
Abstract
This study aimed to compare the effect of high-intensity interval training (HIIT) with additional whole-body vibration (WBV) on body composition and lipid profile in obese/overweight adults on a hypocaloric diet. Forty adults were randomly assigned to (a) HIIT and vibration and hypocaloric diet (HIITWBV, n = 13), (b) HIIT and diet (HIIT, n = 14), and (c) diet only (control [CON], n = 13). High-intensity interval training WBV participants trained 3 times per week for 8 weeks (6 sets × 1 minute of HIIT, cycling at 90% heart rate peak followed by 1 minute of interset vibration, at a frequency of 18 Hz increasing until 25 Hz with a peak-to-peak displacement of 4 mm. Training volume increased 1 set every 2 weeks until 10 sets). The HIIT group performed HIIT training followed by 2 minutes of passive recovery, while the CON continued with their daily activities combined with calorie restriction. Body composition (body fat and fat-free mass) and biochemical indices (glucose, total cholesterol, high-density lipoprotein cholesterol, and triglycerides) were determined. Following 8 weeks, body fat was significantly reduced by 7.5% and both triglycerides and total cholesterol decreased in the HIITWBV group only (−16.5% and −11.7% respectively). This study suggests that HIIT in combination with WBV and a hypocaloric diet can improve overall lipid profile in overweight/obese individuals.
Introduction
It is now well accepted that the prevalence of obesity has reached epidemic proportions and that obesity is associated with an increased risk of comorbidities such as type 2 diabetes, stroke, or hypertension. 1 Dietary modifications and exercise training are fundamental in the prevention and treatment of overweight and obesity, and as such, there is evidence that regular exercise improves blood glucose control in addition to lowering triglycerides, cholesterol, and total body fat. 2
In general, the exercise training programs designed to reduce body mass primarily focus on moderate-intensity continuous exercise; however, such programs have led to modest or even conflicting outcomes with regard to fat loss and glucose and lipid metabolism. 3 Therefore, new strategies designed to lower body mass and comorbidities are urgently required. 4 It is well founded that most obese individuals have sedentary habits and a compromised exercise tolerance, which may prevent them from taking part in regular exercise training. 5 Moreover, lack of time is often cited as a barrier to regular exercise participation in this population group, 6 and in this context, exercise programs that require less time and have the ability to reduce the subjective effort of exercise are highly desirable.
High-intensity interval training (HIIT) is an exercise training modality that alternates between brief repeated bouts of intense exercise and periods of active or passive recovery and has been demonstrated to improve several clinically relevant outcomes. 7 While continuous aerobic exercise of vigorous intensity (≥70% of maximal heart rate [HRmax]) seems to have a greater effect on adiposity than low-intensity continuous aerobic exercise (<60% HRmax) or strength training, 8 the consequence of intense aerobic exercise per se on body composition in obesity is still unclear. 9 High-intensity interval training has been shown to significantly reduce abdominal fat and blood pressure and improve glucose regulation 10 and lipid profiles, 11 and even more so than a group receiving dietary and psychological advice in combination with moderate continuous aerobic exercise. 10 Furthermore, high-intensity aerobic exercise can lead to reductions in both subcutaneous and visceral fat of middle-aged obese women in comparison to low-intensity exercise training. 12 Contrasting with these modalities of continuous aerobic exercise, the effectiveness of HIIT has been documented in populations with metabolic disorders such as obesity (as reviewed by Gibala et al 13 ), and few studies have investigated its effect on body composition or lipid profile. 14
While intense aerobic exercise (both continuous or with intervals) seems to be effective, a combination of strength and aerobic exercise is recommended to improve body composition in obese middle-aged women. 9 One of the time-efficient modalities that can be combined with HIIT is the use of vibration, which alone or in combination with other exercise strategies can decrease fat mass and increase muscle mass. 5 However, Nam et al 15 recently highlighted that the effect of whole-body vibration (WBV) on body composition is not consistent in the scientific literature. Some researchers found a significant decrease in percentage body fat following an 8-month WBV training period. 16 Milanese et al 5 also found a significant decrease in total body fat without changes in body weight after 8 weeks of vibration training, whereas others after 6 to 12 weeks of WBV training in overweight/obese postmenopausal women showed no changes in this outcome. 17,18
The mechanisms underlying the possible improvements in body composition with WBV training have been highlighted in recent reviews. 19,20 While in animal models Reijne et al 21 concluded that WBV training was able to increase blood glucose turnover rates and stimulated hepatic glycogen utilization, stimulating a lipolytic effect, 22 the changes are depending on numerous factors (ie, age). In humans, the potential mechanisms of improved body composition using WBV exercise are increased metabolic demand and energy expenditure that may be associated with the inhibition of adipogenesis and increase in muscle mass (see Cristi-Montero et al 20 for revision). Decrements in plasma glucose associated with muscle contraction 23 or increments in vasodilation and peripheral blood flow, 24 which in turn are closely linked with fatty acid metabolism, 25 have also been suggested.
