
Abstract
Background:
The scratch-collapse test (SCT) is a provocative maneuver used to diagnose compressive neuropathies. Despite multiple studies supporting its use, the SCT remains a controversial point in the literature in regard to its exact clinical application. We performed a systematic review and statistical analysis to provide statistical data on SCT outcomes and elucidate its role in diagnosing compressive conditions.
Methods:
We performed a systematic review of the literature according to Preferred Reporting for Systematic Reviews and Meta-Analyses guidelines. We extracted data of patients with outcomes on the SCT (yes/no) and on an accepted gold standard examination (electrodiagnostic studies). These data were analyzed using a statistical software program to generate the sensitivity and specificity values of the pooled data, as well as kappa agreement statistics.
Results:
For patients with carpal tunnel, cubital tunnel, peroneal, and pronator compressive neuropathies, the overall sensitivity of the SCT was 38%, and the specificity was 94%, with the kappa statistic approximately 0.4. Sensitivity and specificity values were higher for cubital tunnel syndrome and peroneal compression syndrome but lower for carpal tunnel syndrome. Pronator syndrome was also examined, but the data were inadequate for analysis.
Conclusions:
The SCT is a useful adjunct in the armament of diagnostic tools for the hand surgeon. Given its low sensitivity and high specificity, SCT should be used as a confirmatory test, rather than as a diagnostic screening test. More analyses are needed to identify subtler applications.
Introduction
Nerve entrapment is a common condition managed by hand surgeons. However, compressive neuropathies are multifactorial in origin, with widely varied histories and presentations that complicate the diagnosis.1 -5 Anatomic variations in nerve distributions and multiple compression points in each region of potential nerve entrapment can make it difficult to select an appropriate diagnosis and treatment paradigm.6,7
Given this, accurate physical examination maneuvers and diagnostic testing are critical for the management of these patients. Physical examination maneuvers include evaluation of sensation and motor functions, as well as provocative tests like the Tinel sign and Phalen test in carpal tunnel syndrome (CTS).
Despite these techniques, diagnostic uncertainty often remains, resulting in the need for electrodiagnostic studies such as electromyography and nerve conduction studies. These are considered the “gold standard” test for compressive neuropathies and nerve entrapment syndromes.8,9 However, these studies, especially electromyography, are often unreliable because factors such as height and age make it difficult to accurately map nerve and muscle potentials with needle placement. Furthermore, these studies fall short in analyzing complex injury patterns such as double crush syndrome or uncommon injury patterns.10 -12
To combat this, Cheng et al, inspired by Bronson and Beck, published the scratch-collapse test (SCT) in 2008 for the diagnosis of carpal and cubital tunnel syndrome (CuTS). 13 This is a provocative maneuver that depends on the theoretical partial inhibition of all voluntary muscle activities that occur after stimulation of skin at the location of nerve injury. In the SCT, the “silent period” is induced by the examiner at the potential location of nerve injury (the “scratch”). External rotation of the shoulder or hip is then immediately tested. Weakness in external rotation (the “collapse”) is indicative of a positive test and a nerve injury (Figure 1). This test is purported to be more accurate than others in diagnosing subtle nerve injuries.
