
Abstract
The Hiroshima/Nagasaki (H/N) studies by the Radiation Effect Research Foundation have not shown increased leukaemia for acute doses below 200 milli-gray (mGy). By contrast the INWORKS study of leukaemia in workers stated: “This study provides strong evidence of positive associations between protracted low-dose radiation exposure and leukemia”. The INWORKS study also claimed increased leukaemia, not including Chronic Lymphocytic Leukaemia, at cumulative occupational doses of less than 100 mGy. This is contrary to the expectation that the H/N studies would show more severe effects than the worker study because the doses were acute instead of chronic and because the H/N studies included children who had higher rates of radiation induced leukaemia than adults. This paper shows that the INWORKS leukaemia study is consistent with the H/N studies in showing no increase in leukaemia in the low-dose range. In addition, any increase in leukaemia is confined to Chronic Myeloid Leukaemia, possibly from high radiation dose-rates or chemicals.
Introduction
UNSCEAR summarizes the Radiation Effects Research Foundation (RERF) evidence for leukaemia in the Hiroshima and Nagasaki (H/N) Life Span Study cohort as: Acute Myeloid Leukaemia (AML), Acute Lymphoblastic Leukaemia (ALL), and Chronic Myeloid Leukaemia (CML) were “radiation-inducible”. Statistical significance for increased risk vanishes for acute doses less than 200 milli-gray (mGy). 1 Chronic Lymphocytic Leukaemia (CLL) was not increased in H/N survivors.
Regarding RERF and other studies, the UNSCEAR 2013 summary included in the 2019 report noted 2 : “the observational studies had not shown a statistically significant increase in leukaemia incidence at doses to the RBM (Red Bone Marrow) of less than about 400 mGy”. Age dependence was summarized as: “the risk of leukaemia associated with an exposure during childhood appeared to be 3 to 5-fold greater than that with the same exposure during adulthood”.
The Leuraud et al INWORKS study 3 : “quantified associations between protracted low-dose radiation exposures and leukaemia, lymphoma, and multiple myeloma mortality among radiation-monitored adults employed in France, the UK, and the USA”. The H/N doses were in seconds instead of being accumulated over years or decades as in the INWORKS study. Furthermore, the H/N cohort included about 40% children whose susceptibility to leukaemia from radiation was 3 to 5 times that of adults. Therefore, the INWORKS study would be expected to find less radiation induced leukaemia. However, the INWORKS study indicated increased leukaemia mortality for low protracted doses to adults, mostly males, below 100 mGy; whereas the H/N studies do not show excess risk for acute doses below 200 mGy to adults and children of both sexes. This paper attempts to reconcile the INWORKS and the H/N studies.
INWORKS Leukaemia Study
Leuraud et al studied worker mortality from leukaemia, lymphoma, and multiple myeloma in the INWORKS cohort of nuclear workers from the US, UK, and France using 90% confidence intervals (CI). 3 There were just over 308 000 workers, a total of 22% died, 87% were male. Workers had just over 8 million Person Years (PY) follow-up with a mean of 27 years within the 61 years from 1944 to 2005. Average cumulative occupational photon dose was 25 mGy, however, this was converted to 16 mGy average cumulative occupational red bone marrow (RBM) photon dose for this study. 4 Not included were the substantial: occupationally required medical doses, lagged doses, neutron and internal doses, doses from before the dose registries were instituted, and of course unmeasured doses.5,6 Also not included were lifetime non-occupational doses that were 5 or more times the occupational doses. Cumulative, occupational, photon, RBM dose is referred to herein simply as dose.
The dose records and death certificates for these workers plus the national registries were analyzed in terms of PY to estimate the dose response. The statistics for 6 dose bins were listed in the supplementary information. 7 The dose bins and percent of total PY are: the control bin (0-5 mGy) with 65% of the PY, 5-50 mGy dose bin with 28% of the PY, 50-100 mGy with 4% of PY, 100-200 mGy with 2% of PY, 200-300 mGy with just over 0.5% of PY, and >300 mGy dose bin with under 0.5% of the PY. The percentage of the subjects in each bin parallels the percentage of the PY. 7
Low average dose rates are emphasized in the abstract: “Doses were accrued at very low rates (mean 1.1 mGy per year, Standard Deviation 2.6)”. The major result was Excess Relative Risk (ERR), an LNT quantity: “The excess relative risk of leukaemia mortality (excluding chronic lymphocytic leukaemia) was 2.96 per Gy (90% CI 1.17-5.21; lagged 2 years), most notably because of an association between radiation dose and mortality from chronic myeloid leukaemia (excess relative risk per Gy 10.45, 90% CI 4.48-19.65)”. The abstract concludes: “This study provides strong evidence of positive associations between protracted low-dose radiation exposure and
The study investigated ALL, AML, CML, CLL, and OTHER forms of leukaemia as well as Non-Hodgkins Lymphoma, Hodgkins Lymphoma, and Multiple Myeloma. Non-Hodgkins Lymphoma, Hodgkins Lymphoma, and Multiple Myeloma did not have statistically significant positive dose associations and so are not discussed further.
