
Abstract
A 10-year survey of immune status of nuclear power plant (NPP) workers was assessed by cellular and humoral immune parameters. The cumulative doses of NPP workers were in the range of 0.06 to 766.36 mSv. The results did not show significant deviations in the studied parameters of cellular and humoral immunity, but a tendency of elevated values in CD3+4+ helper inducers cells, especially its CD4+62L+ subpopulation, regulatory CD4+25+ cells, CD8+28+ cytotoxic subpopulation, and immunoglobulin M, was established. The observed trend of the above-mentioned parameters could be interpreted by assumption that while the adaptation processes are dominated with low prevalence of T-helper (Th) 1 immune response to cumulative doses less than 100 mSv, a switch to Th-2 response occurred at doses above 100 mSv. The impact of a number of other confounding factors on the immune system does not allow definitive conclusions about the direct radiation-induced changes in immune parameters.
Introduction
A key issue in radiobiology is the health risk assessment. To solve this problem, special attention is paid to the health status of workers chronically exposed to low-dose radiation in nuclear industry. The radiological hazard associated with nuclear generation are notably different from the occupational hazard associated with other methods for power generation. Epidemiological studies 1 –4 of nuclear power plant (NPP) contingents are controversial because of other factors such as living conditions, harmful habits, and improved radiation protection measures in the recent years. Effects of chronic low-dose radiation on changes in immunological parameters and state of subclinical inflammation require careful examination of the immune status of occupationally exposed persons. Some authors found that doses in the range of 10 to 100 mGy lead to prevalence of T1 helper subpopulation (Th1), while doses above 200 mGy switch the prevalence of T2 immune response which determines an increased risk of neoprocesses, infectious diseases, allergies, and autoimmune diseases. 5 –8 At the same time, experimental data established that low doses stimulate antitumor immunity manifested by increased activity of T, natural killer (NK) cells, and B cells and higher production of interleukin (IL) 2 (IL-2), IL-12, interferon γ (IFN-γ) cytokines, and induced T helper 1 immune response. 9 –11
Assessment of the main lymphocyte populations of the NPP workers done by us for the last 10 years didn’t show significant differences in the main lymphocyte populations—B and T lymphocytes and NK cells. 12 Although the average values of studied populations were within the reference limits, some trends were obtained at the statistical processing of the results.
The more pronounced deviations found in T lymphocytes, as well as reports of radiation-induced imbalance between TH1 and TH2 immune responses, 5,10,6 –8 suggested the need to include additional indicators aimed at the expansion and refinement of the studied immune parameters.
Materials and Methods
The studied participants consisted of 2 groups, one of 438 employees (421 males and 17 females) working in NPP Kozloduy, Bulgaria, and the other of 65 control persons (49 males and 16 females) at similar age, sex, and length of service without any work-related exposure to ionizing radiation. The study was conducted under contracts between the National Centre of Radiobiology and Radiation Protection of the Ministry of Health of Bulgaria and the NPP Kozloduy aiming to carry out health monitoring and study potential changes in the immunological status of NPP workers due to low-dose occupational exposure. Informed consent was obtained from all participants.
The group of individuals occupationally exposed to external γ radiation was selected from the service personnel of units 5 and 6 of NPP Kozloduy. The radiation doses were determined by NPP individual exposure monitoring program.
For the purposes of our research, the workers were divided into groups according to the cumulative dose received as follows: internal control; up to dose of 20 mSv; up to dose of 100 mSv; up to dose of 200 mSv; and above dose of 200 mSv (Table 1).
NPP Personnel: Groups According to Received Doses, Average Age and Length of Employment.

Abbreviation: NPP, nuclear power plant.
a Indicate the standard deviation (±SD).
After filling in a questionnaire, all participants were subjected to medical examinations and underwent a basic hematological assay to evaluate their health status. Although no deviations in the basic laboratory tests and current infections were found in any of the respondents, some of them were diagnosed with cardiovascular diseases (hypertension and ischemic heart disease), obesity, undiagnosed chronic hepatitis 10 years ago, and other chronic diseases whose distribution among the groups is illustrated in Table 2.
Health Status of NPP Workers.