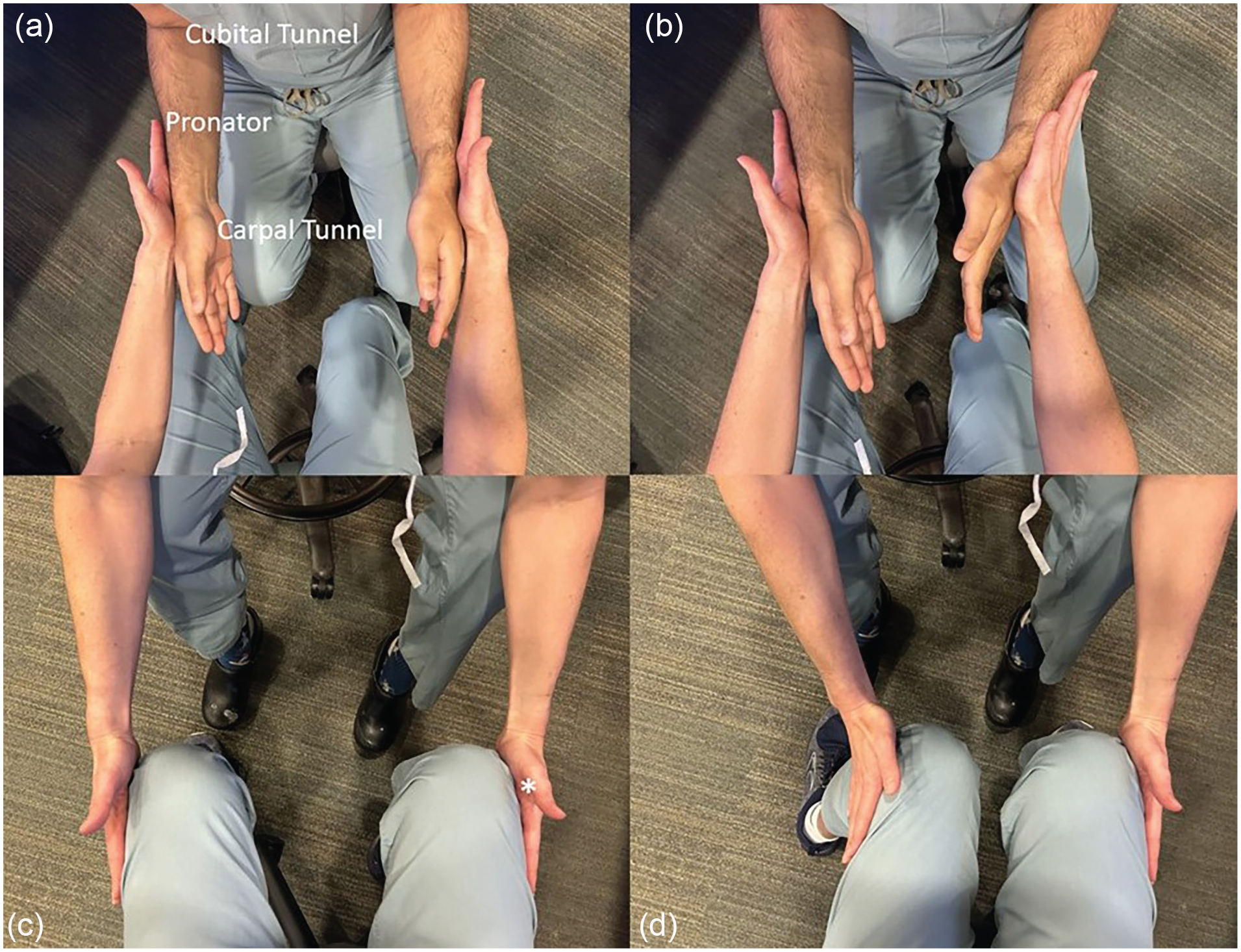
(a) and (b) Demonstration of the scratch-collapse test for the upper extremity. Compression points tested are labeled on (a). (c) and (d) Demonstration of the scratch-collapse test for the lower extremity. Location of scratch for common peroneal syndrome is marked with an asterisk.
However, the SCT remains controversial among nerve surgeons, as outcomes in the literature draw a wide range of conclusions. 14 We performed a systematic review and statistical analysis to determine the utility of this test in various compression neuropathies to help guide surgeons in their examination and interpretation of complex patients.
Methods
Literature Search
A systematic review was performed following the Preferred Reporting for Systematic Reviews and Meta-Analyses statement guidelines (Figure 2). The search was performed using PubMed/MEDLINE, EMBASE, ScienceDirect, and Cochrane Library with the Boolean search string: scratch-collapse test. The Boolean string was adapted for each database according to their specific conditions. Inclusion and exclusion criteria were determined before the review was conducted. Screening criteria excluded nonjournal articles, nonsurgical studies, and articles written in languages other than English without translation. A full-text review excluded any articles without any discussion of SCT or outcomes reporting. The process of article selection was repeated by 2 independent reviewers to ensure transparency and consistency, and the senior author served as the judge. Any disagreement was resolved by a third reviewer. The search was performed again toward the end of the review to ensure consistent results from the search string and selection criteria.
