
Abstract
Background:
The arcade of Struthers was first proposed by Kane et al in 1973. Clinical investigations of this structure have been limited to small case series, focusing on the arcade as an isolated cause of compressive ulnar neuropathy. The purpose of our study was to investigate the incidence of this structure in patients undergoing ulnar nerve transposition.
Methods:
A retrospective chart review of prospectively maintained data in a single surgeon’s practice was performed. Records of patients undergoing surgery for compressive ulnar neuropathy at the cubital tunnel were evaluated for documentation of a compressive arcade of Struthers. In addition, a scoping review of the literature was undertaken to better characterize current understanding of this structure and its recognition in clinical practice.
Results:
A total of 197 patients underwent ulnar nerve transposition. The overall incidence of a compressive arcade of Struthers was noted to be 67 out of 197 (34%). All patients with a compressive arcade were noted to have an internal brachial ligament running below the nerve. Patients undergoing revision surgery were found to have a compressive arcade 51% of the time (20/39), whereas 30% of patients undergoing primary surgery were found to have a compressive arcade (47/158). Only 12 clinical studies examining the arcade of Struthers have been published in the last 20 years, the majority being single case reports.
Conclusions:
Compression of the ulnar nerve by the arcade of Struthers is a common finding and can contribute to compressive ulnar neuropathy at the elbow both in primary and revision cases.
Introduction
Over the last decade, there has been continued interest and debate regarding the surgical treatment of ulnar nerve compression at the elbow. A PubMed search of “cubital tunnel syndrome” yields 316 results for the decade between 2003 and 2012 and 543 results for the decade between 2013 and 2022. Recent publications have focused on characterizing and classifying the severity of nerve compression using electrodiagnostic studies, and in nerve transfer procedures for the treatment of severe disease.1 -6 In comparison, little has been recently published on the debated topic of ulnar nerve compression at the arcade of Struthers, with most studies focused on cadaveric dissections and historical analysis.7,8
A meta-analysis of the current literature suggests that the majority of cadaveric studies that have examined the topic have identified “soft tissue structures” in the medial brachium forming an arcade over the ulnar nerve, with 2 of 3 structures—the medial intermuscular septum and the brachial fascia—being present in all cadavers. 8 However, studies describing this potentially compressive arcade have not consistently defined its constituent structures and anatomic boundaries, which may have contributed to the confusion over its existence. Although there is no consensus on a definition of the structure—an “arcade of Struthers” equivalent of “Osborne’s ligament”—studies cite the medial intermuscular septum, brachial fascia, and the internal brachial ligament as constituent structures.
The current clinical literature on the topic is comprised of case studies and small case series reporting isolated compression of the ulnar nerve by a proximal fibrous arcade.8 -13 However, no clinical reports specifically examining its incidence have been published. We report the incidence in our series of patients undergoing cubital tunnel surgery, wherein we specifically evaluated proximal to our typical expansive exposure (15-18 cm in length, centered at the medial epicondyle) to determine the presence of an arcade of Struthers requiring surgical decompression.14,15
Materials and Methods
Case Series
A retrospective chart review of all patients who underwent ulnar nerve transposition by the senior author (SEM) over a 6-year period (between January 2013 and December 2018) was performed. This study was approved by the Washington University School of Medicine Institutional Review Board (approval no. 201910175). Multiple data points were then extracted from the patient records, including patient demographics, preoperative examination findings, electrodiagnostic findings, and specific operative details. Preoperatively, all patients were examined for a Tinel sign at the cubital tunnel. In our practice, a sensory collapse test (SCT) is also performed in patients with a negative Tinel sign. Fisher’s exact test was used to perform statistical analysis of the two groups for categorical variables.
In the senior surgeon’s practice, submuscular ulnar nerve transposition with a flexor-pronator muscle slide is performed for all patients presenting with ulnar nerve compression at the elbow (procedure video available at https://surgicaleducation.wustl.edu/submuscular-ulnar-nerve-transposition/). 14 In revision cases, all patients are essentially converted to the senior surgeon’s primary procedure of a sub muscular transposition with step lengthening of the flexor-pronator origin. The ulnar nerve is first found proximal and distal to the original incision, and therefore the length of the incisions is longer in a revision surgery compared to a primary surgery (https://surgicaleducation.wustl.edu/revision-ulnar-nerve-transposition-following-failed-submuscular-ulnar-nerve-transposition/). 15 It is the practice of the senior surgeon to use a sterile tourniquet for all patients undergoing ulnar nerve transposition (both primary and secondary), and when the tourniquet is removed to examine for any proximal compression that might compress or kink the ulnar nerve. If a proximal compression is noted that cannot accommodate a fingerbreadth passage above the nerve, the incision is extended proximally and evaluation for an arcade of Struthers is performed and documented. During proximal exploration, we noted the presence of the medial intermuscular septum, brachial fascia, and internal brachial ligament. Specifically, we make a purposeful effort to run a finger proximal to the incision (which typically ends around 8 cm proximal to the medial epicondyle in primary surgeries) to palpate for the internal brachial ligament, which runs below the nerve, running obliquely on the surface of the medial triceps. The fibrous internal brachial ligament is easy to “hook” with a posterior directed finger as it runs obliquely across the soft muscle belly of the triceps.