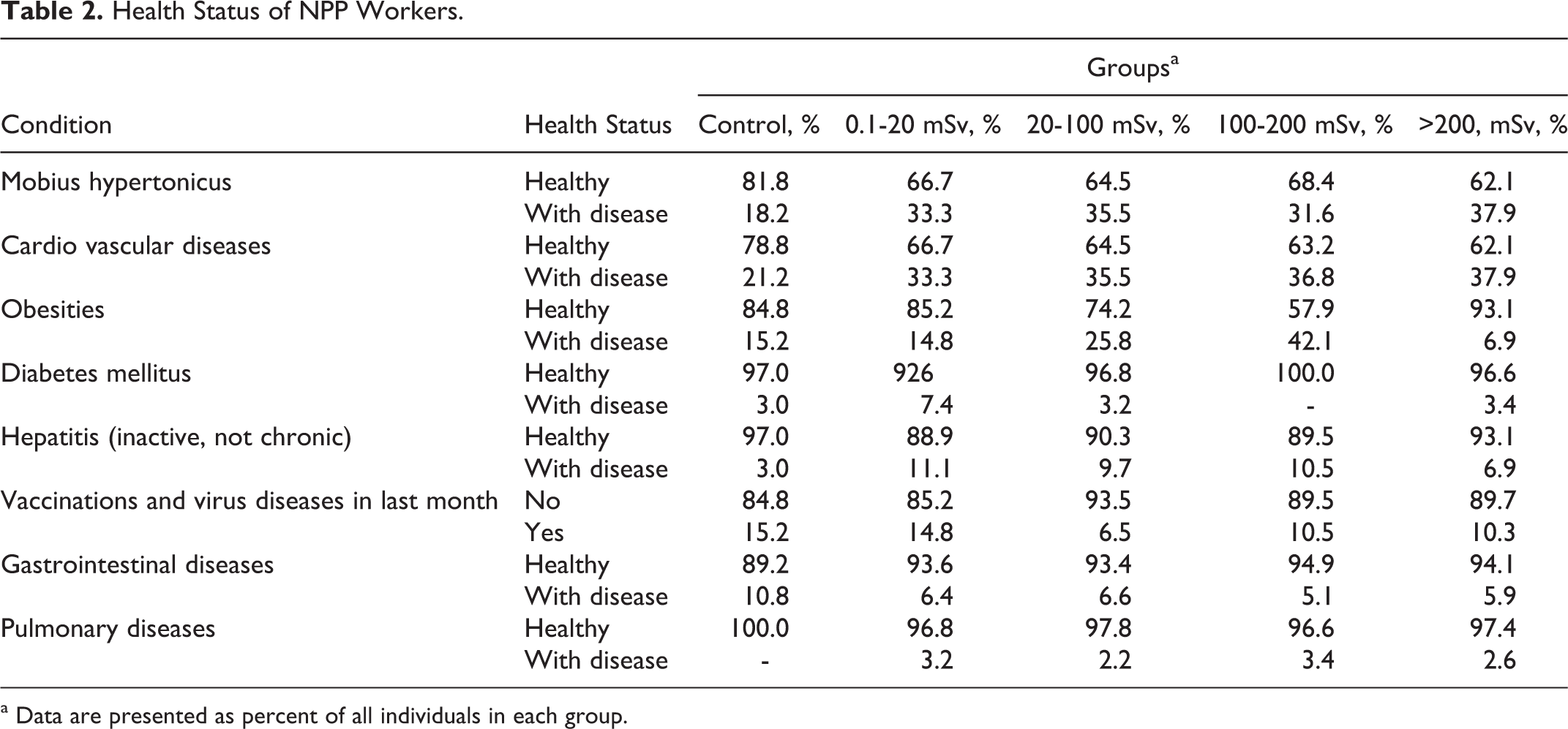
a Data are presented as percent of all individuals in each group.
Four milliliters of blood was collected from each participant by venipuncture into Vacuette EDTA tubes (Greiner Bio-One GmbH, Kremsmunster, Austria). Total white blood cells (WBC) and lymphocytes were counted using an automatic hematology analyzer ABX Pentra 60 C+ (HORIBA GROUP ABX Diagnostics, Montpellier, France) operated in cell blood count + 5 population differential count (CBC+5 DIFF) modes. Blood smears were prepared to observe the WBC morphology. The blood samples were processed, and whole blood was stained with fluoroscein isothiocyanate (FITC)- and phycoerythrin (PE)-conjugated monoclonal antibodies within 6 hours after withdrawal. Lymphocyte subsets were examined as percentages of the lymphocyte count and identified by 2-color flow cytometry in whole blood following erythrocyte lysis according to the method of Jackson 13 as described in Becton Dickinson Monoclonal Antibodies Source Book. Approximately 104 events per sample were analyzed with FACS Calibur flow cytometer (Becton Dickenson Biosciences, San Jose, California). The lymphocyte fraction was gated by forward and right-angle light scatter. Simulset software automatically collected a sufficient number of events to obtain a minimum of 2000 lymphocytes within lymphocyte gate. In addition to the main lymphocyte populations CD3+, CD19+, CD4+, and CD8+, tested in a previous study, in the present investigation CD4+25+, CD4+62L−, CD4+62L+, CD8+28+, CD8+38+ were also analyzed. Simultest IMK-Lymphocyte kit, BD Simultest CD4 FITC/CD62L PE, BD Simultest CD8 FITC/CD28 PE, BD Simultest CD8 FITC/CD38 PE, CD4 FITC, and CD25 PE (Becton Dickinson Biosciences, San Jose, California, USA) were used.
Humoral immunity was studied by the standard method of radial immunodiffusion, and serum levels of immunoglobulin (Ig) G, IgA, and IgM were determined using imunnoplaques (ARCO Inc. Bulgaria, distributer of LTA, Italy).
The reference values for the Bulgarian population defined by the Central Laboratory of Clinical Immunology, University Hospital “Alexandrovska” (Sofia), are listed in Table 3 (Prof. Elisaveta Naumova, Department Clinical Immunology, Alexandrovska Hospital’ Sofia, Bulgaria). In Bulgarian population, no sex-dependent difference is detected in the studied age range.
Reference Valuesa for Lymphocyte Subsets and Immunoglobulin.
