
Abstract
Background:
Carpal tunnel syndrome (CTS), the most common peripheral neuropathy, is currently diagnosed by clinical suspicion supported by tools such as the CTS-6 questionnaire and ultrasound. While these tools are widely used and clinically valuable, diagnostic accuracy may vary based on examiner experience and technique. This study introduces a pilot artificial intelligence (AI)-driven ultrasound pipeline using YOLOv11 for localization, U-Net for segmentation, and ConvNeXt for classification to support CTS diagnosis.
Methods:
In this observational cohort study, patients ≥18 years were screened for CTS from June 2023 to September 2024 by a board-certified hand surgeon using the CTS-6, and ultrasound images of the median nerve were obtained at the carpal tunnel inlet. One hundred twenty-one wrists (73 with CTS/48 without CTS) were used for model training and validation. The AI pipeline sequentially localized the median nerve (YOLOv11), segmented nerve boundaries (U-Net), and classified CTS status (ConvNeXt).
Results:
The ConvNeXt classification model achieved an accuracy of 94.1%, positive predictive value (PPV) of 0.86, and sensitivity of 1.0. The YOLOv11 localization model demonstrated PPV of 0.95 and sensitivity of 0.98. The U-Net segmentation model achieved a validation Intersection over Union (IoU) of 0.86.
Conclusions:
This pilot study demonstrates that an AI-assisted ultrasound pipeline can achieve strong diagnostic performance for CTS. Future work with larger, multi-center datasets and enhanced model interpretability is warranted prior to clinical deployment.
Introduction
Carpal tunnel syndrome (CTS) represents the most prevalent peripheral compression neuropathy, affecting approximately 3% to 6% of the general population, and up to 15% in high-risk occupational groups.1,2 Ultrasound imaging is increasingly used in CTS evaluation due to its noninvasive nature, affordability, and ability to visualize median nerve morphology at the carpal tunnel inlet. In a meta-analysis of 19 studies, median nerve cross-sectional area (CSA) demonstrated a sensitivity of 77.6% and specificity of 86.8%; however, the reported diagnostic threshold values varied widely, ranging from 9 to 15 mm2.2,3 Interoperator variability presents a limitation to the accuracy of ultrasound. In a small study evaluating untrained orthopedic residents and fellows, the accuracy of median nerve identification on ultrasound was only 36%, and just 62% of measurements were within 1 mm2 of the true CSA. 4 Training on carpal tunnel ultrasound measurements improves identification to 97% and measurement to 74%; however, given this wide range in reported accuracy, interoperator variability and subjective interpretation remain important limitations.5,6
The integration of artificial intelligence (AI) into medical imaging has revolutionized diagnostic approaches across multiple specialties, offering unprecedented opportunities for automated, objective, and reproducible image analysis. In the context of peripheral nerve imaging, AI applications have shown promise for enhancing diagnostic accuracy and reducing interobserver variability.7,8 Recent advances in deep learning models have provided robust solutions for each of these components. YOLOv11 (You Only Look Once version 11) represents the latest evolution in object-detection algorithms, offering superior accuracy and computational efficiency for medical image-localization tasks. 9 U-Net architecture has established itself as the gold standard for medical image segmentation, ideal in scenarios with limited training data typical of medical imaging studies.10,11 ConvNeXt, as a modernized convolutional neural network, has demonstrated high-level performance in medical image classification tasks while maintaining computational efficiency.12,13
The goal of this study was to develop and evaluate a pilot, fully automated AI pipeline that mirrors the clinical process of CTS diagnosis while remaining accessible to clinicians without specialized AI expertise. We integrate 3 state-of-the-art deep learning architectures, including YOLOv11 for rapid and precise localization, U-Net for high-accuracy segmentation, and ConvNeXt for robust classification, into a unified and fully automated diagnostic pipeline for ultrasound-based CTS assessment. This synergistic design capitalizes on each model’s strengths to overcome challenges inherent to medical imaging, such as small datasets, heterogeneous image quality, and the need for real-time analysis, with deployment potential on portable ultrasound devices for immediate clinical decision support. By integrating localization, segmentation, and classification into a single workflow, this approach aims to support standardized and reproducible CTS assessment using ultrasound images.
Methods
This pilot observational cohort study included patients of age 18 years or older presenting to a hand specialty clinic and screened for CTS from June 2023 to September 2024. Patients with and without symptoms of CTS were included. Patients were excluded if they had a previous history of carpal tunnel release surgery on the examined wrist. Baseline demographics were collected. To minimize bias, all patients were evaluated by a board-certified hand surgeon per the 2024 American Academy of Orthopaedic Surgeons guidelines with the use the CTS-6 as an objective reference standard. 14 Reflecting the guidelines’ most recent recommendation, electrophysiologic testing was not routinely performed, enabling evaluation of the AI system against real-world diagnostic workflows. The CTS-6 assesses numbness in the median nerve territory, nocturnal numbness, thenar atrophy, Phalen’s test, Tinel sign, and 2-point discrimination to obtain a score out of 26 points, with a positive result defined as a score of ≥12. Ultrasound images of the median nerve were obtained at the carpal tunnel inlet and stored for analysis. Wrists with and without CTS diagnosis were used to train and test the system. Seventy-five percent of the images were used to train the system, and 25% of the images were reserved for testing the system.
