
Abstract
Background:
The role of surgery in normal or very mild median neuropathy can be questioned given that surgery in the absence of pathophysiology may offer only nonspecific effects that can be achieved without surgery, which raises ethical concerns. It’s also important to avoid misdiagnosis: given that mild median neuropathy is prevalent and generally well-accommodated, notable symptoms from mild median neuropathy can signal unhelpful thoughts and feelings of distress that are a more pressing health priority.
Methods:
We identified 38 studies that categorized electrodiagnostic (EDX) measured median neuropathy severity among people being evaluated for carpal tunnel syndrome. We converted the different EDX grades used into one general grading classification. The Kruskal–Wallis test was used to compare the ratio of moderate/severe to mild/normal EDX findings between tests ordered by a surgeon or a nonoperative clinician.
Results:
The median (interquartile range) ratio of moderate/severe to mild/normal EDX findings of median neuropathy at the carpal tunnel was 1.2 (0.91 to 1.8) among tests ordered by nonoperative clinicians and 3.3 (1.5 to 5.3) among tests ordered by surgeons (P = .0023). Only 4.1% of the patients who had EDX testing ordered by a surgeon had no measurable neuropathy. There were zero patients with normal EDX findings in 10 of the 17 (59%) studies in surgeon practices and in 10 of the 21 (48%) in the practices of nonoperative clinicians.
Conclusions:
The observation that in case series documenting EDX severities of median neuropathy, surgeons are mostly treating and operating on moderate to severe pathophysiology, emphasizes that while mild median neuropathy is highly prevalent it is uncommonly considered for surgery.
Level of evidence:
Level II, Prognostic study.
Keywords
Introduction
Background
Objective measurement of idiopathic median neuropathy at the carpal tunnel (IMNCT) is performed using electromyography (EMG) and nerve conduction studies (NCS). The results of these tests are often interpreted as normal, mild, moderate, or severe although the criteria and classification system for each grading system may vary by institution.1 -5 Practice patterns also widely vary as nonspecialists may use electrodiagnostic (EDX) testing as a diagnostic aid or to prioritize specialty care, while surgeons typically use it prior to surgery to confirm appropriateness and as a baseline to help council patients. Additionally, IMNCT is often clinically diagnosed based on characteristic signs and symptoms (carpal tunnel syndrome [CTS]) with a relatively high probability. 6 Therefore, the role of EDX testing in the diagnosis of IMNCT is debated. 7
It is often stated that EDX tests are not a reference standard for the diagnosis of IMNCT.7,8 This, at times, seems to be used as a justification for offering surgery to patients with relatively mild or no detectable pathophysiology on EDX testing. While some surgeons report improvement after carpal tunnel release (CTR) even with mild and normal EDX findings,9,10 these claims do not account for effects unrelated to the treatment of pathology (nonspecific effects) such as regression to the mean and placebo effects. 11 The role of surgery in normal or mild median neuropathy can be questioned given the difficulty distinguishing normal and mild median neuropathy on EDX testing, 7 the fact that mild median neuropathy at the carpal tunnel is highly prevalent and well-accommodated,7,12 -14 and the evidence that symptom intensity correlates more with mindset and circumstances (psychosocial factors) than median neuropathy severity (pointing to priorities in diagnosis and treatment of mental health).15,16
Rationale
Published data regarding levels of median neuropathy severity have the potential to inform debate about offering surgery for median nerves with little or no measurable pathophysiology. If studies of electrodiagnosis among surgeons evaluating people with CTS consist mostly of people with moderate or severe neuropathology, and mild or unrecordable IMNCT are relatively more common in studies of EDX ordered by nonsurgeon clinicians, that would support the concept that mild or unrecordable IMNCT, while quite common, is usually treated nonoperatively, and is likely generally well-accommodated. Such findings would suggest that it might be helpful to deprioritize considerations of surgery for mild or unmeasurable IMNCT associated with notable incapability until accommodation (thoughts, feelings, and security regarding symptoms) is optimized.
Study Questions
We systematically reviewed reports of EDX severity of median neuropathy at the carpal tunnel among people with CTS (suspected IMNCT) to answer this question: What is the ratio between severe/moderate to mild/normal EDX findings of median neuropathy of the carpal tunnel when the test is ordered by a surgeon compared to a nonoperative clinician?
