
Abstract
Background:
Concomitant carpal injuries with dislocations and fracture-dislocations of the carpometacarpal joints (CMCD/FD) are often hard to see on plain radiographs, making advanced imaging a useful diagnostic adjunct. We aim to: (1) characterize bony injury patterns with CMCD/FD; and (2) determine the frequency that preoperative computed tomography (CT) scans change surgical management.
Methods:
A retrospective review was performed of patients who underwent operative fixation of CMCD/FD from 2006 to 2021. X-ray and CT scan diagnoses were reviewed and correlated to intraoperative findings and procedures performed. Statistical analyses were performed to evaluate the frequency in which CT scans changed management and the frequency of new intraoperative diagnoses.
Results:
Seventy-five patients were identified. All patients had a preoperative x-ray, and 27 patients (36%) additionally had a CT scan. Patients who sustained high-velocity trauma were significantly more likely to obtain a CT scan than patients with low-velocity trauma (P = .019); however, the number of additional diagnoses was not significantly associated with trauma velocity (P = .35). Computed tomography scans significantly increased the number of diagnoses (P < .001) and changed operative management in 58% of cases. Six of the 48 patients (12.5%) that did not receive a CT scan had new intraoperative diagnoses, which changed the procedure for five of these patients. New intraoperative diagnoses were identified significantly more when patients did not have a CT scan (P = .04).
Conclusions:
Obtaining a CT scan in CMCD/FD patients changed the patient’s diagnosis at a significant rate and changed operative management roughly half of the time. The authors recommend routine CT scans be obtained in patients with CMCD/FD.
Keywords
Introduction
Carpometacarpal dislocations (CMCDs) and carpometacarpal fracture-dislocations (CMCFDs) are relatively rare injuries, comprising less than 1% of all hand trauma.1,2 These dislocations are often unstable even after reduction, and operative fixation is recommended to restore preinjury anatomy and function. 3 If left untreated, CMCFD can result in diminished grip strength, posttraumatic arthritis, nonunion, and joint instability.2,4
Carpometacarpal fracture-dislocations are commonly diagnosed by plain film, with several techniques described in the literature to optimize diagnostic sensitivity.5,6 Concomitant carpal injuries have been reported, but due to the osteology of these bones, they are often hard to see on plain radiographs, with up to a 50% reported discrepancy in diagnosis between radiographs and computed tomography (CT).7 -9
The purpose of this study is to determine whether CT scans change the diagnosis or management of patients with CMC dislocations and CMCFDs at a significant rate. We hypothesized that obtaining a CT scan would change both the diagnoses and the operative management of CMCFD patients in a significant proportion of cases due to recognition of injuries that would be missed on plain films.
Methods
After hospital institutional review board approval, a retrospective review was conducted for all patients who received care at a single institution in the last 15 years (2006-2021). Patients were identified using the Epic tool SlicerDicer by Current Procedural Terminology codes 26670, 26675, 26676, 26685, or 26686. Patients younger than 16 years were excluded. We additionally excluded patients with mangled extremities, as well as those who proceeded for emergent operative treatment (such as in the case of vascular injury) that would have precluded obtaining advanced imaging prior to the operation.
Demographic data were collected including age and sex, as well as clinical information pertaining to the date, mechanism, and laterality of injury. Imaging reports and clinical images of x-rays and CT scans were reviewed. Any discrepancy between report and imaging was adjudicated by the senior author (K.H.). Information pertaining to surgery, such as intraoperative findings and procedures performed, was collected from operative reports. Medical records were further reviewed for postoperative management, including postoperative immobilization protocols. Mechanisms of injury were classified as either high-velocity or low-velocity mechanisms (Table 1). Of note, fall from height was characterized as a low-velocity mechanism, as no fall was from greater than 15 feet. All data were stored on a secure REDCap database.
Demographic Data.
