
Abstract
This investigation examined the acute effects of continuous whole-body vibration (CWBV) and intermittent whole-body vibration (IWBV) on neuromuscular and functional measures in women with sarcopenia and nonsarcopenic women. Continuous whole-body vibration was one 6-minute exposure, while IWBV consisted of six 60-second exposures to rest intervals (30 Hz, 2-4 mm amplitude). Factorial analyses revealed group × exposure × time interactions for jump height (JH; F = 10.8, P = .002), grip strength (GS; F = 15.5, P < .001), timed up and go test (F = 11.7, P = .002), and sit and reach test (S&R; F = 9.7, P = .004). Both JH and GS significantly improved post-WBV in women with sarcopenia (P < .001), with post-IWBV significantly greater (P < .001) than post-CWBV. Timed up and go test and S&R significantly improved post-IWBV in both the groups (P < .001) with post-IWBV significantly better than post-CWBV (P < .001). Bench press power at 20% one repetition maximum (1RM) revealed an exposure × time interaction (F = 4.6, P = .04) illuminating that IWBV significantly improved muscular power (P < .001). Bench press power at 40% 1RM revealed group × exposure (F = 6.4, P = .016) and exposure × time interactions (F = 5.8, P = .022). Individuals with sarcopenia significantly increased power output (P < .001) post-IWBV which was significantly greater than post-CWBV (P = .037). Bench press power at 60% 1RM revealed an exposure × time interaction (F = 8.6, P = .006), indicating that power was significantly improved post-IWBV (P = .027) and decreased post-CWBV. Berg Balance scale revealed a time main effect (F = 6.64, P = .015), and pain discomfort was significantly lower post-IWBV. These data indicate IWBV may provide a more efficacious exposure pattern in older women when compared to CWBV.
Introduction
Age-related reductions in skeletal muscle mass are linked to decreased quality of life (QOL), mobility, and an increase in adverse health events. 1,2 The reductions in skeletal muscle mass are quantified through a decrease in muscle quantity and quality characterized as sarcopenia. Sarcopenia displays a directly proportional relationship with age, with previous literature revealing reductions in muscle quantity and quality occurring at rates of 1% to 2% and 1.5% to 3% per year after 50 years of age, while corresponding functional impairments become most evident in the seventh decade. 3,4 Although a precise understanding of the mechanisms involved in the progression and onset of sarcopenia remain ambiguous, compelling evidence exists suggesting alterations in the number, size, and remodeling of muscle fibers as well as reduced mitochondrial function, decreased protein synthesis, and diminished neuromuscular integrity, 3,5 all contribute to a clinically diagnosable loss of fat free body mass.
The number of individuals classified as having sarcopenia is expected to increase, as the proportion of older individuals continues to grow. Estimates suggest that sarcopenia affects more than 50 million people and will affect more than 200 million by 2050. 5 Therefore, there is an urgent need for the development of interventions that possess the ability to combat sarcopenia. Resistance exercise (RE) with light or heavy loads appears to have the capacity to mediate the age-related effects on muscle; however, training with heavier loads provides larger increases in muscular adaptation 6 and may provide benefit to the skeletal system. Since it may not be feasible for older individuals to perform heavy RE, alternative interventions, such as whole-body vibration (WBV), are being evaluated as potential interventions to counteract sarcopenia.