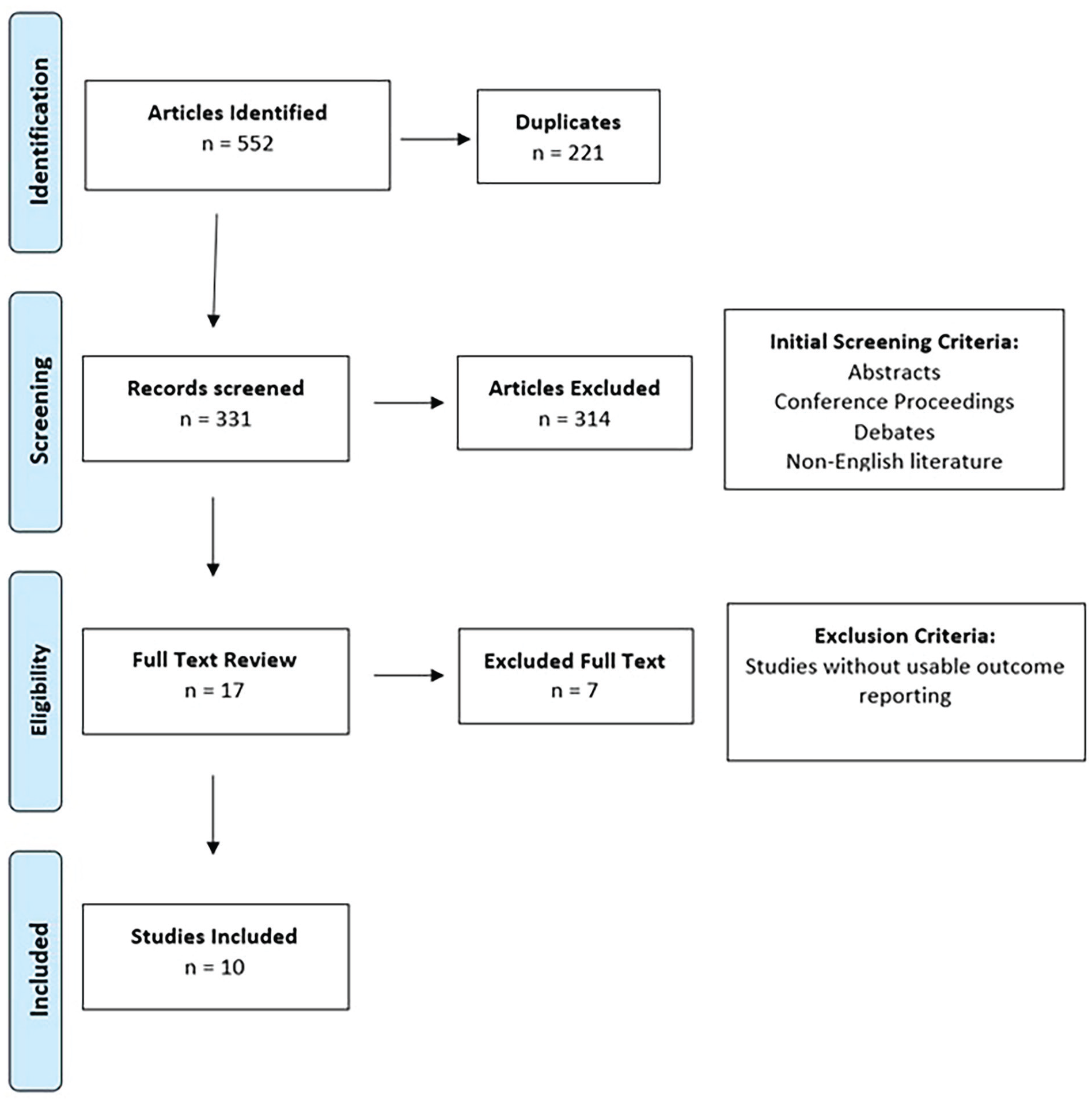
PRISMA flowchart of search parameters used.
Data Extraction
After articles were selected, relevant patient data were extracted. Inclusion criteria were patients with binary data points for the SCT and numerical outcomes on an established gold standard examination as a control. The exact compression point being analyzed was noted but not used as an exclusionary criterion. A separate data set was entered for the pooled analysis each time a test was applied to the set of patients in each article. Bilateral extremities were counted as 2 patients for the purpose of this study.
Statistical Analysis
After patient extraction and classification, sensitivity and specificity were calculated for the pooled data. Kappa values were calculated, and the Fisher Exact test was used to compare sensitivity and specificity values across pooled data. Data analyses were done in SPSS (IBM, Armonk, New York). Meta-analyses were considered but not performed; individual articles did not provide adequate statistical analysis for a meta-analysis. Data from the included articles varied in detail and could not be used to perform a specific analysis.