In overweight and obese individuals, WBV training accelerates the reduction in visceral fat mass during an energy-restricted diet, 26 and more recently, Bellia et al 4 has documented an improvement in body composition, insulin resistance, and glucose regulation after an 8-week WBV intervention. In the same line, Nam et al 15 suggested that vibration exercise was as effective as aerobic exercise in reducing fat mass when combined with dietary intervention; however to our knowledge, no previous studies have assessed both interventions combined on body composition. Based on the aforementioned findings, it is possible that HIIT, which has a positive effect on adiposity, 8 may be used in combination with WBV as this modality is also associated with a change in fat mass in addition to improvements in blood flow. 24 Thus, it can be hypothesized that the combination of HIIT and WBV added to a hypocaloric diet may have the potential to improve body composition in an overweight and obese sedentary population. Therefore, the aim of the current study was to compare the effect of HIIT with additional vibration recovery on body composition and health-related parameters in obese/overweight adults who were placed on a hypocaloric diet.
Material and Methods
Participants
Forty (n = 40) overweight/obese (age: 35 [7] years, body mass: 87.9 [17.9] kg, height: 166 [10] cm, body mass index [BMI]: 27.0-42.1 kg/m2) participants took part in this study (Figure 1). Participants were recruited from the general population through a variety of sources: mass mailings, community events, advertisements, and word of mouth. All participants gave their written informed consent after receiving detailed study information. The inclusion criteria were as follows: males and females older than 18 years of age, with a BMI greater than or equal to 25 kg/m2, and not involved in any physical training for at least 1 year. Exclusion criteria included a history or evidence of advanced cardiovascular complications (including systolic blood pressure >160 mm Hg and diastolic blood pressure >100 mm Hg) or renal or hepatic diseases. Participants with type 1 or 2 diabetes or those on medication known to affect type 2 diabetes and cardiovascular risk factors (lipid lowering, antihypertensive, hypoglycemic, hormone replacement therapy, or insulin) were also excluded. The study conformed to the Declaration of Helsinki and the International Committee of Medical Journal Editors (ICMJE) recommendations for the protection of research participants and ethical approved was granted by a local institutional research ethics committee.

Flowchart of the study.
Study Design
Randomization was performed centrally in a 1:1:1 ratio with the use of a computer-generated random sequence. Participants were stratified by gender by an independent researcher not involved in eligibility, outcome assessment, or intervention. Participants were randomly assigned to: (a) HIIT group with WBV (HIITWBV, n = 13), (b) HIIT (HIIT, n = 14), and (c) control group (CON, n = 13) for 8 weeks. The participants in all groups received a hypocaloric diet with a negative balance of ≈2000 kJ/d compared to their estimated daily energy expenditure (energy expenditure was estimated from calculations of basal metabolic rate incorporating age and body mass). We chose to treat all groups with the same hypocaloric diet as this standardized approach served to eliminate any potential variation that may be attributed to intersubject dietary intake. All participants were requested not to change their lifestyle behaviors such as daily activity, exercise, and sleep pattern throughout the trial.