Materials and Methods
This study was carried out in accordance with our institution’s ethical standards and according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines.
Study Eligibility
Eligible studies were those that reported EDX severity levels of median neuropathy at the carpal tunnel. We excluded studies that did not report levels of severity of median neuropathy, editorials, case reports, nonclinical studies, cadaver studies, conference abstracts, or studies not published in English.
Study Search
We performed a systematic review of studies that reported categories of EDX severity of median neuropathy at the carpal tunnel from PubMed published between 1982 and May 2021. The search was performed on May 18th, 2021 and consisted of terms for: (1) electrodiagnosis/EDX (eg, EMG, NCS, etc.); (2) CTS/median neuropathy; and (3) grade/severity/score/classification.
Article Selection
Two researchers independently screened all titles and abstracts and, if a study was deemed eligible, both researchers screened the full-text with the help of predefined inclusion criteria. Articles met the inclusion criteria if they reported EDX severity categories with a clear distinction of severity grade of median neuropathy at the carpal tunnel. The search resulted in 331 results, and after removing duplicates, we screened 329 articles. One-hundred-six articles were selected for full-text screening, of which 38 were included for data extraction following adherence to inclusion and exclusion criteria (Figure 1, Appendix 1). When a disagreement occurred during article screening, both independent researchers discussed these articles until a consensus was achieved.
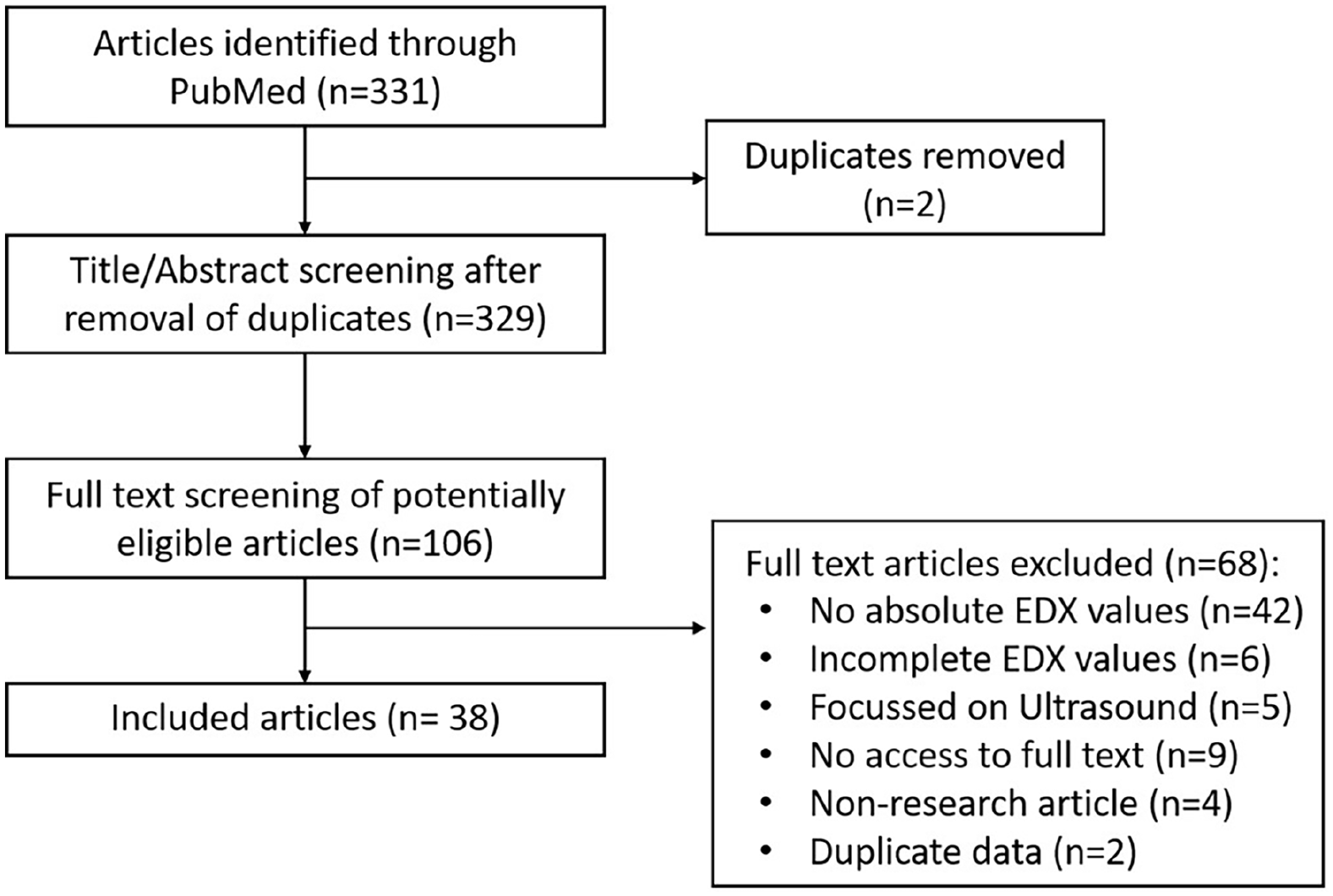
Flow chart of search strategy, inclusions, and exclusions.