Results
Literature Search and Demographic Data
Our literature search yielded 552 articles, 10 of which met inclusion criteria (Table 1).13,15 -23 These articles provided 2279 extremities for analysis. Demographically, 1125 extremities (49.3%) were female, with an average age of 52.1 years. A total of 1377 patients were evaluated for CTS, 788 patients for CuTS, 96 patients for peroneal compression, and 18 patients for pronator syndrome. Electrodiagnostic test (EDX) confirmation of neuropathy was used as the “gold standard” for diagnosis. Ultimately, 1064 patients were diagnosed with neuropathy by EDX. Of the patients with possible CTS, 774 (56%) had electrodiagnostic confirmation of the disease. Two hundred forty-six patients (31%) had CuTS confirmed by electrodiagnostic studies, 26 patients (27%) had peroneal compression, and 18 patients had pronator syndrome. These data are summarized in Table 2.
Articles Analyzed.
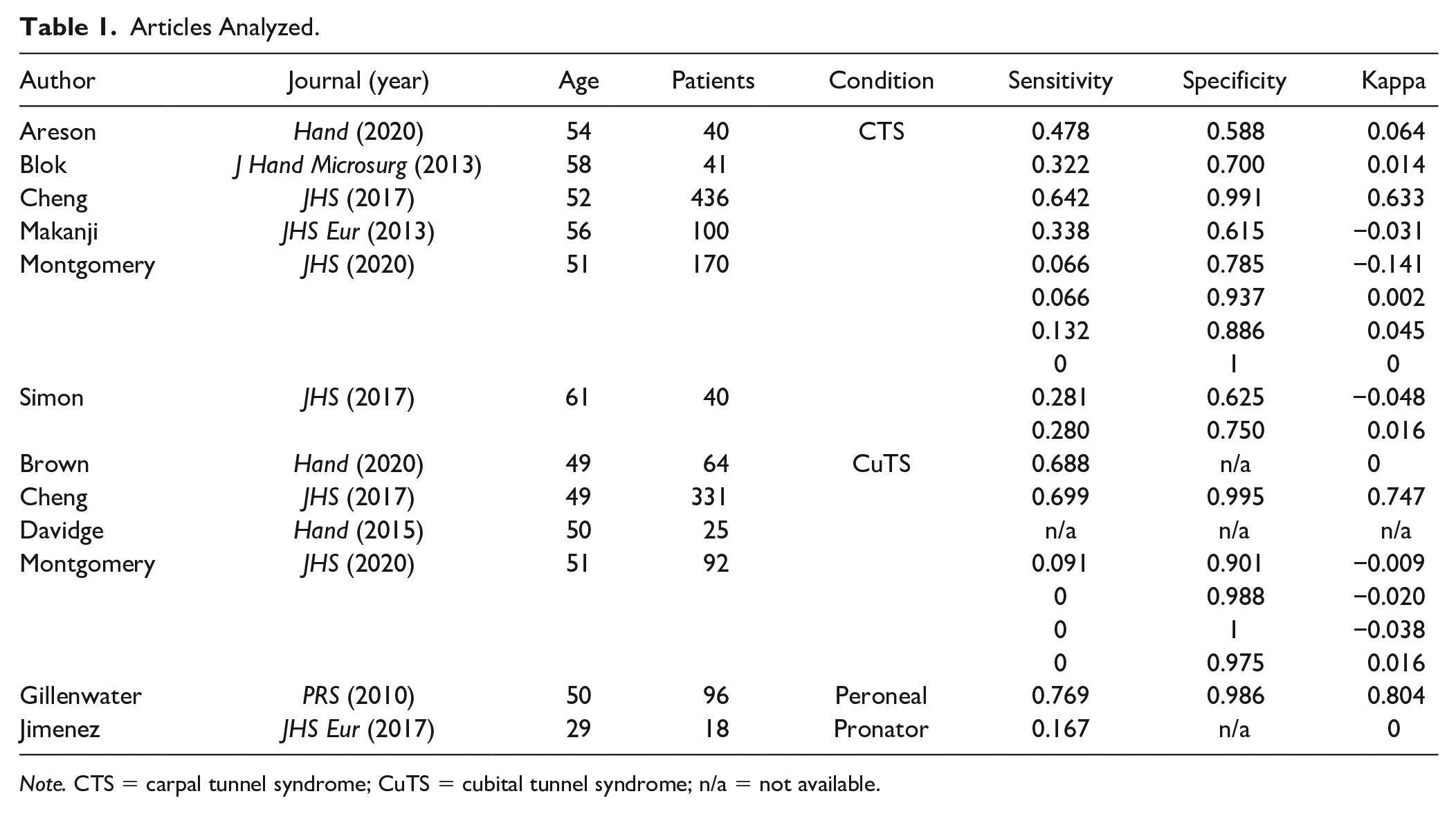
Note. CTS = carpal tunnel syndrome; CuTS = cubital tunnel syndrome; n/a = not available.