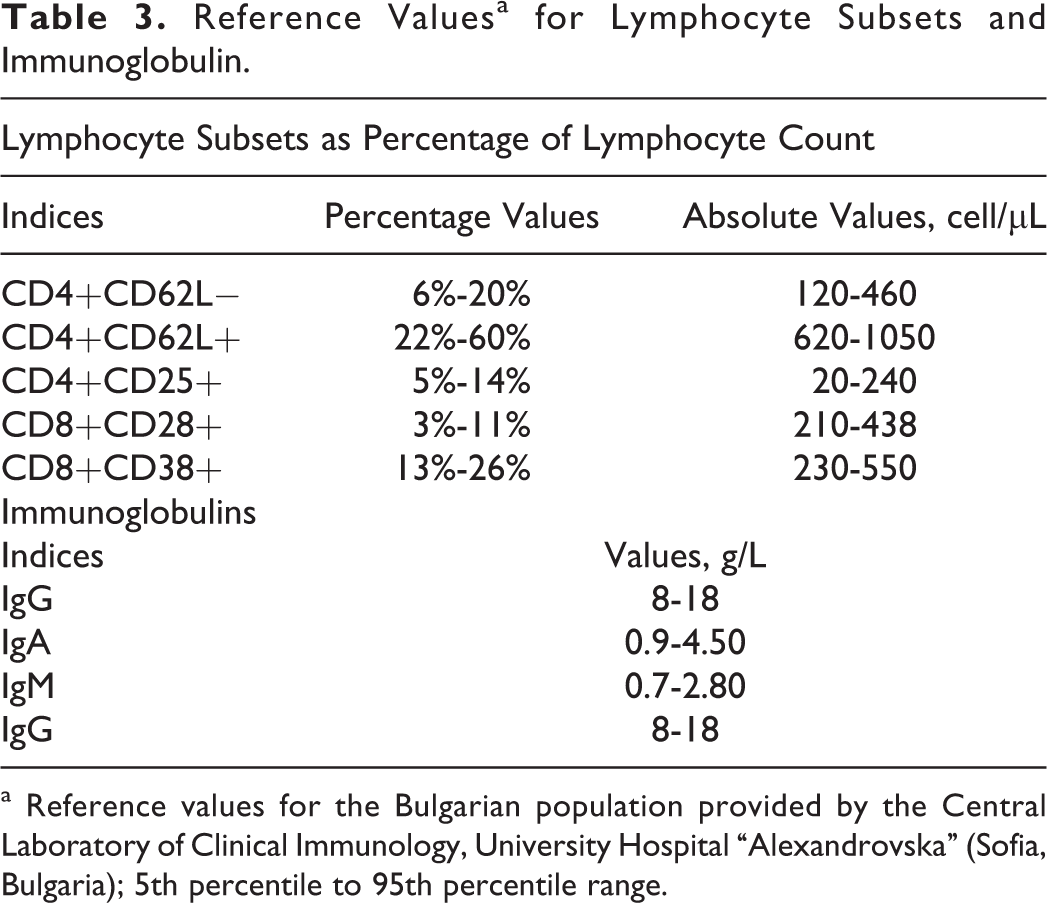
a Reference values for the Bulgarian population provided by the Central Laboratory of Clinical Immunology, University Hospital “Alexandrovska” (Sofia, Bulgaria); 5th percentile to 95th percentile range.
Statistical Methods
The following statistical methods were applied to process the results.
Variation analysis of quantitative variables: Mean, standard deviation, standard error of the mean, and 95% confidence interval of the mean were calculated.
Statistical analysis was performed using parametric and nonparametric methods as follows:
Parametric methods: 1-way analysis of variance (ANOVA) to check the equality of more than 2 mean values in a normal distribution.
Nonparametric methods: Kolmogorov-Smirnov and Shapiro-Wilk tests to check the normality of distribution of quantitative variables; Mann-Whitney U test for comparison of averages in 2 groups of 1 quantitative variable when the distribution is not normal; and Kruskal-Wallis test for comparison of averages in more than 2 groups of quantitative variables when the distribution is not normal.
Frequency analysis: The frequencies of observations occurring in certain ranges of values.
Correlation analysis: Coefficient of linear correlation, parametric (Pearson), and nonparametric (Spearman) analysis.
SPSS version 11.0.1 for Windows was used for data processing. 14,15
Results and Discussion
In our previous study on the same contingent of NPP workers, no significant differences were found between the exposed groups and the control regarding the main lymphocyte populations: B and T lymphocytes and NK cells with phenotypes CD3-16+56+. 12
Although the average values were within the reference limits, a trend of decreasing total CD3+ T lymphocyte was obtained mostly on the account of significant reduction in CD4+ T helper cells with increasing cumulative doses of up to 200 mSv. The heterogeneity of CD3+4+ population and its subpopulations CD4+62L− and CD4+62L+ T cells, as well as activated CD4+25+ T lymphocytes, were investigated for its more precise determination (Figure 1).