Whole-body vibration imparts high-frequency mechanical stimuli that is transmitted through the body. 7 The mechanical stimulus is referred to as the acceleration, which is a product of the frequency and amplitude during an exposure. Previous literature suggests that the mechanical stimuli stimulates endings of muscle spindles which leads to an activation of alpha motor neurons facilitating muscle contraction. 8,9 When compared to RE, WBV provides a substantial advantage, allowing the ability to potentiate muscular activity without the accompanying safety and adherence issues associated with RE. Additionally, previous research indicates that WBV results in comparable muscular adaptations as those observed from RE. 10 -13 However, some research has reported contradictory results, 14 -16 which could be attributed to differences in WBV methodology. The exposure stimulus (Hz) and duration have received thorough evaluation; however, the pattern of exposure is often overlooked. Whole-body vibration protocols utilize 2 exposure patterns, intermittent whole-body vibration (IWBV) and continuous whole-body vibration (CWBV). Intermittent whole-body vibration provides exposures in predetermined exposure to rest intervals, while CWBV provides a single exposure for a predetermined time. 7 Although evidence exists regarding older individual’s response to WBV interventions, there is a dearth of literature evaluating the immediate effects of WBV. Therefore, this deficiency in literature impedes the ability to progress toward forming an optimal vibration protocol to maximize benefits for the elderly individuals. Immediate benefits post-WBV in young individuals include increased muscle function, flexibility, and balance. 17 -22 If similar effects are observed in older individuals, the ability to perform activities of daily living (ADLs) or RE may become easier and may lead to reducing the effects of sarcopenia and improving QOL. Currently, no investigation has compared the acute effects of IWBV and CWBV on neuromuscular and functional measures. Therefore, the purpose of this investigation was to examine the acute effects of IWBV or CWBV on neuromuscular and functional measures in elderly women.
Methods
Participants
Older women (50-70 years) were recruited to participate in the present study. Participants completed a written informed consent form, and all methodology was approved by a university institutional review board. Participant inclusion criteria included ≥50 years of age, no self-reported falls within the previous year, absence of unmanaged cardiovascular disease or diabetes, and the ability to perform strength and power testing. Forty-one women met the inclusion criteria and were enrolled in the investigation. Six women did not complete the investigation for reasons not related to the study; therefore, 35 (N = 35) participants were included in statistical analyses.
Research Design