Quality Assessment
We did not perform a quality assessment since we collected raw descriptive data from cohort studies, for which there is no widely agreed upon quality measure.
Outcome Measures and Data Extraction
The main outcome measurement was the ratio of moderate and severe to mild and normal EDX findings of median neuropathy at the carpal tunnel. Secondary study outcome measurement was the percentage of hands with normal/mild/moderate/severe EDX results.
The following data were extracted from all included studies: study design, setting, the used EDX severity grading scale, number of patients, number of hands, the number of hands with clinical CTS diagnosis/that had EDX/with EDX findings of median neuropathy, percentage of hands with EDX confirmed CTS, the number and percentage of hands with normal/mild/moderate/severe EDX findings, the number and percentage of hands (that had EDX) that received CTR, the number and percentage of hands (that had EDX) with normal/mild/moderate/severe EDX findings that received CTR.
A conversion table was made to convert all the different EDX grading classifications used by studies into one general EDX grading classification as follows: (1) Normal: no significant motor or sensory changes (Distal Motor Latency [DML] < 4.2 millisecond [ms] AND Distal Sensory Latency [DSL] < 3.4 ms); (2) Mild: either significant motor OR sensory changes, but not both (DML > 4.2 OR DSL > 3.4 ms); (3) Moderate: significant motor AND sensory changes were observed, without signs of permanent axon loss (DML > 4.2 AND DSL > 3.4 ms); and (4) Severe: significant motor changes with (near) total absent sensory signaling loss (sensory nerve conduction velocity <20 m/second or not obtainable, sensory nerve action potential <4.0 mv or not obtainable), presence of polyphasic waves, fibrillations, and increased mean duration of motor unit action potential (>20 ms) (Appendix 2). The AANEM grading classification was most frequently used in the included studies (13 of 38 studies).
We considered two different study settings: (1) EDX ordered by nonsurgeon clinicians (possibly more often for diagnosis; n = 21); and (2) EDX ordered by surgeons (possibly more often for preoperative confirmation and as a prognostic tool; n = 17).
Statistical Analysis
Descriptive statistics were performed on the number of hands and percentage of each EDX severity grade, the ratio moderate/severe to mild, and the proportion of hands that received CTR. Continuous variables with a normal distribution were described as mean with standard deviation (SD), nonnormally distributed continuous variables were presented as median with interquartile range (IQR), and categorical data was described as numbers with percentages.
The Kruskal–Wallis H test was used to compare the ratio of moderate/severe to mild EDX findings between the diagnostic and surgical settings when there was a nonnormal distribution of the data. The Student t-test was used to compare the percentage of moderate/severe EDX findings between the diagnostic and surgical settings when there was a normal distribution of the data. All variables with a P-value of below .05 were considered statistically significant.
Results
What Is the Ratio Between Severe/Moderate to Mild EDX Findings of Median Neuropathy of the Carpal Tunnel When the Test Is Ordered by a Surgeon Compared to a Nonoperative Clinician?
