
Abstract
Our aim was to test the effects of Andullation therapy on pain threshold, pain perception, feeling of well-being, arterial pressure, and leg volume in healthy and unhealthy patients. We used a multidirectional vibration (frequency range: 5–40 Hz; peak-to-peak amplitude: 2–8 mm; acceleration: 0.4–2 m/s2) in an undulatory way through the surface of the body when the patient was in contact with a mattress (“andullation”). The vibes traveled from the heel to the head in a random fashion while the participants (N = 50) were lying on the mattress. We measured the pain threshold using an algometer; pain perception and well-being through a visual analog scale (VAS); arterial pressure with an electronic sphygmomanometer; and leg volume with Kuhnke’s technique. Measurements were made just before the first andullation session and after the fifth andullation session. Every participant received andullation sessions of 30 min a day for 5 consecutive days. The patients’ pain threshold significantly (P < .001) increased by 34.48% and 25.79% in the lumbar and trapezius zones, respectively, after 5 sessions of therapy. The subjective perception of pain decreased by 52.3% and the feeling of well-being increased by 45.1%. The systolic and diastolic pressures significantly (P < .001) decreased by 6.44 and 4.68 mm Hg on average, respectively. Leg volume significantly decreased (P < .01) by 64.39 mL after the fifth andullation session. Despite not including a control group in our study, the andullation intervention showed an improvement in pain, well-being, arterial pressure, and lower limb volume in the studied population.
Keywords
Introduction
The effects of vibration on the human body have been widely studied as both a source of injuries and as a way to treat different diseases. The potential risk of using vibration has been well established in the International Standards Organization (ISO, 5349-1) and in British Standard (BS6841). 1 –4 On the other hand, the use of vibrations to improve the effects of physical training and to ameliorate the clinical signs of different pathologies has been extensively reported. 5 –10 However, most interventions have used the whole-body vibration (WBV) technique in a passive mode as well as combined with exertion. 11 –18 Whole-body vibration is normally applied through a platform that vibrates at a fixed frequency and amplitude selected by the user. Normally, participants under experimentation stand up, lean, or sit on the vibrating platform for a short period of time (<5 min).
The acute effects of WBV on pain level, flexibility, and cardiovascular responses have been explored using vibration frequencies of 5–14 Hz and displacements of 2.5–7.5 mm. The results from these studies showed significant improvements in pain level, flexibility, gait speed, sit-to-stand test, and handgrip strength but have failed to show any change in blood pressure. 19,20
Whole-body vibration has been postulated as being able to improve the quality of life of patients with metabolic syndrome and severe chronic obstructive pulmonary disease, along with being able to improve blood flow in patients with type 2 diabetes and muscle flexibility and pain in fibromyalgia and neurological patients. 16,21 Bidonde et al. 21 extensively reviewed the effect of WBV training for fibromyalgia and found several outcomes in fibromyalgia patients (based on the findings of one study) that showed improvements of 39%, 46%, and 36% in pain intensity, fatigue, and stiffness, respectively, after WBV plus mixed exercise, what met the 15% threshold for clinical relevance but at a lower level of evidence.
Active or passive WBV combined with moist heat has been shown to elevate skin blood flow by 450% when using a vibration frequency of 50 Hz and a mechanical displacement of 5–6 mm during 10 bouts of 60 seconds. 16 However, the combination of WBV exercise (26 Hz, 4 mm amplitude) with blood restriction during 10 sets of 1 min on and 1 min off duty cycles produced an increase in electromyogram amplitude and elevation of the lactate and growth hormone responses. 18
Local vibration has also been applied to recovery from exercise. However, the results evidenced no benefit during the recovery, probably because of the weak mechanical action of the vibrations. 17
Currently, little literature exists on the application of andullation on human patients. Andullation is a multidirectional (3 axis oscillations) WBV technique that is delivered in a horizontal position using a massage mattress (see Methods section). It is possible that these kinds of vibrations when delivered in an undulatory mode along the body’s surface may stimulate mechanical receptors on the skin and in the subdermal tissue. However, currently, only 2 articles using andullation appear in databases such as PubMed, Scopus, or Medical Library (a few articles have been published in journals or local publications not included in the Journal Citation Report). One article focused on human patients undergoing in vitro fertilization. 22 The other article showed the effects of andullation on the blood circulation of laboratory animals. 23
In this article, we present for the first time data on the physiological effects of andullation applied to humans. The aim of our work is to ascertain the effects of andullation on objective and subjective pain indicators, on a patient’s sensation of well-being, on arterial pressure, and on lower limb volume.