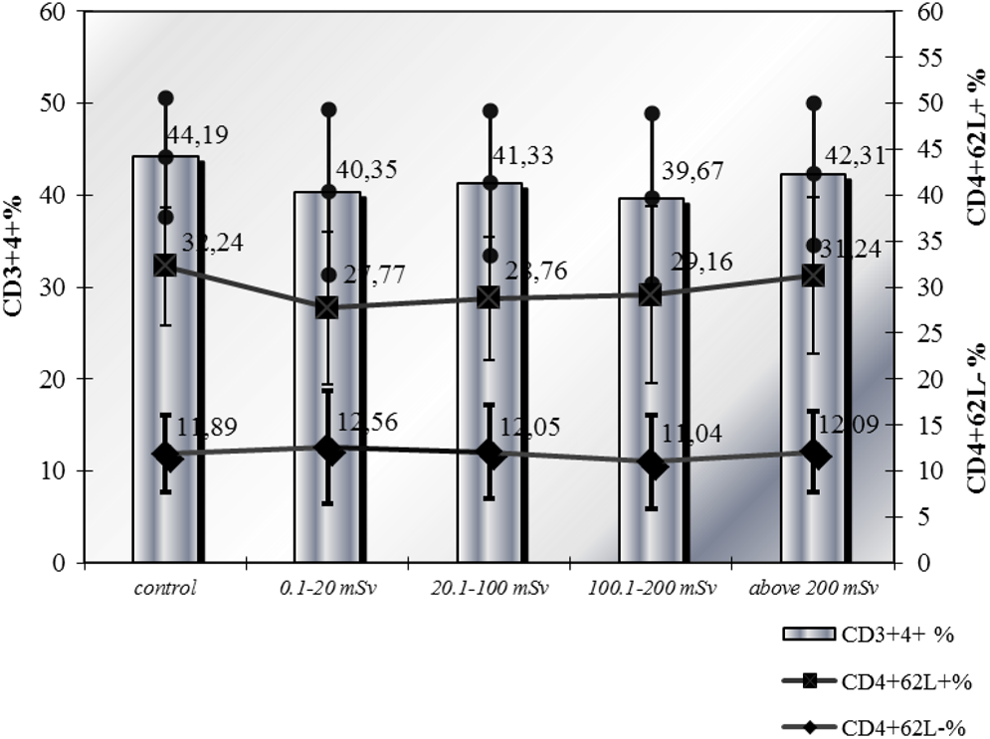
Relative values of CD3+4+, CD4+62L−, CD4+62L+ T lymphocytes.
Lower average percentage values were observed for CD3+4+ lymphocytes in groups with cumulative doses below 200 mSv, statistical confidence was established in the first and third groups, and at doses above 200 mSv there was a tendency of increasing their number (Mann-Whitney U test).
CD4+CD62L−
The data for CD4+62L− subpopulation, mediating helper function in B lymphocyte differentiation, showed a lack of statistically significant differences between the groups and the control (ANOVA; Table 4).
Variation Analysis of CD4+CD62L−, CD4+CD62L+, Activated CD4+25+, Cytotoxic CD8+28+, and Activated CD8+38+ T Lymphocyte in NPP Workers.

Note: Boldface P values show significance of results.
More individuals with elevated above-normal values for CD4+62L− subpopulation were established in the first and fourth groups (Table 5), as the majority of them were smokers (P = .044; Table 6). No correlation of this parameter was found with the dose received, age, and length of service for the observed personnel.
Frequency Analysis of Studied Immune Parameters in NPP Workers given as a Percentage of the Number of Participants Who had Cell Counts Under, Within, or Above Reference Range.
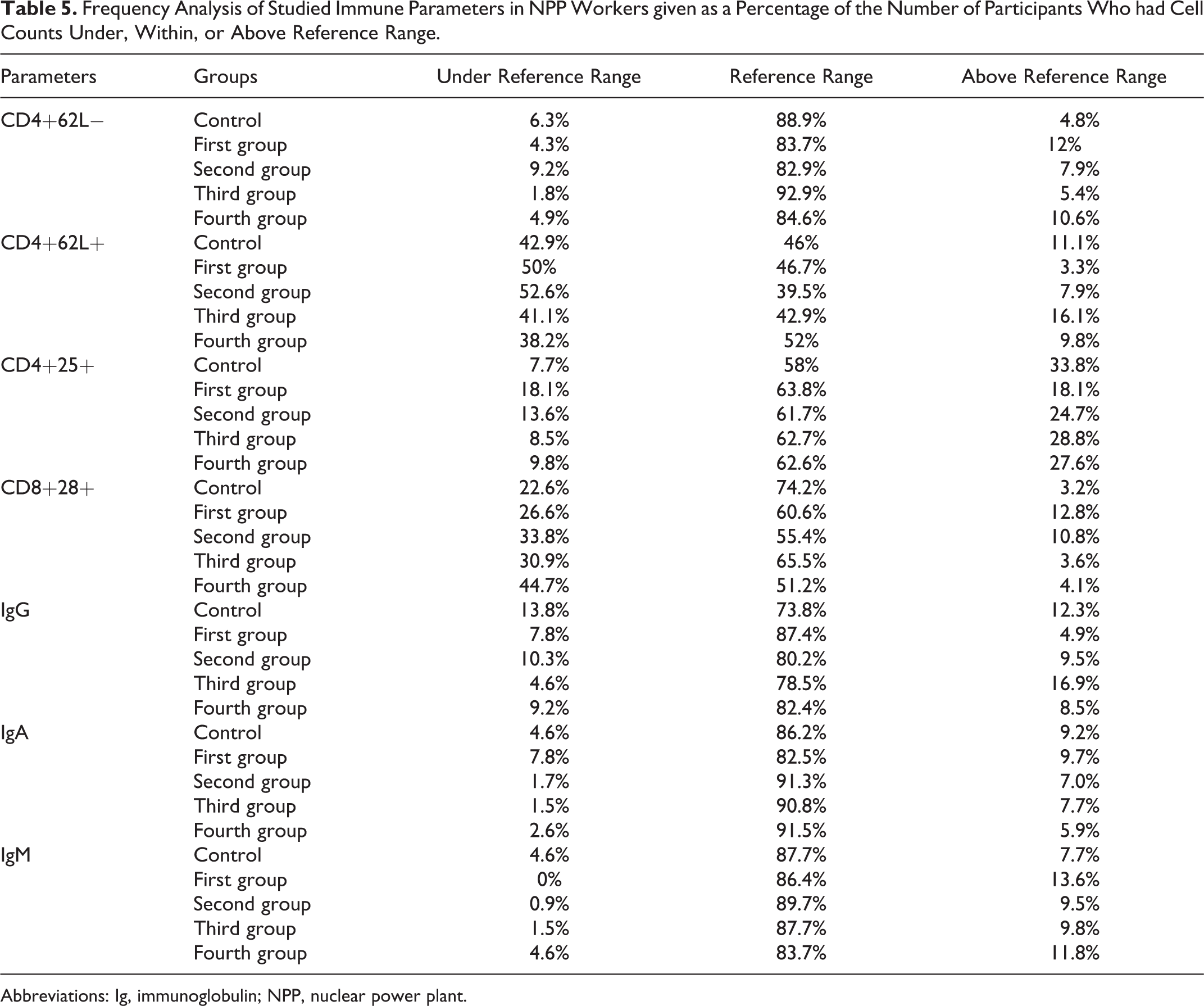
Abbreviations: Ig, immunoglobulin; NPP, nuclear power plant.