Demographic Breakdown.
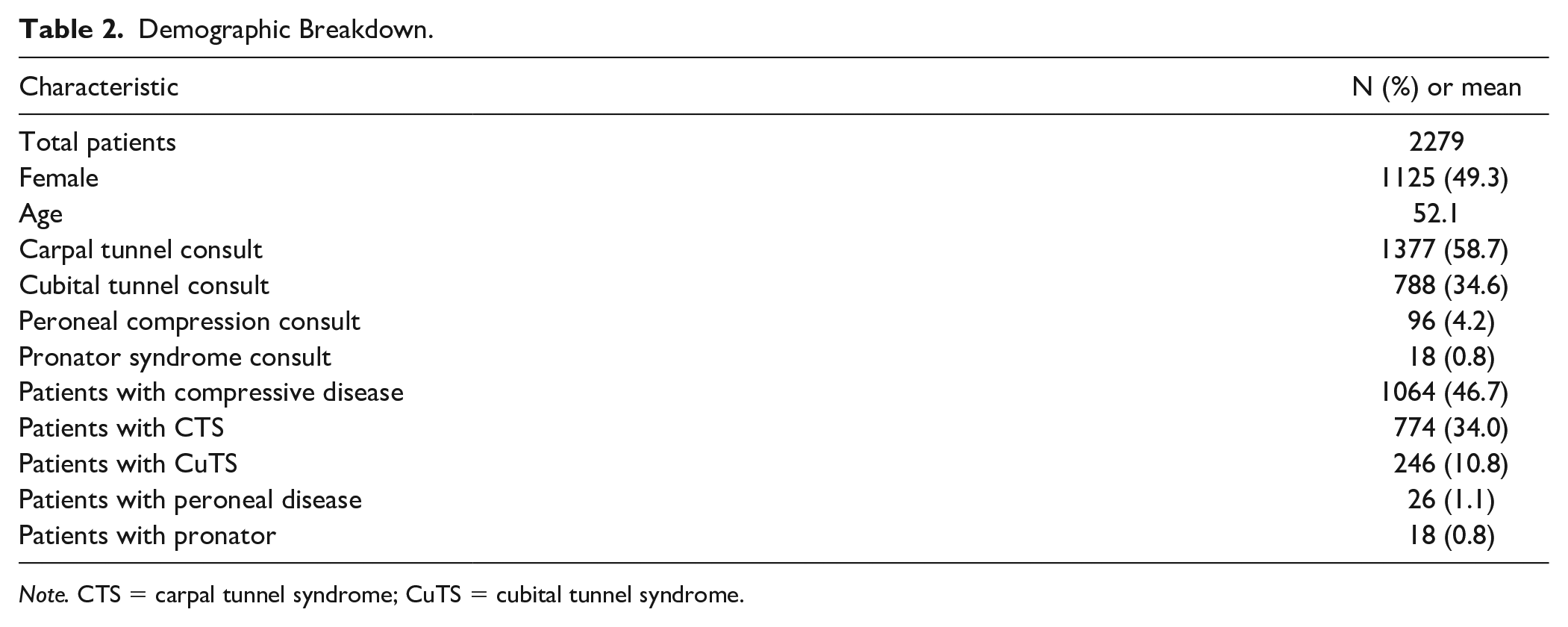
Note. CTS = carpal tunnel syndrome; CuTS = cubital tunnel syndrome.
Sensitivity and Specificity Analyses
Sensitivity and specificity analyses were performed on the pooled data. Of the 2279 extremities evaluated for neuropathies, 400 extremities had a positive SCT and a positive EDX, 71 extremities had a positive SCT and a negative EDX, 664 extremities had a negative SCT and a positive EDX, and 1144 extremities had both a negative SCT and a negative EDX. The statistical analysis yielded an SCT sensitivity of 37.5% and a specificity of 94.2% with a kappa value of 0.329 (Table 3).
Sensitivity and Specificity Breakdown.
