
Abstract
Background
Herd immunity against measles is essential to interrupt measles transmission, and this can only be attained by reaching at least 95% coverage for each of the 2 doses of measles vaccine provided in infancy and early childhood age group. It is important to provide everyone with 2 doses of the measles vaccine in order to effectively safeguard the population. Despite this, little is known about the second dosage of the measles vaccine utilization status and the factors that affect it. Therefore, this study aimed to assess second dose of measles vaccination utilization and its associated factors among children aged 24–35 months in Jabitehnan district, 2020.
Methods
A community-based cross-sectional study design was conducted at Jabitehnan District, Northwest Ethiopia, from September 1st, 2020 to October 1st, 2020. Systematic random sampling technique was used to select 845 mothers/caregivers who had children aged 24–35 months. Both bi-variable and multivariable logistic regression was fitted to identify the determinant factors of second dose measles vaccination utilization. Finally, the statistical significant variables were declared by using 95% CI and P value less than .05 in the multivariable logistic regression analysis. The Hosmer and Lemeshow test was used to check the model’s fit to the data, and the variance inflation factor was used to assess multi-collinearity.
Results
The overall second dose of measles vaccination utilization was 48.1%, (95% CI: 44.7-51.6). Mothers with primary school education (AOR = 1.91, 95% CI: 1.15-3.17), information about MCV2 (AOR = 6.53, 95% CI: 4.22-10.08), distance from vaccination site (AOR = 3.56, 95% CI: 2.46-5.14), knowledge about immunization (AOR = 1.935, 95% CI: 1.29-2.90), and favorable attitude about immunization (AOR = 5.19, 95% CI: 3.25-8.29) were significantly associated factors with second dose of measles vaccination utilization.
Conclusion
Second dose measles vaccination utilization in the district was lower than the national target. Maternal education, distances from vaccination site, information about MCV2, and knowledge about immunization were significantly associated variables with second dose measles vaccination utilization. Therefore, in order to increase the utilization of the second dose of the measles vaccine, improved health education and service expansion to difficult-to-reach areas are required.
Introduction
Every year, a large number of individuals die from the highly contagious disease measles. In 2019, an estimated 207 500 measles deaths were reported worldwide, of which, 147 900 (over 70%) occurred in African countries. 1 Around 134 200 children worldwide died from measles in 2015, making it a major public health issue. 2 There has been progress in the reduction of measles mortality in the last decade in Africa, 3 however, the disease remains an issue in the region,4,5 reflecting the challenge of sufficient herd immunity levels in areas where financial resources are limited.
Childhood immunizations are low-cost, safe, and effective interventions for reducing infant and under-five morbidity and mortality. 6 The majority (90%) of the unimmunized population are in low- and middle-income countries, many of whom are in South-East Asia and Africa. 7 In 2015, 20.8 million infants did not receive the first dose of the Measles Containing Vaccine (MCV1) through routine immunization; Ethiopia accounted for 3.4% of unimmunized infants 8 and 9% of the global measles mortality.9,10
Ethiopia’s childhood immunization coverage has improved through a combination of strategies that include the Reaching Every District (RED) approach, health extension programs, and implementation of Enhanced Routine Immunization Activities (ERIAs).11-13 Despite the tremendous efforts done to decrease measles disease in Ethiopia, measles outbreaks occur repeatedly in different regions of the country. There were 12 districts in Ethiopia where measles outbreaks were reported in 2022, affecting a total of 650 000 children. 14 According to WHO in Africa report in 2022, in Ethiopia, a total of 2755 cases were suspected, among which 2156 were confirmed measles cases. 15 Ethiopia introduced the second dose measles (MCV2) vaccination into the regular immunization program on February 11th, 2019 to be administered at 15 months of age due to continued measles outbreaks, despite the first dosage measles vaccination. 16 According to the 2019 Ethiopian Mini Demographic Health Survey (MDHS) report, immunization rates in Ethiopia remained below target, including for the second dose of the measles vaccination. Only 9.1% of children aged 24–35 months received the second dose of the measles vaccine in 2019. 17 In addition, little is known about the utilization and the determinant factors of second dose measles vaccination (MCV2). Therefore, this community-based study aimed to assess second dose of measles vaccination utilization and its associated factors among children aged 24–35 months in Jabitehnan district, 2020.