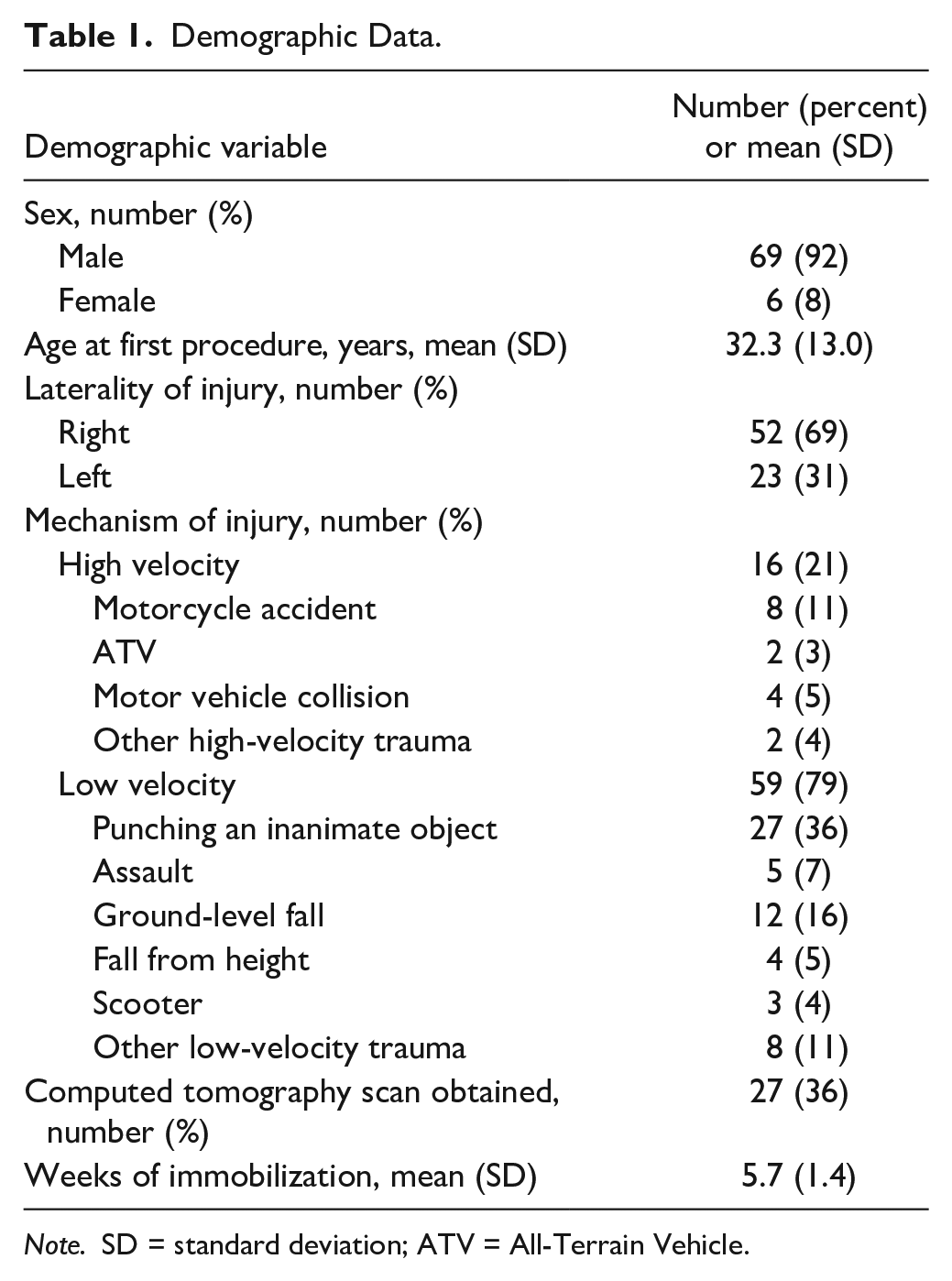
Note. SD = standard deviation; ATV = All-Terrain Vehicle.
