
Abstract
Background:
Specialists recognize discordance between levels of discomfort and incapability and pathophysiology severity among people presenting for care of compressive median neuropathy at the carpal tunnel, but there is limited evidence regarding factors associated with this discordance. Using statistical techniques to identify subgroups of mental health factors and pathophysiology factors among people presenting for care of compressive median neuropathy at the carpal tunnel can help determine their relative association with levels of discomfort and incapability. We therefore asked: (1) Can we identify statistical groupings of mental health and pathophysiological factors among people with compressive median neuropathy at the carpal tunnel? and (2) Is there a difference in pain intensity and magnitude of capability among the identified statical groupings?
Methods:
We performed a secondary analysis of 150 patients using a k-means clustering algorithm to identify statistical subgroups based on symptoms of distress, levels of fear of painful movement, and categorized pathophysiology severity (mild, moderate, or severe) on electrodiagnostic testing by the physician performing the test. We compared the relative levels of pain intensity and magnitude of incapability between the identified statistical groupings.
Results:
There were 4 distinct statistical groupings defined by varying levels of fear of painful movement and feelings of distress (anxiety or depression) regarding sensations with minimal variation in mean neuropathy severity. Groupings with greater distress and fear of painful movement had greater mean pain intensity and magnitude of incapability.
Conclusion:
The evidence that discordance between symptom intensity and compressive median neuropathy severity is accounted for by less healthy mindsets directs clinicians to use relatively notable levels of pain intensity and incapability as a signal to prioritize timely and accurate diagnosis of less healthy mindsets (misconceptions and distress) as a safeguard for comprehensive care.
Introduction
Unhelpful thoughts about sensations and feelings of worry and despair (grouped together by psychologists as distress) account for a substantial part of the variation in levels of discomfort and incapability as quantified using patient-reported outcome measures (PROMs).1-4 Prior studies identified statistical groupings of patients with increasing levels of unhelpful thinking and feelings of distress that correlate with increasing mean levels of incapability.5,6 The strength and consistency of the association of mental and social health with symptom intensity supports comprehensive care strategies tailored to a patient’s specific mental, social, and physiological status.5,6 For example, one study used latent class analysis to identify statistical groupings of distress and unhelpful thoughts regarding symptoms among people undergoing nonoperative care for hip or knee osteoarthritis, finding higher levels of discomfort and incapability in groupings with higher levels of distress. 7 And a cluster analysis of measures of levels of symptoms of anxiety and depression and levels of unhelpful thinking regarding symptoms (kinesiophobia and negative pain thoughts) among patients with upper-extremity illness found that groups of patients with lower amounts of distress and unhelpful thoughts had significantly less incapability and lower pain intensity. 8
Experiments using PROMs often demonstrate that the severity of pathophysiology—radiographic severity of osteoarthritis of the knee or trapeziometacarpal articulations,9,10 and rotator cuff tendinopathy, 11 for instance—has more limited association with levels of discomfort and incapability than one might intuitively expect. As a next step in understanding the relative association of levels of discomfort and incapability with levels of pathophysiology severity relative to levels of distress and unhelpful thinking regarding sensations, we propose including pathophysiology severity in the identification of statistical clusters. In the context of knee osteoarthritis, this approach yielded 6 statistical groupings based on mean Kellgren-Lawrence (KL) grade of osteoarthritis and mean levels of mental health, and lower mean levels of capability and self-efficacy were tied largely to variations in mental health with relatively less variation according to pathophysiology severity. 12
Compressive median neuropathy at the carpal tunnel (the symptoms and signs of which are carpal tunnel syndrome [CTS]) represents another opportunity to test cluster analysis with combinations of fear of painful movement (unhelpful thoughts), feelings of worry or despair, and measures of pathophysiology severity (electrodiagnostic test results). To date, levels of incapability have limited correlation with electrophysiological severity in people with compressive median neuropathy at the carpal tunnel.13,14 For instance, among 70 patients with electrodiagnostically confirmed median neuropathy presenting to a hand surgery specialist, there was no correlation between electrophysiological severity and levels of incapability measured using the Quick Disabilities of Arm, Shoulder, and Hand (QuickDASH), and more than a third of the variation in incapability was accounted for by unhelpful thinking and feelings of worry or despair. 15 As an example of the importance of mental health among people with CTS, a study of 60 patients found that greater symptoms of depression and pain anxiety were associated with greater carpal tunnel symptom intensity measured using the Boston Carpal Tunnel Questionnaire both before and after surgery. 16
A next step would be to identify statistical groupings of both mental health and median neuropathy severity in patients with CTS and determine whether both factors contribute to distinct levels of increasing magnitude of incapability. We therefore asked: (1) Can we identify statistical groupings of mental health and pathophysiological factors among people with compressive median neuropathy at the carpal tunnel? and (2) Is there a difference in pain intensity and magnitude of capability among the identified statical groupings?
