
Abstract
The endoplasmic reticulum (ER) is an important cellular organelle, and ER dysfunction has an important impact on a variety of biological processes. In this study, we explored the role of ER stress in cervical cancer by establishing a prognostic model related to ER stress. This study included 309 samples from the TCGA database and 15 pairs of RNA sequencing data before and after radiotherapy. ER stress characteristics were obtained by the LASSO regression model. The prognostic value of risk characteristics was analyzed by Cox regression, Kaplan‒Meier, and ROC curves. The effects of radiation and radiation mucositis on ER stress were evaluated. We found that ER stress-related genes were differentially expressed in cervical cancer and could predict its prognosis. The LASSO regression model suggested that risk genes had a strong ability to predict prognosis. In addition, the regression suggests that the low-risk group may benefit from immunotherapy. Cox regression analysis showed that FOXRED2 and N staging could be independent factors affecting prognosis. ERN1 was significantly affected by radiation and may be related to the occurrence of radiation mucositis. In conclusion, ER stress activation might have a high value in the treatment and prognosis of cervical cancer and has good clinical prospects.
Introduction
Cervical cancer is the fourth most common malignant tumor in the world, and it is still the second leading cause of female cancer deaths in developing countries. 1 The prognosis of cervical cancer depends on the treatment effect.2,3 About 20–22% of cervical cancer patients relapse within 5 years after treatment. 4 Radiotherapy is the main treatment of cervical cancer. 5 The main methods include external beam radiosity (EBRT) and brachytherapy.6,7 The early cervical cancer without metastasis can be effectively treated by radical hysterectomy plus adjuvant radiotherapy and chemotherapy. 8 The 5-year survival rate can reach 88%–95%. 9 However, for patients with advanced cervical cancer, traditional treatment methods have not achieved satisfactory results.
ER stress is a homeostasis imbalance in the ER caused by the accumulation of unfolded or misfolded proteins and the change of calcium concentration.10,11 At present, many studies have proved that ER stress is involved in the occurrence and development of various human cancers. 12 ER stress is associated with autophagy in gastric cancer and glioma.13,14 However, excessive and persistent ER stress may trigger programmed cell death or apoptosis. 15 For example, drug-induced apoptosis of lung cancer cells is related to endoplasmic reticulum stress. 16 ER stress is closely related to mitochondrial function in cervical cancer and breast cancer, drugs play an anti-cancer role through mitochondrial dependent ER stress pathway.17-19 In addition, ER, as a self-protection mechanism of stress, is involved in the proliferation of cancer cells under hypoxic environment and resistance to radiotherapy or chemotherapy. 20 At present, studies have shown that squalene cyclooxygenase inhibitors, as a new tumor specific radiosensitizer, can improve the radiotherapy effect by promoting ER stress and inhibiting homologous recombination. 21 Moreover, the activation of ER stress related genes is related to inflammation and immune infiltration. 14 The combination of immunotherapy and radiotherapy has become a popular research field after the publication of the PACIFIC22,23 and PEMBRO-RT studies.24,25 ER stress activation is an independent prognostic factor of glioma patients, and it can promote the infiltration of macrophages, which has been confirmed in glioma. 26 In clinic, targeted therapy combined with immunotherapy can prolong the survival time of patients. 27 However, it did not achieve the desired efficacy, which suggests that we should conduct more in-depth molecular research to reveal new targets to guide clinical individualized treatment.
To sum up, ER stress may be a potential tumor treatment target in the future. However, in cervical cancer, the relationship between ER stress and tumor biological characteristics, immune invasion, radiotherapy, and clinical prognosis is still unclear, which is worthy of our in-depth study.
Methods
Datasets
The transcriptome RNA sequencing data and clinical data of the FPKM file were downloaded from The Cancer Genome Atlas (TCGA) database. Patients with incomplete survival information were excluded. 309 samples were downloaded, including 306 cervical cancer samples and 3 normal tissue samples of adjacent cancer.
Endoplasmic Reticulum Stress Genes Acquisition
The MSigDB database (http://www.broad.mit.edu/gsea/msigdb/) downloaded 255 endoplasmic reticulum (ER) related genes.