The percentage of moderate and severe IMNCT on EDX was higher among tests ordered by surgeons (76%) compared to the nonsurgeons (50%) (P = .0040) (Table 1 and Figure 2). Only 4.1% of the patients who had EDX testing ordered by a surgeon had no measurable neuropathy, and there were zero patients with normal EDX findings in 10 of the 17 (59%) studies of surgeon practices and 10 of the 21 (48%) in studies of nonsurgeon practices. The median (IQR) moderate/severe to mild/normal ratio of EDX findings of median neuropathy at the carpal tunnel was 1.2 (0.91 to 1.8) in the nonsurgeon settings and 3.3 (1.5 to 5.3) in the surgeon settings (P = .0023) (Table 2).
Demographics of the Number and Percentage of Each Electrodiagnostic Severity Grade of Median Neuropathy at the Carpal Tunnel (CTS) in Different Settings.

SD = standard deviation; CTR = carpal tunnel release.
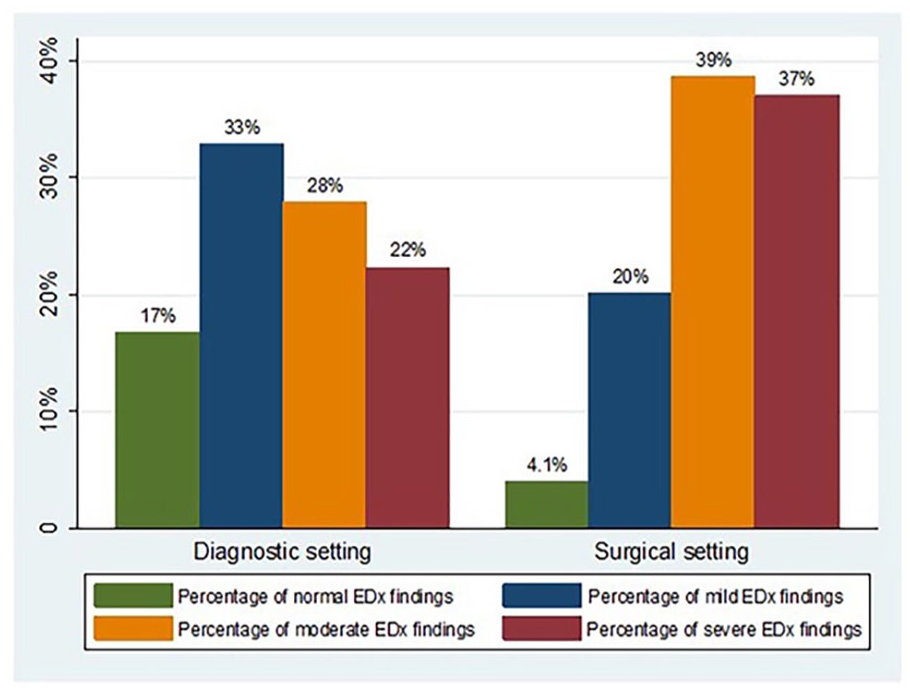
Percentage categorical severity of median neuropathy by setting.
Descriptive Statistics on the Ratio of Moderate or Severe to Mild or Normal Electrodiagnosis of Median Neuropathy at the Carpal Tunnel in Different Settings.
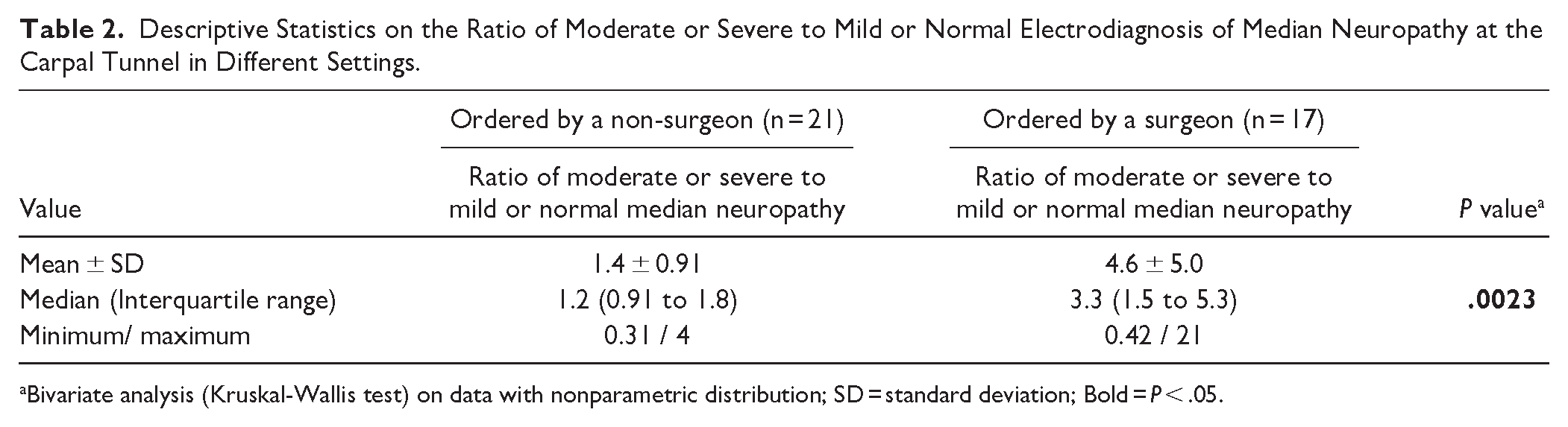
Bivariate analysis (Kruskal-Wallis test) on data with nonparametric distribution; SD = standard deviation; Bold = P < .05.