Methods
Study Design and Setting
We performed a secondary analysis of data from a prior study of English-speaking new and return hand surgery specialty care patients, age 18 to 89 years old, diagnosed with compressive median neuropathy at the carpal tunnel confirmed on electrodiagnostic testing. Demographics included sex, level of education, marital status, insurance provider, type of visit, and age. This article was written according to the Strengthening the Reporting of Observational Studies in Epidemiology checklist for cross-sectional studies.
Participants
There were a total of 150 patients diagnosed with CTS who had electrodiagnostic tests with a severity rating assigned by the clinician who performed the study. Sixty-four percent (96 of 150) were women. The mean age was 56 ± 14 years (Table 1).
Patient Demographics and Clinical Characteristics (N = 150).
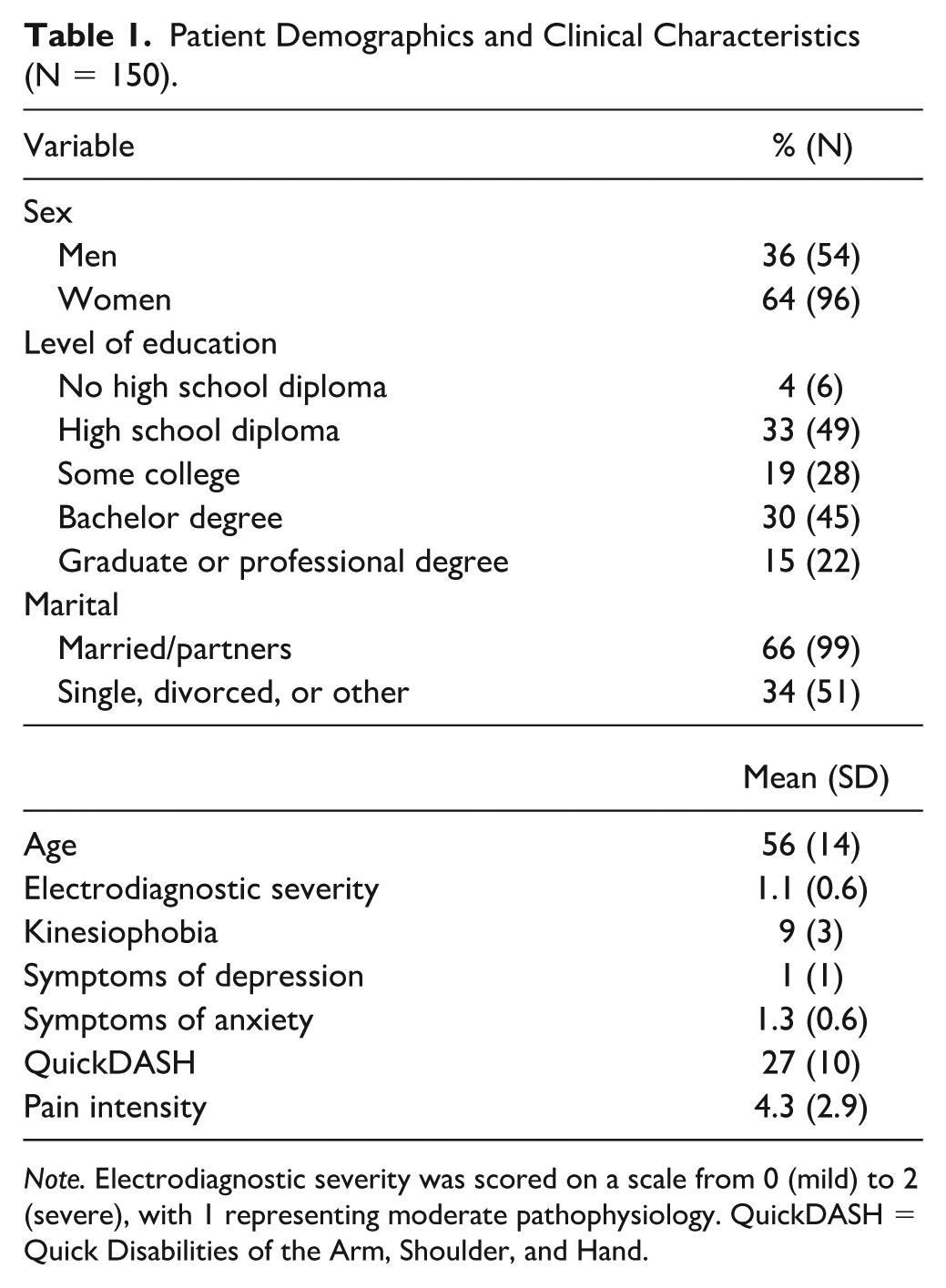
Note. Electrodiagnostic severity was scored on a scale from 0 (mild) to 2 (severe), with 1 representing moderate pathophysiology. QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand.
Primary Outcome Measures
Upper-extremity-specific level of capability was measured using the QuickDASH questionnaire. 17 Scores on the QuickDASH range from 0, representing no symptoms or incapability, to 100, representing maximum symptom intensity and incapability. Pain intensity was measured using an 11-point ordinal scale (Numerical Rating Scale) from 0 representing no pain to 10 representing the worst pain imaginable. 18
Mental Health Measures
We measured fear of painful movement using the 4-item version of the Tampa Scale for Kinesiophobia. Each item was rated on a 4-point Likert scale, resulting in a scale between 0 and 16, with higher scores indicating greater fear of painful movement. 19
