
Abstract
Salter-Harris II (SH2) proximal/middle phalanx fractures are common injuries in children and heal well with immobilization. We conducted a systematic review of nonsurgical treatments for SH2 proximal/middle phalanx fractures. The constructed search strategy used descriptors that included synonyms for “phalanx fracture,” “proximal/middle phalanx,” and “fracture treatment.” All steps of the process were performed by 2 independent reviewers. Articles of any study design that included children treated for SH2 proximal/middle phalanx fractures were included. Results were analyzed for summary statistics and interobserver agreement. Findings were reported in keeping with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The initial search yielded 3511 studies. Five studies met the final criteria: 1 randomized controlled trial (RCT), 3 prospective studies, and 1 retrospective study. Three studies employed a combination of taping and splinting strategies. All fractures healed with no reported complications. At the final follow-up, all studies reported full or nearly full range of motion and high rates of patient comfort and satisfaction. The RCT found lower rates of secondary displacement in the taping (6%) versus splinting (23%) group. Due to small sample sizes and heterogeneous study designs, conclusive recommendations cannot be drawn. More research is needed to determine the feasibility, compliance, safety, and effectiveness of taping these injuries.
Keywords
Introduction
The hand is the second most common site of fracture in children, representing one fourth of all pediatric fractures.1,2 Management of these injuries accounts for a significant proportion of pediatric emergency department visits. Over 70% of hand fractures involve the phalanges, and the proximal phalanx is the most fractured bone. 3 Almost 80% of proximal phalanx fractures are either juxta-epiphyseal or Salter-Harris II (SH2). 4 Most of these fractures heal well without surgical intervention. Traditionally, children are immobilized with a cast or splint for 2 to 4 weeks until the fracture heals.5,6
Less restrictive treatment such as buddy taping has been demonstrated to confer a more time- and cost-effective method to treat metacarpal neck fractures in adults. 7 Taping an injured digit to an adjacent finger is an inexpensive and relatively simple procedure for primary practice and emergency department visits. Moreover, buddy taping enables early mobilization that promotes quicker recovery with range of motion and strength and improves time to return to normal function.8 -11 Studies examining rigid casts versus flexible bandages in children with distal radius buckle fractures further report increased patient comfort and comparable functional outcomes of the softer option.12,13
The goal of this study was to systematically review less restrictive treatment options of SH2 proximal and middle phalanx fractures to identify existing evidence as well as gaps in knowledge.
Methods
A systematic review of nonsurgical treatment options of SH2 proximal and middle phalanx fractures was performed to synthesize evidence-based treatments. This systemic review was conducted and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocols (PRISMA-P). 14
Eligibility Criteria
Inclusion criteria were studies of any design that included pediatric patients treated nonsurgically for SH2 proximal and middle phalanx fractures of any finger published in English. Studies reporting distal phalangeal fractures of the hand, open fractures, pathological fractures, and exclusively hand fractures other than SH2 proximal and middle phalanx fractures were excluded.
Outcome Measures
All outcomes reported by the studies were recorded. This included clinical and functional outcomes as well as patient-reported factors such as comfort, cost, convenience, preference, compliance, complications, and overall patient satisfaction.
Search Strategy
A peer-reviewed search strategy was conducted on June 28, 2022. 15 Databases searched included MEDLINE(R) ALL via Ovid, Embase Classic + Embase via Ovid, Cochrane Central Register of Controlled Trials via Ovid, and CINAHL via EBSCOhost. The databases were searched on July 19, 2022. The search strategy was developed in Medline and translated to other databases. The main search concepts were comprised of terms related to finger phalanges, Salter-Harris fractures, and conservative treatments.
The following steps were performed by two independent reviewers. The obtained articles were first screened based on titles and abstracts, followed by full-text review, if relevant. Disagreements in the title and abstract screening were automatically included for full-text review. Disagreements in full-text review were managed with discussion with all reviewers and the senior author until consensus was reached. Reference lists of included sources were also searched for additional studies. A standardized data-collection form developed according to the Cochrane guidelines was used to extract data from the selected articles. 16
Evidence and Quality Assessment
The level of evidence was determined using the Oxford Center for Evidence-based Medicine Levels of Evidence. 17 The evaluation of quality of the included studies was performed using MacDermid’s Structured Effectiveness Quality Evaluation scale (SEQES), which is a 24-item critical appraisal tool that provides a comprehensive assessment based on 7 categories: study question, study design, subjects, intervention, outcomes, analysis, and recommendations. 18 For reference, a low-quality score ranges from 1 to 16, moderate quality from 17 to 32, and high quality from 33 to 48.