Clinical Samples and Data Collection
In this study, we collected 15 patients with cervical cancer (FIGO Ⅱ b–Ⅳ b) undergoing radical radiotherapy from June 2021 to December 2021. Before the patient started external radiation therapy (about 1–3 days before treatment), gynecological examination were carried out to comprehensively evaluate the tumor focus. At this time, a small piece of tumor tissue and normal tissue adjacent to the tumor were taken as samples before radiotherapy. When the patient had accumulated 20–40 Gy of external irradiation, the gynecological examination were performed again to evaluate whether the tumor size was suitable for intraluminal irradiation. At this time, a small piece of tumor tissue and normal tissue adjacent to the tumor were taken again as samples after radiotherapy. Immerse the specimen in formalin liquid and store it at −80°C. The short-term radiotherapy effect and local mucosal reaction of patients were recorded (Supplementary Table 1 recorded patient information).
Differential Genes Analysis
RNA sequencing was conducted with an Illumina Hiseq sequencing platform with 200-bp paired-end reads following the manufacturer’s protocol. For mRNA transcripts, DESeq software was used to screen known transcripts differentially expressed in different sample groups, meeting | log2FC |≥1 and P value<=.05 differential expression range. Differential transcripts between the two groups were screened as radiotherapy related genes (Supplementary Table 2 recorded the differentially expressed genes before and after radiotherapy) using the limma package in the R software to study the differentially expressed mRNA.
Survival and Cox Regression Analysis
Kaplan–Meier survival analysis was performed using R package survival and surviviner. Univariate and multivariate Cox regression were conducted to identify the independent risk factors of prognosis. The area under the ROC curve (AUC) was measured to indicate the accuracy of prognosis. The forest maps and nomogram were constructed by R package forestplot and rms.
Establishment of Risk Prognosis Model
The prognosis risk model of ER stress genes was established by using Lasso regression analysis. Patients were divided into two high- and low-risk groups according to the risk scores by using median as threshold. The R package glmnet and survival were used.
Gene and pathway correlation analysis
Collect the genes contained in the corresponding pathways and calculate the enrichment fraction of samples on each pathway in turn, so as to obtain the connection between samples and pathways. It was analyzed by R software GSVA package, and the correlation between genes and pathway scores was analyzed by Spearman correlation.