Levels of symptoms of anxiety and depression (often grouped by psychologists as symptoms of distress) were quantified using 2 measures. Symptoms of depression in the last 2 weeks were quantified using the 2-item version of the Patient Health Questionnaire, resulting in a score from 0 to 8, with higher levels indicating greater symptoms of depression. We also used 1 item from the EQ-5D-3L (EuroQol-5 Dimensions-3 Level) that has 3 possible degrees of anxiety/depression: I am not anxious or depressed; I am moderately anxious or depressed; and I am extremely anxious or depressed.
Pathophysiology Measurement
Median neuropathy severity was quantified as mild (0), moderate (1), or severe (2) based on categorization of electrodiagnostic findings as applied by the clinician performing and interpreting the test. Median neuropathy severity was measured preoperative for all patients. Because specific measurements of the test can be variably interpreted by surgeons and to reflect daily practice as accurately as possible, we used the interpretation of the clinician performing the test. In the clusters, a mean of 1 (moderate pathophysiology severity—typical of most published series of carpal tunnel releases) was labeled as average.
Ethical Approval
We obtained institutional review board approval for this cross-sectional study.
Statistical Analysis
A k-means clustering algorithm was fit to the data, allowing up to 20 unique clusters of symptoms of distress (depression and anxiety), levels of fear of painful movement (kinesiophobia), and median neuropathy severity on electrodiagnostic testing. Using the elbow method, the 4-cluster model was determined to be the best fitting model (Figure 1). Z-scores represent the central tendency of the group, relative to the entire population where a positive z-score indicates a higher average than the population. We used the Kruskal-Wallis test with Dunn post hoc pairwise comparison to study associations of each cluster with the QuickDASH score and Numeric Rating Scale for pain.