Scoping Review
Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a systematic review of the literature was conducted using the search terms “arcade” and “struther” using the PubMed and Scopus databases. After replicates were removed, abstracts and then full-text articles were reviewed for inclusion. English language studies addressing clinical outcomes were included. Cadaver studies, studies which did not discuss arcade of Struthers, and review studies were excluded from the analysis.
Results
Case Series
One hundred ninety-seven patients underwent ulnar nerve transposition at the elbow by the senior author in the study period. Patient demographics are summarized in Table 1. There were no significant differences in the demographics of patients who underwent Struthers release as compared to the full cohort. The majority of patients in the study were men and middle aged (Table 1). In patients who had an internal brachial ligament present, passage of a digit along the course of the ulnar nerve was obstructed by this ligament passing obliquely posterior to the nerve. A tenotomy of the internal brachial ligament passing posterior to the nerve was performed at multiple levels, and the brachial fascia overlying the anterior surface nerve was decompressed. Finally, any adjacent residual medial intermuscular septum was excised. In all cases, the presence of the internal brachial ligament was key in rendering the arcade compressive, basically “closing” the loop between the confluence of the medial intermuscular septum and brachial fascia. The incidence of a compressive arcade of Struthers was 34% (67/197) in the study cohort. Patients who underwent Struthers release were more likely to have a positive sensory collapse in the medial arm (Table 2).
Patient Demographics.
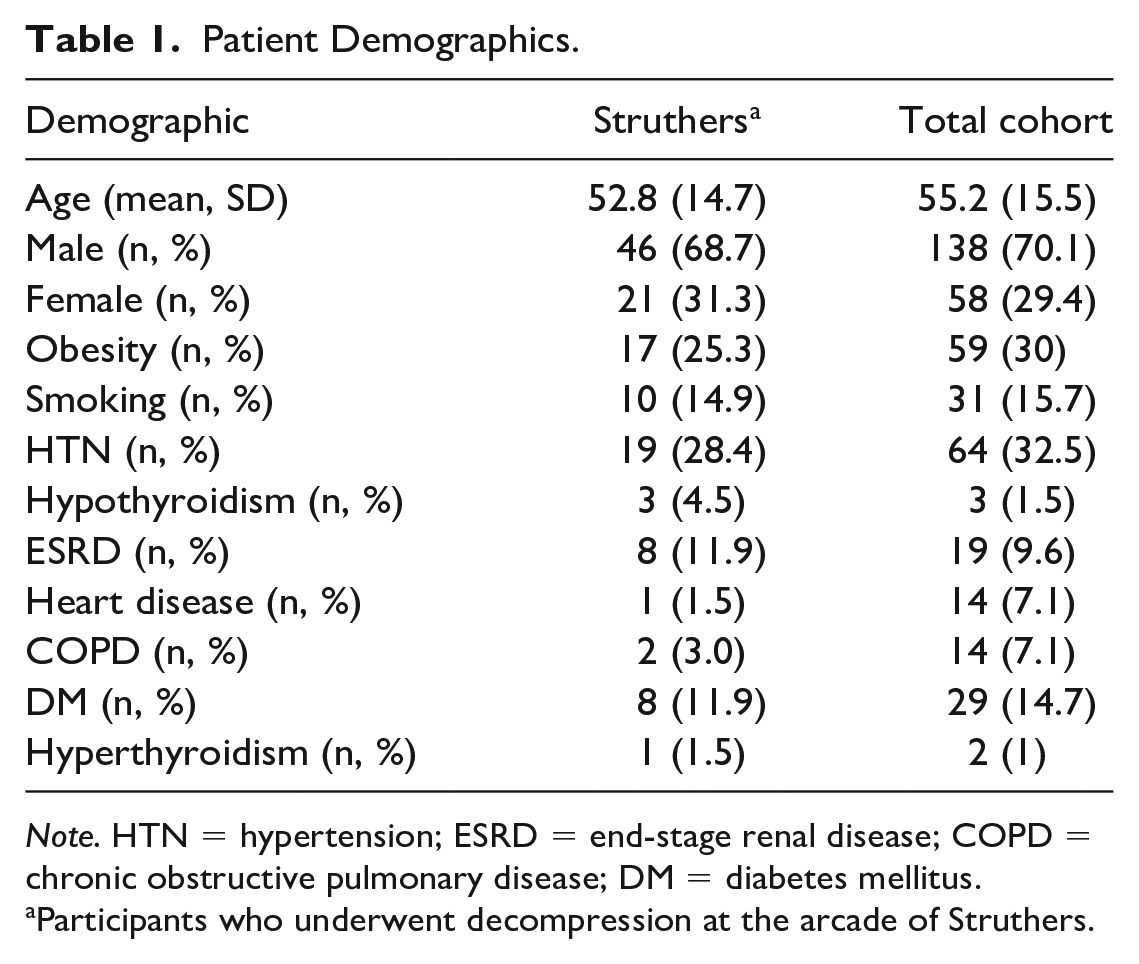
Note. HTN = hypertension; ESRD = end-stage renal disease; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus.