Immune Infiltration Analysis
CIBERSORT (http://cibersort.stanford.edu/) was used to calculate the composition of immune cells from the gene expression profiles. We calculated the infiltration levels of 22 immune cells in cervical cancer, as well as the difference of immune score between different groups.
Statistical Analysis
Use R software (version 4.1.0) to process all data and use R language to draw. The difference between the two groups of samples passed the Wilcox test, and the R software package ggplot2 was used for mapping. P < .05 was considered statistically significant.
Results
Differential Expression of ER Stress Genes in Cervical Cancer
The differential expression between cervical cancer and normal adjacent tissues was analyzed. As shown in Figure 1, there are 4093 differentially expressed genes in cervical cancer and normal adjacent tissues, including 1792 up-regulated genes and 2301 down-regulated genes. Then, the differentially expressed genes were intersected with 255 ER stress genes to obtain 47 ER stress genes differentially expressed in cervical cancer, including 21 up-regulated genes and 26 down-regulated genes (Supplementary Table 3). These results suggest that ER stress genes are differentially expressed in cervical cancer. Volcanic map shows differentially expressed genes in cervical cancer. Red represents up regulation and green represents down regulation. There are 4093 differentially expressed genes, including 1792 up regulation and 2301 down regulation.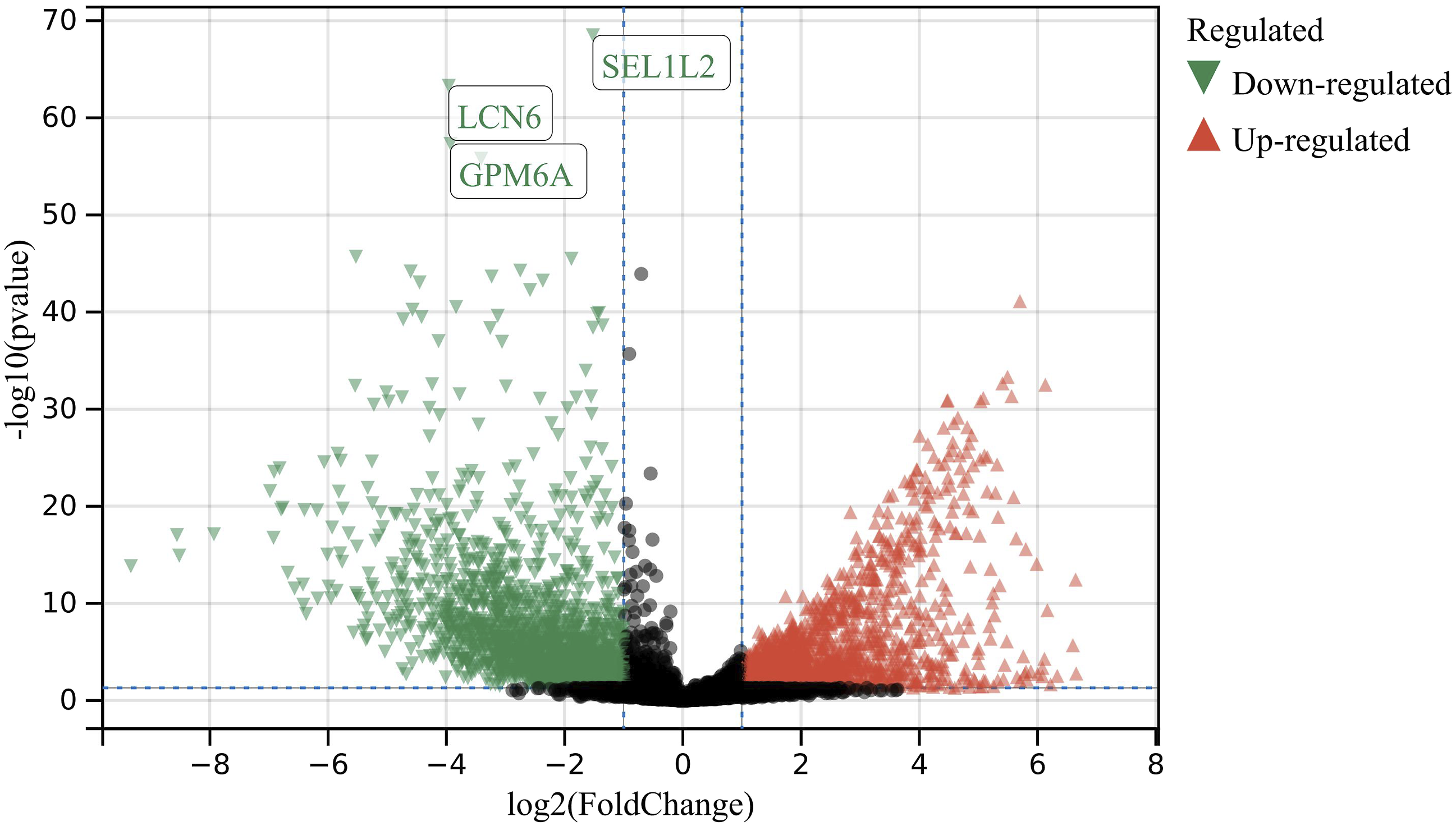
ER Stress Genes Predicted the Prognosis of Cervical Cancer Patients
We performed a batch prognostic analysis of 255 ER stress related genes downloaded from the MSigDB database and drew K-M curves. The results showed that 25 ER stress genes were associated with prognosis in cervical cancer (Supplementary Figure 1, P < .05). Among them, low expression of 16 genes indicates a good prognosis and high expression of 9 genes indicates a better prognosis, suggesting that ER stress related genes predict the prognosis of cervical cancer patients. In addition, we analyzed the expression of the above 25 genes in cancer tissues and adjacent tissues, and the results showed that a total of 12 genes were differentially expressed in cervical cancer and affected the prognosis (Figure 2(A) and (B)). Box diagram A and B show the expression of 25 ER stress related genes that have an impact on the prognosis. Among them, the differentially expressed genes in cervical cancer include BHLHA15, ERLEC1, ERN1, ERO1A, RNF139, RNF186, SERINC3, CDK5RAP3, ELAVL4, FOXRED2, PIK3R2, and RNFT2. Red represents normal tissue and blue represents cancer tissue.