During the first visit, each participant completed informed consent, and health status questionnaires (HSQs) were required to perform submaximal familiarization trials of each included measure, become familiar with the body composition analysis positioning, and were provided with medical clearance forms. Once medical clearance was obtained, participants returned to the laboratory and underwent body composition analysis, then performed a 5-minute cycle warm-up (<50 Watts), followed by neuromuscular and functional measures testing without vibration exposure in the following order: vertical jump (VJ) height, bench press 1 repetition maximum (1RM), Berg Balance Testing, grip strength (GS), timed up and go (TUG), sit and reach flexibility testing, and bench press power (BPP) testing. Following the initial testing visit, each participant performed 4 total testing visits encompassing neuromuscular and functional measure testing. The 4 visits were randomized into 2 testing visits per exposure (Figure 1) and included a 5-minute cycle warm-up (<50W) prior to testing. During each WBV visit, participants performed the neuromuscular and functional measures, rested for 30 minutes, underwent WBV (IWBV or CWBV), and then reperformed the measures. Vibration protocols were randomly selected before each visit and then removed to ensure no duplication.
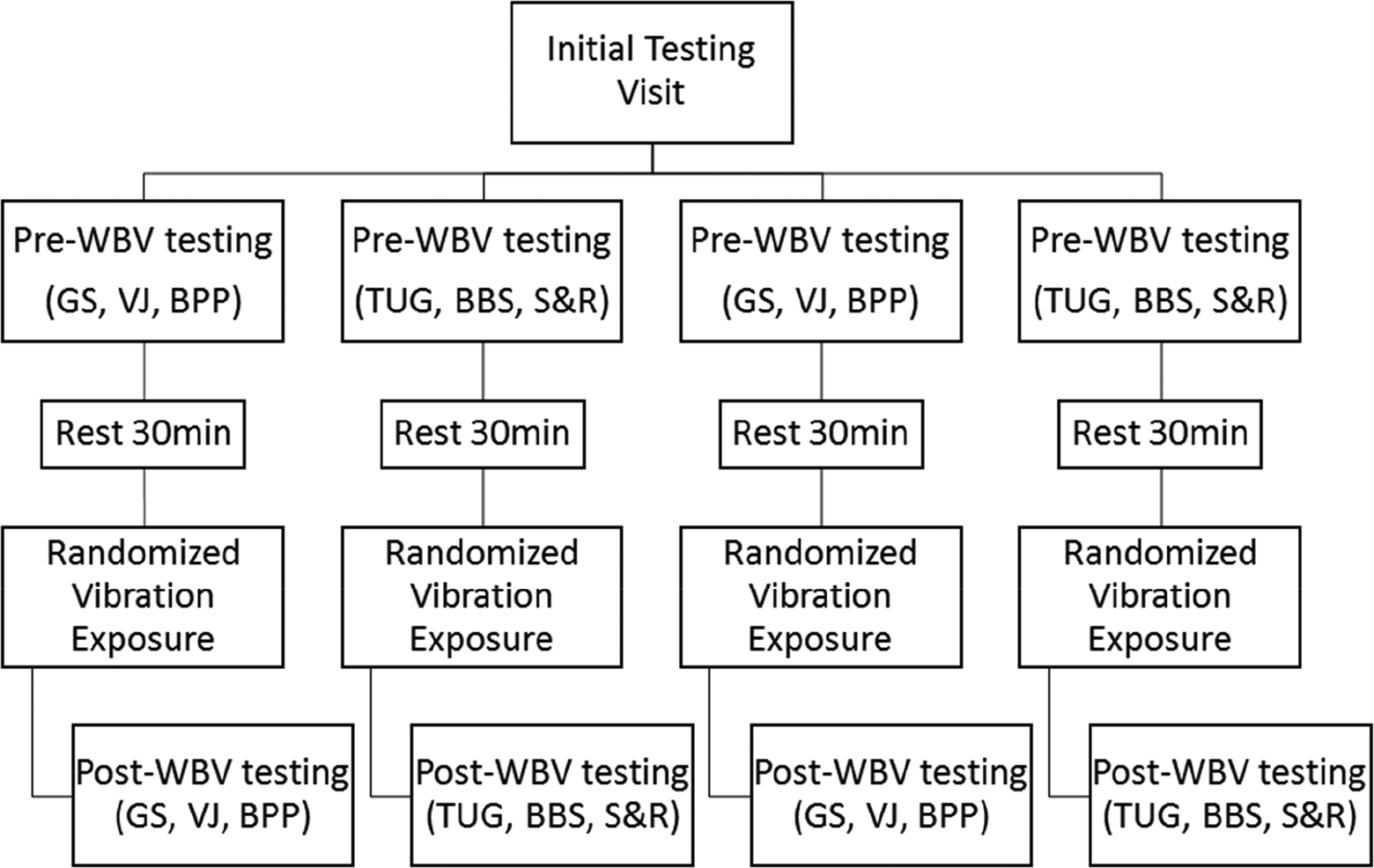
Participant testing design.
Questionnaires
Each participant completed a physical activity scale for the elderly (PASE) and a HSQ. The PASE consists of a brief survey to assess physical activity in older individuals combining activity from leisure, household, and occupational activities. The HSQ was a laboratory designed questionnaire collecting information regarding demographics, current and past medication history as well as current and past musculoskeletal injuries.
Body Composition Analyses
Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer (Novel Products Inc., Rockton, Illinois), and body mass was measured to the nearest 0.1 kg by a digital scale (Tanita, Arlington Heights, Illinois). Dual energy X-ray absorptiometry (GE, Lunar Prodigy, Madison, Wisconsin) was used to assess body composition. One qualified technician performed all scans, analyses of scans, and quality assurance procedures prior to each scan. Precision coefficients of variation of 1.31%, 0.67%, 1.18%, and 0.84% for percentage of body fat, bone free lean body mass, fat mass, and lean body mass, respectively, have been determined from the laboratory. Sarcopenia was determined by a skeletal muscle index <0.512, which was calculated as the quotient of appendicular skeletal mass over body mass index. Appendicular skeletal mass was calculated using the sum of lean tissue mass from the arms and legs determined by regions of interest positioned bisecting the glenohumeral joint and femoral neck, respectively. 23
Whole-Body Vibration Exposure
Whole-body vibration was applied using a Power Plate platform (Northbrook, Illinois) with a frequency of 30 Hz and amplitude of 2 to 4 mm. The CWBV consisted of one 6-minute bout of WBV, while the IWBV consisted of six 1-minute exposures separated by a 1-minute rest interval. Exposure durations and frequencies were selected based on previous research. 24 -26 During each exposure, participants stood bare foot on the platform, legs shoulder width apart, knees flexed to a 30° angle, and their arms placed equidistant on the device handles.