Methods
Participants
Seventy human participants were recruited among the student and staff population of the Faculties of Medicine and the Physiotherapy (University of Seville). Twenty participants dropped out of the study because they did not fulfill the experimental conditions; specifically, 14 of 20 failed to attend one or more of the 5 sessions for the andullation intervention. The other 5 participants succumbed to several illnesses during the experimental period and rejected the intervention, and one participant declined to participate. Finally, 50 participants were selected for the andullation experiments. The participants were between 18 and 68 years old. The participants’ biometric characteristics are shown in Table 1. The following inclusion criteria were established for the current study: healthy participants and unhealthy participants (with mild chronic arthropathies and/or fibromyalgia but not to the point of curtailing their normal activities). The exclusion criteria were as follows: participants with severe cardiac disease, participants with surgical prosthesis who were less than 6 months away from implantation, participants with severe retinopathies, and participants with circulatory vertebra-basilar insufficiency.
Biometry of the Experimental Participants.
We used the checklist (version 1.0) of the TREND (transparent reporting of evaluations with nonrandomized designs) statement 24 to report the steps of the intervention applied in this study. A flow diagram of the intervention is shown in Figure 1. The dependent variables (pain threshold, pain perception, well-being perception, arterial pressure, and lower limb volume) were measured before and after the andullation sessions.

Flow diagram of the clinical intervention.
All participants (N = 50) were fully informed about the andullation device and the entire procedure. Finally, all of the participants voluntarily signed a written consent. The participants were also informed about their possibility to withdraw from the study at any time. The participants agreed to participate for 5 days for 1 h/day. The experiments were carried out at the same place (clinical room) and within the same environment (22ºC and 75% humidity). The experimental condition and the protocol used in this study were approved by the local ethics committee (Comité Ético de los Hospitales Universitarios Virgen del Rocío y Virgen Macarena de la Junta de Andalucía, code: 1740-N-17 Spain), following the 2003 Helsinki Declaration.
Procedure
Data on the effects of andullation therapy were collected from April to November of 2018. A medical anamnesis was completed for every subject before the andullation intervention. The anthropometric characteristics of the participants were measured by means of a stadiometer (50–260 cm, 1 mm accuracy; SECA 206, Spain) and a scale (0–250 kg, 50 g accuracy) (SECA, Spain). We used a visual analog scale (VAS) for pain and well-being perception, which was presented before and after the andullation therapy. The patient’s well-being perception included how he or she felt about his or her mental tension, moodiness, relaxing condition, and sleep quality. The scale for pain perception is a 100-mm line joining both the “maximal pain” end to the “no pain” end. Therefore, the participants marked their perceptions of pain over the scale without having to use numbers. After doing this, a researcher read the actual number on the numbered reverse of the scale. The scale for well-being perception was a 100-mm line limited by “no-well-being at all” and “full well-being,” and the scores were obtained similarly as for the pain perception scale.
