
Abstract
Objective
This study aimed to assess the probability of reaching an adequate pharmacokinetic/pharmacodynamic (pK/pD) index for different cefepime dosages in frail patients with bacteremia treated in the emergency room.
Methods
Simulation study based on Gram-negative bacterial strains that cause bacteremia. The probability of reaching a time above the minimum inhibitory concentration (MIC) at 50% and 100% dosing intervals (fT > 50 and fT > 80% MIC) was assessed for two different renal clearance intervals.
Results
One hundred twenty nine strains were collected, the predominant species being Escherichia coli (n = 83 [64.3%]). In patients with a ClCr of 30 mL/min, an fT > 50% MIC was reached in more than 90% of the simulations. However, a dose of at least 1 g every 12 h must be administered to reach an fT > 80% MIC. In patients with a ClCr of 30–60 mL/min, the probability of reaching an fT > 50% MIC was higher than 90% with doses of 1 g every 8 h or more, but this value was not reached in > 90% simulations for any of the doses tested in this study.
Conclusions
Standard cefepime dosing can reach an adequate PK/PD index in frail patients. Nevertheless, a high dose or extended infusion is necessary to reach an fT > 80% MIC in patients with a ClCr > 60 mL/min.
Introduction
Infection in frail patients is among the major causes of emergency room visits worldwide and continues to be associated with high mortality rates of 15% to more than 50%. 1
Gram-negative bacteria, the main causative agents of sepsis in elderly patients, are predominant in urinary, abdominal, and respiratory infections.2-4 Cefepime is one empirical treatment of choice in patients with healthcare-associated infections, showing good activity against most strains of Enterobacteriaceae and Pseudomonas spp.5,6 Although cefepime is widely used, its dosing in frail patients remains uncertain, especially in critically ill patients. Several studies have shown that patients with sepsis could be underdosed at the commonly used cefepime doses, 7 postulating the need to surpass a minimum inhibitory concentration (MIC) > 50% of the dosage interval (T > MIC) to reach adequate drug activity toward improving the results with high doses.8-10 However, the use of high-dose cefepime has been associated with significant adverse effects such as neurotoxicity, especially in patients with reduced renal function.11,12 In turn, the increase in resistance observed in recent decades makes it necessary to reassess the doses used in this group of patients.
This study aimed to assess the probability of reaching an adequate pharmacokinetic/pharmacodynamic (pK/pD) index for different dosages of cefepime at different degrees of renal function based on isolates from blood cultures derived from frail patients treated in an emergency department (ED).
Material and Methods
A simulation study was performed based on data from patients with Gram-negative bacteremia treated in a frailty unit of an emergency department (ED) between July 2018 and December 2020. Bacteremia-causing strains that were intrinsically resistant to cefepime were excluded. The ED frailty area includes elderly patients with high complexity and need for care, identified using the “Clinical Frailty Scale.” 13
Pharmacokinetic Parameters Used in the Simulation Model.

Cl, clearance; ClCr, renal clearance; Vd, volume of distribution.
A total of 1000 Monte Carlo simulations were performed at different doses and renal function degrees using Excel®. Six different doses of cefepime (1 and 2 g every 8, 12, and 24 h) administered in 0.5-h infusions were evaluated, and the time above the MIC was calculated using the following formula
17