Immune Parameters of Smokers and Alcohol Consumers.
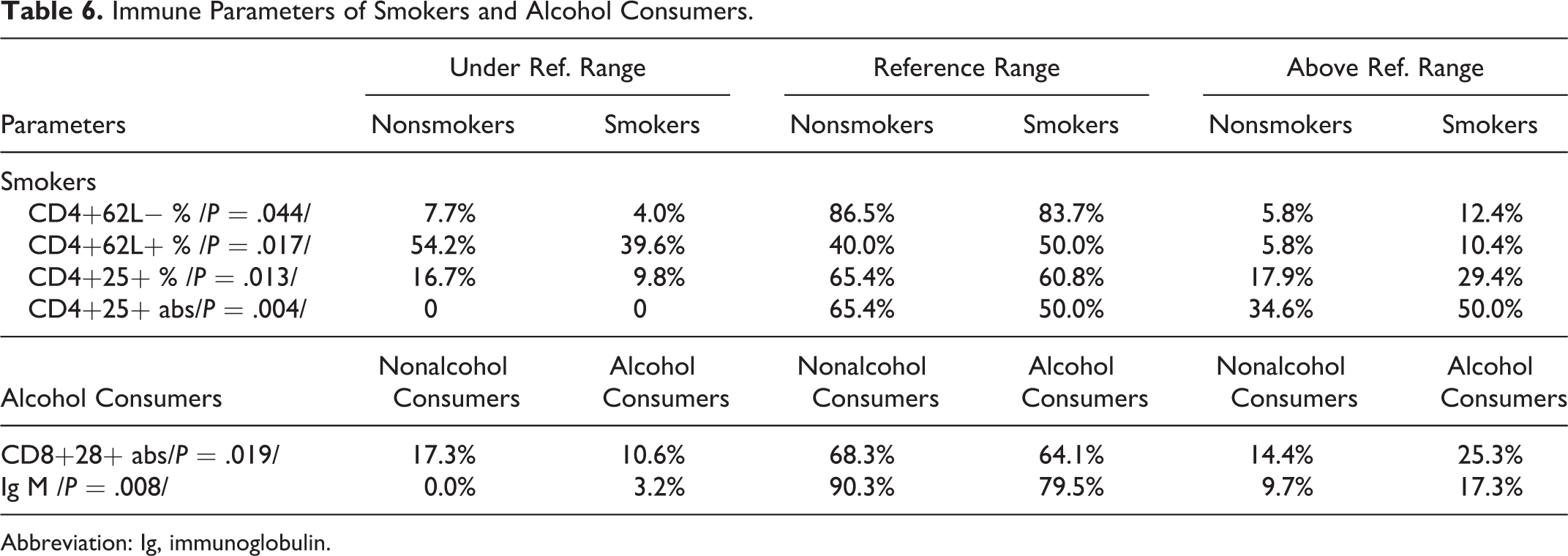
Abbreviation: Ig, immunoglobulin.
CD4+CD62L+
Statistically significant reduction in the mean proportional values of CD4+62L+ subpopulation inducing suppression of B lymphocyte differentiation was found in the first and second groups. Comparison within groups showed statistically significant differences between the mean values in the first and fourth groups (P = .003) and second and fourth groups (P = .021). Upward trend in the average number of this parameter was established with increase in cumulative dose up to 200 mSv, and thereafter it remained at the same level (Table 4).
Frequency analysis showed the highest percentage of persons with values below the reference in the first and second groups, 21.8% and 22.8%, respectively (Table 5). The consumption of alcohol and cigarettes was least significant (P = .017) favoring mainly deviations in this subpopulation (Table 6).
There was a significant weak positive correlation of the relative values of CD4+62L+ lymphocytes with the length of service of respondents (r = .118 at P = .017). The results indicated that with increasing cumulative dose up to 200 mSv, the growth of CD4+62L+ subpopulation was significant and repeated the tendency observed for CD3+4+ cells. At doses above 200 mSv, an elevation in CD4+CD62L cells was observed, but CD4+CD62L+ subpopulation remained at almost the same number. Some authors have reported that the memory CD45RO+CD4+ cells could be divided into 2 subgroups based on expression of L-selectin receptor (CD62L). 16,17 It was found that the memory CD4+CD62L+ lymphocytes predominantly produce IL-4 and IL-5 cytokine profile specific for Th2 immune response, while the memory L-selectin negative CD4+ T cells produce IFN-γ leading to Th1 response. Whether the reduced values of CD4+62L+ lymphocytes in participants with cumulative doses below 100 mSv express prevalence of Th1 response at low doses still remains an assumption due to incomplete research (haven’t distinguished memory and naive cells) but is an important issue for future studies.