Statistical Analysis
Descriptive statistics of study and patient characteristics and outcomes was performed. Cohen’s Kappa was used to calculate inter-rater agreement. A meta-analysis was not performed due to heterogeneity between studies, varying methodology, and lack of consistency in reporting outcome measures.
Results
Study Extraction
The study-identification process is shown in Figure 1. The initial search yielded 3511 results, and following removal of duplicates, 2351 titles and abstracts were reviewed. Two-hundred and twenty-nine studies underwent full-text review, and 5 met the eligibility criteria. Examination of reference lists from included articles did not yield any additional studies for inclusion. Cohen’s Kappa for inter-rater agreement for title and abstract screening as well as full-text review was 0.57 and 0.38, respectively.
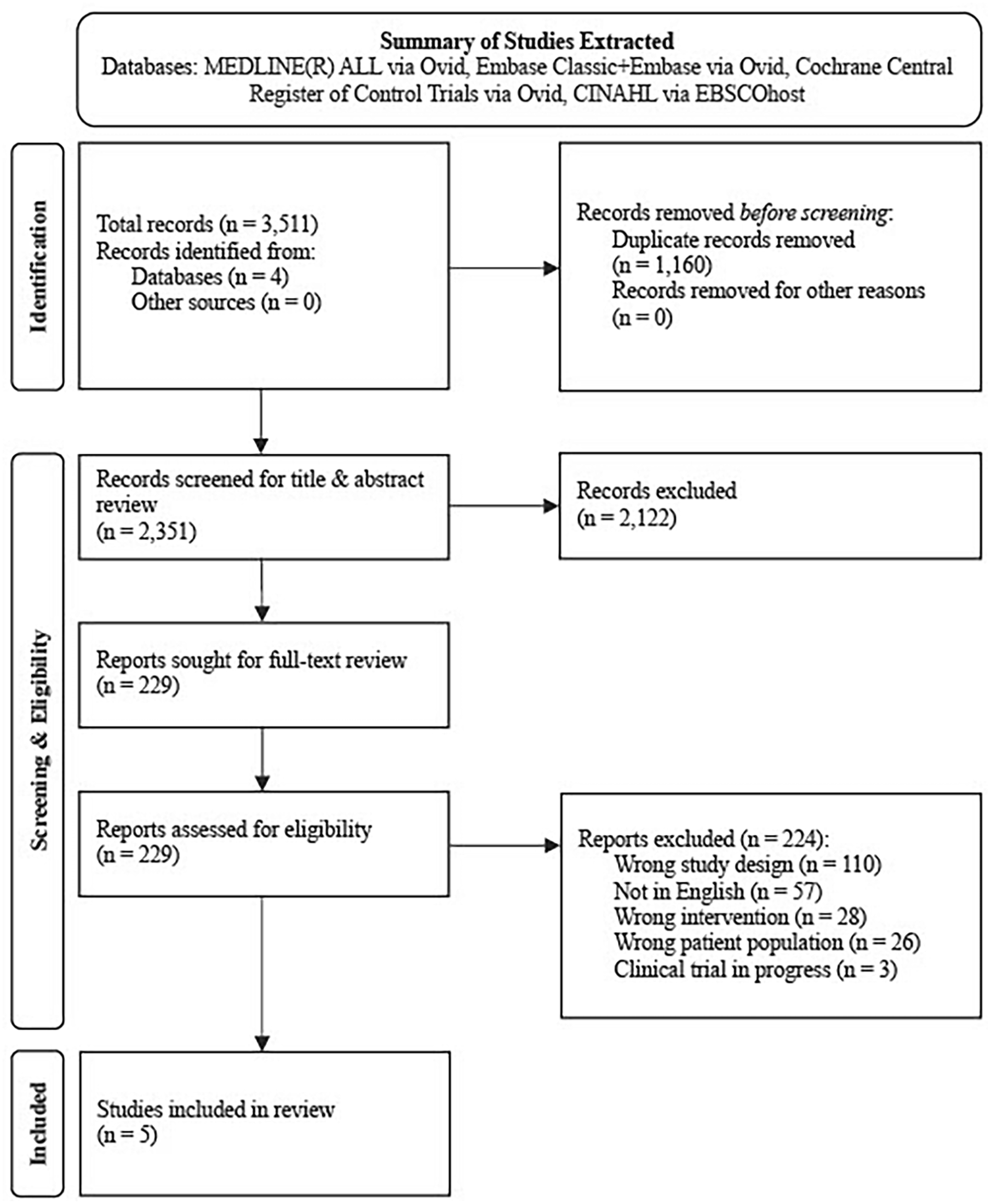
Overview of study-extraction protocol.