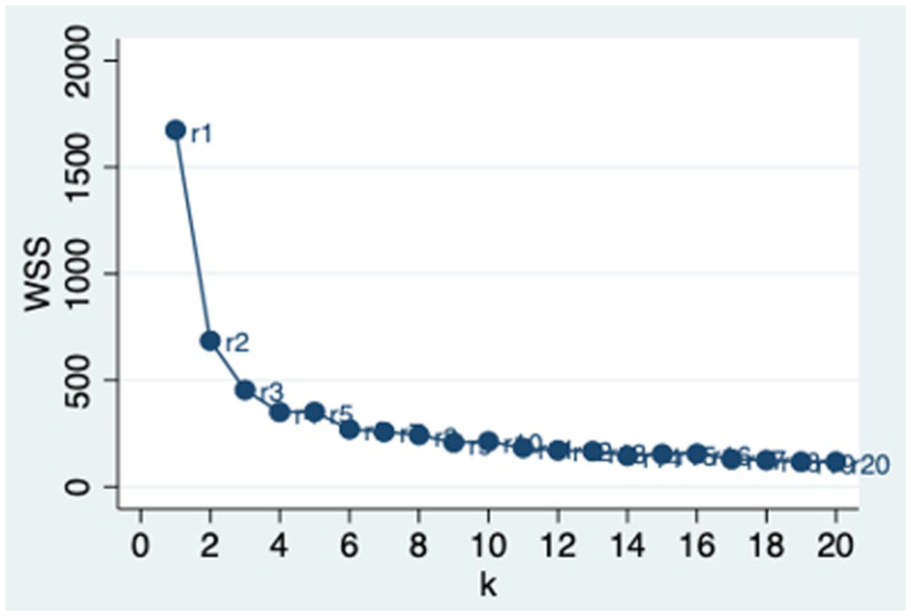
WCSS plotted against the number of clusters (k). The optimal k is indicated by the elbow point where further increases yield diminishing returns.
Results
Statistical Groupings of Mental Health and Pathophysiology Factors
Cluster analysis identified 4 distinct statistical groupings of measures of fear of painful movement (unhelpful thoughts), symptoms of distress, and median neuropathy severity (Table 2). Group 1 was characterized by low distress, low unhelpful thoughts, and average median neuropathy (Table 2). Group 2 had average distress, low unhelpful thoughts, and average median neuropathy. Group 3 had higher distress, low unhelpful thoughts, and average median neuropathy. Group 4 had severe distress, severe unhelpful thoughts, and slightly worse median neuropathy. The median neuropathy severity in group 4 was considered “slightly worse” neuropathy due to a slightly higher z-score compared with the first 3 statistical subgroups (Table 2).
Characteristics of Mental Health and Median Neuropathy Clusters of 150 Patients With Carpal Tunnel Syndrome.
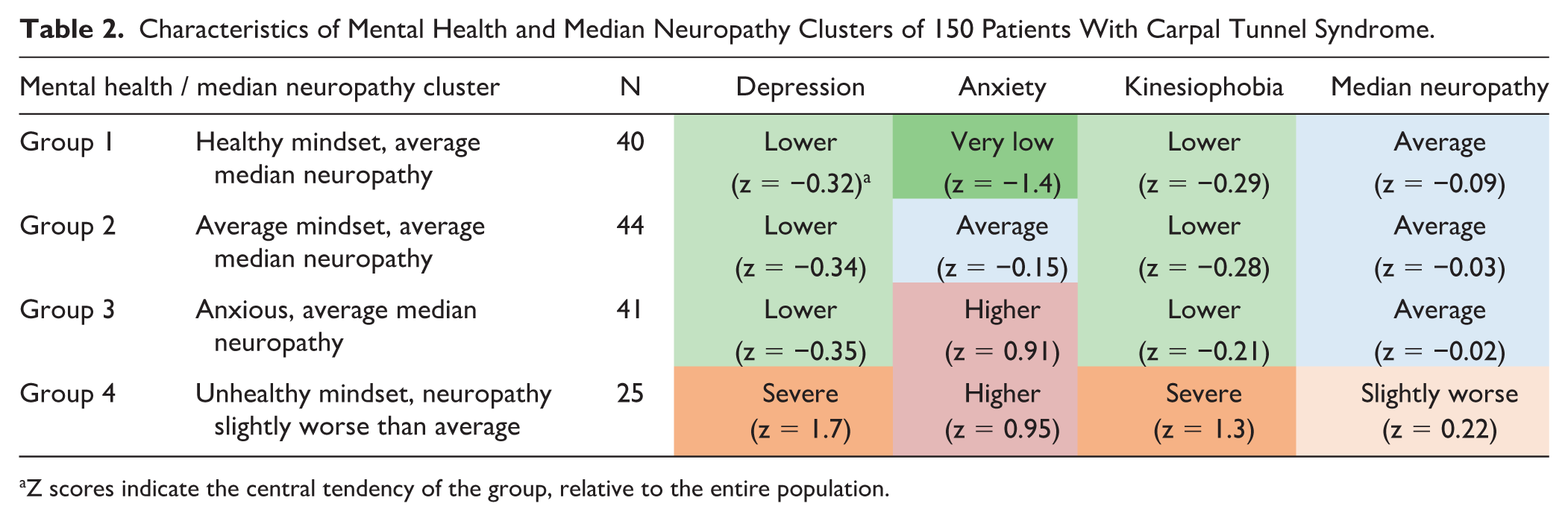
Z scores indicate the central tendency of the group, relative to the entire population.
Differences in Levels of Discomfort and Incapability by Statistical Grouping
Pain intensity was significantly higher in group 4 (unhealthy mindset, slightly worse median neuropathy; pain intensity 6.0 ± 2.6) compared with both group 1 (healthy mindset, average pathophysiology; pain intensity 2.9 ± 2.7) and group 2 (average mindset, average median neuropathy; pain intensity 4.2 ± 2.8; Table 3). Pain intensity was also significantly higher in group 3 (anxious, average median neuropathy; pain intensity 4.8 ± 2.6) compared with group 1.