Participants who underwent decompression at the arcade of Struthers.
Preoperative Patient Characteristics.
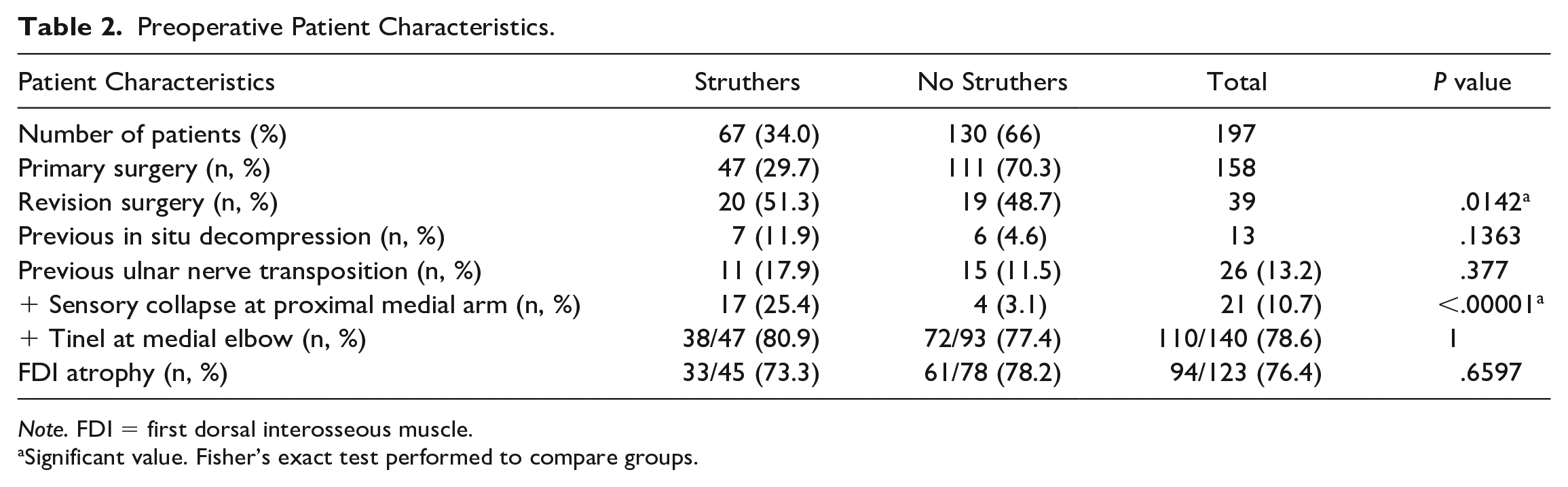
Note. FDI = first dorsal interosseous muscle.
Significant value. Fisher’s exact test performed to compare groups.
The majority of patients in the cohort underwent primary transposition, but 39 patients (19.8%) were referred for revision ulnar nerve surgery. A higher proportion of patients undergoing revision surgery (51%) had an arcade of Struthers, as compared to 30% of patients undergoing primary ulnar nerve surgery (20/39 revisions vs 47/158 primaries, 29.7%, odds ratio = 2.49 [95% CI, 1.22-5.08], P = .014). However, because most patients were undergoing primary transposition, although a lower proportion of them were found to have a compressive arcade, they still represented the majority of patients found to have an arcade of Struthers (47/67, 70.1%). Finally, patients with a positive sensory collapse at the medial arm were more likely to have a constrictive arcade of Struthers requiring release (25.4% vs 3.1%, P < .00001).
Scoping Review
One hundred nine records were identified using the PubMed and Scopus databases (Figure 1). Fifty-six full-text articles were reviewed for inclusion, and 12 were included in the final analysis (Table 3). The frequencies of study types are represented in Figure 2. Twelve clinical studies were included in the final analysis. Only 3 articles reported more than 2 patients, all of which examined the arcade as an isolated compressive structure. Two studies examined young athletes at risk of ulnar neuropathy at the elbow.16,17 Kawabata et al 16 found that tenderness at the arcade of Struthers was associated with ulnar nerve displacement with throwing. Noda et al 17 compared 20 asymptomatic baseball players to 20 players with symptoms of ulnar neuropathy, and utilized ultrasound to determine the cross-sectional area of the ulnar nerve at various compression points in both upper extremities (throwing and nonthrowing side). They found the ulnar nerve to be more swollen at the arcade of Struthers on the throwing side of symptomatic participants compared to participants without ulnar neuropathy. There was no difference in cross-sectional area of the ulnar nerve on the nonthrowing side between the symptomatic and asymptomatic groups. Gao et al 18 conducted a retrospective analysis of 56 patients with ulnar neuropathy—all evaluated by ultrasound—and reported two patients with isolated compression by the arcade of Struthers.