Methods
Study Design and Settings
This community-based cross-sectional study design was conducted at Jabitehnan District in Amhara region from 1st September 2020 to 1st October 2020. It is located 180 km from Bahir Dar, the capital city of Amhara region and 385 km from Addis Ababa, the capital city of Ethiopia. It is bordered on the west by Burie district, on the southwest by Sekela district, on the east by Dembecha district, and on the north by Quarit district. It has a total population of 226 000 and area of 1200.5 km2. It had 39 rural and 3 urban Kebeles, 41 health posts and 11 health centers. Health posts and health centers give vaccination services for children based on their residence: children who reside within 5 km radius of the health center receive their vaccination at the health center and those who reside beyond 5 km from the health center receive their vaccination in health posts and outreach settings (a total of 126 sites). Mothers/caregivers who had children aged 24–35 months and who had lived at least 6 months in Jabitehnan district were the source population, while mothers/caregivers who had children aged 23–35 months in the selected Kebeles of Jabitehnan district were the study population of the study. Those mothers/caregivers who were seriously ill during data collection period were excluded from the study.
Sample Size and Sampling Procedures
Sample size was determined by using single population proportion formula n =
Multi-stage systematic random sampling technique was used to select study participants. The district was stratified into 38 rural and 3 urban Kebeles, and 9 rural and 1 urban Kebeles (25% of Keble’s in both strata) were selected randomly. Samples were distributed proportionally by their number of households (HHs) having children aged 24–35 months of randomly selected Kebeles. Finally, eligible children aged 24–35 months were selected using systematic random sampling technique with “k” value of 2, and lottery method was used to select the first household for data collection of this study. A household having more than 1 child aged 24–35 months in this study was studied by selecting the young child and for twin selecting the one by lottery method.
Measurements and Variables
Second dose measles vaccination utilization was the outcome variable of this study. Socio-demographic characteristics (age, sex, residence, educational status, marital status, occupational status and income, number of infants, and religion), obstetrics-related factors (visits of antenatal care, postnatal care, illness of mothers, type of pregnancy, place of birth and maternal conference participation and birth attendant), access-related factors (time to reach vaccination site, mode of transportation, place of vaccination, and availability of electronic media and availability of telephone), and awareness-related factors (information about measles vaccine, knowledge, and attitude) were independent variables.
Second Dose Measles Vaccination Utilization
If a child had received the second dose measles vaccine between the ages of 15 and 24 months in addition to a first dose of measles vaccination received before, he/she was considered as having received the second dose measles vaccination, coded as “1.”
Knowledge
Eight knowledge assessment items were used and those who scored greater than 50% of the total knowledge measuring score were considered as having good knowledge. 18
Attitude
For Likert-scale attitude assessment items, strongly agree and agree were considered as positive and neutral, disagree and strongly disagree were considered as negative attitude. If respondents positively react, at least 75% or more of attitude questions were considered as favorable attitude.19,20
Data Collection Tools and Procedure
Data were collected through an interviewer-administered pretested structured questionnaire developed from different literatures,21-26 and information about children’s vaccination status was collected from children’s vaccination card and mothers/caregivers. Socio-demographic information, maternal health services, knowledge, access-related factors, and a child’s second dose of measles vaccination status were included in the questionnaire. Eight diploma and two BSC qualified nurses were recruited for data collection and supervision, respectively.
Data Quality Control
The questionnaire was prepared in English and translated to Amharic which is the local and working language in the study area and back to English by language experts to maintain consistency.
Prior to data collection, 1-day training was given for data collectors and supervisors on the study objectives, data collection instruments, techniques, and producers. A pretest was done on 43 mothers/caregivers (5%) at Dembecha district, nearby district, and necessary amendments were done based on the pretest findings. The consistency and completeness of data were checked by the principal investigator and supervisors on daily basis. The reliability of the tool was checked by investigators, and Cronbach’s α for measuring knowledge was .97, and attitudes .78, respectively, indicating good reliability.