The analysis of other adverse factors such as smoking showed an increase in the average CD4+62L− values and a reduction in CD4+62L+ cells (Table 6). This could contribute to the observed tendency assuming that the predominant respondents were smokers. Other studies 18,19 showed stress-induced changes in manifestation of CD62L adhesion molecules, suggesting that acute stress leads to increased CD62L− against CD62L+ on lymphocytes, while chronic stress changes them reciprocally—reduced CD62L—and increased CD62L+ lymphocytes. It cannot conclusively be said whether the observed increase in average CD4+62L+ cell subpopulation at cumulative doses above 100 mSv is determined by the chronic stress, including radiation impact or probably both mechanisms are involved.
CD4+25+ T Lymphocyte
Recently, a number of publications deal with the role of CD4+25+ T lymphocytes in the prevention of autoimmune, infectious, and inflammatory diseases. 20 –22 Since such phenotypic characteristics have both activated helper inducer and regulatory CD4+25+ lymphocytes (which are distinguished by the degree of expression of CD127 molecule), it is also necessary to determine greater accuracy for this receptor in further studies. It is known that ionizing radiation producing functional alteration of the immune system and breaking self-tolerance could cause autoimmune diseases. Sakaguchi et al 23 experimentally demonstrated that elimination of CD4+CD25+ T regulatory cells led to development of various organ-specific autoimmune diseases in mice.
By applying the Mann-Whitney U test, statistically significant decrease in CD4+25+ was found in the first group compared to control, followed by a tendency of gradual increase in the average percentage values to those of the control up to the fourth group (Figure 2). The comparison between the groups showed statistically significant difference in mean results between first and third groups (P = .006) and for the proportion of CD4+CD25+ population to all CD3+4+ T lymphocytes between first and fourth groups (P < .000; Table 4). The frequency analysis indicated the highest percentage of persons with elevated values for this parameter in the control group (33.8%) followed by third group (28.8%; Table 5). The results of our study are in agreement with data of Xu Y et al, 24 Lacoste-Collin et al, 9 and Liu SZ et al 25 for increased expression of IL-2 receptor on T lymphocytes in exposure to low doses. Similar data for increase in regulatory T-lymphocyte population was reported by Torkabadi et al 26 and Kusunoki et al 27 for angiography medical staff and people who survived atomic bombing, respectively. It is suggested that this is an indirect effect on the secretion of soluble factors from irradiated cells, which is interpreted as a manifestation of a protective mechanism.
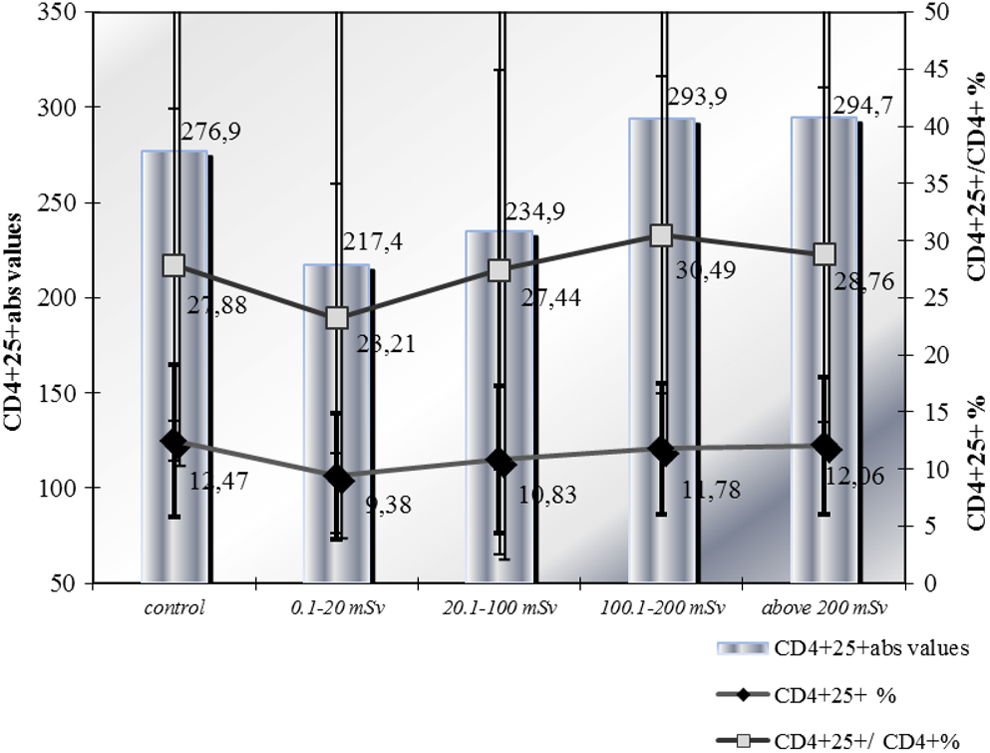
CD4+25+ T lymphocytes.