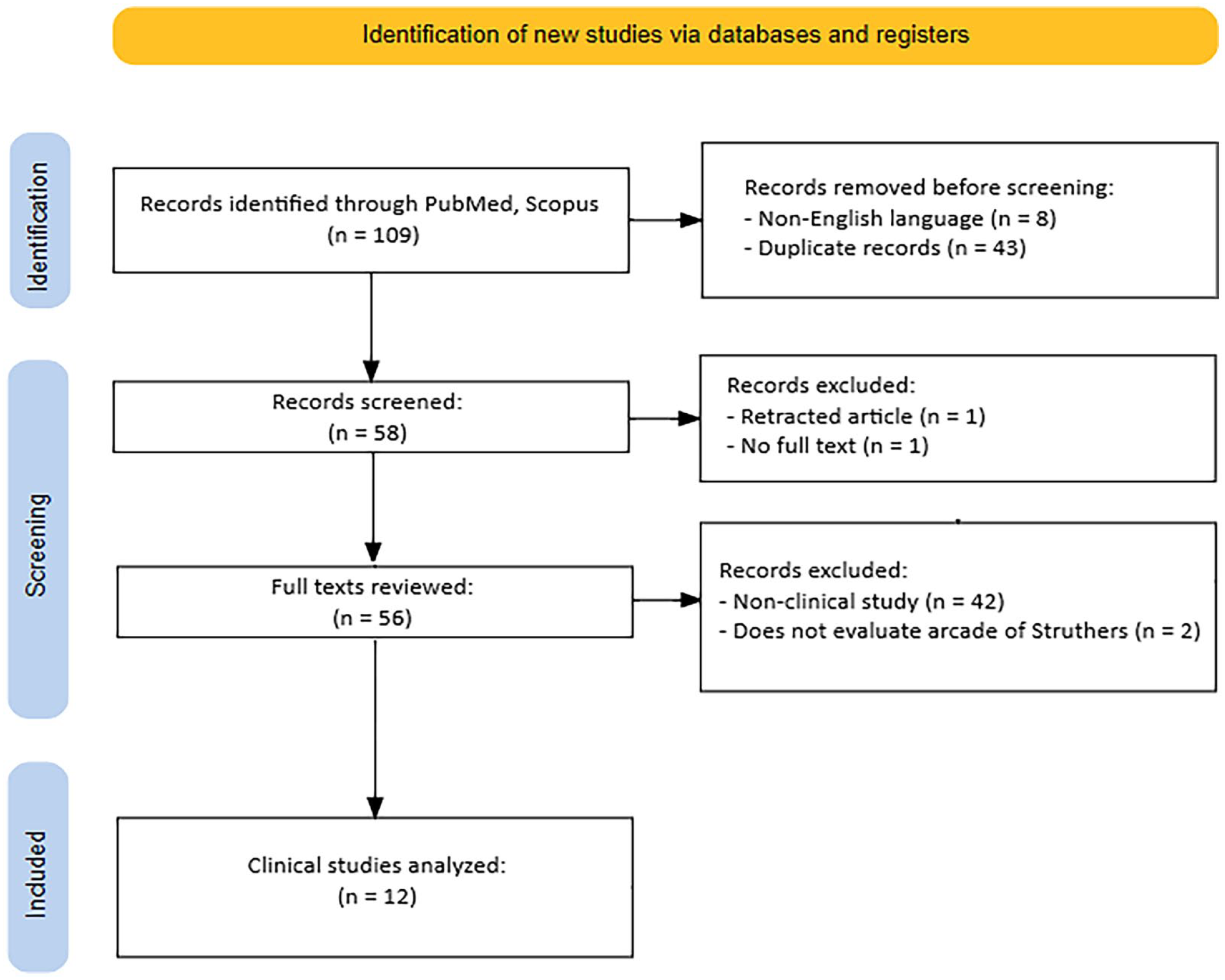
Scoping review flow diagram.