Data Processing and Analysis
The data was entered into Epi-data version 4.6 Software and exported to SPSS version 23 for cleaning, coding, and analysis. Descriptive measures were computed to summarize the participants’ socio-demographic characteristics and second dose measles utilization. Bi-variable and multivariable logistic regression analysis was used to assess any association between each independent variable and second dose measles utilization. Independent variables with a P-value of less than .2 during the bi-variable logistic regression were entered into the multiple logistic regression analysis. Adjusted odds ratio (AOR) with a 95% confidence interval and P-value <.05 was used to show the association between explanatory and dependent variables. Variables with P-value of <.05 were considered as significant. Model fitness was checked using the Hosmer–Lemeshow goodness-of-a-fit test (P = .58), and multi-collinearity was also checked using the Variance Inflation Factor (VIF), VIF <10 and tolerance greater than .1 were used to declare the absence of multi-collinearity.
Results
Socio-Demographic Characteristics
Socio-demographic characteristics of mothers/caregivers of children aged 24–35 in Jabitehnan district (N = 837).

Obstetric History and Access Information, Maternal Awareness, and Attitude
Obstetric history, access information, maternal awareness, and attitude characteristics of mothers/caregivers with having children aged 24–35 months in Jabitehnan district, 2020 (N = 837).

Childhood Vaccination Utilization
Childhood vaccination utilization mothers/caregivers with having children aged 24–35 months in Jabitehnan district, 2020 (N = 837).

Factors Associated With Second Dose Measles Vaccination Utilization
After controlling for the effects of potentially confounding variables using multiple logistic regressions, finally, primary maternal education (AOR = 1.909, 95% CI: 1.149-3.169), information about MCV2(AOR = 6.525, 95% CI: 4.222-10.084), knowledge about immunization (AOR = 1.935, 95% CI: 1.293-2.895), distance from vaccination site (AOR = 3.560, 95% CI: 2.464-5.144), and favorable attitude about immunization (AOR = 5.192,95% CI: 3.250-8.294) remained significant in the multivariate analysis (P ≤ .05).
Factors associated with childhood second dose vaccination utilization of mothers/caregivers who had children aged 24–35 months in Jabitehnan district, 2020 (N = 837).
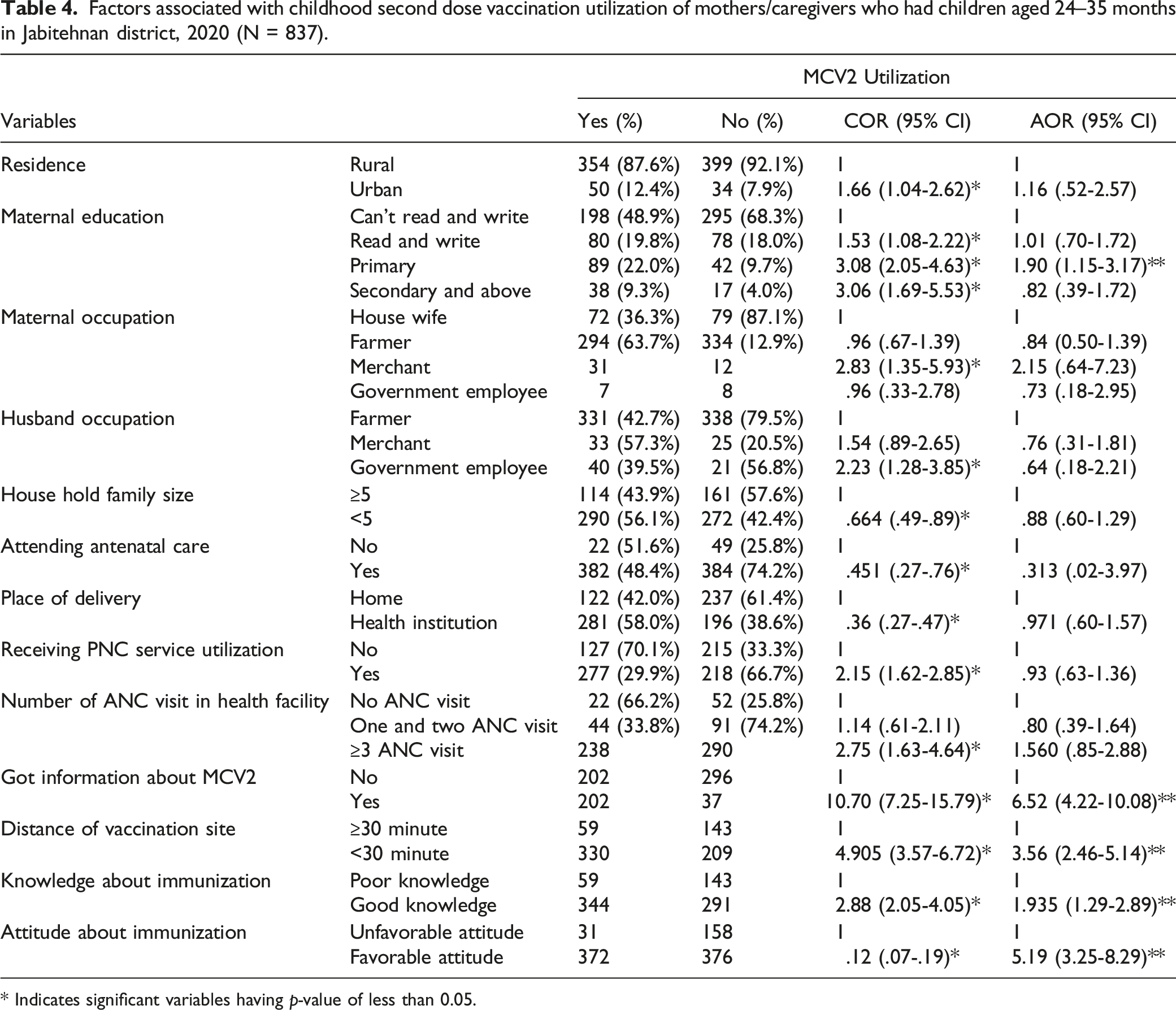
* Indicates significant variables having p-value of less than 0.05.
Discussion