Exercise Testing
Following a 5-minute warm-up at 50 W, participants performed an incremental test on a cycle ergometer (Kettler Axiom P2, GmbH & Co KG, Ense-Parsit, Germany). Resistance was increased by 1 W every 2 seconds until volitional exhaustion or at the point at which pedal cadence fell below 50 rpm. Maximal effort was determined when 2 or more of the following criteria were met: (1) unable to continue pedaling, (2) ±10 beats/minute from age-predicted HRmax, and (3) rating of perceived exertion (RPE) >8 (using a 0-10 scale). During the test, peak power output and HRpeak were recorded. Heart rate peak obtained during the maximal graded test was used to set the intensity for HIIT training.
Eight-Week Training
During the training intervention, HIITWBV participants trained on a cycle ergometer (Kettler Axiom P2) 3 times per week for 8 weeks (with at least 1 rest day between sessions) and performed 6 sets × 1 minute of HIIT at 90% HRpeak followed by 6 × 1 minute of interset vibration at a frequency of 18 Hz and a peak-to-peak displacement of 4 mm (acceleration 2.6 g). The extra 1 minute of recovery compared to the HIIT-alone group was needed for preparation on the platform. Training volume increased 1 set every 2 weeks until 10 sets at week 8 and vibration was increased similar to HIIT bouts until 25 Hz (4 mm). Participants adopted an isometric squat position (approximately 100° knee flexion) lightly holding the handrails of a side-alternating WBV platform (Physio Wave 700; Globus, Trevisio, Italy). Participants were asked to wear the same sports footwear during all exercise and vibration sessions. The total interset rest time was 2 minutes. The HIIT-only group performed HIIT training followed by 2 minutes of passive recovery (participants rested or pedaled slowly at a resistance lower than 50 W), while the control group continued their daily activities in line with the same nutritional guidelines provided to the other participants. All training sessions ended with a 5-minute load-less cooldown period. Heart rate and RPE (using a 0-10 scale) were recorded at the end of each interval. Since all individuals were overweight or obese, a calorie-restricted diet (≈2000 kJ less than their daily energy expenditure for each person) was provided for all participants. The energy intake for each individual was approximately 50% to 55% carbohydrate, 30% lipids, and 15% protein. Standard food frequency questionnaires were administered to compare relative information on adherence to the dietary regimen.
Clinical Measures
At baseline and following 8 weeks of exercise training, all participants had blood pressure, body mass, height, and waist circumference measured. Blood pressure was monitored in a quiet room after resting for 10 minutes using Omron electronic blood pressure equipment (Omron BF-306; Omron Healthcare Europe BV, Hoofddorp, the Netherlands). Body mass was measured to the nearest 0.01 kg using electronic scales and height to the nearest 0.01 m using a portable stadiometer (Seca 217 Mobile Stadiometer; Seca, Hamburg, Germany). Body mass index was calculated as body mass divided by height squared (kg/m2). Waist circumference was measured between the lower rib and the iliac crest and hip circumference at the widest point around the greater trochanter. The body composition of each participant was analyzed using the body impedance analysis using Bodystat 1500 (Bodystat Ltd, Douglas, Isle of Man, United Kingdom), which is a 4-terminal single-frequency (500 µA at 50 kHz) analyzer. Resistance and reactance were measured between the right wrist and the right ankle, and total body fat, fat-free mass, and percentages were estimated from the manufacturers’ equations. Participants were asked to fast within 4 hours of the test, not to exercise within 12 hours, and to avoid alcohol or any other known diuretic. The device was tested for validity and reliability with results showing good to excellent fat and fat-free mass test–retest reliability. 27
Biochemical Analysis
Blood samples were collected between 08:00 and 09:00 hours from an antecubital forearm vein in the fasted state before and following 8 weeks of exercise training. Blood was collected in a vacutainer tube containing EDTA and immediately placed on ice. Plasma was subsequently separated by centrifugation (3000g, 10 minutes, 4°C). Total cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, and plasma glucose were determined using the Reflotron system (Boehringer-Mannheim, Mannheim, West Germany) with commercial kits. Low-density lipoprotein (LDL) was determined indirectly by using Friedewald formula: LDL = Total cholesterol (TC) − HDL + (triglyceride [TG]/5).