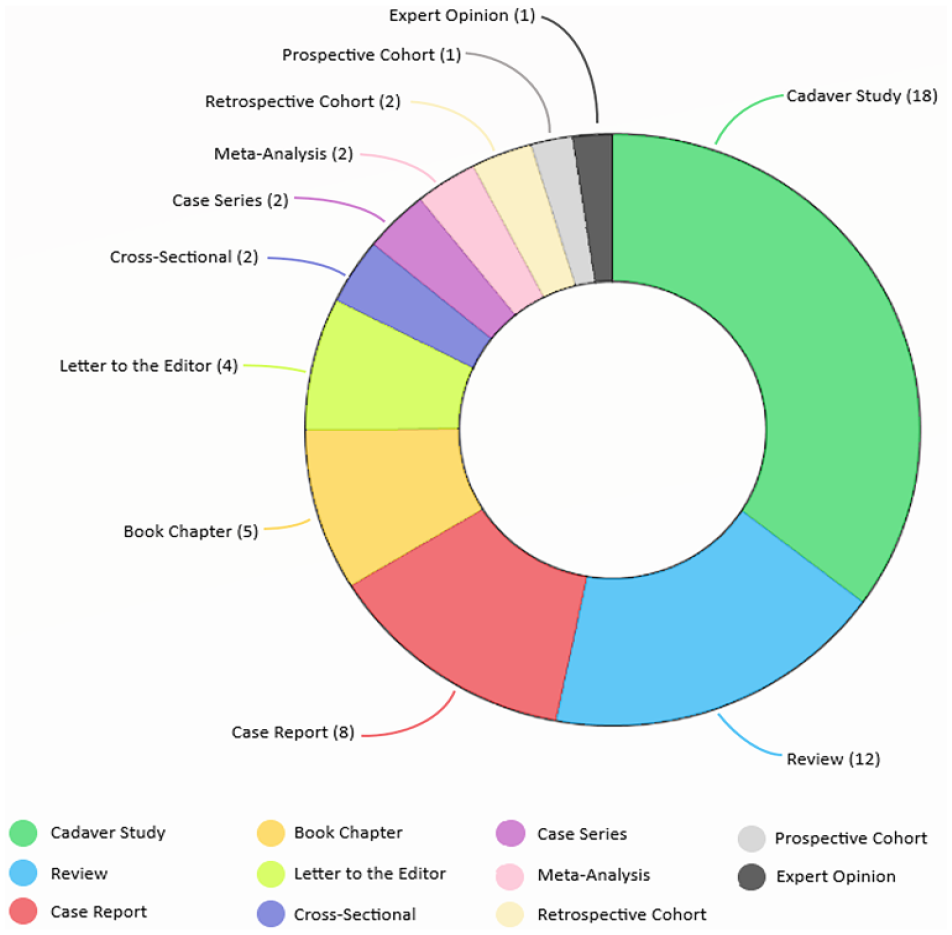
Breakdown of articles identified by systematic review.
Summary of Results of Scoping Review.
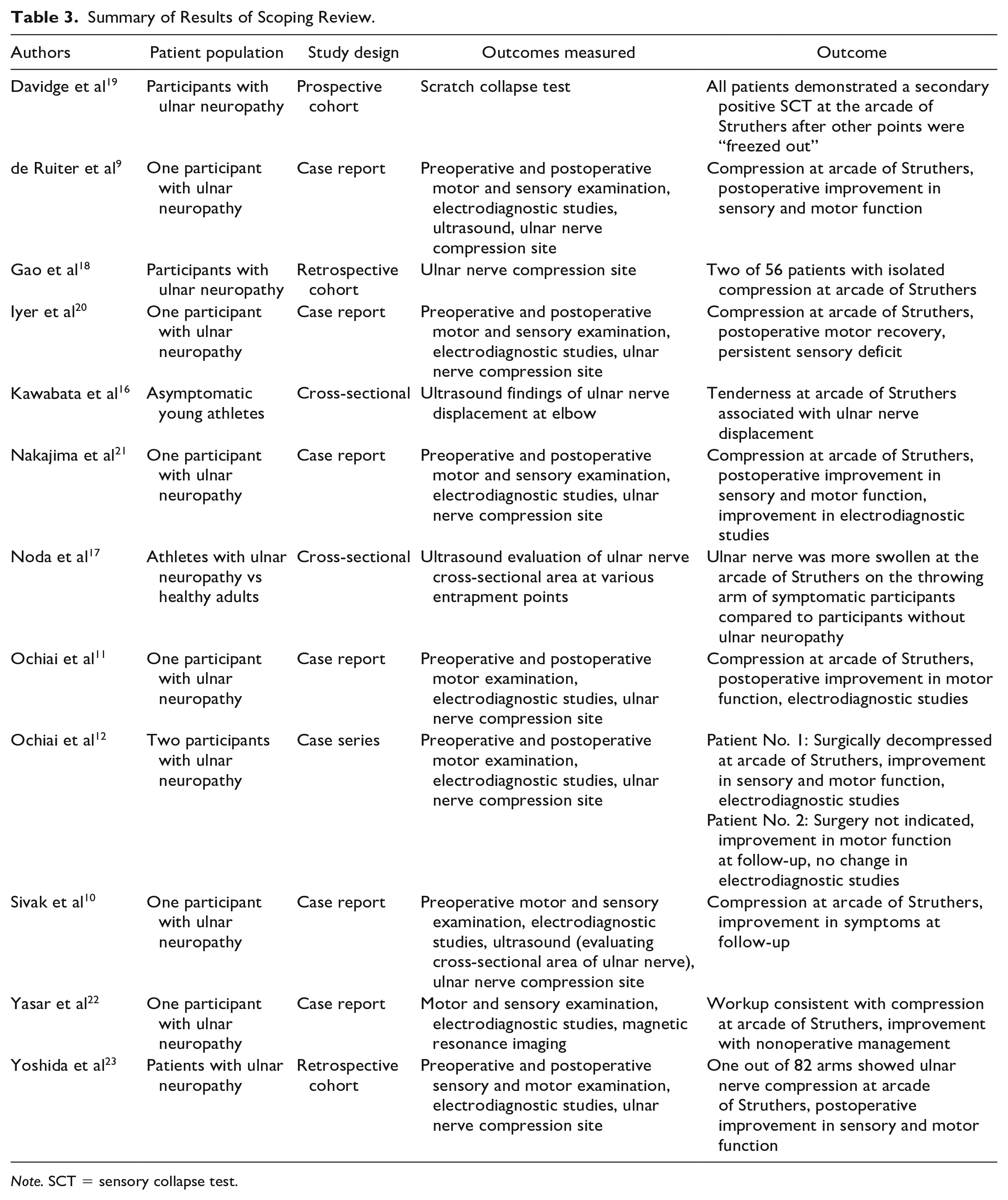
Note. SCT = sensory collapse test.