Establish Risk Prognosis Model
In order to establish a comprehensive risk prognosis model, we performed LASSO regression analysis on 25 ER stress genes related to prognosis in TCGA cohort. First, the LASSO regression model was used to plot partial likelihood bias and log(λ), as shown in the figure, lambda. min = .0205 (Figure 3(A) and (B)). Then, 16 genes were identified as risk genes, and patients were divided into high-risk group and low-risk group according to the median risk score. The heat map showed the expression of 16 risk genes in the risk model (Figure 3(C)). The calculated risk score was Risk score = (−.2175) * ATP2A3+(.0268) * BHLHA15+(.1392) * CDK5RAP3+(.0981) * CXCL8+(−.0848) * DERL3+(.2798) * EDEM3+(−.6261) * ELAVL4+(.0556) * ERLEC1+(−.3856) * FOXRED2+(.1613) * HERPUD2+(.1235) * JUN+(.0808) * PDIA3+(−.0991) * PIK3R2+(−.2406) * SELENOK+(.3283) * SERINC3+(.0711) * TMCO1. As shown in the Kaplan–Meier curve in Figure 3(D), the low expression of risk genes indicates a good prognosis (P < .05). Based on 16 risk factors, a prediction model of 1-year, 3-year, and 5-year survival status was established. The ROC curve was shown in Figure 3(E). The AUC values of 1-year, 3-year, and 5-year were .76, .81, and .82, respectively. To sum up, ER stress genes significantly affected the prognosis of cervical cancer patients and had a strong predictive ability. The prognosis of low expression group of risk genes was better than that of high expression group. Establishment of risk prognosis model (A) Based on TCGA database, LASSO regression analysis was conducted on 25 ER stress genes (P < .05) that have an impact on prognosis, and 16 genes were screened as risk factors. (B) Partial Likelihood Deviation and Log(λ) Lambda. min = .0205. (C) The heat map shows the expression of 16 risk genes in the risk model. (D) K-M curve showed that the prognosis of low-risk group was better than that of high-risk group. Red represents low-risk group (L) and blue represents high-risk group (H). (E) The ROC analysis was used to judge the accuracy of the prediction model. Green, blue, and red represent the living conditions of 5, 3, and 1 years, respectively, and the corresponding AUC values are .82, .81, and .76, respectively.
ER Stress Gene FOXRED2 Was an Independent Risk Factor Affecting Prognosis
Combined with some clinical information, including age, T stage, N stage, univariate COX regression found that CXCL8, DERL3, EDEM3, ERLEC1, FOXRED2, HERPUD2, JUN, PDIA3, SERINC3, TMCO1, and clinical factors T stage, N stage were significantly correlated with the prognosis of patients (P < .05, Figure 4(A)). Then, multivariate COX regression analysis further confirmed that FOXRED2, and N stages can be used as independent prognostic factors for cervical cancer patients (Figure 4(B)). In particular, the low expression of FOXRED2 had strong statistical significance as a poor prognostic indicator (Figure 4(C)). These results suggested that the ER stress gene FOXRED2 may serve as a potential target to guide clinical treatment and prognosis. In addition, to reveal the potential mechanism of FOXRED2, we calculated the correlation between FOXRED2 and 20 common pathways (Supplementary Figure 2). The results showed that the Pearson correlation coefficients between FOXRED2 and G2M checkpoint, DNA replication, and IL1 Anti-inflammatory signaling pathway were .38, .36, and .33. It was suggested that FOXRED2 may be related to the above three pathways. Single factor/multi factor COX analysis(A) univariate/multivariate COX regression analysis of 16 risk factors in cervical cancer combined with clinical factors (age, T stage, N stage). (B) Multivariate COX analysis showed that FOXRED2 and N staging were independent risk factors for prognosis. (C) The nomogram can predict the overall survival period of 1, 3, and 5 years for patients with cervical cancer; Independent risk factors had the strongest predictive ability for 5-year survival rate.