Data were analyzed using IBM SPSS Statistics for Windows, version 28.0. 10 Descriptive statistics were used to evaluate patient, injury, and surgical characteristics. Chi-square tests of independence and Fisher’s exact tests were utilized to compare diagnoses found via x-ray versus CT scan. Group injury patterns and changes in treatment management when new diagnoses were made from CT scan were evaluated using logistic regression. Statistical significance was considered at the P < .05 level.
Results
A total of 75 patients were identified. Most patients were male (92%), and the average age was 32 years. All patients had a preoperative x-ray of the affected hand, and 27 patients (36%) additionally had a CT scan. Demographics are described in Table 1. Roughly 80% of our patients sustained their injuries in a low-velocity trauma. Patients who sustained high-velocity trauma were significantly more likely to have had a CT scan preoperatively than patients who sustained low-velocity trauma (P = .019). Most common mechanisms of injury for patients who received a CT were motorcycle accidents (26%), punching inanimate objects (26%), ground-level fall (15%), fall from height (11%), or other low-velocity trauma (11%). In comparison, those that did not receive CT scans had mechanisms of injury that were generally of lower velocity, including punching an inanimate object (41%), ground-level fall (17%), and assault (10%). Most patients in the sample sustained a CMCD/FD of the small finger (20% for dislocation/59% for fracture-dislocation) and/or ring finger (12%/41%, respectively) (Table 2).
X-Ray and Computed Tomography Diagnoses.
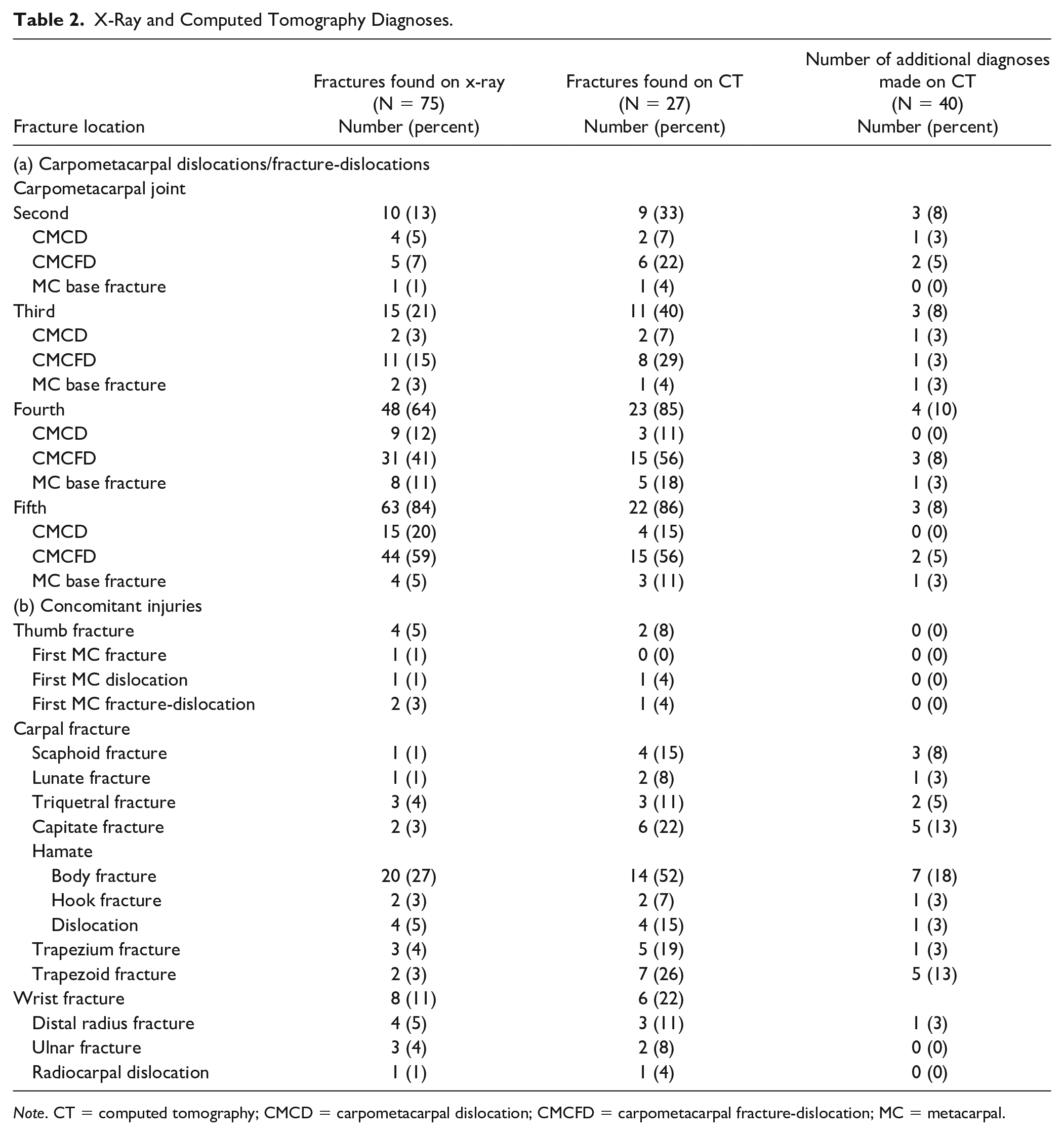