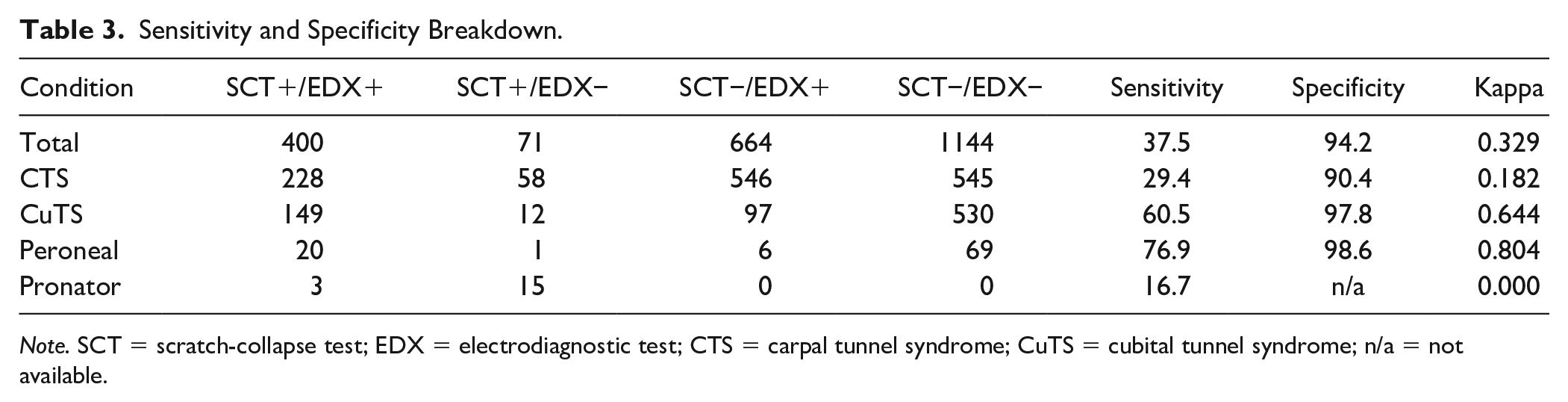
Note. SCT = scratch-collapse test; EDX = electrodiagnostic test; CTS = carpal tunnel syndrome; CuTS = cubital tunnel syndrome; n/a = not available.
Among patients with CTS, 228 had both tests positive, 545 had both tests negative, 58 had only a positive SCT, and 546 had only a positive EDX. This yielded a SCT sensitivity of 29.4% and a specificity of 90.4%. The kappa value for patients with CTS was 0.182 (Table 3).
Among patients with CuTS, 149 had both tests positive, 530 had both tests negative, 12 had only a positive SCT, and 97 had only a positive EDX. This yielded an SCT sensitivity of 60.5% and a specificity of 97.8%. This set of patients had a kappa value of 0.644 (Table 3).
For extremities with peroneal nerve compression, 20 extremities had both tests positive, 69 extremities had both tests negative, 1 extremity had only a positive SCT, and 6 extremities had only a positive EDX. This led to an SCT sensitivity of 76.9% and a specificity of 98.6%. The kappa value for these patients was 0.804.
All patients with pronator syndrome had a positive EDX. Only 3 patients had a positive SCT, and the remaining 15 had a negative SCT. This led to an SCT sensitivity of 16.7% and a specificity that could not be calculated. The kappa value for these patients was 0.000 (Table 3).
Comparisons of Sensitivity and Specificity Values
Finally, we performed comparisons between sensitivity and specificity values to determine if there was statistical difference between the calculated values. These data are presented in Table 4. We found that the CTS and pronator sensitivity and the CuTS and pronator sensitivities were statistically equivalent. All other comparisons showed statistical difference. On the other hand, only the CTS to CuTS and CTS to peroneal comparisons were statistically significant for the specificity; all others were statistically equivalent.
P Values for Sensitivity/Specificity Comparison.