Statistical Analyses
Participant number was estimated as follows: based on an alpha risk of 5% with 80% ± 20% power and an expected dropout rate of ≈10%, we estimated that 13 to 15 participants per group is sufficient to detect a change from relative baseline of ≈2% using percentage body fat as the primary outcome. Changes in all other variables were considered as secondary outcomes.
The data are presented as mean (standard deviation). All measurements were normally distributed as determined by the Kolmogorov-Smirnov test. Analysis of variance (ANOVA) for repeated measures was used to determine a significant time × group interaction effect and thus differences between groups (HIITWBV vs HIIT group vs control group) and changes over time (before vs after the training intervention). Student t test for paired samples was used to locate the difference within groups, while a 1-way ANOVA was used to determine between-group changes. Effect sizes were calculated using Cohen d to quantify the magnitude of the difference between pre- and posttest. Values of Cohen d of 0.20 to 0.49 were considered small, values of 0.50 and 0.79 considered moderate, and values ≥0.80 considered large. 28 Statistical significance was set at P < .05. Analysis was performed using SPSS version 17.0 (SPSS Inc, Chicago, Illinois).
Results
The main characteristics of the participants at baseline are described in Table 1. There were no significant differences at baseline between groups for any variable (P > .05).
Participants Characteristics.a

Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; HIIT, high-intensity interval training; SBP, systolic blood pressure; SD, standard deviation; WBV, whole-body vibration; WHR, waist to hip ratio.
a Values are mean (SD).
On average, participants allocated to HIITWBV and the HIIT-only groups attended 23.2 (1.0) and 23.4 (0.8) out of 24 training sessions, respectively. Therefore, 100% of participants attended more than 80% of the exercise sessions. No harmful effects of the 8-week exercise intervention were noted in the HIITWBV and the HIIT-only groups. The effect of exercise training on body composition and lipid profile is presented in Table 2. Following 8 weeks of exercise training, percentage body fat was reduced in the HIITWBV group only (P < .05). However, body mass did not change across the training phase, in any group (P > .05).
Effects of the Exercise Training on Body Composition, Glucose, and Lipid Profile.
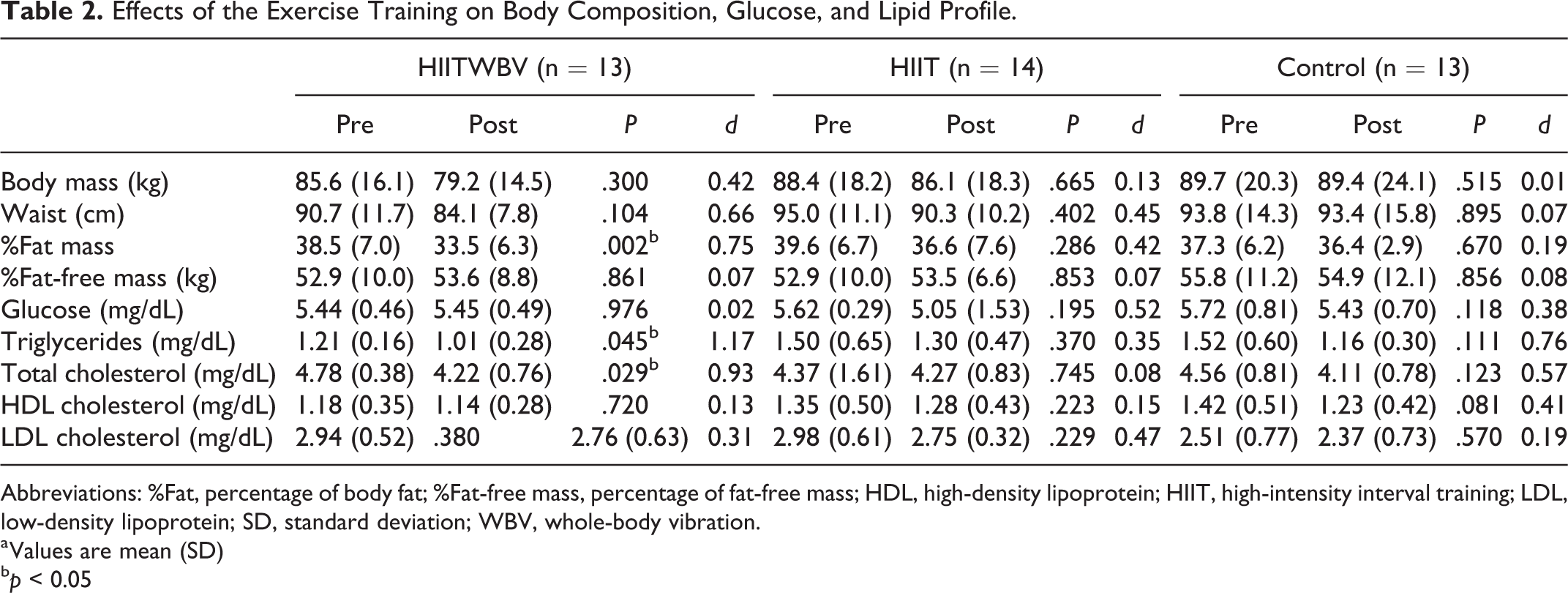
Abbreviations: %Fat, percentage of body fat; %Fat-free mass, percentage of fat-free mass; HDL, high-density lipoprotein; HIIT, high-intensity interval training; LDL, low-density lipoprotein; SD, standard deviation; WBV, whole-body vibration.
a Values are mean (SD)
b p < 0.05
Both triglycerides and total cholesterol decreased in the HIITWBV group (P < .05); however, no change in blood glucose concentration was observed for any group. There were no changes observed in blood metabolites for either the HIIT or control group following exercise training (P > .05).
Discussion
The aim of the current study was to compare the effect of HIIT combined with additional vibration on body composition and lipid profile in obese/overweight adults who were administered a hypocaloric diet. This study demonstrates that vibration added to HIIT and a hypocaloric diet in overweight/obese individuals can improve fat mass, blood triglycerides, and cholesterol concentration compared to HIIT and diet or to diet alone and that these beneficial effects can be detected within 8 weeks of exercise training.
