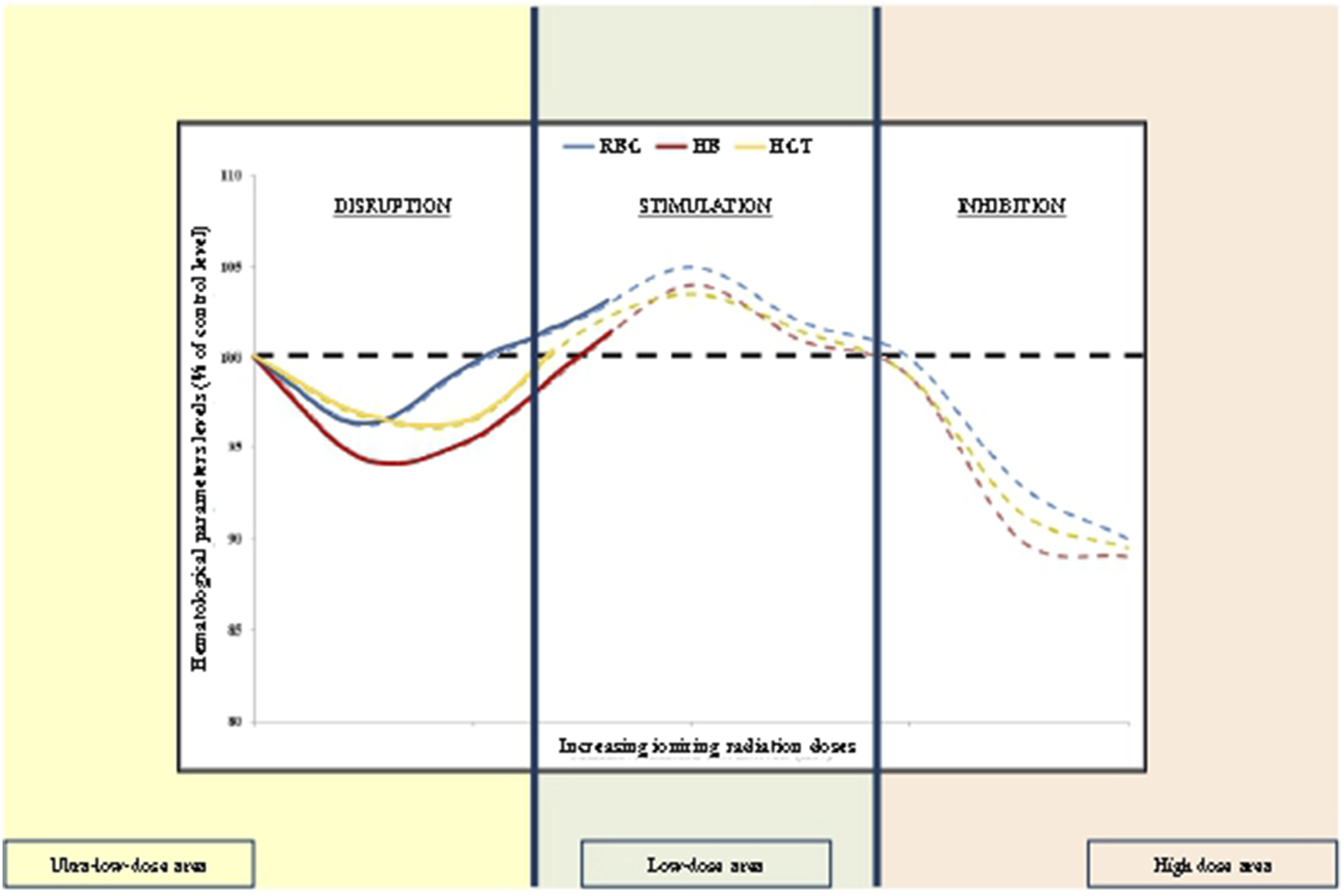
These hypotheses may characterize a possible view to interpret also our results and, especially, the non-linear dose-response relationship determined The possible increased susceptibility of RBCs to hemolysis, at the lowest cumulative doses, would be due to the ability of IR to increase the fragility and vulnerability to rupture of their cell membrane, consistent with findings in the literature.41,42 At these levels, the degree of hemolysis is likely too low to trigger compensatory mechanisms. However, as the cumulative dose of exposure increases, the enhanced hemolysis induces a stronger compensatory activation (i.e., erythropoiesis), which allows a stimulatory effect (RBC, HB, and HCT values exceed those found in the control group).29,43 However, future molecular investigations are necessary to verify and confirm this possible mechanism of action. Additionally, the data from our study would be suggestive of a triphasic dose-response (TDR) curve. TDR is a very interesting, but much less studied, phenomenon related to the well-known hormetic responses, basically be characterized by ultra-low-dose inhibition, low-dose stimulation and high-dose inhibition. 44 IR-induced TDR was first observed by Hooker et al 44 evaluating the chromosomal inversion frequency in the spleen tissue of pKZ1 mice. In detail, their findings revealed three different phases of response with an initial induction of inversions (at ultra-low doses) followed by a decrease (below endogenous inversion frequency) at low doses and then again an increase at the higher exposure doses.44,45 A similar TDR was also observed measuring the number of apoptotic events in an in vivo study performed on the embryos of zebrafish (Danio rerio) exposed to 150 kV X-rays with different levels of hardness. 46 These findings may suggest that TDR in IR exposed living organisms may be a much more common phenomenon than heretofore observed. 46 In this regard, it is plausible to speculate that our data fit well and provide support for a TDR even though the cumulative dose intervals investigated in this study are very low and thus allow us to observe only the first two areas of the TDR (ultra-low-dose inhibition and low-dose stimulation). However, such a peculiar dose-response relationship needs to be confirmed under experimental and longitudinal occupational studies to verify whether such biological changes may be effectively related to the IR exposure or to the intrinsic variability in hematological parameters that could have biased the obtained findings. Additionally, occupational exposure to low-dose IR may affect the antioxidant status of radiation workers, in turn responsible for hematological changes. 29 A radiation hormetic phenomenon has been reported by Tian et al 29 with respect to the glutathione (GSH) levels that have been reported to increase with annual effective dose from 0 mSv to 0.5 mSv, but reduced after 0.5 mSv. Under low-dose range, IRs may induce the elevation of GSH level in order to facilitate scavenging radical oxygen species (ROS); when the cumulative dose continues to rise, the decline in GSH concentration may be a disadvantage to scavenging ROS.