We used an algometer (Dolorimeter, Rhabmedic, Spain; range from 0 to 10 kg/cm2; accuracy: 0.1 kg/cm2) to obtain an objective measurement of the pressure-induced pain on the skin surface over the trapezius muscle (3 cm cranial to the scapular spine and in the middle point between the posterior apophysis of C7 and the lateral limit of the acromion) and over the lumbar muscle (5 cm lateral to the posterior apophysis of L2). The algometer consists of a manometer connected to a metallic rod that ends in a 10-mm circle. Once the end of the rod was placed on the skin, the pressure was manually increased until the participants felt pain. The pressure pain threshold was defined as the minimal pressure (kg/cm2) that would produce pain. 25 –27
The andullation device (Home Health Product; medical device [andumedic] certificated as Class IIa by Health Spanish Authorities) consists of a mattress that includes 70 motors to produce vibrations of different amplitudes (ranging from 2 to 8 mm peak to peak), accelerations (0.4–2 m/s2), and frequencies (ranging from 5 to 40 Hz). We chose a frequency of 15 Hz, amplitude of 7 mm, and acceleration of 1 m/s2 as the parameters for the andullation intervention. The activation and amplitude of the vibrations were computer controlled and sequentially activated to produce a vibratory wave through the whole body of the subject, who stayed in a decubitus supine position on the mattress. The vibrations traveled from the heel to the head or vice versa. We also measured a portion of the volume (more than 70% of the whole volume) of the thigh and leg using Kuhnke’stechnique. 28 In short, we measured 5 circumferences separated by 4 cm along the thigh and another 5 circumferences along the leg. The volume of every 4-cm long cylinder was calculated and added to the results following Kuhnke’s corrections, as expressed in the following formula:

where V is the volume of the thigh of the leg,
The time course of the procedure was the following (Figure 2): (a) after medical anamnesis, an anthropometry was performed; (b) both subjective and objective evaluations of the participant’s pain threshold was carried out using the algometer and the VAS described above; (c) the participants were placed in decubitus supine position on the andullation device and did not move for the 15-min session; at the end of this period, the arterial pressure (Omron sphygmomanometer device with an arm cuff, Oregon Inc., USA) and thigh and leg volumes were measured. Every measurement was repeated twice for the same researcher, and the average value was incorporated into the database; (e) then, the participants received a 30-min andullation session a day for 5 days; (f) after the fifth andullation session, the participants stayed for a 15-min period on the mattress. During the last 5 min of this period, arterial pressure and thigh and leg volume were measured again. Finally, pain level and well-being perception were again evaluated.
Statistics
We used the standardized differences of the mean to predetermine an acceptable size of the sample. Using the NQuery software, version 7.0, we entered a mean difference equal to or higher than 25% (two-unit variability), a .05 of significance level (α), and a standard deviation (σ) of 4.232, resulting in a sample size equal to 49 paired for a 90% of statistical power. A normality test was conducted to the differences in the mean values of selected variables before and after the andullation therapy. When the data belonged to a normally distributed population, a Student t test for paired samples was used, and the significance was established as P < .05. These data derived from a non-normal distributed population were analyzed with the Wilcoxon test at significance of P < .05. In every case, a confidence interval of 95% was used. We also calculated Cohen’s d (mean difference/standard deviation) for the size of the effect produced by the andullation intervention. We estimated the size of the effect considering <0.2 as low, <0.5 as medium, and <0.8 as large. All the statistical calculations and data plots were carried out using a professional spreadsheet (OriginPro (2015), OriginLab corp. Northampton, MA, USA), NQuery, version 7.0 (StatSols, 2019), and SPSS (IBM SPSS Statistics for Windows, Version 25.0. IBM Corp., Armonk, NY, USA) software.
Results
We conducted a noninvasive intervention with a sample of 50 healthy and unhealthy participants using a waving vibes device (AndullationÒ). The participants were laid in a horizontal position during all the andullation sessions. We obtained significant differences in the mean values (N = 50) for pain threshold, pain perception, well-being perception, and lower limb volume before and after the intervention.

Measurements carried out before and after the andullation intervention.
Pain
The pain threshold for the trapezius zone increased by 25.79% after the andullation intervention. The pain threshold (N = 50) over the skin on the trapezius muscle before the first andullation session was 3.76 (1.79) kg/cm2 (mean [SD]) and 4.73 (2.14) kg/cm2 (P < .01) after the andullation on the fifth day; the confidence interval (CI) (95%) increased from 0.51665 to 1.38735. The pain threshold in the lumbar zone increased by 34.48% after the andullation intervention. The mean value (N = 50) of the pain threshold in the lumbar zone immediately before the first intervention with andullation was 4.152 (1.77) kg/cm2and went up to 5.584 (2.19) kg/cm2 (P < .001) after the last andullation session on the fifth day (Figure 3), with a CI (95%) going from 0.99888 to 1.86512. The largest pain threshold increase (1,432 kg/cm2) was measured in the lumbar zone between the preandullation session on the first day and the postandullation session on the fifth day. The effect size of the pain threshold for the lumbar and trapezius zones after the fifth andullation session was 0.807 (large) and 0.528 (medium), respectively. The full data are presented in Table 2.

Changes in the pain threshold induced by andullation. The columns represent the mean and standard deviation of the pain thresholds before the first andullation session (Day 1 PRE); Day 5 POST are the data measured after the last andullation session on the fifth day of therapy. n = number of subjects;
Pain Threshold (Pthres) Changes Before and After the Intervention with Andullation.a

Abbreviations: CI: confidence interval; LZ: lumbar zone; SD: standard deviation; SEM: standard error of the mean; TRP: trapezius zone.
aEffect size: as described in statistic. PRE and POST is related to before and after the andullation intervention.