To the best of our knowledge, this is the first study combining HIIT with vibration in obesity management. From our data, it would seem that WBV enhances the positive effects of HIIT and diet on body composition. Even though no significant differences in waist circumference or fat-free mass were detected between groups, percentage fat mass significantly decreased in the HIITWBV group and in the HIIT from relative baseline values, although the latter was not significant. Studies examining the short-term effects of HIIT on body composition in obese individuals are scarce 10 ; however, our data agree with that of a previous study in obese patients using HIIT. 29 Using WBV alone or added to endurance training can also lead to a decrease in percentage fat mass in obese middle-age females, 30 and the improvements obtained in percentage fat mass are greater to the ones reported adding WBV to a hypocaloric diet. 26 Indeed fat mass reduction is also greater following 8 to 12 weeks of WBV training in women 5 using synchronous vibration or in type 2 diabetic patients using dynamic exercise with WBV on a side-alternating platform. 24
The improvements in percentage fat mass were accompanied by a decrease of more than 7% in waist circumference (an important indicator of visceral adipose tissue [VAT]) in the HIITWBV group only. Our results (a decrease close to 5 cm) are in agreement with previous studies using the metabolic syndrome as the primary pathology, 10,31 and the change observed may be considered clinically significant in this population. 32 It has previously been shown that vigorous-intensity exercise significantly reduces VAT compared to moderate-intensity exercise 8,12 and that vibration can decrease VAT more than aerobic exercise plus diet or diet alone. 26 The combination of diet plus WBV also results in positive (nonsignificant) changes in VAT when compared to other intervention groups including a diet-only group or a program consisting of aerobic interval training only. 26 Vissers et al 8 suggests that there may be an exercise intensity threshold that controls VAT reduction, and it may possibly be due to the proportion of carbohydrate and fat being oxidized by muscle. 33 Furthermore, it has been postulated that HIIT results in greater lipolysis, and this may contribute toward the facilitation of a greater postexercise energy expenditure and fat oxidation. 34 This hypothesis may be a possible reason as to why vibration may cause a significant reduction in waist circumference. 35
Interventions combining WBV and aerobic exercise 36 with adjuvant dietary changes are more effective for weight management than an exercise or a diet-only intervention. The current study was therefore designed to assess the effects of HIIT plus WBV and diet, and our results regarding body mass (−6.4 kg or −7.5%; −2.3 kg or −2.6% in HIITWBV and HIIT, respectively) and waist circumference are consistent with those generally reported in HIIT studies using obese participants. Despite these improvements, no changes in fat-free mass were observed for any group. Heydari et al 37 and Gillen et al 14 found small increments in fat-free mass following 6 and 12 weeks of HIIT in young overweight men and women, respectively. However, von Stengel et al 38 report no additive effect over exercise training with regard to lean body mass when vibration is added. When static and dynamic exercises were performed on a vibration platform over a 24-week program, a modest but significant (+ 2.2%) increase in fat-free mass was found. 39 We also noticed that mean fat-free mass following the 8 weeks of training was not dissimilar between intervention groups; despite this, in overweight obese individuals, we observed an increase in fat-free mass (3.3%, P = .861) in the HIITWBV and (2.3%, P = .853) HIIT group. One potential explanation for the lack of a selective difference between groups/factors could be due to the consequence of limited statistical power. Any future study using the same methodological design would need more than double the existing participant number. Although these discrepancies can also be explained by differences in the exercise type (static vs dynamic exercises on the platform), Cochrane 36 reports that WBV alone does not have the capacity to increase energy expenditure for weight reduction, and may be due to the protocol used (frequency or duration). Therefore, longer and more intense protocols are warranted in future studies.