Grip Strength
Grip strength was assessed using a hand-held dynamometer (Takei Instruments, Japan). Participants stood with the shoulder adducted, elbow flexed to 90°, and were instructed to provide maximum effort for several seconds and then relax on verbal command. Measurements were taken 3 times on the dominant hand separated by 60 seconds, and the average of the trials was included in the analyses.
Vertical Jump
Jump height (VJ) was determined from 3 countermovement jumps performed on a Just Jump mat (Just Jump; Probotics Inc, Huntsville, Alabama). Participants were instructed to descend into a comfortable, self-selected countermovement depth, incorporating their naturally synchronized arm swing action, immediately jump straight up in one continuous motion, refrain from bending their legs in the air, and ultimately land with both feet on the mat. Three jump trials were performed, separated by 60 seconds, and the average was included in the analyses.
Bench Press One Repetition Maximum Testing
Bench press 1RM testing began with each participant performing 1 set of 10 repetitions with a polyvinyl carbon pipe. Following 60 seconds rest, participants performed 1 set of 5 repetitions with a 10-pound barbell. After 2 minutes rest, the load was increased in 5 to 10 pound increments until a maximum effort to failure was achieved, with each 1RM test determined within 5 attempts.
Bench Press Power
Bench press power at 20%, 40%, and 60% bench press 1RM were measured using a FitroDyne analyzer (Tendo Weightlifting, Trencin, Slovak Republic). Participants were instructed to push the barbell with as much force and as fast as possible. Each participant performed 3 repetitions at 20%, 40%, and 60% of 1RM in randomized order, with 60 seconds between subsequent trials, with the average value for each intensity included in the analyses. Percentages were determined from 1RM testing during the initial testing visit, and participants were provided 1-minute rest between repetitions.
Timed Up and Go Test
The TUG consisted of participants starting in a seated position, rising from the seat, moving as quickly as possible to a cone placed 3 m in front of the chair, and returning to the seated position. Test times were recorded using a stopwatch and started upon the participant’s first movement and time stopped when the participant returned to the original seated position. Participants were instructed to only use their upper body to rise from the chair only when absolutely necessary. Three trials were performed separated by 60 seconds, and the average value was included in the analyses.
Berg Balance Scale
The Berg Balance scale (BBS) consists of 14 items that are scored on a scale of 0 to 4. The BBS is a commonly employed clinical evaluation used to assess an individual’s static and dynamic balance, providing insight into their capacity to perform balance and mobility tasks, which include measures of single and double leg performance, weight transfers, and body control. A score of 0 is given if the participant is unable to perform the task, and a score of 4 is given if the participant is able to complete the task as described. The maximum achievable score is 56, and the BBS testing order was identical for each participant.
Sit and Reach
The sit and reach test (S&R) was administered using an Accuflex Tester (Gym Closet, Inc, Temperance, Michigan) and completed according to the American College of Sports Medicine guidelines. 27 Each participant performed 3 trials separated by 60 seconds, each measurement was recorded to the nearest half centimeter, and the average of the 3 trials was included in the statistical analyses.
Rating of Perceived Discomfort
Following each WBV exposure, participants were asked to rank their discomfort. The Numeric Rating Scale for Discomfort is a segmented numeric version of the visual analog scale which requires the participant to rate their discomfort from 0 to 10. A score of 0 indicates no discomfort while a score of 10 indicates the most discomfort the participant can endure.