The study calculated: doses of each subject, Relative Risk (RR) of each dose bin for each disease subtype, average dose per bin, and related data listed in the supplementary information. 7
Pooling Disparate Data Sets
Leuraud et al pools the data for CML, AML, ALL, and OTHER because previous studies, principally from H/N, indicated that all of these caused leukaemia.1,2,8 However, the INWORKS cohort does not include children which typically contract ALL and AML. In addition, the H/N cohort is over 50% female, but the INWORKS cohort is only 13% female, with about 20% of the average dose of males. 9 Furthermore, an increase in CLL was not observed in the H/N cohort, however, Japan has much lower CLL rates than Western countries and so this effect may be different in the INWORKS cohort. Another difference is dose-rates are typically much lower. Therefore, the H/N results should not be used to determine what types of leukaemia to pool in this worker study. Instead, the study should determine which types of leukaemia are associated with radiation and should be pooled.
Figure 1 plots the RR for the 4 types of leukaemia listed in the supplementary information for Leuraud et al and OTHER, which does not include the 4 main types of leukaemia. The Excel trendlines are plotted to indicate correlation. CML (solid line) is positively correlated with dose, ALL and CLL (dotted lines) are negatively correlated, and AML and OTHER (dashed lines) are essentially uncorrelated. For H/N, the dose response in children was greater for acute forms of leukaemia and in adults it was greater for CML. Only CML has a positive dose response for the INWORKS cohort. RR vs. dose and the trendlines for five types of leukaemia.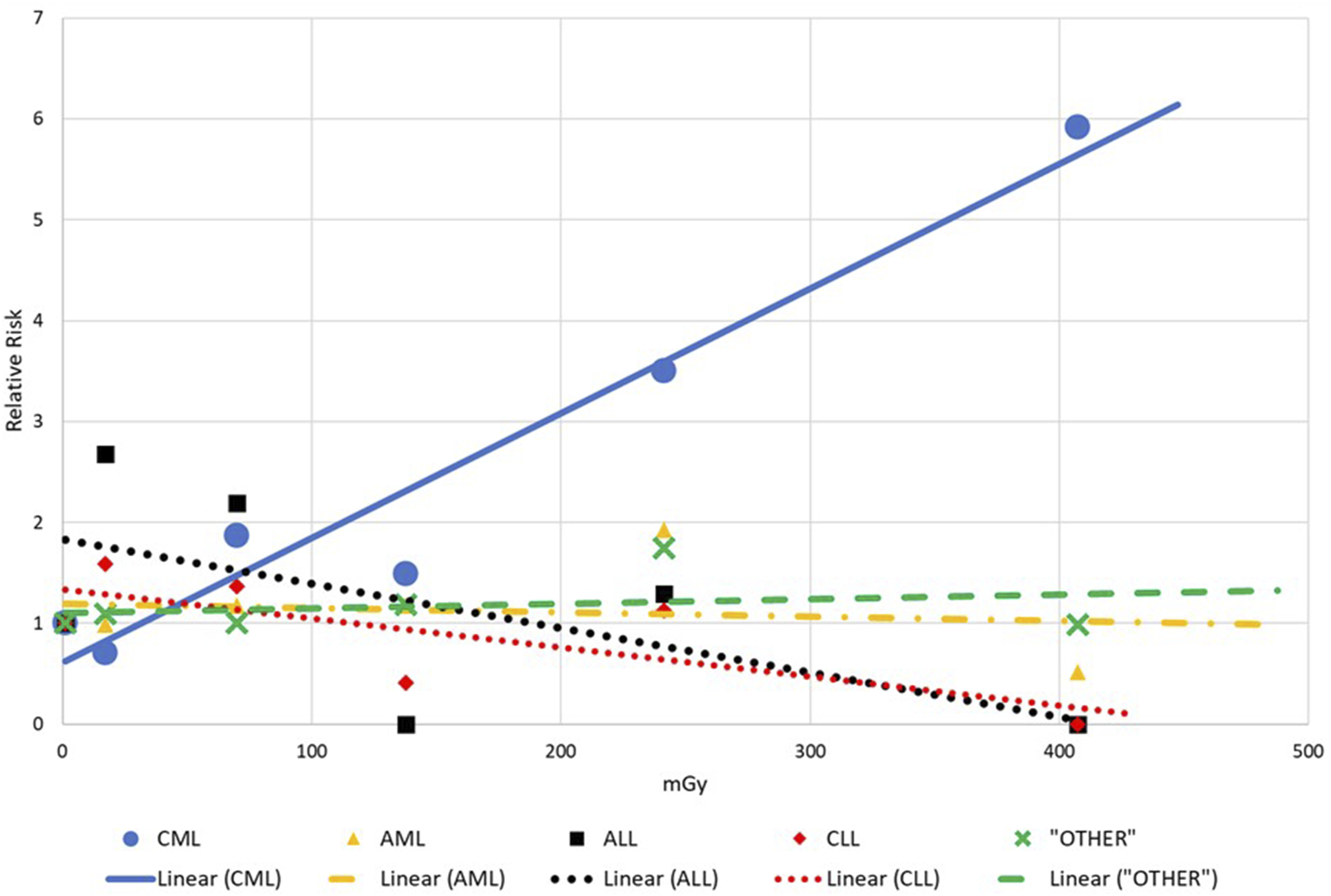