Discussion
The etymology, and indeed existence, of the arcade of Struthers has been debated for several decades.7,13 In a foundational textbook first published in 1988, it was stated that: In our personal series of more than 500 ulnar nerve explorations, a discrete arcade of Struthers has never been identified. However, in patients who have previously had an anterior transposition and who have failed to improve, the surgical re-exploration clearly shows an ulnar nerve being tethered proximally and usually about 8cm proximal to the medial humeral epicondyle by the fascia already described, which runs from the medial head of the triceps to the medial intermuscular septum.
24
Since then, this view has been widely disseminated. Notably, the internal brachial ligament was not mentioned in this series, and use of a nonsterile tourniquet in the 1980s precluded proximal extension of the dissection. However, over the last three decades, with routine use of a sterile tourniquet, the senior author has noted this discrete structure in many patients in her clinical practice, and has made examination for a compressive arcade of Struthers, with proximal exploration of the ulnar nerve, a routine.
This practice of specific proximal exploration largely developed due to an unrelated phenomenon—the increasing incidence of obesity, and the senior author’s move to the Midwest of the United States. Due to the conical shape of the upper arm in obese patients, nonsterile tourniquets obstruct access to the typical incision needed to evaluate the arcade, especially in revision surgery. By contrast, when removing the tourniquet, it is possible to palpate more proximally, to extend the incision as needed, and evaluate for the presence of a proximal compressive band around the ulnar nerve. This proximal exposure also allowed the senior surgeon the opportunity to clearly observe the fascial anatomy around the ulnar nerve at this level.
Multiple definitions of the anatomic band exist, without consensus on the contributions of different soft tissue structures to the arcade.25 -28 In our experience, this compressive arcade is dependent on the confluence of three structures, with the presence of the internal brachial ligament posterior the nerve being critical in completing the loop around the nerve, rendering the overlying medial intermuscular septum and brachial fascia compressive. The internal brachial ligament separates from the medial intermuscular septum near the coracobrachialis, intimate with the medial triceps muscle, running diagonally in a plane posterior to the ulnar nerve to rejoin the septum just proximal to the medial epicondyle.25,29 Second, the medial intermuscular septum runs anteriorly and lateral to the ulnar nerve. Finally, the brachial fascia invests the triceps muscle laterally and runs anterior to the nerve, attaching to the medial intermuscular septum. Thus, it is the presence of the internal brachial ligament as a static and dynamic (as it moves with the triceps muscle) compressive structure that renders the other two structures compressive to the ulnar nerve. When examining the proximal arm intraoperatively, a focus is now placed on using a finger to palpate deep and lateral to the nerve, which will demonstrate the presence of the narrow, oblique, tendinous internal brachial ligament on the triceps muscle, coursing posterior to the nerve.
Kane et al, who were first to describe this arcade, attributing it to John Struthers, stated that it is formed by a “thickening of the deep investing fascia of the distal arm, by superficial muscular fibers of the medial head of the triceps, and by attachments of the ‘internal brachial ligament.’”27 -29 Tubbs et al performed dissection of 15 cadavers and defined a soft tissue thickening in the medial inferior arm “crossing” the ulnar nerve in 86.7% of cases. 30 In this study, multiple structures were seen as potential contributors, including the internal brachial ligament, the brachial fascia, and the medial intermuscular septum. 30 These authors devised a classification system based on the structure that was considered most compressive in each cadaver. 30 They found the internal brachial ligament to be the primary contributor to a compressive arcade in only 19.2% of cadavers, whereas the brachial fascia was deemed most compressive in 57.7% of the arms, and the medial intermuscular septum in 23.1%. 30 The contrast between our findings may be due to the authors’ approach of describing a static compressive structure. In our experience, the arcade of Struthers is a dynamic structure that requires the presence of all three constituents. It is the movement of the internal brachial ligament on the medial triceps that renders the other two structures compressive.
Caetano et al 31 dissected 40 limbs, identifying a “fibrous tunnel” under which the ulnar nerve passed in 100% of cadavers. They defined the arcade as:
. . . a fibrous canal on the medial aspect of the middle- and lower-third of the arm, consisting of the medial head of the triceps brachii and its aponeurotic expansion, which extends into the intermuscular septum, and internal brachial ligament . . .