Statistical Analyses
Three-way repeated-measures analyses of variance (ANOVA; group [sarcopenia and nonsarcopenia] by condition [CWBV and IWBV] by time [pre-WBV and post-WBV]) were used to test the main effects and interactions between the group, condition, and time for each variable. Whenever a significant 3-way interaction was observed, separate 2-way repeated measures ANOVA for each group were conducted, and post hoc comparisons with Bonferroni correction were examined. Reliability of neuromuscular and functional measures was assessed using intraclass correlation coefficients (ICC) between the initial testing visit and all pre-WBV exposures. An α level of .05 was used, and analyses were conducted using Statistical Package for Social Sciences (SPSS, version 21, Chicago, Illinois). Sample size was calculated a priori with an estimated effect size of 0.25 which required a sample size of N = 30 to achieve a statistical power of 0.80.
Results
Thirty-five women completed the study with 15 participants classified as sarcopenic (Table 1). 28,29 Each outcome measure revealed moderate to excellent 30 reliability (ICC: 0.71-0.95) across all trials and were not significantly different across testing days. Significant differences were observed across all time points for the neuromuscular and functional measures between the sarcopenic and nonsarcopenic groups. Percentage change post-WBV for functional measures are presented in Figures 2 and 3 for the sarcopenic and nonsarcopenic groups, respectively, and neuromuscular measures for both groups are reported in Table 2. Discomfort scores reported immediately post-WBV revealed a significantly lower score post-IWBV when compared to post-CWBV. Finally, all participants were able to complete each exposure pattern while maintaining the instructed position on the vibrating platform.
Physical Characteristics.

Abbreviations: ASM, appendicular skeletal muscle mass; BMI, body mass index; cm, centimeters; DBP, diastolic blood pressure; SBP, systolic blood pressure; mm Hg, millimeters mercury; kg, kilograms.
a Significantly different between groups at P < .05 level.
b Significantly different between groups at P < .001 level.

Functional measure percent change following IWBV (solid bar) and CWBV (gray bar) for sarcopenic group. Significance as follows: α, P < .001 between vibration patterns; β, P < .001 pre- to postvibration; δ, P < .05 pre- to postvibration. BBS indicates Berg Balance Scale; CWBV, continuous whole-body vibration; IWBV, intermittent whole-body vibration; S&R, sit and reach flexibility test; TUG, timed up and go test; VJ, vertical jump.