Figure 2, which plots the 6 RR points for ALL, shows a problem with calculation of ERR. The solid line represents the ERR of 5.80 found by Leuraud et al The dotted line is the negatively sloped trendline for the 6 RR points. The solid ERR line results from setting the intercept to RR = 1 and combining the 2 points with RR = 0 and the point indicated by an arrow which has just 1 ALL case. These actions mean that ERR depends upon just 3 data points and does not represent the data. This ERR does not represent the data because the RR for the 5-50 mGy data point is statistically significant above RR = 1 at 2.68 and there are no cases in the highest dose bin. RR vs. dose for ALL; Excel trendline is dotted and ERR line is solid.
ERR and Trendline Slopes.

The Leuraud et al abstract states the main result, ERR = 2.96/Gy, which is entirely due to CML since removing CML, as done in the last line of Table 1, produces a negative trendline slope and R∧2 of 0.002. The Leuraud study compares ERR for leukaemia, excluding CLL, in several case studies. However, these ERR should not be calculated since CML, AML, ALL, and OTHER should not be pooled.
LNT vs Threshold Model for CML
Summary of CML Deaths.
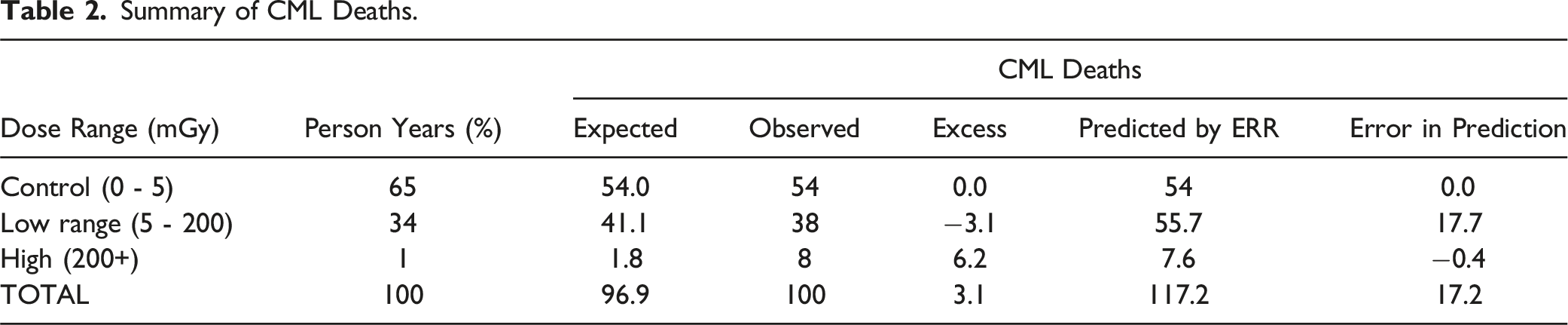
Table 2 also compares CML mortality as predicted by the ERR of 10.45/Gy to observed numbers of CML deaths. The ERR predicts 55.7 deaths in the low-dose range but only 38 were observed. LNT does not represent CML due to the large absolute (17.7) and almost 50% relative error in the low-dose range. This data supports a threshold of about 200 mGy, and not LNT, in agreement with the H/N studies. This data also shows that excess CML, and indeed leukaemia excluding CLL, is due entirely to the 8 workers who died of CML in the high-dose range.