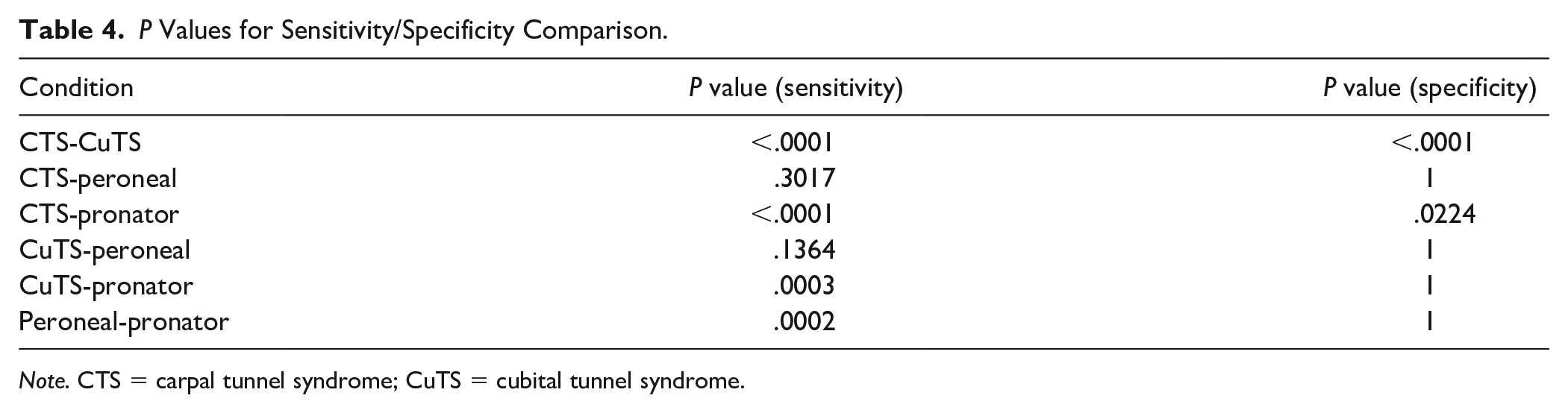
Note. CTS = carpal tunnel syndrome; CuTS = cubital tunnel syndrome.
Discussion
The SCT is a useful tool in the armamentarium of the hand surgeon to diagnose compressive neuropathies. However, due to the subjective nature of the test, the variability in test administration, and the ineffable ambiguity that plagues nerve compression itself, the utility of the SCT has been called into question. Given this, we performed a statistical analysis of all studies with quantifiable evaluation of the SCT against the accepted gold standard EDX to determine if the SCT is in fact a useful test that should be performed regularly.
For our pooled data set encompassing all compression neuropathies, we found that the SCT had a sensitivity of 37.5% and a specificity of 94.2%, with a kappa statistic of 0.329. This indicates that compression neuropathies cannot be excluded in patients with a negative SCT (tests with low sensitivities cannot exclude diagnoses; the false-negative rate is high) but can be confirmed in patients with a positive SCT (tests with high specificities can confirm diagnoses; the false-positive rate is low). Together, this suggests that the SCT is not a good screening test for patients with compressive neuropathies; ideal screening tests have high sensitivities to ensure that patients with the conditions are caught (a low false negative rate is desired). However, the SCT can be used for a confirmatory test as the specificity is high, implying a low false positive rate. The kappa statistic underlines this, demonstrating a “fair” agreement between the EDX and the SCT, as described by Cohen’s interpretation of the value.
We also applied these analyses to each specific compression tested. Patients with CTS had a lower sensitivity and specificity, whereas patients with CuTS and peroneal compression had higher values for both. The pronator syndrome patients could not be adequately analyzed as all patients in the data set had compression on EDX, so specificity could not be discussed.
Both sensitivity and specificity were statistically significantly lower in CTS patients than those for the other compressive neuropathies. Accordingly, the kappa value was 0.171 for CTS, suggesting slight agreement, 0.644 for CuTS, suggesting substantial agreement, and 0.804 for peroneal patients, suggesting a near-perfect agreement.
These outcomes are reflected in the individual articles used in this analysis. Areson et al performed a blinded SCT versus EDX study which showed a poor sensitivity and specificity as well as agreement between the studies. 23 This compelled the authors to argue against the use of the SCT in CTS. Meanwhile, Blok et al studied a similar set of patients. 22 They found poor sensitivity as well, but they also found excellent specificity compared with Areson et al, with a greater agreement, which they interpreted as an indeterminate result needing more studies. Similar findings were reported by Simon et al, who again found poor sensitivity with good specificity and kappa value. 16 Makanji et al 18 compared the SCT to other tests, such as the Tinel test, and found that the sensitivity of the SCT was worse although the specificity was better, as did Montgomery et al. 17 Both these studies argued for more stringent indications for SCT application.