While no formal power calculation was performed due to the exploratory nature of this AI model–development study, we followed established recommendations for medical imaging studies, aiming for a minimum of 100 cases to balance model training complexity with dataset diversity. The 121-wrist dataset was deemed sufficient to train, validate, and assess the feasibility of the model while avoiding overfitting. All models were trained using a conservative learning rate and Adam optimization. Demographic data were summarized using mean and standard deviation, while model performance was evaluated using precision, recall, and Intersection over Union (IoU).
A schematic overview of the training process is provided in Figure 1. The AI system first identifies the median nerve using the YOLOv11 model, an advanced real-time object-detection architecture optimized for high precision in small anatomical structures within ultrasound images. YOLOv11 was trained to localize the nerve at the carpal tunnel inlet by generating bounding boxes that tightly encompass the nerve, even in cases with suboptimal image quality or anatomical variability. Once localized, the cropped region containing the median nerve was passed to a U-Net segmentation model, which performed pixel-level delineation of the nerve’s contour. U-Net’s encoder-decoder structure, with skip connections, preserved fine spatial details critical for accurate CSA computation. The segmented nerve mask was then used as the primary input to a ConvNeXt classification model, which extracted high-level morphological and textural features to determine whether the image was consistent with CTS. Rather than relying on predefined measurements or thresholds, ConvNeXt utilizes convolutional filters trained end-to-end to identify patterns directly from the image data. These features include global and local shape characteristics (e.g., nerve enlargement, boundary irregularity, and degree of flattening), internal echotexture (e.g., hypoechogenicity and heterogeneity), and edge sharpness at the nerve-surrounding tissue interface, all of which have been associated with CTS in prior ultrasound studies. Through supervised learning with gold-standard labeled CTS-positive and CTS-negative examples, the computational model optimizes its parameters to emphasize image regions and feature combinations that most strongly contribute to accurate classification. Altogether, this sequential, modular design allowed each network to specialize in its respective task, including localization, segmentation, and classification, while reducing error propagation and improving interpretability.
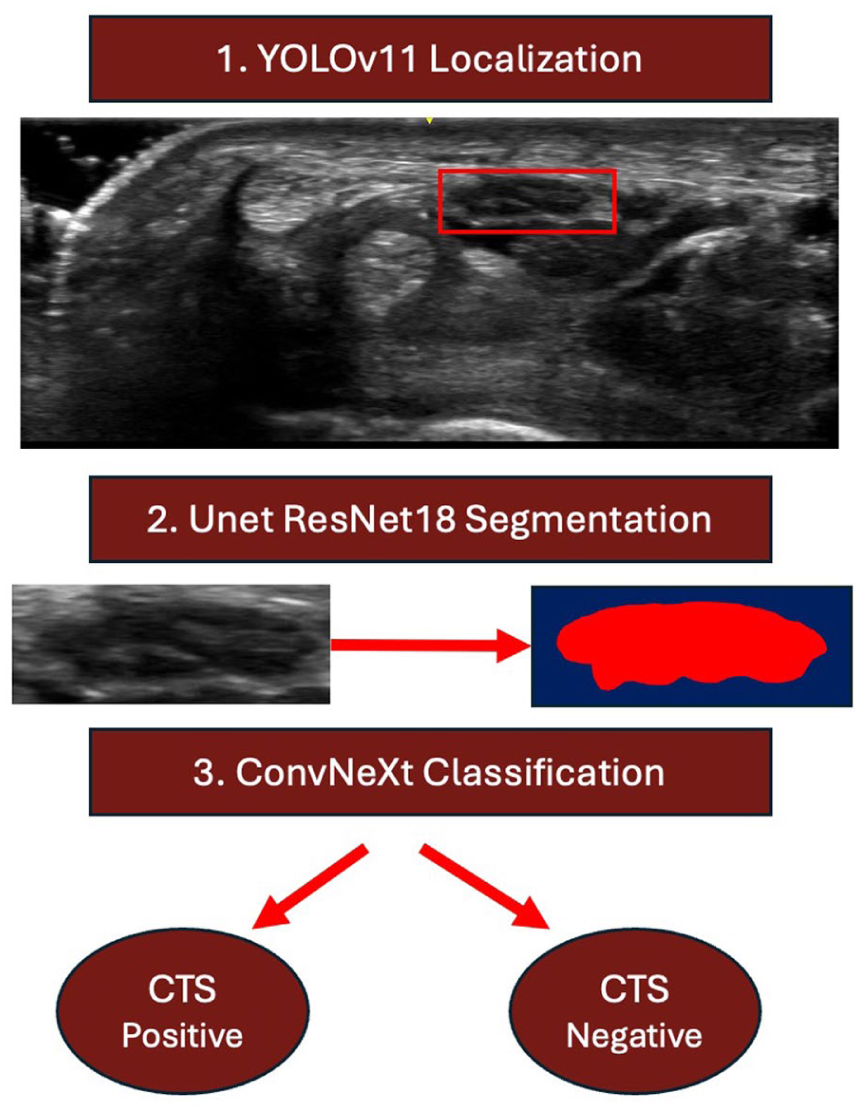
The deep learning pipeline for carpal tunnel classification first utilized YOLOV11 to identify the median nerve, then outlined its shape with U-Net, and finally implemented ConvNeXt to identify carpal tunnel syndrome diagnosis.