Functional measure percent change following IWBV (solid bar) and CWBV (gray bar) in nonsarcopenic group. Significance as follows: δ, P < .05 pre- to postvibration. BBS indicates Berg Balance Scale; CWBV, continuous whole-body vibration; IWBV, intermittent whole-body vibration; S&R, sit and reach flexibility test; TUG, timed up and go test; VJ, vertical jump.
Neuromuscular Measures for Sarcopenic (n = 15) and Nonsarcopenic Groups (n = 20).
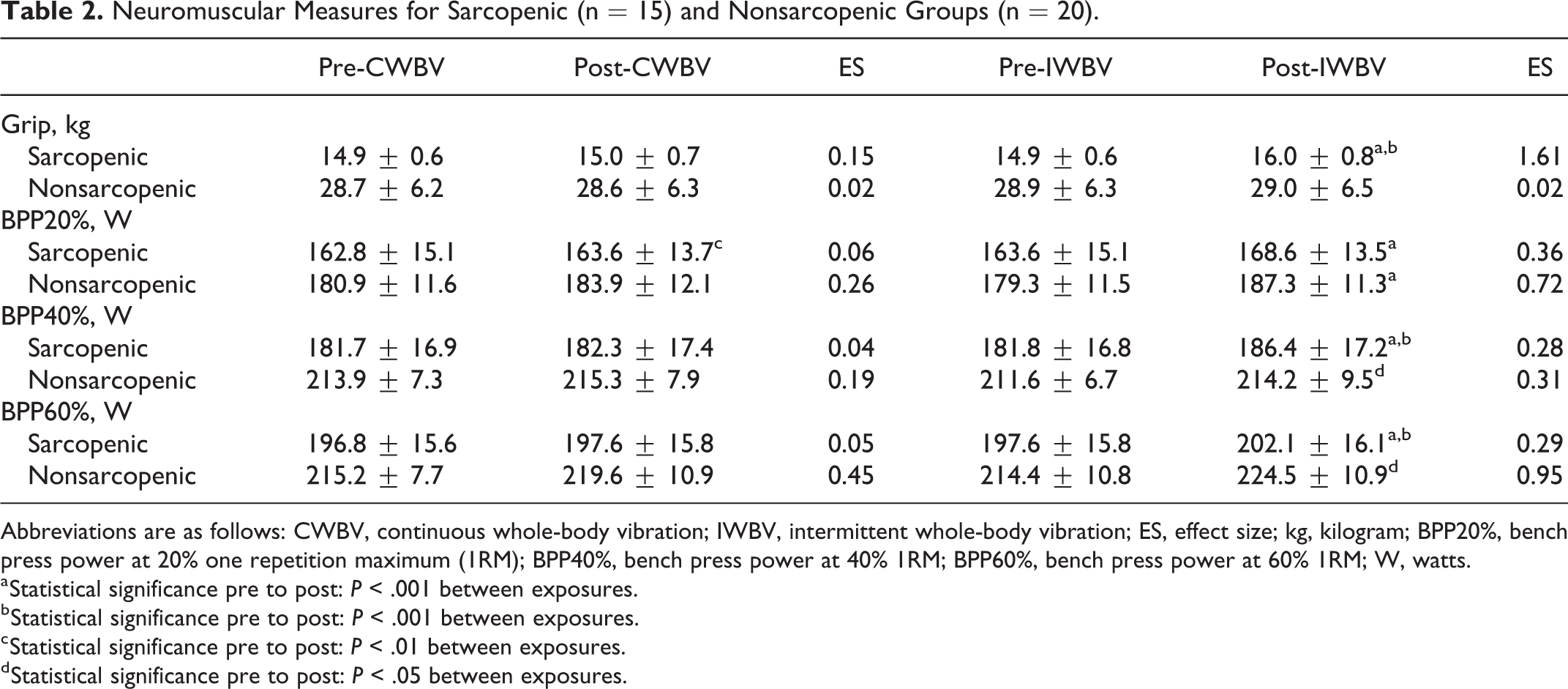
Abbreviations are as follows: CWBV, continuous whole-body vibration; IWBV, intermittent whole-body vibration; ES, effect size; kg, kilogram; BPP20%, bench press power at 20% one repetition maximum (1RM); BPP40%, bench press power at 40% 1RM; BPP60%, bench press power at 60% 1RM; W, watts.
a Statistical significance pre to post: P < .001 between exposures.
b Statistical significance pre to post: P < .001 between exposures.
c Statistical significance pre to post: P < .01 between exposures.
d Statistical significance pre to post: P < .05 between exposures.
Analysis of the VJ data revealed a significant group × intervention × time interaction (F = 10.8, P = .002, η2: 0.89). There were significant main effects for intervention (F = 76.7, P < .001, η2: 0.85) and time (F = 86.8, P < .001, η2: 0.86) as well as a significant intervention × time interaction (F = 81.2, P < .001, η2: 0.85) for the sarcopenic group. Vertical jump significantly increased post-IWBV (P < .001) and was significantly higher than post-CWBV (P < .001). No significant main effects (intervention P = .08; time P = .5) or interactions (intervention by time interaction, P = .8) were observed in the nonsarcopenic group.
There was a significant group × intervention × time interaction (F = 15.5, P < .001, η2: 0.31) for GS. Women with sarcopenia revealed significant intervention (F = 53.8, P < .001, η2: 0.79) and time (F = 27.1, P < .001, η2: 0.57) main effects and an intervention × time interaction (F = 27.1, P < .001, η2: 0.65). Grip strength significantly increased post-IWBV (P < .001) and was significantly stronger than post-CWBV (P < .001). No significant main effects (intervention P = 0.21; time P = .83) or intervention × time interaction (P = .57) were observed in nonsarcopenic individuals. Berg Balance scale had a significant time main effect (F = 6.64, P = .015, η2: 0.17), and the post hoc analyses indicated that BBS were significantly improved post-WBV (P = .015).