On the other hand, Cheng et al studied the SCT in both CTS and CuTS and found that the sensitivity and specificity were improved compared with other provocative tests. 13 The outstanding data provided by this group are influenced by the fact that this study comes from the Mackinnon group, which introduces bias as the outcomes from the surgeon who pioneered this technique are understandably superior to those of other centers.
This fact also applies to the outstanding results in CuTS patients. Cheng et al, Davidge et al, and Brown et al provided a vast majority of the patients for the cubital tunnel analysis.13,15,21 Again, these articles are all products of the Mackinnon group, which suggests that the test performed by Dr. Mackinnon may be superior in subtle ways to that performed by other surgeons. However, these data are somewhat corroborated by Montgomery et al, who provided a similar specificity with a worsened sensitivity in a group of patients who were not directly evaluated by Dr. Mackinnon.
For both the peroneal and pronator nerve compressions, 1 article was available for each of them. Gillenwater et al, again a product of the Mackinnon group, demonstrate outstanding results for the peroneal compression patients, with the bias discussed above needing to be considered. 19 Jimenez and Delgado performed an analysis of pronator syndrome with a poor sensitivity and an incalculable specificity. 20 Although it provides some benefit as it does not come from the Mackinnon group, the limited data provided prevent application.
Interestingly, CTS patients had worse sensitivity and specificity on SCT than patients with CuTS. One explanation is that the Mackinnon group contributed the vast majority of CuTS patients but only provided a portion of the CTS patients. As a result, CTS patients had a wider variety of care providers performing the SCT, introducing variability into the performance of an already difficult examination maneuver. It is also possible that a wider clinical range of CTS was represented; CTS is familiar to the layperson, and thus, these patients are more likely to present to hand surgeons for evaluation and treatment. 24 In comparison, CuTS is less well known, and patients may not come to be evaluated until later stages, affecting the SCT. As discussed by Garcia-Medrano et al, the SCT has a stronger response with a more severe disease. 25 It may be that the “early” CTS patients contribute more to the “false-negative” group for the SCT.
The spatial relationship between the cubital tunnel and carpal tunnel may have implications for the SCT. At the level of the cubital tunnel, the ulnar nerve has given off very few branches—essentially all axons are present. Irritating this nerve during the SCT would provide a stronger signal to inhibit the spinal reflex as there is larger amplitude of current with more axons. 10 At the carpal tunnel, however, the median nerve has already significantly branched. In addition, there is variable neuroanatomy because of median-ulnar connections such as the Martin-Gruber and Richie-Cannieu coaptations.26,27 Irritation at the carpal tunnel involves fewer axons, resulting in a weaker signal to the spinal cord. In addition, signals from the carpal tunnel must travel further compared with the cubital tunnel, partially explaining worsened outcomes.
This study has multiple limitations. Although it is a pooled analysis across multiple studies, the percentage of patients from the Mackinnon group is relatively high. As discussed above, this introduces systematic bias into the study, as evaluation by the inventor of the test is inherently different from the evaluation by those who have learned from others. This point has been emphasized by the Mackinnon group in a recent work addressing how to perform the examination in detail. 28 Additional studies by other practitioners are necessary.
Further limitations are inherent; during a systematic review, we cannot guarantee that all studies were identified despite a rigorous search process. Also, symptom severity was not controlled for, again introducing bias. Regarding our statistical method, we opted to perform a pooled analysis rather than the more traditional meta-analysis. Although pooled analyses can identify trends in data that may not exist, and are thus inferior to meta-analyses, a proper meta-analysis requires certain data from the literature such as statistical outcomes reporting or detailed descriptions of each patient. Unfortunately, these data were not available.
Conclusion
The SCT is a provocative maneuver used by clinicians to aid in the diagnosis of compressive neuropathies. The utility and generalizability of the SCT remain controversial. We performed a systematic review and pooled analysis to determine if the SCT is comparable to accepted, gold standard electrodiagnostic studies. We found that the sensitivity of the scratch-collapse was poor, but the specificity was excellent. Although these data are heavily biased by the group of physicians who pioneered the examination, we believe that the SCT is a useful adjunct study that can confirm a diagnosis of nerve compression but should not be used as a first-line screening test.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All human and animal studies have been approved by the appropriate ethics committee and have, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Statement of Informed Consent
All patients were informed of possible participation in any 165 experimental treatments in this study and agreed to participate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
All sources of funds supporting the completion of this manuscript are under the auspices of the University of California, Los Angeles.