Patients in Low-Risk Group May Benefit From Immunotherapy
In order to study the relationship between ER stress genes and immunotherapy in cervical cancer, we analyzed the mutation of immune checkpoint in high-risk groups. The results showed that CTLA4, HAVCR2, LAG3, PDCD1, and TIGIT were highly expressed in low-risk groups, suggesting that patients in low-risk groups were more likely to benefit from immunotherapy (Figure 5(A), P < .05). Then, to further explore the relationship with local immune microenvironment, we used CIBERSORT algorithm to calculate the infiltration proportion of 22 kinds of immune cells. By comparing the immune infiltration of high-risk group and low-risk group, it was found that T cells CD8 and Tregs had a particularly significant infiltration in low-risk group, while macrophages M0, mast cells activated, and neutrophils had a particularly significant infiltration in high-risk group (P < .0001, Figure 5(B)). In addition, NK cells resting, dendritic cells activated in high-risk group, B cells naive, plasma cells, T cells follicular helper, macrophages M2, and dendritic cells resting in low-risk group also infiltrated (P < .05), indicating that the immune infiltration in high- and low-risk groups was obviously different. The above results suggested that different immune cell infiltration may indicate that patients in different risk groups which can further predict the prognosis of patients. Correlation between high- and low-risk groups and immune events (A) Mutations of eight immune checkpoints in high-risk groups: CTLA4, HAVCR2, LAG3, PDCD1, and TIGIT were highly expressed in low-risk groups, with statistical significance (P < .05). (B) 22 kinds of immune cell infiltration in high- and low-risk groups: T cells CD8 and Tregs had a particularly significant infiltration in low-risk groups, while macrophages M0, mast cells activated, and neutrophils had a particularly significant infiltration in high-risk groups (P < .0001). NK cells resetting, dendritic cells activated in high-risk group, B cells naive, plasma cells, T cells follicular helper, macrophages M2, dendritic cells resetting in low-risk group were infiltrated (P < .05). Red represents low-risk group, blue represents high-risk group.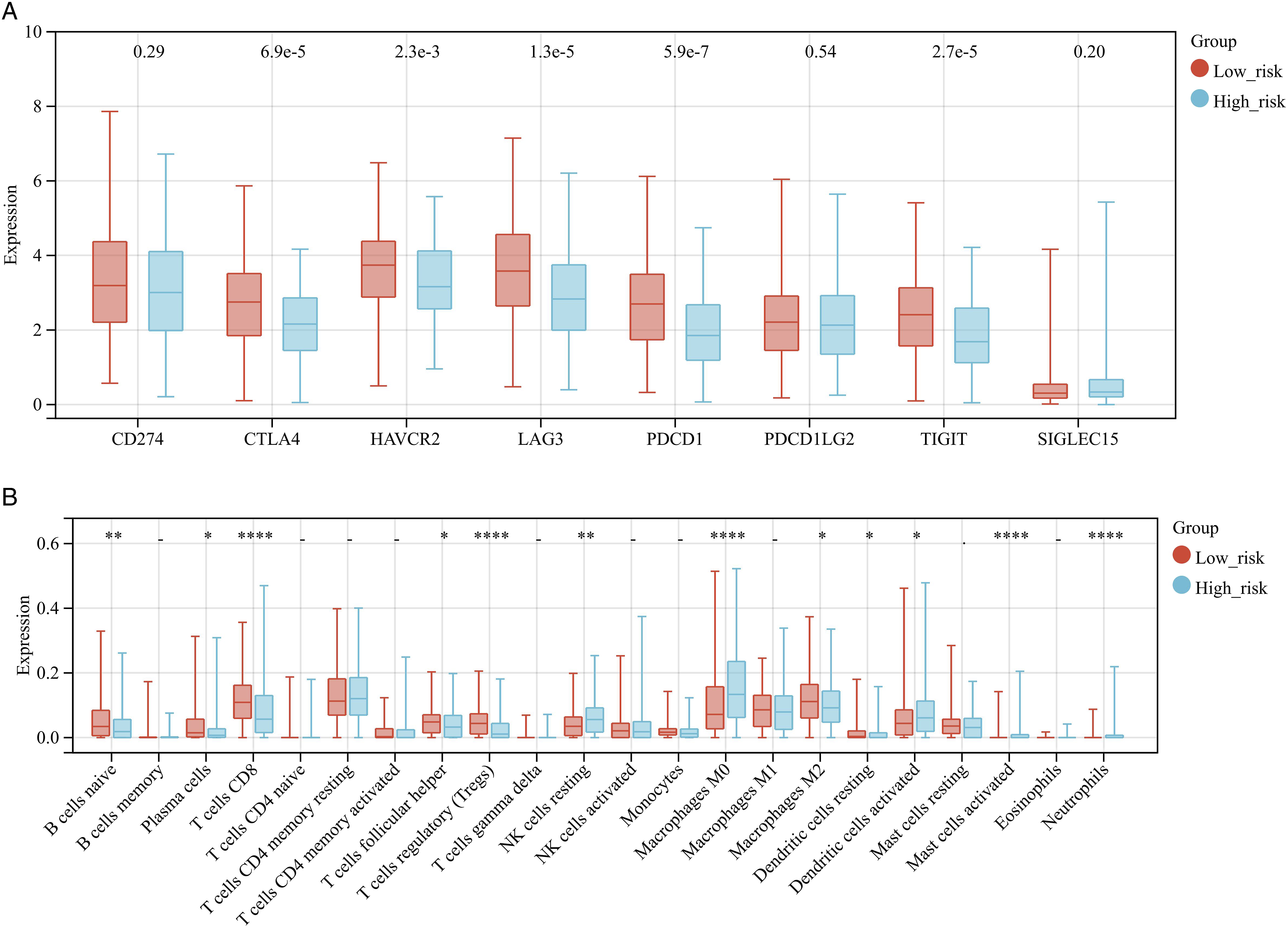
Acquisition of Differentially Expressed Genes in Cervical Cancer After Radiotherapy
We collected 15 cervical cancer patients requiring radical radiotherapy clinically, analyzed the sequencing data of 15 cervical cancer patients, and obtained 4675 differentially expressed genes before and after radiotherapy (Supplementary Table 2). Among them, 3275 genes were up-regulated and 1400 genes were down-regulated after radiotherapy (Figure 6). Volcanic map shows the differentially expressed genes in 15 patients with cervical cancer before and after radiotherapy. There are 3275 up-regulated genes and 1400 down-regulated genes after radiotherapy.