The mean value of the pain perception significantly (P < .001) decreased by 52.3% from 2.92 (2.66) before the first andullation session to 1.09 (1.85) after the fifth andullation session, as shown in Figure 4.
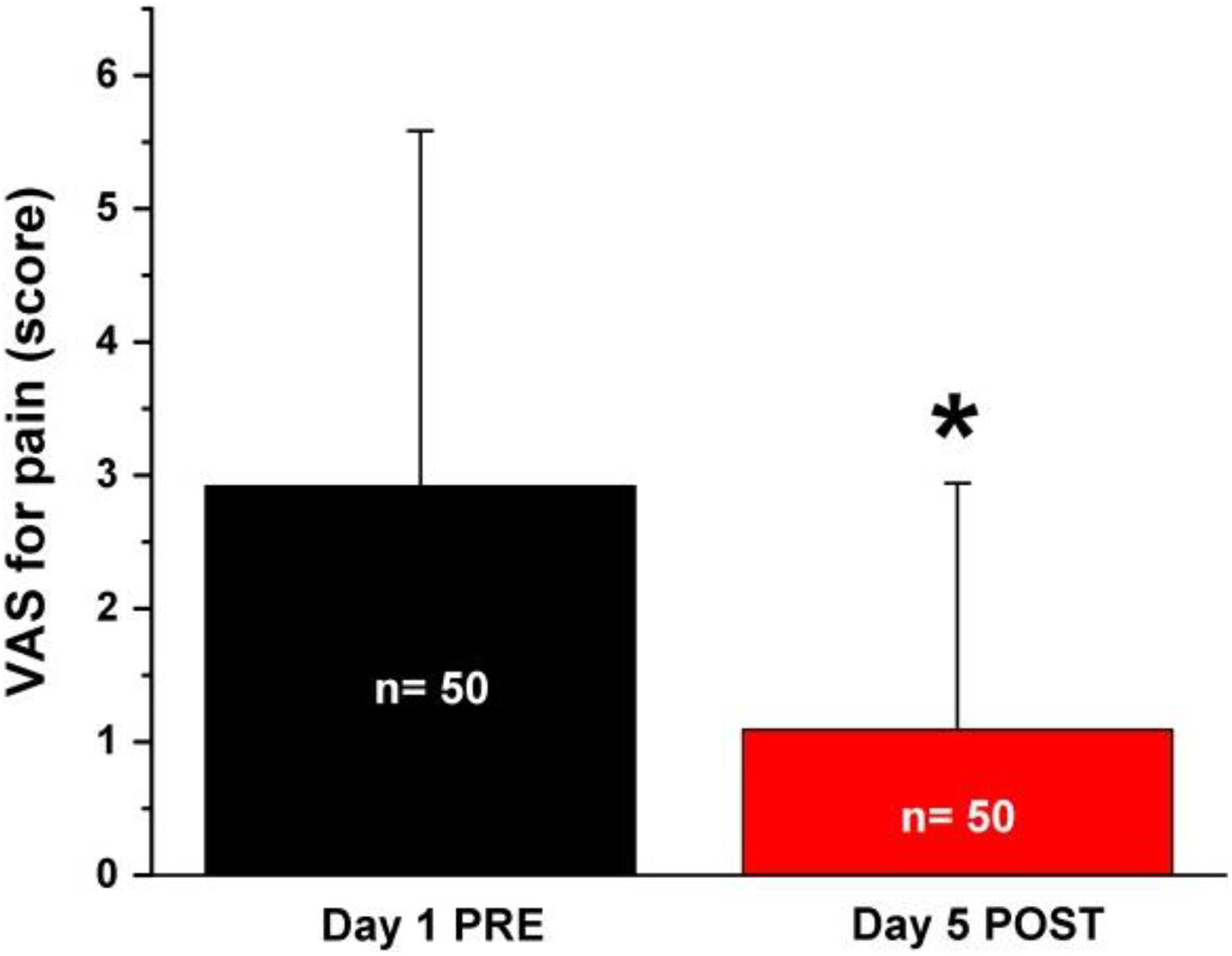
Changes in the mean values of the VAS score before the first intervention and after the fifth intervention with the andullation device. *Statistical significance (P < .01).