Although interesting results emerged from our investigation, some limits should be considered for their correct interpretation, in order also to plan suitable future investigations. First of all, the number of the enrolled workers should be enlarged to obtain more representative samples of the healthcare population exposed to IRs. This may allow to extrapolate information relative to the different job tasks performed, e.g., physicians, nurses or technicians, and to determine the possible confounding role of other occupational exposures, that may have additive or synergic effects on the hematopoietic system.
Conclusion
The present study allowed to demonstrate different effects exerted by diverse levels of low-dose IR exposure on hematological parameters. For the RBC, HB and HCT values, our results confirm the occurrence of a radiation hormetic phenomenon, characterized by an adaptive response at low doses, more than adverse health effects. This appears extremely important from a risk assessment and management point of view. Additionally, we could demonstrate the possibility to employ early changes induced by IRs in occupationally exposed populations to guide appropriate biological monitoring strategies for health surveillance plans. Although interesting, future, large multicenter longitudinal studies are warranted to more deeply investigate these alterations in various exposed populations considering the doses of exposure, as well as all the factors that may impact on the IR exposure, such as the type of work and the length of employment, together with possible conditions of co-exposure, e.g., to chemical agents, or environmental and lifestyle factors. This may allow to confirm the obtained findings, in the attempt, also, to explain the different results achieved for the diverse hematological parameters investigated. Experimental and epidemiological studies on workers, integrated with molecular epidemiology and system biology investigations may ensure a suitable multidisciplinary approach to extrapolate data able to provide guidance to appropriate IR risk assessment and management strategies.
Footnotes
Authors’ Note
The U.S. Government is authorized to reproduce and distribute for governmental purposes notwithstanding any copyright notation thereon. The views and conclusions contained herein are those of the author and should not be interpreted as necessarily representing policies or endorsement, either expressed or implied. Sponsors had no involvement in study design, collection, analysis, interpretation, writing and decision to and where to submit for publication consideration.
ORCID iDs
Ethical Statement
Author Contributions
Veruscka Leso: Conceptualization, Methodology, Writing – original draft, Writing – review and editing; Luca Fontana: Conceptualization, Methodology, Writing – original draft, Writing – review and editing; Daniela Pacella: Methodology, Formal analysis, Writing – review and editing; Giuseppe Barbato: Data curation, Writing – original draft; Vincenzo della Puca: Data curation, Writing – original draft; Edward J. Calabrese: Writing – original draft, Writing – review and editing; Ivo Iavicoli: Conceptualization, Methodology, Writing – original draft, Writing – review and editing, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. EJC acknowledges long-time support from the US Air Force (AFOSR FA9550-19-1-0413) and ExxonMobil Foundation (S18200000000256).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the Corresponding author on reasonable request.