They also noted that the ulnar nerve at times runs under the triceps muscle itself, and at other times under its “aponeurotic expansion.” Finally, they note that, proximally, a fascial band between the intermuscular septum and internal brachial ligament can form the roof of the tunnel. 31
In contrast, Dellon reported on cadaver dissections of 104 upper extremity specimens in which he was unable to identify a structure corresponding to the arcade of Struthers, and noted anecdotally that: Our personal observation in more than 300 cubital tunnel surgeries is that we have not yet encountered a discrete fibrous band in this location, proximal to the elbow, as a source of ulnar compression neuropathy.
32
Similarly, Bartels et al demonstrated how the technique of fascial dissection can “create” a fibrous fascial band that can be called an arcade, but contend that this is a biproduct of the method of cadaveric dissection and not clinically relevant. 31 However, unlike the ligament of Struthers, the arcade of Struthers, as described by Kane et al, is not a discrete fibrous band, but a confluence of structures that together can serve as a point of dynamic compression.
In addition to cadaveric studies,31,21,33 -35 several case studies have reported isolated compression of the ulnar nerve proximal to the cubital tunnel in untraumatized and unoperated arms. De Ruiter et al reported a case of a patient who presented with symptoms and signs of cubital tunnel syndrome that were not supported by electrodiagnostic studies or ultrasound of the elbow. 9 This patient was found to have a compressive muscular arcade in the distal arm, which was noted on ultrasound examination. 9 Sivak et al 10 reported a patient with severe ulnar neuropathy on clinical examination, localizing by conduction block and ultrasound changes approximately 8 cm proximal to the medial epicondyle. Ochiai et al11,12 reported three cases of ulnar nerve entrapment in the middistal brachium that were localized by electrodiagnostic findings, and reported symptom improvement with release of an arcade of Struthers alone in two patients. In addition, in a retrospective analysis of endoscopic cubital tunnel release, Yoshida et al 23 noted only 1 of 84 patients who had a proximal point of compression requiring release.
In secondary cases, although the primary site of compression is often located distally, proximal compression has frequently been reported in a proportion of these patients.36,37 Gabel and Amadio also noted a high rate (>50%) of compression by an arcade of Struthers in a series of revision ulnar nerve surgeries. 37 In personal communication, Robert J. Spinner has also noted a higher incidence of compressive arcade of Struthers in reoperative patients and posttraumatic ulnar neuropathy. Other reports have suggested that proximal kinking of the nerve can be caused by unreleased proximal fibrous structures only in cases of transposition.32 -34,38,39 However, contrary to what has been previously suggested, this structure was also found in patients who had previously only had an in situ decompression (7/67, 11.9%), and in previously unoperated arms (47/67, 70.1%).
The medial intermuscular septum and the deep brachial fascia have long been discussed in isolation as potentially compressive structures of the ulnar nerve.24,39 In fact, a “compartment syndrome” of the median and ulnar nerves in the arm has been described as a cause of severe neuropathy.40,41 We propose it is the interaction of the three structures—the medial intermuscular septum, brachial fascia, and internal brachial ligament, when present—creating the distinct compressive entity: the arcade of Struthers (Figure 3). We suggest that the internal brachial ligament lying posterior to the ulnar nerve renders the other two ubiquitous structures compressive as it “closes the loop” around the ulnar nerve.