Note. CT = computed tomography; CMCD = carpometacarpal dislocation; CMCFD = carpometacarpal fracture-dislocation; MC = metacarpal.
The most common concomitant injuries in CMCFDs of the wrist were CMCFDs of the other digits and carpal bone fractures (Table 2). There were a number of injury patterns that were apparent in our cohort (Figure 1). Of the patients who sustained CMCD/FD of the small finger, 59% also sustained a CMCD/FD of the ring finger, and 50% sustained a hamate fracture (Figure 1a). Patients with a CMCD/FD of the ring finger were also likely to sustain CMCD/FD of the small finger (96%) or hamate fractures (80%) (Figure 1b). Patients who sustained CMCD/FD of the index and long fingers were more likely to have sustained a high-velocity trauma than patients with isolated fourth and/or fifth carpometacarpal joint (CMCJ) injuries (64% and 57% vs 13% and 13%, respectively, P < .001). Accordingly, patients with a CMCD/FD of the long finger had significantly more concomitant injuries on average than patients with a CMCD/FD of the fourth and fifth CMCJ (P = .003 and <.001, respectively), and patients with a CMCD/FD of the index finger had significantly more concomitant injuries than patients with a CMCD/FD of the fifth CMCJ (P = .02). Patients with a CMCF/FD of the long finger were likely to present with CMCF/FD of the index (42%), ring (75%), and small (50%) fingers, as well as hamate (58%) and trapezoid (50%) fractures (Figure 1c). Similarly, fracture-dislocation of the second CMCJ often presented with fracture-dislocation of the third and fourth CMCJs (86% and 71% of patients, respectively) and, less commonly, the fifth CMCJ (29% of patients), as well as trapezoid (71%), hamate (43%), lunate (29%), and trapezial (29%) fractures (Figure 1d).