For the measles to be eradicated, a high level of population immunity is necessary, and receiving the second dose of the vaccine was long seen as proof of immunity. It is important to provide everyone with 2 doses of the measles vaccine in order to effectively safeguard the population. This study was aimed to determine the second measles vaccination utilization and associated factors among children aged 24–35 months in Jabitehnan district.
The overall second dose measles vaccination utilization among children aged 24–35 months in this study was 48.1% (95% CI: 44.7, 51.6). This implies that the remaining 51.9% children were unvaccinated and might be susceptible to measles disease. The utilization of second dose measles vaccination was below the threshold for stopping the measles transmission, which is 95% 27 but higher than the Ethiopian mini demographic health survey finding of Amhara region (13%), and at Kakamega district in Kenya 17.9%. 21 This discrepancy might be due to time of the study; the MDHS was conducted at the beginning of launching of the second dose measles vaccine in Ethiopia, whereas the current study was conducted after 18 months of the program endorsement. A pool of children without immunity against measles infection is produced as a result of the low use of MCV2 and the constant coverage of MCV1. Major measles outbreaks occur as a result of this immunity gap. It was crucial to meet the national vaccination goal of 95% of children receiving MCV1 and MCV2 in order to achieve elimination of measles.
Similar finding was observed in Mtiwara, Tanzania 44.2% 28 . However, the finding observed in this study was lower than results in Zhejiang province in China 93.3%, 22 Tokyo in Japan 90.8%, 24 South Africa 83%, 28 Sudan 72%, 29 and in Eretria 96.7%. 30 This discrepancy might be due to difference in health service accessibility and socio-demographic characteristics. Another possible explanation for lower coverage of second dose measles vaccination in this study might be related with lack of awareness about second dose measles vaccination due to time of launching of the service and time of immunization. This study found that maternal education, getting information about MCV2, distance from vaccination sites, and knowledge and attitude about immunization were factors associated with measles second dose vaccination utilization.
Accordingly, children born from mothers having primary education were more likely to receive a second dose of vaccine than their counterparts. This finding was consistent with studies done in Zhejiang province east China 23 and in Brazil city. 31 In contrary, this finding was inconsistent with study done at Mtiwara district in Tanzania, 32 and at Aceh Jaya province in Indonesia. 33 The possible justification might be that educated mothers might have had better knowledge about vaccine preventable disease and recognized the importance of vaccine by bringing their child to the vaccination site.