Leuraud et al states: “The ERR of leukaemia excluding CLL was not attenuated when restricted to doses of less than 300 mGy or less than 100 mGy”. This is a markedly different viewpoint from Table 2 and requires an explanation. CML in the 0-100 mGy range has only 3 data points: the 0-5 mGy control point, the 5-50 mGy bin with RR = 0.71, and the 50-100 mGy bin with RR = 1.87. These 3 points produce an ERR of about 10/Gy. However, there are about 7 times more PY in the 5-50 mGy bin than the 50-100 mGy bin and together these bins have 4.7 fewer deaths than expected. Simply changing the dividing line between the 2 bins from 50 mGy to, for example, 40 mGy would make RR <1 for both bins. This would then make the ERR over the 0-100 mGy range negative. This shows that changing bin boundaries can change the appearance of the data and the calculated ERR substantially. Leuraud et al claimed for the less than 100 mGy dose range: “90% CIs were much wider when based on data for the restricted dose range”. Instead, it should have been admitted that there was no statistical significance even with 90% CI. In summary, LNT is inappropriate for CML and a threshold of 200 mGy best describes this data.
Temporal Analysis of CML
A follow-up to the INWORKS studies, with many of the same authors, detailed the time-based characteristics of cancers particularly CML. 10 The ERR listed in the supplementary information shows that many of the 8 high-dose CML deaths occurred after age 80, fewer between 60 and 80, and still fewer before age 60. 11 If we assume that the ERR is proportional to the number of deaths in the high-dose range, then the 8 high-dose CML deaths would be distributed as: 1 before age 60, one or 2 between 60 and 80, and five or 6 after age 80. This would mean that these 8 lived relatively long lives.
Furthermore, the RERF found that leukaemia mortality among Hiroshima/Nagasaki survivors peaked between 2 and 10 years after exposure and then declined rapidly for CML but less so for AML among children. 7 The INWORKS study found ERR was high for 2-10 years after exposure, and it was more than double that for 20-30 years after exposure. However, ERR was negative for both 10-20 years or greater than 30 years after exposure. If we assume that ERR is proportional to the number of high-dose CML deaths, then there are 2 or 3 high-dose CML deaths 2-10 years after exposure and 5 or 6 high-dose CML deaths 20-30 years after exposure. The RERF and INWORKS results taken together suggest that the 2 or 3 high-dose CML deaths 2-10 years after exposure, and likely before age 75, possibly were due to nuclear work. The 5 or 6 high-dose CML deaths 20-30 years after exposure were after age 80 and were likely not due to nuclear work.
Discussion and Conclusion
The H/N RERF studies concluded there was no increase in leukaemia excluding CLL below 200 mGy. Leuraud et al investigated dose response for 8 forms of disease and suggested there was a linear dose response for leukaemia excluding CLL that extended below 100 mGy. This paper attempts to reconcile the 2 viewpoints.
The major conclusion of Leuraud et al was that CML, ALL, AML, and OTHER had an ERR of 2.96/Gy, an LNT result. However, these should not be pooled since CML is positively correlated, ALL is negatively correlated, and AML and OTHER have no dose dependence. A secondary point is that if the ERR does not represent the data, as for ALL, then it should not be reported.
Leuraud et al found a statistically significant ERR of 10.45/Gy for CML. However, Table 2 has fewer CML deaths than expected, even without radiation, below 200 mGy. A threshold model better describes this data than LNT since there are about 17 fewer CML deaths than LNT predicts below 200 mGy, which is a large absolute and relative error. Leuraud et al suggested that there is a very high ERR for CML for the dose range of 0-100 mGy. However, this is not true since the ERR would be negative over the 0-100 mGy dose range if the boundary between the 2 bins is moved from 50 mGy to, for example, 40 mGy.
Table 2 has 8 CML deaths in the high-dose range above 200 mGy when only 2 were expected. It was shown that 5 to 6 of 8 died after the age of 80, likely not due to nuclear work. The other 2 to 3 died before 80 possibly due to nuclear work.
These 2 to 3 should be investigated further. Were they related. Did they work in the same facility or with the same chemical process? What were their actual recorded doses? Were they involved in the same accidents or cleanups? Of the 100 people that died of CML, 21 were exposed to neutrons. 3 Did these 2 to 3 workers have neutron exposures? This high-dose range has lifetime cumulative RBM average dose of about 300 mGy, but the actual average dose measured, as opposed to RBM dose, is about 500 mGy. 4 The actual dose for these 2 or 3 workers might be much greater than the average of 500 mGy and could be much greater still if internal contamination and neutrons were included. These workers might have had very high maximum dose-rates on specific days. For example, 400 Fukushima workers had low and protracted doses for most of their career and then received from ∼100 mGy to 250 mGy in 2011, March. There were many accidents and high dose-rates in the early years of the study. If total dose exceeded 100 mGy in a month, then low protracted doses should not be considered responsible.
This paper concluded that ALL, AML, and OTHER should not be pooled with CML since they are negatively correlated or uncorrelated with dose. CML does have a positive dose response, but only in the high-dose range due to or 3 worker deaths. Leuraud et al has not shown that low protracted doses cause CML. Finally, there is no evidence of increased leukaemia below 200 mGy RBM photon dose in both the INWORKS and H/N data.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.