Quality Assessment
Table 1 summarizes the SEQES scores evaluated for each included study. Structured Effectiveness Quality Evaluation Scale scores ranged from 13 (low quality) to 42 (high quality). Most of the included studies were moderate or high in quality. One study had a low quality score given poor study design.
Studies Assessed via Structured Effectiveness Quality Evaluation Scale (SEQES).

Result totals relate to study quality based on the following breakdown: low quality 1 to 16, moderate quality 17 to 32, high quality 33 to 48.
Study Design
All studies involving nonsurgical treatment options of proximal and middle phalanx fractures in children were included. This amendment was made to the original protocol as some of the studies did not identify Salter-Harris fracture subtypes or grouped various subtypes together. Although this resulted in deviation from the original protocol, it broadens the scope by including fractures that may have otherwise been missed or excluded. Table 2 summarizes the study characteristics.
Study Designs.
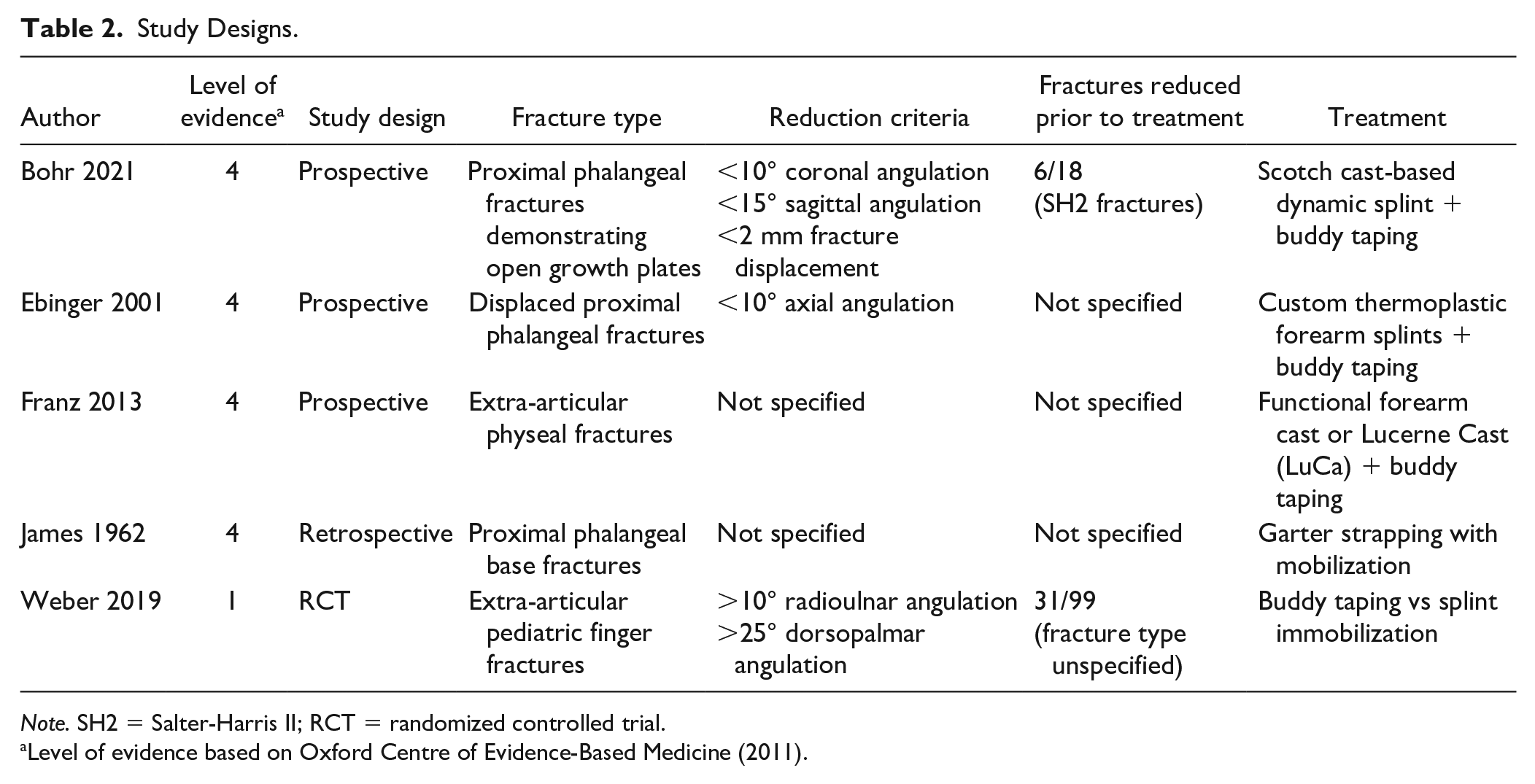
Note. SH2 = Salter-Harris II; RCT = randomized controlled trial.
Level of evidence based on Oxford Centre of Evidence-Based Medicine (2011).
A variety of nonsurgical techniques were identified, including taping to an adjacent uninjured finger or wearing a forearm cast or splint but allowing protected mobilization of the injured digits via taping. Of the prospective studies, Bohr, Ebinger, and Franz employed the use of a splint plus buddy taping technique to treat their study population.19 -21 Notably, the terminology to describe the taping regimens also varied between studies. Weber and James utilized taping regimens without additional casts or splints; however, James referred to their taping pattern as garter strapping.22,23 The randomized controlled trial (RCT) by Weber was the only article to compare taping versus splinting techniques for the treatment of proximal and middle phalanx fractures. 21 Overall, all treatment designs enabled immediate mobilization of the proximal and distal interphalangeal joints.19 -23