A significant group × intervention × time interaction (F = 11.7, P = .002, η2: 0.26) was observed for TUG. Individuals with sarcopenia revealed significant main effects for intervention (F = 27.5, P < .001, η2: 0.66) and time (F = 57.2, P < .001, η2: 0.80) as well as a significant intervention × time interaction (F = 45.8, P < .001, η2: 0.77). Post hoc analyses revealed significant decreases post-WBV (CWBV P = .02; IWBV P < .001). Significant differences were observed between post-WBV TUG scores revealing that TUG time was significantly faster (P < .001) post-IWBV. Nonsarcopenic individuals displayed main effects for intervention (F = 5.8, P = .026, η2: 0.23) and time (F = 8.9, P = .008, η2: 0.32). Furthermore, IWBV significantly improved TUG time (P = .014), while CWBV did not.
The S&R revealed a significant group × intervention × time interaction (F = 9.7, P = .004, η2: 0.23). For women with sarcopenia, the main effects for intervention (F = 29.3, P < .001, η2: 0.68) and time (F = 41.6, P < .001, η2:0.75) and a significant intervention × time interaction (F = 22.4, P < .001, η2: 0.62) were observed. Both exposures (CWBV P = .001; IWBV P < .001) significantly improved S&R, with post-IWBV producing a significantly greater (P < .001) S&R than post-CWBV. In nonsarcopenic individuals, a significant main effect for time (F = 5.9, P = .025, η2: 0.24) indicated improved S&R scores post-WBV.
Bench press power at 20% 1RM (BPP20%) revealed a main effect for time (F = 16.2, P < .001, η2: 0.33) and a significant intervention × time interaction (F = 4.6, P = .04, η2: 0.12). Bench press power at 20% was significantly greater post-IWBV (P < .001) but not post-CWBV (P = .133). Bench press power at 40% 1RM revealed a significant time main effect (F = 8.6, P = .006, η2: 0.21) and significant group × intervention (F = 6.4, P = .016, η2: 0.16) and intervention × time interactions (F = 5.8, P = .022, η2: 0.15). Pairwise comparisons indicated the BPP40% was significantly greater post-WBV (P = .006). Women with sarcopenia significantly increased power (P < .001) post-IWBV, and the power post-IWBV was significantly greater (P = .037) than post-CWBV. Significant main effects for time (F = 13.9, P = .001, η2: 0.29) and intervention (F = 5.4, P = .027, η2: 0.14) were observed and an intervention × time interaction (F = 8.6, P = .006, η2: 0.21) for bench press power at 60% 1RM (BPP60%) indicating that BPP60% was significantly greater (P = .001) post-WBV.
Discussion
Given the magnitude of change in neuromuscular and functional performance and post-WBV discomfort ratings, the present findings indicate that IWBV may be a more advantageous exposure pattern for older women compared to CWBV. Additionally, the present data provide novel evidence that upper body muscular performance can be augmented following upright WBV application. Finally, older women classified as having sarcopenia experience a greater improvement post-WBV when compared to those not classified as sarcopenic; thus, WBV could potentially be prescribed as a form of therapeutic intervention in women with sarcopenia and may augment a carefully designed RE program.
The novel design and inclusion of older individuals in the present study creates a challenge to compare our findings with those previously reported in young participants. The present data indicates that IWBV may be a more efficacious exposure pattern. For example, the nonsarcopenic women revealed no significant improvements post-CWBV; however, TUG time and BPP were significantly improved post-IWBV. Women with sarcopenia significantly improved in each assessment measured, with the exception of the BBS post-IWBV, while only TUG time, S&R, and BPP20% were significantly improved post-CWBV. Finally, both groups of women reported lower discomfort scores post-IWBV, thus indicating a more tolerable exposure pattern.