Relatively high incidence of people with cardiovascular disease and hypertension in both controls and in groups with higher cumulative dose and the role of this subpopulation in preventing and slowing the progression of atherosclerosis 28,29 probably reflects activation of the immune response due to subclinical inflammation in part of the respondents. 30,5 The observed significant, slightly positive correlation with age for this parameter and for its proportion to all CD3+4+ cells (r = .201 and r = .173, respectively) could be interpreted as a response of the organism to the upsurge in these processes. Cigarette smoking contributes to deviations in this index (P = .013; Table 6) suggesting that smoking might also influence the observed tendency.
In our previous study, 12 we observed slight increase in the average counts of CD8+ lymphocytes in groups exposed to lower cumulative doses, which could be explained by the finding of Bogdandi et al 31 that CD8+ and B cells are rather resistant to low doses such as occupational ones. There are also experimental data about enhancement of the function of macrophages and the response of CD8+ T cells at low-dose exposure. 32
For a more precise analysis, suppressor cytotoxic T lymphocytes used the marker CD28 + to distinguish CD28+ cytotoxic and CD28 suppressor subpopulations (Figure 3). Statistically significant decrease in the relative values of this parameter was found in the fourth group compared to control (P < .009) as well as in intergroup analysis (Mann-Whitney U test) between fourth and first (P < .000), fourth and second (P = .018) groups, respectively (Table 4).
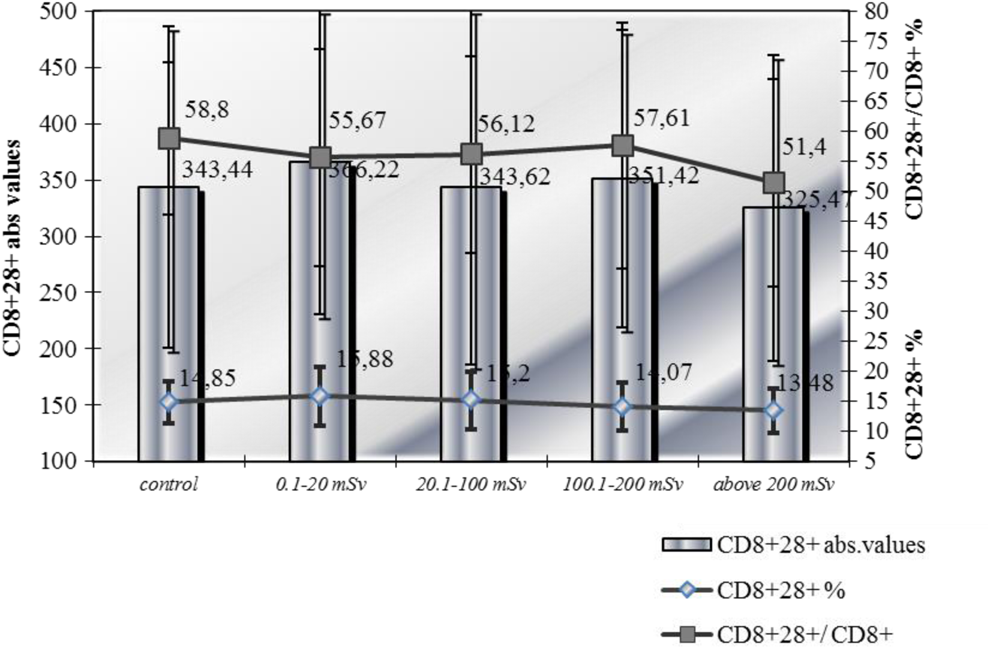
Cytotoxic T lymphocytes (CD8+28+).
A significant weak negative correlation of the values with the received dose (r = −.203 at P = .000) and the age (r = −.144 at P = .004) was found. A tendency of reducing the relative values of cytotoxic CD8+28+ T lymphocytes to total suppressor-cytotoxic T lymphocytes with increasing cumulative dose was observed which was confirmed by established negative correlation with dose (r = −.143 at P = .004).
More individuals with elevated parameters above the reference values were in the first (12.8%) and second groups (10.8%; Table 5).
In individuals consuming alcohol, the percentage of deviations for studied parameter was significantly higher (P = .019; Table 6). The observed increase in CD8+28+ T lymphocytes in the first 2 groups which are dominated by younger people who declared higher alcohol consumption could be in confirm of the impact of alcohol on the studied immune parameter. A marked downward trend was observed for cytotoxic CD8+28+ T subpopulation of CD3+8+ lymphocytes and upward tendency for their suppressor CD28+8− T lymphocytes with increase in cumulative dose. These results are supported by a study of Lui SZ et al 25 who considered that low doses could increase expression of CD28 and lead to immune stimulation while high doses lead to CTLA-4 expression and immunosuppression.
The prevalence of suppressor T lymphocytes in groups with higher cumulative dose could be associated with compensatory activation of regulatory suppressor mechanisms in response of the polarization to humoral-type immune response with increasing in dose.
Activated T lymphocytes (CD8+38+)
The results obtained for activated CD8+38+ subpopulation of T lymphocytes analyzed by Kruskal-Wallis test did not show statistically significant differences in the average values of exposed groups compared to controls. In intergroup analysis made by Mann-Whitney U test, a significant reduction in the relative values of the indices was recorded in third and fourth group compared to the first group (P = .047 and P = .001, respectively) and in fourth group compared to second one (P = .014; Table 4 and Figure 4).