Treatment Outcomes
Table 3 outlines the reported outcomes from each study. In total, 180 patients were included. Only three studies specified the SH2 fracture subtype, which accounted for 30 of these patients (17%). Treatment duration ranged from 1 to 4 weeks, and follow-up duration was 3 weeks to 1 year.
Patient Characteristics and Outcomes.
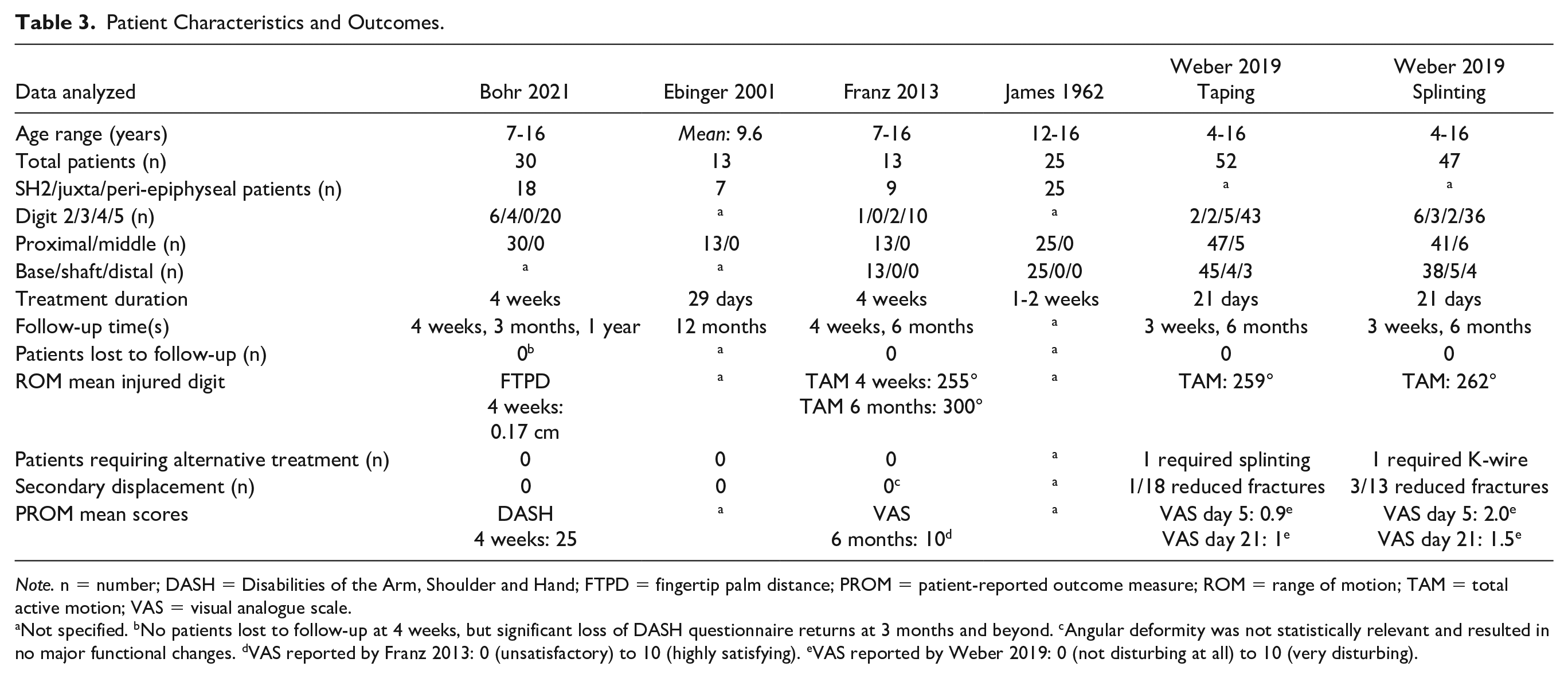
Note. n = number; DASH = Disabilities of the Arm, Shoulder and Hand; FTPD = fingertip palm distance; PROM = patient-reported outcome measure; ROM = range of motion; TAM = total active motion; VAS = visual analogue scale.
Not specified. bNo patients lost to follow-up at 4 weeks, but significant loss of DASH questionnaire returns at 3 months and beyond. cAngular deformity was not statistically relevant and resulted in no major functional changes. dVAS reported by Franz 2013: 0 (unsatisfactory) to 10 (highly satisfying). eVAS reported by Weber 2019: 0 (not disturbing at all) to 10 (very disturbing).
Bohr assessed patient recovery through fingertip palm distance (FTPD) and the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire. A mean FTPD of 0.17 ± 0.27 cm (mean ± SD) was reported at the final follow-up which indicated near-complete range of finger motion. The mean 4-week DASH score was 25 overall (minimal difficulty and excellent clinical outcome). 19
Franz reported total active motion (TAM) and visual analogue scale (VAS) of patient and parent satisfaction. The mean finger TAM increased from 255° at 4 weeks to 300° at the final 6-month follow-up (maximum TAM score of 305°). In the SH2 patients specifically, the mean finger TAM scores improved from 266° at 4 weeks to 299° at 6 months. The VAS mean score for all patients at 6 months was 10 (highly satisfying). 21