Using the same VAS as described in the Methods section, the well-being of the participants improved after the intervention. The well-being score changed significantly (P < .001) from 5.88 (2.24) to 8.46 (1.88), a 45.1% increase, as shown in Figure 5.

Changes in well-being of the participants (N = 50) in the study. *Statistical significance (P < .001).
Arterial Pressure
Both the systolic and diastolic pressures changed after 5 andullation sessions. The systolic pressure significantly (P < .001) varied by 5.21%, going from 123.6 (16.9) mm Hg at the first andullation session to 117.16 (15.1) mm Hg after the fifth session of andullation, with lower and upper CIs (95%) of 4.005 and 8.234 and 3.709 and 9.170, respectively (Figure 6).

Changes in the systolic and diastolic pressures before the first and after the fifth andullation session. The data plot is truncated for a better visualization of the change. Day 1 PRE: data obtained before the first intervention on the first day. Day 5 POST: data measured after the fifth andullation session. *P ≤ .001. N = 50.
Diastolic pressure also significantly (P < .001) decreased by 6.05% after the 5 andullation sessions. The diastolic pressure mean values before the andullation session were 77.34 (9.5) mm Hg and were 72.66 (8.4) mm Hg after the fifth andullation session. The lower and upper limits of the confidence intervals were 1.707 and 4.492 for the values on the first day before the andullation intervention and 3.042 and 6.31 after the last andullation session (Figure 6).
Lower Limb Volume
Leg volume significantly (P < .01) decreased on average by 64.39 mL (20.98) after the 5 andullation sessions (Figure 7). The confidence intervals were 11.35 (lower limits) and 74.37 (upper limits). However, the thigh mean volume was not significantly (P < .16) lower (134.65 mL) after the 5 andullation sessions. The thigh mean (SD) volume before andullation was 4191.85 (1376.36) and dropped to 4057.2 (1290.92) after the fifth day of the andullation therapy (Figure 7).
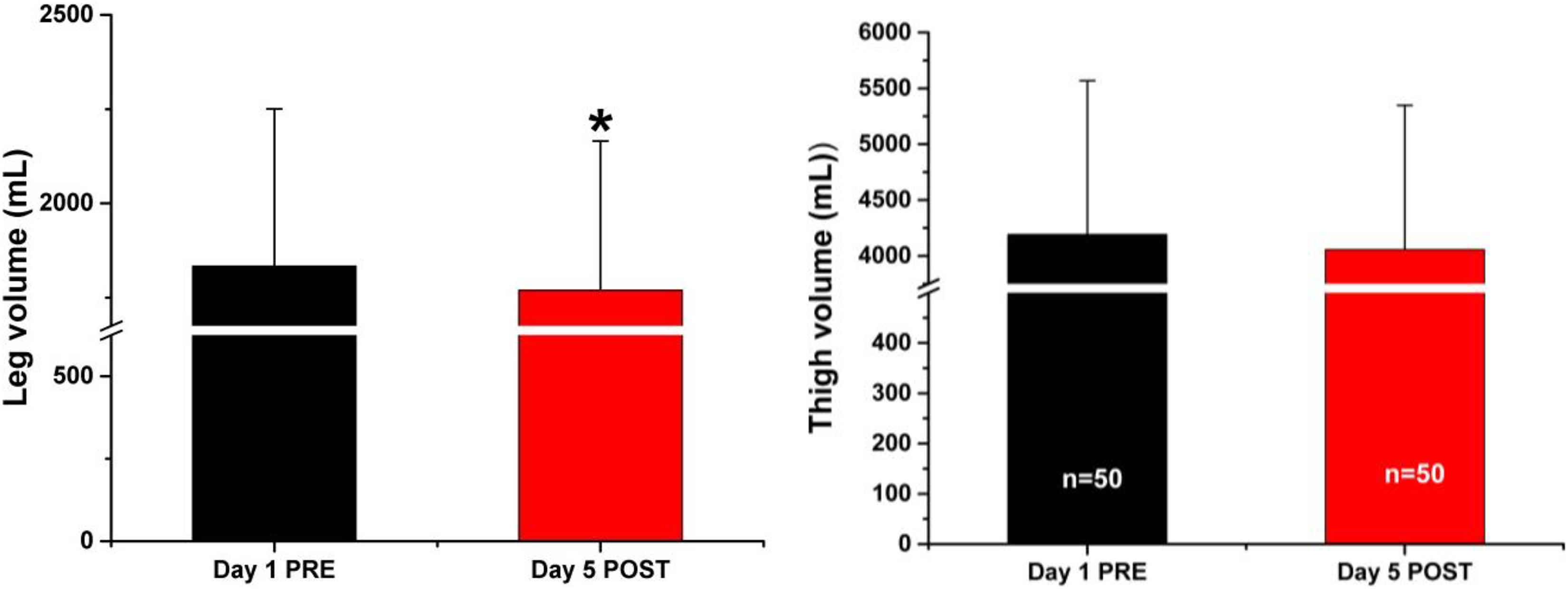
Changes in leg and thigh volume of participants (N = 50). Values are expressed as the mean and standard deviation. Day 1 PRE: measurements made before the andullation session. Day 5 POST: measurements made after the fifth session of andullation therapy. *Statistical significance for P < .05. (N = 50 for leg and thigh volumes).