Radiotherapy and ER Stress Genes
We analyzed the relationship between 25 ER stress genes related to the prognosis of cervical cancer and radiotherapy. The results showed that radiotherapy could significantly change the expression of ER stress genes. The expression of BHLHA15 was significantly increased after radiotherapy, and the expression of FOXRED2 was significantly decreased after radiotherapy (Figure 7(A), P < .001). Then, we analyzed the correlation between radiation mucositis and ER stress genes expression, and divided the patients into mucosal reaction group and non-mucosal reaction group. The results showed that ERLEC1, ERN1, SERINC3, and TMED2 were highly expressed in the mucosal reaction group (Figure 7(B)), suggesting that the high expression of the four genes above indicated that the possibility of radiation mucositis after radiotherapy was greater. In addition, the occurrence of radiation mucositis may be regulated by some genes, which is worthy of further exploration. ER stress related genes and radiotherapy (A) Radiotherapy can significantly change the expression of ER stress genes. The genes with different changes before and after radiotherapy were: ATP2A3, BHLHA15, DERL3, ERN1, ERO1A, FOXRED2, PDIA3, PIK3R2, RNF175, TMCO1, UBQLN1 (P < .05), among which, BHLHA15, FOXRED2 had significant changes after radiotherapy (P < .001). Blue represents before radiotherapy and red represents after radiotherapy. (B) ERLEC1, ERN1, SERINC3, and TMED2 were highly expressed in the mucosal response group (P < .05). Red represents local mucosal reaction after radiotherapy, while blue represents no reaction.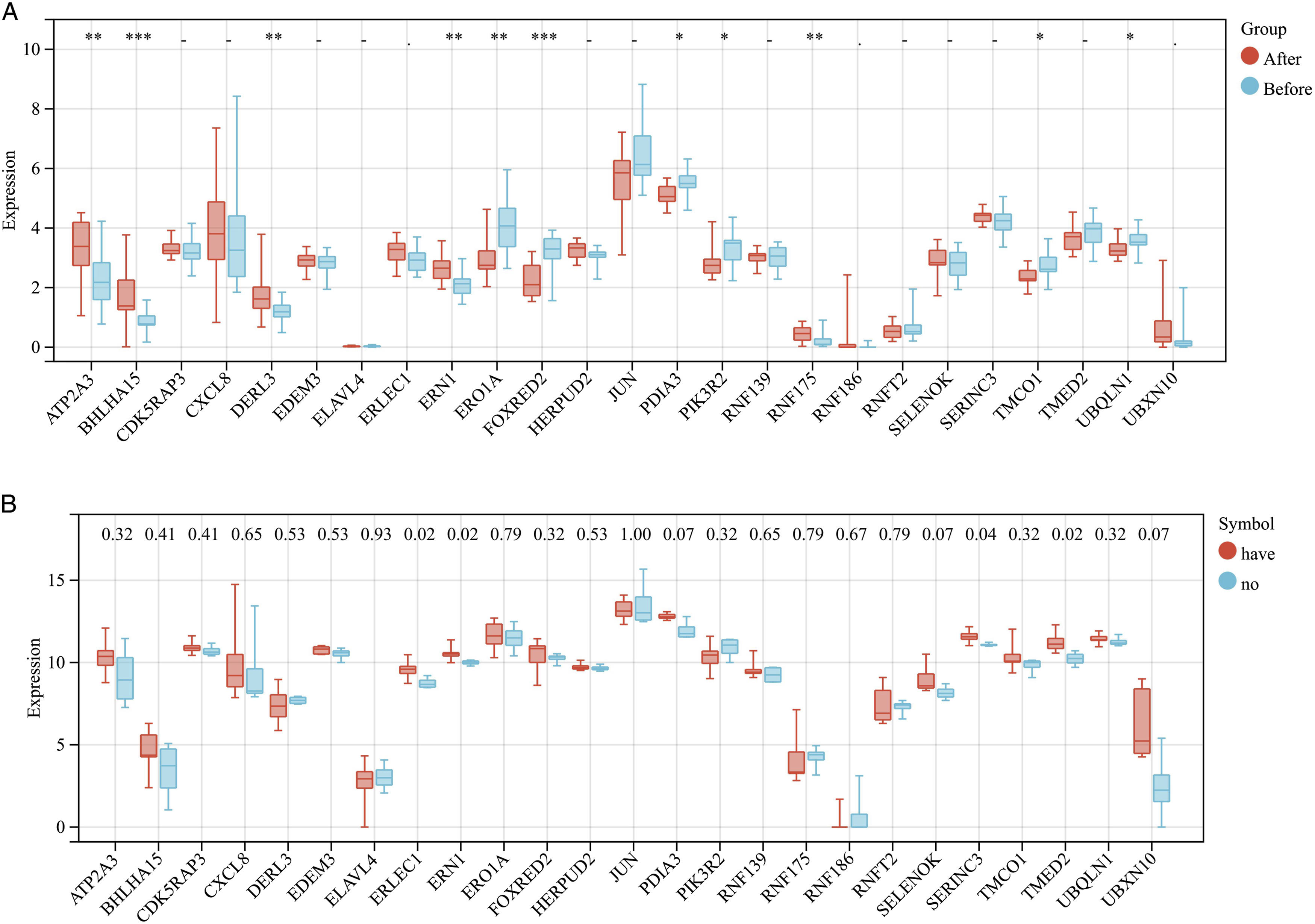
Discussion
At present, the treatment of cervical cancer has been significantly developed, but the task of finding an accurate target or improving radiotherapy sensitivity is a long way to go. In the past decade, ER stress has gradually come into the public’s view. It has proved that the impact on individualized treatment of tumors cannot be ignored in glioma, gastric cancer, breast cancer, and other cancers.13,14,20 At present, there are few studies in cervical cancer, which provides a new idea for improving individualized treatment of cervical cancer patients.