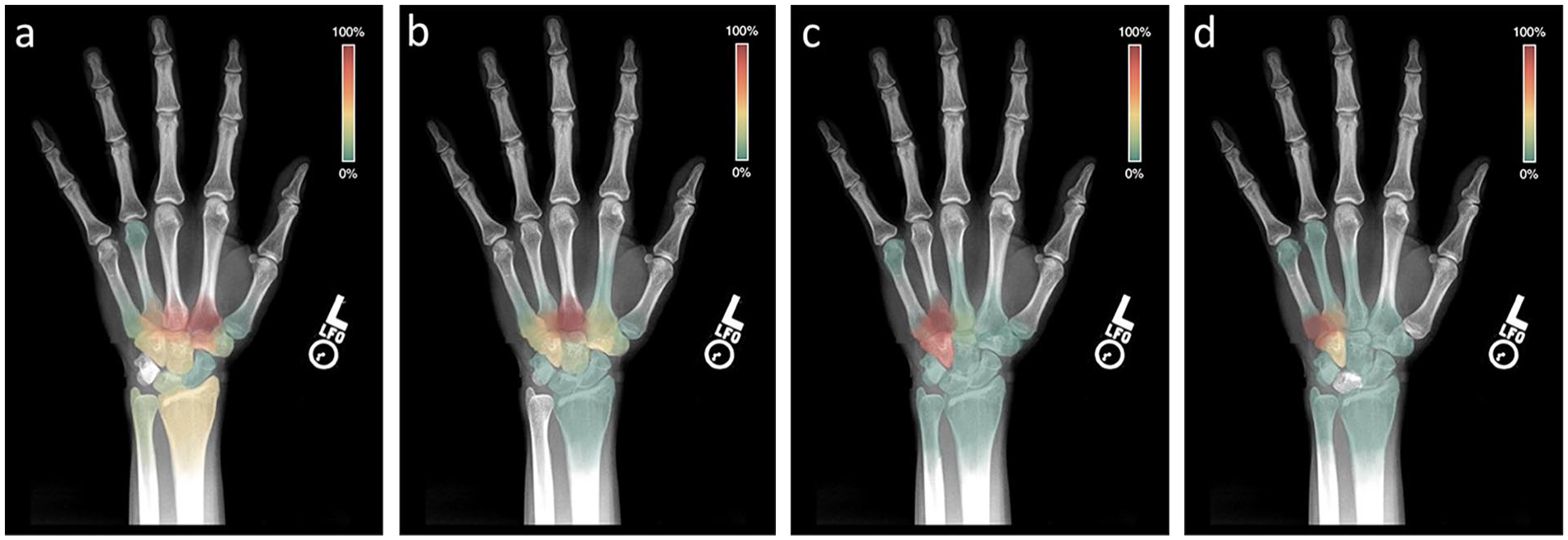
Heat map demonstrating the frequency of associated concomitant injuries with a (a) small finger carpometacarpal joint dislocation/fracture-dislocation (CMCD/FD), (b) ring finger CMCD/FD, (c) long finger CMCD/FD, and (d) index finger CMCD/FD.
Computed tomography scans significantly increased the overall number of diagnoses, χ2 (1, N = 211) = 206.88, P < .001, with 40 additional diagnoses made by CT that were not seen on plain films (Table 2). Nineteen patients (70.4%) who got a CT scan obtained a new diagnosis. The number of additional diagnoses found on CT did not change significantly by velocity of injury mechanism (P = .35). The most clinically significant of these additional diagnoses included 10 additional CMCD/FD, 3 additional scaphoid fractures, and 1 additional hook of hamate fracture. A CMCD/FD of the ring and small fingers significantly changed the odds of having a carpal fracture such that the odds of having any carpal fracture were 5.33 times greater with ring finger CMCD/FD (B = 1.67, SE = 0.51, P = .001) and 0.23 times less with a small finger CMCD/FD (B = −1.46, SE = 0.71, P = .04). In addition, CMCD/FD of the long finger trended toward significance, such that the odds of having any carpal fracture was 3.15 times greater when patients had this injury (B = 1.15, SE = 0.65, P = .08). Patients who sustained high-velocity trauma were significantly more likely to have trapezial, trapezoid, and hook of hamate fractures than our low-velocity injury cohort (P = .006, .004, and .043, respectively).
Of the 19 patients who had newly diagnosed injuries on CT scan, 58% had changes in their operative plan to treat the additional injuries. The probability of the procedure changing with additional CT diagnoses trended toward significance such that the odds of the procedure changing was 7.33 times greater when the patients had a new diagnosis (B = 2.00, SE = 1.17, P = .09). In addition to the clinically significant CMCD/FD, scaphoid fractures, and hamate hook fracture mentioned earlier, 3 hamate body fractures and 3 trapezoid fractures were addressed intraoperatively. While the procedure for these patients changed, the length of postoperative immobilization was not significantly affected (P > .5). For the 48 patients that did not receive a CT scan, a new intraoperative diagnosis was made in 6 patients (12.5%), which changed the procedure for 5 of these 6 patients. These diagnoses included 2 capitate fractures, a scaphoid fracture, a hamate fracture, a lunate dislocation, a trapezial dislocation, and 3 additional CMCD/FDs. Significantly more new intraoperative diagnoses were identified when patients did not have a CT scan, χ2 (1, N = 75) = 3.97, P = .04.