Statistical Groupings of Mental Health/Median Neuropathy and Corresponding Levels of Discomfort and Incapability.

Note. Clusters with less healthy mindsets have greater levels of discomfort (pain intensity) and incapability, relatively independent of median neuropathy severity. Level of incapability was measured using Quick Disabilities of Arm, Shoulder, and Hand questionnaire; pain intensity was measured using the Numeric Rating Scale from 0, no pain, to 10, the worst imaginable pain.
The magnitude of incapability (QuickDASH) was significantly higher in group 4 (QuickDASH: 62 ± 20) compared with both group 1 (41 ± 18) and group 2 (47 ± 15; Table 3). Magnitude of incapability was also significantly higher in group 3 (54 ± 18) compared with group 1 (41 ± 18; Table 3).
Discussions
The known discordance of symptom intensity from pathophysiology severity might be accounted for by variations in mental and social health. If so, comprehensive care strategies could use such discordance to assist with timely and accurate diagnosis and treatment of the psychosocial aspects of the illness. The discordance of knee osteoarthritis severity and symptom severity is accounted for by levels of unhelpful thinking and symptoms of distress with surprisingly limited association of symptom intensity with radiographic osteoarthritis severity.9,12,20 In this study of patients with symptoms from compressive median neuropathy at the carpal tunnel (CTS), the 4 identified statistical groupings of fear of painful movement (unhelpful thoughts) symptoms of distress, and neuropathology severity associated with greater levels of discomfort incapability and were determined primarily by differences in mental health with little or no variation in median neuropathy severity.