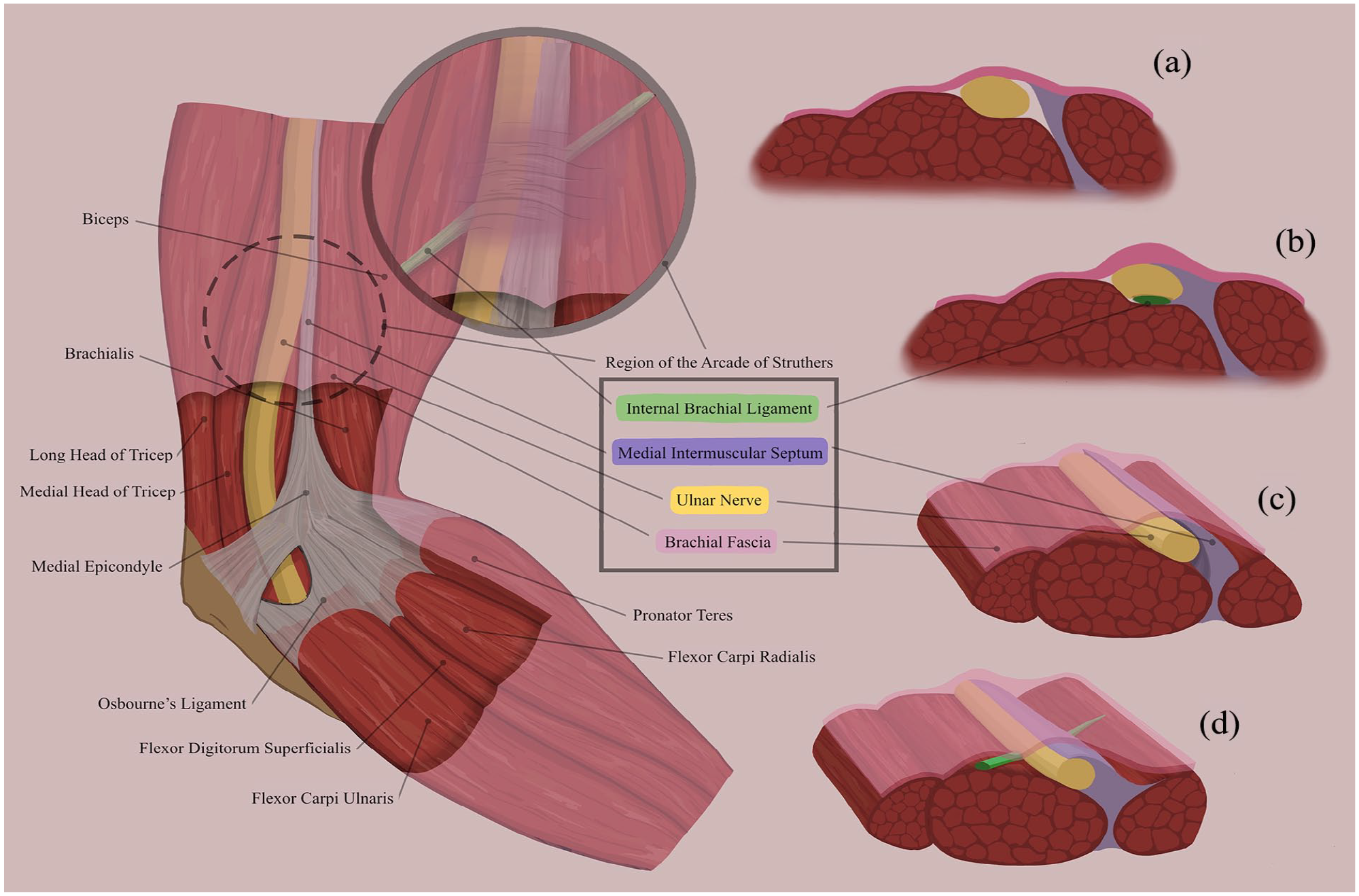
The region of the arcade of Struthers is unique in respect to the relationship of the brachial fascia, the medial intermuscular septum, and the internal brachial ligament.
Specifically, at the conclusion of each case, after we remove the tourniquet, we palpate proximally along the ulnar nerve, and when the internal brachial ligament is present, a significant compression is easily recognized with a discrete tendinous band posterior to the ulnar nerve, running obliquely on the medial triceps muscle lateral to and below the ulnar nerve. We previously “missed” this compression point as our dissection did not include this proximal evaluation, and we were not methodically looking for the arcade prior to the 1980s. Preoperatively, this structure can be anticipated with tenderness to palpation along the nerve proximal to the medial epicondyle, and with an SCT, if that test is part of the surgeon’s clinical examination. 42
The SCT, formerly known as the scratch collapse test, is a provocative test, similar to Tinel’s, Phalen’s, or pressure provocative test. Like other unusual reflexes (eg, cremasteric), the SCT is a spinal reflex. It is in response to an area of potential nerve compression where substance P is increased, stimulating the nociceptive Schwann cells around the previously considered free nerve endings and resulting in a withdrawal reflex with sensory stimulus such as touch, scratch, or even wind over the area of consideration. 43 When performed correctly, as described by Kahn et al, the SCT can confirm the presence of a conduction block in a patient with normal electrodiagnostic studies indicating Sunderland 0 injury.
A Tinel sign is usually not elicited over the arcade. However, a pressure provocative test can be positive. Just as the medial intermuscular septum may “kink” the ulnar nerve with transposition surgeries, so too can the arcade of Struthers. It is our opinion that the additional time and extension of the incision required to evaluate for the presence of an internal brachial ligament specifically are warranted. The ligament, if present, is seen adjacent to the nerve running with a vascular leash. Using a finger, it can be palpated as a distinct tendinous band coursing from lateral to medial posterior to the nerve about 10 cm proximal to the medial epicondyle.
In closing, we acknowledge seminal articles by Kane et al and Spinner and Kaplan in 1973 and 1976 as important observations on the arcade of Struthers.27,28 It will only be identified with a purposeful effort to palpate proximally. If only the overlying brachial fascia and medial intermuscular septum are released, and the internal brachial ligament is not released, then the internal brachial ligament will remain as a possible dynamic point of compression on the ulnar nerve.
Footnotes
Ethical Approval
This study was approved by the institutional review board of Washington University School of Medicine.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional) and with the Helsinki Declaration of 1975, revised in 2008.
Statement of Informed Consent
Informed consent was waived due to the retrospective nature of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.