When cells are stimulated by various strong factors, cell homeostasis is broken. To survive, a series of protective events will be initiated, including endoplasmic reticulum stress. 28 However, cancer cells exposed to hypoxia tumor microenvironment and intracellular DNA damage stress are prone to endoplasmic reticulum stress, and these mechanisms have been proved to be involved in the progression and drug resistance of human cancer. 29 In addition, some studies have shown that the activation of ER stress can induce cancer cells to sleep, while cancer cells in the resting state are insensitive to radiotherapy and chemotherapy, which ultimately leads to tumor recurrence and progression. 30 However, the biological function of ER in cervical cancer has not been fully understood, especially the role of ER stress in regulating the prognosis, immune microenvironment, and radiotherapy effect of cervical cancer.
In this study, LASSO regression model, AUC prediction model, and COX regression analysis were established to confirm that ER stress related genes can regulate and predict the prognosis of cervical cancer patients. Combined with some clinical factors, we determined that gene FOXRED2 and N stage can be used as independent prognostic factors of cervical cancer patients. FOXRED2 is a gene related to ER stress, which is highly expressed in human tumors of non-small cell lung cancer, colorectal cancer, and breast cancer. Moreover, forced expression of FOXRED2 can target the hypoxia of tumor cells, and can be used as a target to activate certain drug action sites. 31 In non-small cell lung cancer, FOXRED2 gene is one of the genes with the strongest correlation with KRAS mutation. FOXRED2 mutation can make the prognosis of NSCLC even better. 32 In this study, the expression of FOXRED2 is higher than that of normal tissues adjacent to cancer, and the high expression indicates a better prognosis. This suggests that FOXRED2 gene may have the same effect in cervical cancer. However, in the follow-up analysis, we learned that the expression of FOXRED2 was significantly reduced after radiotherapy, which indicates that the effect of using some targeted drugs in cervical cancer patients after radiotherapy is lower than that before radiotherapy, which provides us with unique insights into the clinical application of targeted drugs and non-targeted drugs. Therefore, our research provides a new idea for understanding the potential role of ER stress related genes in the prognosis of cervical cancer and analyzes their use as potential biomarkers of cervical cancer.