Previous research provides compelling evidence advocating IWBV as an intervention to combat the effects of sarcopenia. Wei et al 31,32 employed 4 IWBV frequency/duration combinations with 5-minute rest intervals and observed significant improvements in functional and neuromuscular measures following 12 weeks of IWBV training. Additionally, Chang et al 33 employed an IWBV design exposing participants to ten 60-second exposures with 30-second rest intervals 3 times a week for 12 weeks and observed improved skeletal muscle index, physical fitness, and QOL. Interestingly, the aforementioned study consisted of institutionalized participants, while the present study and those of Wei et al 31,32 were community-dwelling seniors. Although this study examined healthy older women, it should be mentioned that WBV interventions have been shown to be an effective training modality in clinical populations, such as the oldest old (80+ years) 34 and those with type 2 diabetes. 34 -36 Cumulatively, these data suggest that IWBV possesses the ability to acutely and chronically augment neuromuscular and functional indices as well as enhance QOL in sarcopenic and clinical populations.
In an attempt to isolate the ideal exposure pattern, we employed a study design that equated volume between exposures. It could be speculated that greater change post-IWBV may be due to the balance of potentiation and fatigue. 37,38 Previous literature indicates that WBV can preferentially stimulate fast-twitch muscle fibers 39 ; however, the CWBV exposure may have reached its peak application with the participant on the platform allowing fatigue to set in, whereas IWBV potentiated performance without fatigue accumulation. Future research should examine the influence of exposure time on subsequent performance and the underlying mechanism(s) associated with each exposure pattern.
The observation of improved neuromuscular performance following a bout of WBV is supported by previous research, with most of these observations in young participants. 17,21,22,38,40,41 However, Giombini et al 25 examined the influence of vibration frequency on power output of the lower limbs in older women using an IWBV protocol. The study employed a 60-second rest to interval paradigm with a similar frequency as the present study and observed increased power output. The authors speculated that different frequencies may be required to facilitate neuromuscular augmentation for different areas of musculature; however, the present data reveals that IWBV also possessed the ability to significantly increase upper body power, thus contradicting the speculation.
Upper body neuromuscular performance was significantly improved post-IWBV in women with sarcopenia. The same measures, with the exception of GS in nonsarcopenic women, were improved post-IWBV with the only measure significantly improved post-CWBV being BPP20% in women with sarcopenia. Based on the data from the current study, CWBV does not appear to augment upper body neuromuscular performance. 17,42,43 The present observations are novel and may provide the basis for future studies. Given age-related flexibility and mobility impairments, the present data advocate maintaining upright posture, which reduces the requirement for participants to assume incommodious positions during WBV. These improvements may allow ADL to become less labor intensive and may increase independence or QOL.
Timed up and go test time and S&R significantly improved following both exposures in women with sarcopenia; however, post-IWBV produced significantly better scores than post-CWBV. Previously, Tsuji et al 44 examined the effects of IWBV and observed significant decreases in TUG time as well as a nonsignificant increase in S&R. Decreased TUG time is meaningful, as the test evaluates an integration of strength, agility, coordination, and power of the lower limbs. The present data revealed significant improvements in S&R following either exposure in women with sarcopenia and nonsignificant improvements in nonsarcopenic women; thus, the data from both studies indicate that flexibility can be improved post-WBV. Furthermore, Carlucci et al 45 employed a 9.5-minute CWBV exposure and reported no changes in postural control in elderly women, which is in agreement with the present data for both exposure patterns. Therefore, the combined findings suggest that WBV can be safely administered without compromising stability post-WBV.
The current study was not without limitations. First, the study was designed to compare the acute effects of CWBV and IWBV. Therefore, we cannot discuss or allude to an “optimal” protocol, only suggest which exposure pattern may progress the development of an “optimal” protocol. Second, the selected duration may not have elicited the most profound improvements. Although many of the included measures revealed significant improvements, we cannot rule out that moderate increases or decreases in exposure duration may have produced different results. Third, the study design only evaluated neuromuscular and functional measures once after the exposure; thus, we are not able to discuss how long the improvements were maintained post-WBV or the effects of a WBV training program. Finally, our results may not be generalized to older men since the study consisted of only women.
Conclusions
In conclusion, WBV appears to be a possible intervention for augmenting neuromuscular and functional measures in elderly women. Furthermore, IWBV appears to be a more efficacious exposure pattern, and we recommend that IWBV be implemented in health care or assisted living facilities to garner improvements in neuromuscular and functional performance in attempt to reduce the difficulty in ADL while increasing independence and QOL.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.