Weber reported TAM and VAS for patient comfort in both taping and splinting groups. In this study, VAS scores were parent-reported based on phalanx appearance and ranged from 0, not disturbing, to 10, very disturbing. Mean TAM scores were comparable between groups, with 259° reported in the taping group versus 262° with splinting (P = .51). Conversely, mean VAS scores were better in the taping (0.9) versus the splinting group (2.0) after 5 days (P = .01) and comparable between groups at 3-week follow-up (P = .25). One patient in the taping group required cross-over to the splint treatment group due to secondary displacement. The caregivers of another patient randomized to the taping group feared that taping was insufficient and requested a supplementary splint. In the splinting group, 1 patient with a proximal shaft fracture required secondary reduction and K-wire immobilization. 22
In addition, Weber noted the cost of taping was significantly lower (38 euros) than the cost of splinting (160 euros), leading to a parental preference for the more economical option. The average time for application was also less for taping (4.8 minutes) compared to splinting (15.8 minutes), which resulted in a clinician preference for the timesaving option. 22
All fractures healed, and no delayed or nonunions were reported by any of the studies.19 -23 Franz commented on a slight, but clinically insignificant, ulnar angulation (range 2°-6°) in three patients treated with SH2 injuries. 20 As mentioned earlier, Weber reported a secondary displacement for one of the 52 patients in the taping group. This was detected at the first follow-up visit on day 5 and the patient was changed to the splinting regimen. In comparison, 3 of the 47 patients in the splinting group had secondary displacements. Moreover, the risk of secondary displacement was not higher with treatment by buddy taping alone than by rigid immobilization with a forearm-based splint. 22
Discussions
This systematic review evaluates the evidence for nonsurgical treatment options for SH2 proximal and middle phalanx fractures. Results were limited to 3 prospective studies, 1 retrospective study, and 1 RCT.