Similarly, children whose mothers/caregivers got information about second dose measles vaccine were more likely to receive their vaccine. This finding was supported by the study done at Kakamega district in Kenya 21 and at Tokyo in Japan, 24 which enumerated that lack of information as the most important barrier for second dose measles vaccine. However, studies from Zhejiang province in China 23 and in Brazil city 31 did not show similar results as ours. The possible justification might be that mothers/caregivers who have better information about second dose measles vaccine may recognize the importance of the vaccination and bring their children to the vaccination site.
In addition, those children whose mothers/caregivers traveling to the nearest vaccination site were more likely to receive second dose measles vaccine compared to those who had to travel longer distances to get vaccination service. This was in line with the finding of the study done at Kakamega district in Kenya 21 and finding of the study in Shenzhen east China. 26 This was inconsistent with the finding of the study done in Aceh Jaya province in Indonesia. 33 The possible justification might be due to their given time commitment and workload from household duties; mothers or caregivers who traveled a great distance might choose not to bring their children to the vaccination site.
Children whose mothers/caregivers having good knowledge about immunization were more likely to receive second dose measles vaccination compared to that of children whose mothers/caregivers having poor knowledge about immunization. This was in line with a study done at Lawra district in Ghana. 26 This suggests that mothers/caregivers having a better understanding of childhood vaccination, and vaccine preventable diseases are more likely to bring their child to the vaccination site. Finally, children whose mothers/caregivers with favorable attitude towards childhood vaccination were more likely to be vaccinated the second dose measles vaccine compared with their counterparts. This could be suggested that mothers/caregivers who had unfavorable attitude about second dose measles vaccination might not bring their children to the vaccination site by their appointment. However, in this study, predictor variables of other studies such as residence, maternal occupation, husband occupation, family size, place of delivery, and ANC & PNC utilization were not associated. 34 This might be due to difference in socioeconomic, study design, and study period.
Strengths and Limitation of the Study
This study was the first which had been conducted in a community setup in our country, Ethiopia. Despite this, some of the children had no vaccination cards, and information about vaccination status had to be limited to the mother’s verbal responses which might be liable to recall bias.
Conclusions
Second dose measles vaccination utilization was low compared to the national immunization targets (95%). Maternal level of education, distance from vaccination site, information about MCV2, maternal knowledge about immunization, and maternal attitude towards immunization had statistical significant association with second dose measles vaccination utilization. Therefore, the regional health bureau with zonal department should enhance maternal education to advance their knowledge and to change their attitudes towards childhood immunization including second dose measles vaccination.
Footnotes
Acknowledgments
Authors would like to thank the Debre Markos University College of Health Sciences for providing this opportunity to conduct this research work. In addition, our gratitude goes to Jabitehnan health district office for their cooperative and providing necessary information. Also, we are grateful to acknowledge our study participants for providing the necessary information and the data collectors for collecting the data carefully.
Authors’ Contributions
Aynalem Demewoz done the conception, study design, execution, acquisition of data, drafting, revising or critically reviewing the article, Bekalu Endalew also done the conception, study design, execution, acquisition of data, drafting, revising or critically reviewing the article, Muluye Gebrie Mengie done the conception, study design, execution, acquisition of data, drafting, revising or critically reviewing the article, Moges Wubie (Assistance Professor), done the conception, study design, execution, acquisition of data, drafting, revising or critically reviewing the article and Dubie Jara made a significant contribution to the analysis and interpretation, gave final approval of the version to be published, Esmelealem Mihretu Kassegn also made a significant contribution to the analysis and interpretation, gave final approval of the version to be published and Abiot Aschale, made a significant contribution to the analysis and interpretation. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent
The ethics approval was obtained from the Debre Markos University Research and Ethical Review Committee, College of Medicine and Health Sciences (Ref.No/HSC/R/C/Ser/Co/72/11/13). In addition, letters of authorization gained from Jabitehnan district health office before contacting participants. The participants were then fully briefed about the study’s purpose and benefits and obtained written informed consent for both data collection and publication. Confidentiality was maintained through anonymity and privacy measures were taken to preserve the right of the participants throughout the research including with regard to publication. Finally, the selected participants were asked about their willingness to join the study. Any study participant willing to engage in the study and those who wanted to stop an interview at any time were allowed to do so. This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable for this study.
Availability of Data and Material
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.