Discussion
Background and Rationale
IMNCT can be diagnosed based on characteristic symptoms and signs with a high probability 6 and the role of EDX testing in diagnosis is debated.7,8 This sometimes seems to be used as a justification for offering CTR to patients with mild or normal EDX findings. The role of CTR for mild IMNCT or normal EDX tests can be questioned, as the pathology may not be the most important health priority and such surgeries may not outperform nonspecific effects such as the placebo effect. The aim of this study was to look at the proportion of moderate/severe and mild/normal EDX findings in nonsurgeon and surgeon practices to provide an estimate of the magnitude of abnormal EDX associated with evaluation by a surgeon. The proportion of moderate/severe EDX findings and the ratio of moderate/severe to mild/normal EDX findings were significantly higher when the test was ordered by a surgeon to tests ordered by a nonsurgeon clinician.
Limitations
This study has a number of limitations. First, there is a level of uncertainty regarding the strategies and intent of EDX utilization across different settings as studies often did not outline their EDX strategy in detail. Nevertheless, the comparison between nonsurgical clinicians (presumably diagnostic) and surgeons seems likely to represent the characteristics of people under consideration for possible surgery and the numbers and proportions of EDX criteria are relatively consistent within each setting across studies. Second, there were various scales for categorizing EDX results among the studies included. It was fairly easy to regroup categories based on common features and we believe our recategorizations are likely reproducible and representative of important differences in pathophysiology.
What Is the Ratio Between Severe/Moderate to Mild EDX Findings of Median Neuropathy of the Carpal Tunnel When the Test Is Ordered by a Surgeon Compared to a Nonoperative Clinician?
The observation that the ratio of severe/moderate to mild/normal EDX findings was higher when the test was ordered by a surgeon than a nonsurgeon and the fact that 10 of 17 studies reported that zero patients with normal EDX findings were considered for an offer of surgery, might reflect that surgeons primarily consider surgery in patients with moderate and severe EDX findings and that it is uncommon to consider surgery for patients with mild and normal EDX findings. When one reads about surgery for CTS, one might get the impression that normal or mild EDX testing should not deter one from offering surgery, but various lines of evidence suggest that most surgeons think otherwise.17,18 According to a study from Canada in 2015, 99% of the surgeons would recommend splinting instead of surgery for patients with mild EDX findings. 18 Another study reported a decrease in offer of CTR with lower severities (54% for severe, 46% for moderate, 33% for mild, and 6% for normal), and also reported a higher odds ratio [OR] for CTR in moderate and severe compared to mild cases (OR = 2.48, 95% confidence interval [95% CI] [1.04 to 5.93], P = .04; and OR = 3.79, 95% CI [1.51 to 9.50], P = .005 respectively). 17 These findings suggest that surgeons who offer surgery to people with normal EDX tests may be relative outliers, and that the norm is to offer surgery to people when neuropathy is moderate or severe. Moderate to severe disease is both easier to distinguish from normal 7 and more likely to have greater correspondence between symptoms and pathophysiology.17 -19 At milder levels of neuropathy, mental and social health factors associated with greater symptom intensity and greater magnitude of incapability15,16 might give a clinician the impression of more advanced pathology—a potential bias that clinicians can anticipate and prepare for. 20 There is evidence that, in general, surgeons tend to determine severity based on signs of advanced pathophysiology rather than magnitude of incapability. 21 This suggests that surgeons who consider IMNCT severe based on notable symptoms and incapability are, again, in the minority. Future studies might evaluate the benefit of specific debiasing strategies that might help clinicians distinguish variation in comfort and capability (illness) from variation in pathophysiology, which are notably distinct.22,23