The t1 and t2 values were calculated using the following formulas

The percentage of patients assessed for each dosage regimen was calculated considering a value of fT > 50% MIC and fT > 80% MIC using the following formula
Results
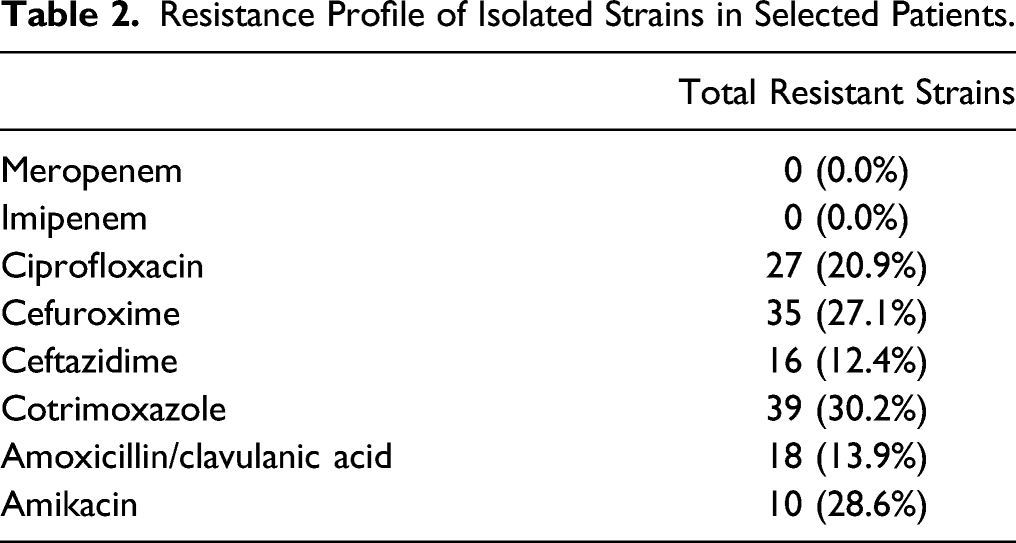
Resistance Profile of Isolated Strains in Selected Patients.
The probabilities of target attainment for cefepime administered at 1 g and 2 g every 8, 12, and 24 h for the simulation in the set of bacterial strains considered for the different degrees of renal function are shown in Figure 1. In patients with a ClCr of < 30 mL/min, for all doses from 2 g every 24 h, an fT > 50% MIC was reached in more than 90% of the simulations. Nevertheless, a dose of at least 1 g must be administered every 12 h to reach an fT > 80% MIC. In patients with a ClCr of 30–60 mL/min, the probability of attaining an fT > 50% MIC was higher than 90% at doses of 1 g every 8 h and higher, and this value was reached in > 90% of the simulations only at a dose of 2 g every 8 h. Figure 2 shows the relationship between MIC and fT > MIC for cefepime at the different doses and degrees of renal function tested in this study. Probability of target attainment of time > 50% (T > 50%) and > 80% (T > 80%) MIC for the strains included in this study. ClCr, renal clearance; MIC, minimum inhibitory concentration. Probability of target attainment (PTA) by MIC value for 50% and 80% of the dosing interval for different doses of cefepime in patients with different degrees of renal function. ClCr, renal clearance; PTA, probability of target attainment.

Discussion
Based on the results, intermittent infusion doses of cefepime were able to attain an fT > 50% MIC in our patients. However, the target of fT > 80% MIC requires the administration of a dose of 1–2 g every 8 h, especially in patients without severe renal function impairment.
In cases of severe infection, selecting an adequate dose of antibiotics is associated with improved clinical results. In turn, several studies have shown that insufficient doses are associated with the increased selection of resistant strains.17,18 For this reason, the pK/pD index has become a key parameter in selecting antimicrobial dosing with the highest probability of reaching the concentrations associated with an increased response to treatment. In addition to the intrinsic resistance of bacterial strains to antibiotics, variations in the Vd, Cl, or protein binding strongly affect the concentrations that they reach in the infectious focus and therefore, the probability of a treatment response. In our model, we included important variations in Vd and clearance to simulate the wide variability of situations that occur in frail patients, especially those with sepsis.
Cefepime, as with all other β-lactam drugs, shows time-dependent activity determined by the fT > MIC value. Despite its wide use, the pK/pD index shows some discrepancies with this antibiotic. In a study of patients with bacteremia and sepsis, an fT > 80% MIC with cefepime was associated with a lower risk of negative results related to bacterial eradication and clinical cure. 9 Another study of patients infected with P. aeruginosa showed that microbiological eradication was associated with attaining a target of fT > 60% MIC. 19 Finally, in patients with Gram-negative bacteremia, other authors demonstrated that survival was related to attaining a target fT > 68–74% MIC. 10 Septic patients with bacteremia require urgent bactericidal action. Under this premise, here we simulated the ability of cefepime to reach values of fT > 50% and >80% MIC.
In line with the above, according to our simulation model, doses of 2 g every 8 h or as an extended infusion are necessary in seriously ill patients with good renal function. Therefore, this group of patients must be identified to optimize their dosage. In this study, 10% of strains had intermediate sensitivity to cefepime, a higher percentage than that found in the simulation model. The increase in this strain type among patients treated in the emergency room makes it necessary to re-evaluate the drug dosage, especially in patients with serious infections. In fact, several authors have shown that increases in the bacterial MIC of cefepime are associated with worse clinical outcomes, most likely associated with inappropriate dosage. 20
Study limitations include the uncertainty of the Cl and Vd values used in the model given the lack of data on these parameters in frail patients treated in the emergency room. For this reason, data from young patients were used instead. In turn, we have not considered the ability of the predicted concentrations to access the infectious focus of the patient. The drug’s penetration into the lungs, abscesses, or other foci demonstrated a lower concentration than that in the bloodstream. Cefepime has shown adequate penetration into lung tissue, close to 100%. 21 However, critically ill patients with a high Vd or Cl could benefit from doses administered as extended infusions to ensure adequate exposure.
In summary, the standard doses of cefepime reach an adequate PK/PD value in frail patients with impaired renal function. However, doses of 2 g every 8 h or as extended infusions are necessary to reach an fT > 80% MIC in patients with adequate renal function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.