Discussion
Dislocations and fracture-dislocations of the CMCJs are uncommon, occurring at an incidence of 0.2% to 1% of all hand injuries. 4 These injuries are typically due to either high-velocity injuries such as motor vehicle accidents or delivering a blow with a closed fist. 11 Due to its relative mobility and decreased stability as compared to the more radial CMCJs, the small finger CMCJ is most frequently involved in single-digit CMCJ dislocations as well as 80% of multiple-digit dislocations and typically presents with dorsal dislocation. 12 The most common pattern of a multi-digit injury is a combined fourth and fifth CMCD/FD, and common concomitant injuries include fourth and/or fifth metacarpal base fractures and hamate fractures. 11 X-ray findings for these injuries include loss of parallelism of the articular spaces, overlapping articular surfaces, and indistinct cortical rims. 13 One method of fracture detection involves the use of metacarpal cascade lines, which are superimposed lines through the longitudinal axis of the metacarpals that normally converge at a point 2 cm proximal to the distal radius articular surface. A lack of convergence of these lines suggests CMCJ injury. 6
The treating physician must have a high index of suspicion for this injury as they can frequently be missed, and delayed diagnosis can result in substantial dysfunction and worse surgical outcomes. 2 There is no consensus on the use of advanced imaging for characterization of potentially operative concomitant injuries in the setting of CMCD/FD. Previous studies have shown that the sensitivity of x-ray for diagnosis of concomitant carpal injuries is lacking, with up to 50% of initial wrist injuries being undiagnosed with plain films.7,8 These findings suggest that CT is a useful adjunct if there is clinical suspicion for additional injury.
This study aims to answer the question: Is obtaining a CT scan in a patient with a CMCD/FD likely to change that patient’s management? We demonstrate that one should have a high suspicion for concomitant injuries in both low- and high-velocity mechanisms that cause a CMCD/FD in the hand. In comparison to plain films alone, obtaining a preoperative CT scan frequently led to new bony injury diagnosis and changed operative management just over half of the time. These diagnoses ranged from fractures and fracture-dislocations of surrounding metacarpals to fractures of the carpal bones. These findings suggest that CT scans are a useful adjunct to identify clinically relevant injuries in patients with CMCD/FD, even in the setting of low-velocity trauma. In particular, damage to the second and third CMCJ was associated with a high proportion of concomitant injuries, suggesting that injuries capable of disrupting these highly stable joints are likely to damage other surrounding structures and should thus be investigated more thoroughly.
More investigation is required to discern which other clinical or injury factors can predict the utility of a CT scan for this injury. A larger sample size would help discern this and better characterize the different injury patterns depending on the involved digit for a CMCD/FD. The study is additionally limited by the retrospective nature of the study. Because CT scans were presumably obtained when the suspicion for missed injury was high, it is more difficult to draw a conclusion regarding whether a CT scan should be obtained when degree of suspicion for a concomitant injury is low. However, the rate of new diagnoses made during surgery for patients with only plain films suggests that more routine cross-sectional imaging may be of benefit in preoperative planning. Future work should include an increased sample size and potentially a prospectively collected cohort.
Conclusion
Obtaining a CT scan in CMCD/FD patients changed the patient’s diagnosis at a significant rate and changed operative management 58% of the time. The authors recommend routine CT scans be obtained in patients with CMCD/FD.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). A waiver of informed consent was obtained from our university institutional review board for this study.
Statement of Informed Consent
A waiver of informed consent was obtained from our university institutional review board for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.