Some surgeons might argue that offering surgery to patients with mild and normal EDX findings is justified by evidence that outcomes after CTR are unrelated to the EDX severity.9,10,21,24 -28 For instance, one study reported improvement of patient-reported outcome measures (Q-DASH) after CTR treatment irrespective of mild, moderate, or severe EDX severities. 10 A similar study reported that Boston Carpal Tunnel Questionnaire scores after CTR were independent of preoperative distal motor latency. 9 Caution is warranted, as the lack of correspondence between outcomes and pathology in patients with documented IMNCT may be due to the strong influence of psychosocial factors on patient-reported outcome measures.15,16 There is also a need to acknowledge and respect the influence of nonspecific factors (changes in symptoms unrelated to changes in pathology). For instance, while a study of 57 people diagnosed with CTS in spite of normal EDX studies noted symptom improvement in 40 of 57 patients after CTR, 28 there is no way to know if the alleviation of symptoms was related to improvements in pathophysiology from surgery since there was no measurable pathology. Likewise, in the absence of simulated surgery controls, one cannot discern whether improvement is due, in whole or in part, to nonspecific effects such as the placebo effect. It is possible that these patients did not have IMNCT, in which case their surgery could only have nonspecific effects. A systematic review of simulated surgery-controlled trials (none addressing CTR) reported improved outcomes in both the intervention and simulated surgery in 38 of the 53 (72%) included studies, and there was no difference between actual and simulated surgery across several types of illnesses in 51% of the included studies. 11 In the absence of measurable pathology (entirely subjective illness) the only acceptable way to study the potential benefits of surgery is with a randomized, double-blind simulated surgery-controlled trial.
Published EDX studies of patients preparing for surgery demonstrate that surgeons mostly consider surgery among people with symptoms from moderate or severe disease and uncommonly consider surgery among people with normal EDX testing. The enumerated reasons for caution in offers of surgery for borderline and normal EDX of the median nerve at the carpal tunnel include: (1) the absence of evidence that CTR in patients with normal EDX severity outperforms nonspecific effects and has more potential for benefit than for harm (which raises ethical concerns); (2) the observation that the norm is for surgeon to determine severity based on measurable pathology rather than magnitude of capability; 20 and (3) the consistent observation that symptom intensity and magnitude of incapability correlate more with mental health than measurable pathology. 16 Advocates of surgery in patients with normal or borderline EDX can perform a blinded, randomized comparison of division of the transverse carpal ligament with simulated (placebo) division to establish whether or not surgery has more than nonspecific effects.
Supplemental Material
sj-docx-1-han-10.1177_15589447241284776 – Supplemental material for Most Carpal Tunnel Releases Address Moderate or Severe Median Neuropathy
Supplemental material, sj-docx-1-han-10.1177_15589447241284776 for Most Carpal Tunnel Releases Address Moderate or Severe Median Neuropathy by Niels Brinkman, Calvin Chandler, David Ring, Gregg Vagner and Lee Reichel in HAND
Supplemental Material
sj-xlsx-1-han-10.1177_15589447241284776 – Supplemental material for Most Carpal Tunnel Releases Address Moderate or Severe Median Neuropathy
Supplemental material, sj-xlsx-1-han-10.1177_15589447241284776 for Most Carpal Tunnel Releases Address Moderate or Severe Median Neuropathy by Niels Brinkman, Calvin Chandler, David Ring, Gregg Vagner and Lee Reichel in HAND
Footnotes
Acknowledgements
The authors would like to thank Amirreza Fatehi (Doctor of Medicine, MD) for their contributions to this article.
Ethical Approval
This review of online data did not require ethical approval.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
No patients have been involved in this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DR received royalties from Skeletal Dynamics for an internal joint stabilizer elbow and from Wolters Kluwer. DR is a deputy editor for Hand and Wrist and Clinical Orthopaedics and Related Research.® DR received honoraria from various CME providers, hospitals, and universities.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.