Discussion
The main objective of this work is to clarify the possible effects of a novel vibratory therapy (Andullation) on pain, well-being, arterial pressure, and lower limb volume in healthy and unhealthy patients. For this first approach, we did not recruit a control group to avoid possible ethical conflicts with unhealthy participants not receiving the treatment, hence implying a limit to the generalization of the possible results. On the other hand, the design of the study as a pairwise analysis allowed us to compare paired samples before and after the intervention.
Pain Threshold
We chose 2 different body areas covering the trapezius and lumbar muscles to test the pain threshold of the participants. We chose the area over the trapezius muscle, because it is one of the most sensitive to psychological and physiological stress. 29,30 On the other hand, the lumbar zone is probably the most commonly tested area in painful pathologies of the lower back. 29,31 –33 We measured the pain threshold using an algometer device, because it is the most frequently used device by clinical therapists when compared with controlled heating source devices.
It has been shown that vibrations are related to a decrease in pain sensitiveness. 31 The mechanical characteristics of the andullation device allowed the stimulation of the skin and the muscular and subcutaneous tissues with a new pattern of vibes. According to the gate control theory, the stronger the activation of mechanical peripheral receptors are, the weaker the nociceptive signal entering the brain will be. 34,35 This effect might be accounted for by decreasing the magnitude of the nociceptive input to the projection neurons in the dorsal root of spinal cord, which could underlies the increase in the pain threshold observed in our study. Another possible effect could be that vibratory stimulation enables the facilitation of the synapses of the peripheral receptor fibers because of the inhibitory interneurons in the dorsal root of the spinal cord, but this remains to be clarified. On the other hand, the magnitude of the change in the pain threshold seems to be large because the andullation intervention was only applied for 30 min a day for 5 days. The possible effects of longer andullation sessions on pain threshold are out of the scope of the current study. Using shorter interventions, Sá-Caputo et al. 20 found a significant (P=.031) reduction in the pain level of a group of 29 patients with metabolic syndrome after they had been submitted to 3 bouts (1 min each) of WBV exercise. Our results also showed a significant reduction in the pain level after the intervention when using a visual analog pain scale. Unlike Sá-Caputo et al., we measured the pain level in a more objective way using an algometer and obtained a significant increase in the pain threshold levels of the patients.
Similarly, when using a vertical vibrational platform, Alev et al. reported a reduction in VAS for pain although they did not discuss any mechanism by which the vibration can reduce pain or improve the body’s tonic reflexes. The amplitude of the vibration and the frequency are the key points in this procedure, because they determine the load imposed by the vibration in the neuromuscular system during training. 36 However, WBV differs remarkably from an andullation device. Whole-body vibration uses the same vibratory characteristics to the part of the body on the platform, whereas andullation uses a wave of multidirectional vibrations over the whole surface of the patient who is reposed on the mattress.