The treatment modalities included in this systematic review found excellent functional and clinical outcomes. At final follow-ups, all studies reported full or nearly-full range of motion as well as high rates of patient comfort and satisfaction. Of note, in the RCT by Weber, higher satisfaction at early follow-up was observed for taping compared to splinting. 22
In the adult population, buddy taping has shown promise in various hand fractures, including fifth metacarpal neck fractures and metacarpal diaphyseal fractures. There is significant empiric support for taping in the treatment of metacarpal neck fractures. Multiple randomized trials have found taping to be effective for improving pain, range of motion, strength, and time to return to work in comparison to plaster immobilization.10,11,24 A systematic review and meta-analysis also recommended buddy taping over plaster and immobilization for uncomplicated closed fifth metacarpal neck fractures. 25 Likewise, a prospective single-center study found metacarpal diaphyseal fractures treated with taping resulted in little pain, stiffness, strength loss, and no cases of nonunion. 26
Buddy taping may also provide practical benefits in terms of cost and time for application. Taping may also be simpler to administer and less dependent on the skill of the clinician.
Moreover, the studies included did not report any skin complications or issues with compliance. This contrasts with a prior report of pediatric hand surgeons who reported skin injuries, infections, low compliance, and secondary displacements when using buddy taping for various finger and toe injuries. 27
Limitations
There are several limitations to the studies included in this review. Only 1 of the 5 studies was of high quality. There was considerable variation in the reported outcome measures such as range of motion or follow-up times. Many studies lacked control groups for comparison and had small sample sizes. Moreover, variation in treatment designs incorporating taping made it difficult to isolate the specific effects of buddy taping. Certain treatment designs combined forearm casting or splinting with taping, whereas others used taping alone. As such, this heterogeneity in treatment and outcomes prohibited pooling of outcomes.
Furthermore, some of the studies did not provide specific information on the type of injury or fracture. SH2 injuries were possibly grouped with more severe injuries. For example, Weber noted that a patient in the taping regimen was switched to splinting due to secondary displacement, but the specific fracture for this patient was not reported. In the same article, the caregivers of another patient expressed concerns that taping was not providing adequate immobilization for their child and requested a switch to the splinting group, yet the type of fracture was undisclosed.
Conclusion
Due to the limitations mentioned earlier, it is difficult to make recommendations on the efficacy of buddy taping as a treatment modality. More robust studies are needed to make definitive conclusions. Consistent inclusion criteria, treatment methods, structured outcome measures, large sample sizes, and comparison groups will help provide greater empirical support for buddy taping as a treatment modality. Assessment of patient comfort and satisfaction at earlier follow-up intervals may lend greater support for taping than for other measures. Future studies should also specify the type of Salter-Harris injury, especially when reporting complications or issues. Notably, during the screening process, we identified some ongoing randomized controlled clinical trials investigating buddy taping for pediatric finger fractures. 28 These results are pending. Despite these limitations, the studies included in this review show promise for taping as a treatment modality consistent with our hypotheses and anecdotal experience. Nearly all fractures healed, no functional deficits were reported, and patient-reported outcomes were overwhelmingly positive.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.