Results
Images from 121 wrists (73 with CTS/48 without CTS) were obtained. Eighty wrists belonged to female-identifying patients, and 41 belonged to male-identifying patients. The average age was 58.2 years (SD 15.66 years). The average manually measured median nerve CSA was 12.99 ± 3.81 mm2 in CTS-positive patients, and 9.49 ± 2.99 mm2 in CTS-negative patients. The images were split into 92 training and 29 validation samples.
The YOLOv11 system accurately located areas of interest in the images with an average precision of 0.99 at an IoU threshold of 50. It had a positive predictive value (PPV) of 0.949 and a sensitivity of 0.984. The U-Net segmentation model achieved a validation IoU of 0.86. The ConvNeXt classification model demonstrated an accuracy of 94.12%, with sensitivity of 1.0 and a PPV of 0.86.
Discussion
This pilot study demonstrates the feasibility of an AI-assisted ultrasound pipeline for CTS diagnosis that integrates localization, segmentation, and classification into a single automated workflow. Unlike conventional ultrasound assessment, which is highly operator-dependent, this approach offers standardized image interpretation that may be particularly valuable for clinicians with varying levels of ultrasound experience. Ultrasound image collection can be performed in office, without requiring additional office visits or invasive testing as per electromyography (EMG).
The methodology of this study leveraged a 3-tiered AI pipeline: localization with YOLOv11, segmentation with U-Net, and classification with ConvNeXt. This modular design mirrors the clinical workflow for image-guided diagnosis of a disease. Importantly, the dataset incorporated both CTS-positive and CTS-negative patients, including asymptomatic individuals, thereby providing the model with clinically relevant heterogeneity.
The pattern of average CSA between CTS-positive and CTS-negative groups correlated with prior literature which generally references a cutoff of 10 or 11 mm2 in diagnosis of CTS, though standardized cutoff values have yet to be established.14-16 AI classification likely incorporated additional image features beyond size alone, including nerve shape, echotexture, and boundary definition. These findings suggest that AI models may capture subtle imaging characteristics not readily quantified by human observers. Future work incorporating explainable AI methods may help clarify which features most strongly influence classification decisions.
These findings resonate with broader trends identified in a recent scoping review of AI applications in ultrasound for CTS: deep learning techniques—including Convolutional Neural Networks and emerging transformer‑based architectures—have demonstrated strong performance in median nerve segmentation, CSA measurement, diagnostic classification, and severity grading. 8 Our study particularly stands out in its combination of median nerve identification, segmentation, and accurate prediction of CTS diagnosis with high precision and recall. Machine learning technology has also demonstrated significant improvements in diagnostic accuracy in quantitative analysis of thenar muscle atrophy ultrasound images in CTS. 17 Beyond CTS, AI has been effectively employed in other peripheral neuropathies, including cubital tunnel syndrome (CuTS). For example, Shinohara et al 18 used a deep learning model to predict CuTS on ultrasound images with an accuracy of 0.90, precision of 0.86, and a recall of 1.00.
Limitations include the modest dataset size, reliance on a single clinical evaluator, and absence of electrophysiologic confirmation. Accordingly, these results should be interpreted as preliminary. Larger, multi-center studies with multiple expert raters and complementary diagnostic standards are needed.
Conclusion
This pilot study supports the potential role of AI-assisted ultrasound analysis as a diagnostic support tool for CTS. The proposed pipeline demonstrated high accuracy, sensitivity, and precision while aligning with clinical workflows. With further validation, integration of explainable AI, and expansion across diverse clinical settings, this approach may enhance the accessibility, consistency, and efficiency of CTS diagnosis.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Christopher Gonzalez, Dr. Fritz Steuer, and Dr. Stephen Canton for their invaluable assistance in coordinating various aspects of this project. Their support and dedication played a significant role in ensuring the successful execution of the research.
Ethical Considerations
This study was approved by our institutional review board.
Author Contributions
All authors have made substantial contributions to the conception, design, collection of data, and drafting of the work; have approved the final version; and agree to be accountable for the results.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was supplied by the UPMC Bethel Musculoskeletal Research Center.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JRF is a consultant for Sonex Health, LLC; however, this relationship has no conflict with this manuscript.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.