Another interesting finding in the current study was that the addition of HIITWBV significantly improved blood triglycerides and total cholesterol. This is particularly important as it is well established that obesity is associated with a decrement in the ability of skeletal muscle to oxidize lipid 40 and this type of combined intervention may contribute toward decreasing the susceptibility of impaired glucose tolerance or type 2 diabetes. No study to date has reported that HIIT improves total cholesterol or triglyceride concentration, and only one HIIT-based study has observed a positive change in blood lipids. 41 As HIITWBV improved these parameters within the current study, it may be considered that vibration can have an additional effect. While the role of vibration in lipids remains unclear, significant increments in plasma epinephrine and norepinephrine have been reported after vibration 42 together with changes in blood flow. 24 In support, previous work from our laboratory has shown that a 12-week WBV program including dynamic platform exercise can significantly increase leg blood flow velocity in type 2 diabetes and these changes were associated with changes in percentage body fat. 24 It is therefore feasible to postulate that the changes observed in percentage fat body and/or lipids as a function of HIITWBV may be due to an increase in blood flow brought about by the vibration per se rather than HIIT exercise only. However, this notion is speculative and further work is required to substantiate this claim.
There are several limitations to this study that need to be considered. Firstly, despite the prospective calculation of power, the number of experimental participants was low and that may have contributed to the lack of overall change observed in body composition and lipid profile. In order to overcome this aforementioned limitation, there is a need for future studies to use a larger sample size than that incorporated in the present study, and our retrospective calculation of power confirms this. Secondly, all experimental participants were placed on a hypocaloric diet while required to perform exercise, and as such, the effect of diet alone may have masked the potential effects of HIIT or WBV per se. Thirdly, the training period was relatively short (8 weeks), and this may have hindered specific biochemical improvements (in glucose, for example). However, despite these limitations, our data demonstrate that an 8-week intervention combining HIIT and vibration training together with a hypocaloric diet can improve body composition (percentage fat mass) and lipid profiles (triglycerides and total cholesterol) in overweight and obese participants. These results may be used as support for the prescription of different intensities of aerobic exercise and recovery methods in the management for obesity, aiming not only to increase energy expenditure but also to improve the lipid profile in this population.
Footnotes
Authors’ Note
Trial Number: ACTRN12613000287730. Sañudo contributed to study concept and design, interpretation of data, critical review of the manuscript, and made intellectual contributions to approval of final manuscript. Del Pozo-Cruz J contributed to drafting and critical review of the manuscript. Lopez-Lluch contributed to reagents, materials, data analyses, and displays; Muñoz contributed to data acquisition. Davison contributed to interpretation of data and critical review of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.