The use of vertical WBV together with exercise for the treatment of sports injuries 37 –39 can produce positive results for the pain VAS. Evidence for WBV is not clear when it comes to reducing pain in patients with diseases such as fibromyalgia. 11,21 Moretti et al. 21,40 concluded that it was not possible to evaluate the magnitude of the effect of WBV treatment and stated that the results are based on evidence of very low quality and were inconclusive regarding pain. There is no evidence to demonstrate the use of WBV therapy throughout the body for the treatment of women with fibromyalgia, because there are no clinically relevant effects in reducing pain, controlling fatigue, and improving quality of life. 21,40 Collado-Mateo et al. 41 compiled 8 articles on WBV, of which only in one of them was pain specifically assessed and showed an improvement compared with the control group. However, no objective measurement of pain level was used in these studies, whereas in our study, the pain, which was produced by pressure applied over 2 body areas, was quantified by an algometer. Furthermore, we obtained an effect size of 0.8 (considered large) for the changes produced by andullation therapy on the pain threshold in the lumbar zone.
The well-being scores of most of the participants in our study improved after the andullation therapy. Because the experimenter did not intervene in the decision of the participants and because the participants were not informed of any expectancy of the treatment, the changes in the score values came from the internal feelings of the participants.
Arterial Pressure
The systolic and diastolic arterial pressure dropped by 6.44 mm Hg and 4.68 mm Hg, respectively, on average. These changes could be attributed to the change in body position from standing up to lying on the mattress. Nevertheless, to allow for cardiovascular adaptation, we waited for 15 min after the change in body position to measure arterial pressure before the first andullation session. Arterial pressure was measured again after the fifth intervention. Therefore, we ensured that changes in arterial pressure were closely related to the vibration therapy. On the other hand, the magnitude of the changes was small, as expected when taking into account the daily 30-min period of the vibratory stimulation; even so, these changes were statistically significant. Other authors have reported changes in arterial pressure using vibratory devices (WBV) associated with exertion, which is known to affect arterial pressure. 7,42,43 However, Sá-Caputo et al. 19,20 did not find any change in the arterial pressure of participants with metabolic syndrome after 3 bouts of 1 min WBV stimulation. Possibly, the physiological characteristics of the selected patients with metabolic syndrome, the small surface (only feet on the vibratory platform) receiving the vibration, and the short time (1 min ×3) of the vibration stimulation influenced those results.
In our study, the participants did not perform any exercise when on the mattress. The arterial pressure of the participants was measured using a conventional electronic sphygmomanometer. Nevertheless, to reduce the variability in the final reported values of this device, we repeat twice the measurement of the arterial pressure and the mean of these 2 values used for comparison. The electronic blood pressure measurer also avoided a subjective appraisal of the Korokov’s sounds that an experimenter can hear in mechanical sphygmomanometers.
The changes in lower extremity volume could be ascribed to the lying position. Nevertheless, we waited for 15 min, keeping the patient in the same position as in the andullation session before measuring the leg volume, so fluid drainage from the leg was possibly stabilized before the andullation session. The fact that the change in thigh volume after the andullation sessions was not significant (P < .16) might be explained by the large volume of this area, which would require a larger difference of volume or a larger population for a small increment of volume to become significant. The small change in thigh volume might also be because of drainage from the leg to the thigh.
Although other techniques, such as disc model or water displacement volumetry for limb volume determination are available, 44 Kuhnke’s technique is simple, precise, and easily adaptable to the different shapes of legs.
Conclusions
Our results showed a significant augmentation of the pain threshold and well-being after 5 andullation sessions of 30 min each in healthy and unhealthy participants. The values of pain perception, arterial pressure, and lower limb volume decreased significantly after the andullation sessions. These results indicate that an andullation device may be a nonrisky instrument that can be applied as a therapy for pain relief and valuable for lessening arterial pressure and lower limb volume.
Limitations of the Study and Clinical Applications
Because we included healthy and unhealthy participants with a wide range of ages in our study, we cannot specify the effects of andullation therapy on one specific group regarding either age or mild diseases within the whole range (18–68 years old). Therefore, the possibility exists that the effects were larger for unhealthy participants than for healthy one. This remains to be clarified.
Because we did not use a control group for different reasons, we cannot extrapolate our results to the general population. Nevertheless, andullation therapy has shown to be beneficial for most of the participants in our study, suggesting that it can be a helpful tool for clinical applications to improve the quality of life of patients.
Footnotes
Acknowledgments
The authors are thankful to Dr Angel Vilches for statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fundación para la Investigación de la Universidad de Sevilla (FIUS) and, partially, by Home Health Products (HHP), Spain.