Activated T lymphocytes (CD8+38+).
A significant weak positive correlation of the relative values of the parameter with received dose (r = .171 at P = .005) and a negative one of absolute values with the length of service (r = −.139 at P = .022) were observed.
The established increase in the activated CD8+38+ subpopulation in groups with lower cumulative doses and the gradual decrease with growth up of the dose could be connected with the reaction of the activated immune system to exogenous irritants of working environment based on adaptive processes occurring in the body.
Indicators of Humoral Immunity
Regardless of the absence of significant differences in the number of B lymphocytes between exposed and control groups found in our previous study, 12 the serum immunoglobulin was examined as an expression of their function. Normal distribution of results was found by Kolmogorov-Smirnov test for all 3 immunoglobulins, and Kruskal-Wallis test was applied for their analysis.
Immunoglobulin G
Although serum levels of immunoglobulin G did not show any statistically significant differences both between exposed groups and to control, there was some trend of increase in third group, after a drop to the control level in the first group, and in the fourth group again approaching the level of control (Table 7 and Figure 5). No correlation of the study parameter was found with the received dose, age, or length of service of the respondents but a slight, positive correlation was observed for the results of IgA (r = .187). The frequency analysis revealed more people with elevated levels of this immunoglobulin in third group (16. 9%) and in control (12.3%; Table 5).

Immunoglobulin G, A, and M.
Immunoglobulin G, A, and M.

Immunoglobulin A
The analysis of IgA with Mann-Whitney U test showed higher average values in all groups of professionally exposed persons compared to controls but statistically significant in third and fourth group (Table 7 and Figure 5).
Slight positive correlations of IgA with age and length of service were established (r = .150 and r = .126 at P = .000) as well as for IgG and IgM (r = .187 and r = .259, respectively). More of the individuals with elevated serum levels of IgA were observed in the first and third groups and in the control (Table 5).
Immunoglobulin M
The results for IgM was similar to that mentioned earlier—relatively higher average values compared to control in the first, second, and third groups and significant only in the first group (Table 7 and Figure 5). Frequency analysis confirmed the previous result of elevated levels of IgM observed in the first group (13.6%; Table 5).
It was found that alcohol consumption contributes to obtained deviations (P = .008; Table 6). Significantly weak negative correlation was established for IgM with the received dose (r = −0.112) and a positive one for immunoglobulin A (r = .259).
The analysis of IgG, IgA, and IgM indicating the functional activity of B cells showed a tendency for increasing their serum concentrations in persons with cumulative dose up to 200 mSv and reducing it at higher doses to values close to control. In interpretation of data on immunoglobulin concentrations, it should be noted that the effects of other adverse factors or harmful habits might cause similar changes. In our study, it was observed that alcohol drinkers frequently have elevated levels of IgM. Japanese authors 8,30,33,34 conducted a long-term study of atomic bomb survivors and also reported elevated IgM serum concentration due to compromising of the immune system that lead to some viral antigens reactivation or to the development of autoimmune processes. According to Kusunoki et al, 8 chronic effects of low radiation doses in the range 100 to 150 mSv result in prevalence of Th2 immune response causing many diseases characterized with increased immunoglobulin production. It is not excluded that this tendency reflects the adaptation of individuals to environment factors, but it could also be the expression of humoral-type prevalence at doses above 100 mSv. A slight positive correlation of IgA with age and length of service and weak negative correlation of IgM with cumulative doses differs from our previous studies and some reports 34 that observed a dose-dependent increase in these immunoglobulins.
On the other hand, Godekmerdan et al 2 found significantly lower levels of serum IgG, IgA, and IgM in professionally exposed individuals compared to control group. These discrepancies could be due to both the different number of respondents and the epidemiological situation, taking into account the relatively short half-life of immunoglobulins studied.
Conclusion
In this survey, no direct radiation-induced changes in the immune parameters of NPP workers occupationally exposed to low doses were established. Apart from the absence of significant deviations in the normal range for the studied parameters, the observed trends in some of them do not preclude any radiation effects. There is a tendency for changes in some of observed parameters at cumulative doses 100-200 mSv which remain or approximate control values at higher doses. Relatively more manifested tendencies are observed in CD3+4+ helper inducers cells and especially its CD4+62L+ subpopulation, activated/regulatory CD4+25+ cells, CD8+28+ cytotoxic subpopulation, and immunoglobulin M. Interpreting the observed trends of the studied parameters, it could be assumed that while the adaptation processes are dominated in low doses with low prevalence of Th1 immune response (increased CD8+, cytotoxic CD8+28+ and activated CD8+38+ lymphocytes) when increasing the dose above 100 to 200 mSv, the immune response shift to humoral type and compensatory mechanisms are involved to balance it (increased CD4+25+, CD4+62L+, and CD8+28− lymphocytes). Although such a hypothesis could explain some of the dependencies, its proof requires additional research including the cytokine profile of cellular populations. It is known that the balance between Type 1 and Type 2 cytokines changes with age. The Th1 immune response predominates in adults and Th2 in elderly population so that the shift from Th1 to Th2 cytokine profile could be an age-associated mechanism for immune dysfunctions. 35 The observed slight variations are hardly related only to radiation factor but to the impact of a number of other exogenous and endogenous factors on the immune system. In conclusion, it must be stressed that the significance of variations in the reference range is speculative and speak only of the existence of some trend of changes and as Fujiwara said, only 10% of them can be explained by the effect of low radiation doses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.