Limitations
There are several limitations to this study. First, previous studies found that some patients answer questionnaires regarding symptoms of distress hastily and not forthrightly with notable floor effects.21,22 Nevertheless, studies using these instruments identify important associations. We also had relatively limited measures of mental health consisting of just 3 items. Readers should consider that a study with more mental health items, forthrightly completed might show even stronger associations of mental health factors with measures of symptom intensity and magnitude of incapability. Second, expert input is needed to inform the construction and interpretation of the statistical models. For example, judgment plays a role when selecting the number and size of each phenotype and creating categories within mental health measures. In this study, for example, we classified group 4 as “slightly worse pathophysiology” in relation to the other groups. However, the z-score is only 0.22, meaning that this group of patients is only 0.22 standard deviations above the mean of the entire study population, which might be considered average pathophysiology. Studies that use cluster analysis might benefit from setting thresholds for describing relative values for each category in advance to limit bias. Third, the interobserver reliability for electrophysiology-based categorical severity ratings of median neuropathy can be limited, introducing another area of potential variation or subjectivity. However, severe pathophysiology is relatively easily rated and should provide adequate discernment. We relied on the categorical severity rating of the physician who performed the study, which reflects daily practice. Fourth, some might wonder if using QuickDASH for measurement of levels of capability rather than a nerve or hand-specific measure can affect the results. We think not, given the evidence that disease, anatomy, and region-specific PROMs give similar results. 23
Statistical Groupings of Mental Health and Pathophysiological Factors
The finding of 4 different statistical groupings of symptoms of distress, fear of painful movement (unhelpful thoughts), and median neuropathy severity among patients, with relatively little variation in neuropathy severity, adds further evidence that what differentiates people with musculoskeletal illness with a discordance between pathophysiology severity and symptom intensity, is partly the degree of pathophysiology they have developed, but mostly their thoughts and feelings about their body’s sensations. These results align with recent studies that found hip and knee osteoarthritis severity had limited variation in the statistical groupings compared with mental health factors9,12,24 and a study of compressive median neuropathy at the carpal tunnel that found limited association of symptom intensity with pathophysiology severity. 15 Musculoskeletal specialists tend to assume or intuit a direct correspondence between symptom intensity and level of incapability and pathophysiology. This cognitive bias is faulty, and musculoskeletal specialists need to anticipate the discordance between symptoms and pathophysiology and the mindsets that are associated with this discordance.
Differences in Magnitude of Incapability and Pain Intensity Within Statistical Groupings
The finding that statistical groupings of greater fear of painful movement (unhelpful thoughts) and feelings of distress are associated with greater levels of discomfort and incapability emphasizes the importance of mental health to overall musculoskeletal health. 25 These findings address people with sufficient concerns about symptoms to seek care. Population-based data suggest that symptoms of depression and levels of pathophysiology severity may have comparable association with magnitude of capability, particularly at moderate levels of pathophysiology severity. 26 For instance, Kim et al 26 studying people aged 65 and older in a Korean town as part of a study of the elderly found that a threshold level of symptoms of knee osteoarthritis was associated comparably with a threshold level of symptoms of depression (odds ratio: 5.9) and with levels of pathophysiology severity (odds ratio of 2.6 for KL grades 2 or 3; odds ratio of 7.2 for KL grade 4). It is possible that mental health factors may have relatively greater association with incapability among people who seek musculoskeletal specialty care, and therefore future studies might focus on studying these associations and maybe even the effects of intervention in population-based cohorts.
Conclusions
In a study of people with CTS, we found that statistical groupings of patients that are associated with greater levels of symptom intensity are determined more by thoughts and feelings than median neuropathy severity. The discordance between pathophysiology severity and symptom severity is consistent in prior evidence and places emphasis on the importance of treatment strategies based in the biopsychosocial paradigm of human illness. Specifically, musculoskeletal specialists can be mindful that greater levels of discomfort and incapability tend to represent worse mental health rather than greater severity of pathophysiology. Unexpected levels of discomfort and incapability can contribute to timely and accurate diagnosis of feelings of distress and unhelpful thoughts (misconceptions) regarding the body and its sensations and support comprehensive, whole-person care strategies.
Footnotes
Authors’ Note
This work was performed at the University of Texas at Austin, Texas, USA.
Ethical Approval
Ethical approval to report this case/these cases was obtained from the office of research support and compliance, The University of Texas at Austin.
Statement of Human and Animal Rights
This study complied with all ethical standards.
Statement of Informed Consent
Since this study performed a secondary analysis of existing data, no ethical committee approval regarding obtaining informed consent was needed for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.