Some studies have shown that the activation of endoplasmic reticulum stress can inhibit the anti-tumor immune response and provide opportunities for tumor formation. ER stress plays an important role in the occurrence and development of tumors. Clinical trials have shown that anti CTLA4 therapy combined with anti PD-L1 therapy has a good clinical application prospect in recurrent or metastatic cervical cancer. 33 PDCD1 overexpression is related to immune cell infiltration, especially Macrophages M0, M1, CD4-T-cells, CD8-T-cells, and T cells follicular helper. 34 TIGIT is a new target with good clinical prospects. There is sufficient evidence that TIGIT pathway regulates T-cell-mediated and natural killer cell-mediated tumor recognition in many cancers (including cervical cancer) in vivo and in vitro.35,36 In this study, we found that the expression of the above immune checkpoint was up-regulated in the low-risk group, and the prognosis of the low-risk group was better than that of the high-risk group, which suggested that ER stress related genes regulate tumor immunotherapy. This is consistent with the current research.37-39 In addition, T cells CD8 and Tregs were significantly infiltrated in the low-risk group. Current research shows that T cell infiltration is associated with poor prognosis, which is contrary to our research results,40,41 considering that it is caused by different grouping patterns. In this study, T cells CD8 and Tregs infiltration are good prognostic markers in the low expression group of risk genes.
Finally, we obtained the expression profile data of cervical cancer before and after radiotherapy and analyzed the relationship between ER stress related genes and radiotherapy. Some ER stress related genes were affected by radiation; BHLHA15 and FOXRED2 were most significantly affected by radiation. BHLHA15 has been proved to be related to colon tumorigenesis in mouse experiments, and less research has been done in tumor radiotherapy. 42 In this study, the gene FOXRED2 was confirmed to be an independent risk factor affecting the prognosis of cervical cancer, and its expression was significantly affected by radiation. Both can be used as new targets to guide clinical treatment. In addition, the expression of ERN1 increased after radiotherapy, and it was highly expressed in the mucosal reaction group. Current studies have shown that there is a close relationship between radiation-induced oxidative burst, UPR,, and autophagy induction, which may be related to ERN1/IRE1. 43 It can be inferred that ERN1 plays an important role in radiotherapy, and the occurrence of radiation mucositis may be regulated by genes, which are worthy of our in-depth study.
Conclusion
In this study, we comprehensively evaluated the impact of 255 ER stress related genes on the prognosis of cervical cancer patients. The results showed that there were 25 genes related to prognosis. By building a risk prognosis model, the low-risk group had a good prognosis. FOXRED2 and N stage could be regarded as independent risk factors affecting the prognosis. Then, it was found that the low-risk group might benefit from immunotherapy, and T cells CD8 and Tregs infiltration might suggest a better prognosis. Finally, radiotherapy could change the expression of ER stress related genes in cervical cancer tissue, and the occurrence of radiation mucosal reaction may be related to ERN1. These findings might provide an important reference for personalized clinical treatment and prognosis of cervical cancer.
Supplemental Material
Supplemental Material - Endoplasmic Reticulum Stress Could Predict the Prognosis of Cervical Cancer and Regulate the Occurrence of Radiation Mucositis
Supplemental Material for Endoplasmic Reticulum Stress Could Predict the Prognosis of Cervical Cancer and Regulate the Occurrence of Radiation Mucositis by Xue Liu, Jing Song, Hui Liu, Zhiqiang Sun, Huiwen Ren, Judong Luo in Dose-Response
Supplemental Material
Supplemental Material - Endoplasmic Reticulum Stress Could Predict the Prognosis of Cervical Cancer and Regulate the Occurrence of Radiation Mucositis
Supplemental Material for Endoplasmic Reticulum Stress Could Predict the Prognosis of Cervical Cancer and Regulate the Occurrence of Radiation Mucositis by Xue Liu, Jing Song, Hui Liu, Zhiqiang Sun, Huiwen Ren, Judong Luo in Dose-Response
Supplemental Material
Supplemental Material - Endoplasmic Reticulum Stress Could Predict the Prognosis of Cervical Cancer and Regulate the Occurrence of Radiation Mucositis
Supplemental Material for Endoplasmic Reticulum Stress Could Predict the Prognosis of Cervical Cancer and Regulate the Occurrence of Radiation Mucositis by Xue Liu, Jing Song, Hui Liu, Zhiqiang Sun, Huiwen Ren, Judong Luo in Dose-Response
Footnotes
Author Contributions
XL and J-DL contributed to the conception of this study. XL contributed significantly to analysis and manuscript preparation. HL guided bioinformatics analysis. JS, H-WR and Z-QS collected clinical samples. Final approval of manuscript by all authors.
Declaration of Conflicting Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82073339 ). Project of Wuxi Health Committee (Q202015).
Data Availability Statement
All data generated or analyzed during this study are included in its supplementary material files. Further enquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.