
Abstract
Background:
Outcomes for routine hand procedures, such as carpal tunnel release, trigger finger release, and first dorsal compartment release, are typically reported as “highly successful” with “infrequent complications” based on classic literature. No contemporary study has utilized a large prospective registry to assess patient willingness to repeat surgery. We utilized a prospective hand registry to evaluate the proportion of patients that would repeat surgery after common hand procedures.
Methods:
We utilized a prospective, hand surgery registry to collect postoperative patient likelihood to repeat surgery in patients undergoing surgery for 9 common hand procedures. All measures were reported at 12, 24, or 52 weeks. We analyzed the percentage of patients that would repeat the procedure for all diagnoses, as well as stratified by the most common 9 isolated diagnoses.
Results:
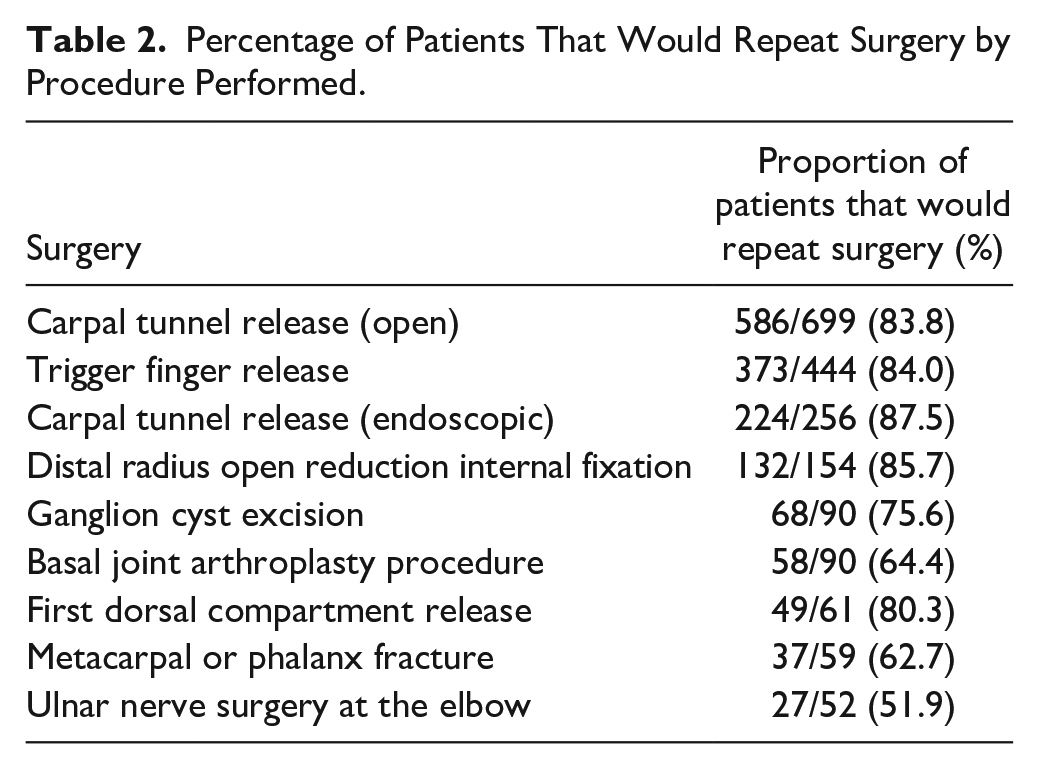
At the time of analysis, 1905 patients met our inclusion criteria. The average percentage of patients across all procedures that would repeat surgery was 81.6%. When stratified by the most common 9 diagnoses the percentage of patients that would repeat surgery ranged from 51.9% (ulnar nerve surgery at the elbow) up to 87.5% (endoscopic carpal tunnel release).
Conclusions:
After undergoing routine hand procedures, a significant percentage of patients would choose not to repeat surgery. Hand surgeons can do better in setting clear and realistic preoperative expectations when counseling patients prior to even routine hand surgeries.
Keywords
Introduction
Healthcare quality has become an increasingly important metric across surgical specialties, including hand surgery. 1 The definition of healthcare quality has evolved over time, with the current paradigm largely built upon the Institute of Medicine’s framework for patient-centered care that is responsive to individual patient preferences, needs, and values. 2 Multiple authors have articulated the need to further define quality within the unique context of hand surgery.3,4 A variety of patient-reported outcome measures (PROMs) have been employed to this end, but each has its own defined minimal clinically important difference, which are unique for particular pathologies.
A frequently used surrogate for quality has been patient-reported satisfaction, despite being an imperfect solution to measuring quality. Previous literature has noted that patient satisfaction is a complex goal which can be affected not only by the technical expertise of the surgeon, but also pain, function, psychosocial factors, and even the cost of parking. 1 Patient-reported likelihood to repeat surgery is another valuable metric which focuses the patient’s evaluation on whether their preoperative expectations of the surgery align with outcomes. It takes into account not only the final outcome, but also the course taken to reach that point. A procedure might provide patients with pain relief and return of function, but if it required years of therapy and months of missed work that were inconsistent with preoperative expectations, patients may not choose to repeat the surgery. It is important to make the distinction that quality encompasses more than simply the technical skill of the surgeon in performing a procedure. A technically perfect surgery with no complications might still result in a patient who would not repeat surgery if the patient still has functionally limiting symptoms afterwards.
Preoperative patient expectations can also significantly affect final satisfaction and can confound the interpretation of PROMs.5-7 These complexities mean that research is all the more warranted to better understand and measure patient satisfaction. Satisfaction rates after common hand procedures are notably lacking in the published literature, perhaps because the definition of satisfaction is not lucid. However, asking patients the likelihood that they would repeat surgery encompasses a variety of objectives closely related to satisfaction. Therefore, we set out to prospectively quantify a single aspect of patient satisfaction after elective hand surgery by asking patients their likelihood to repeat surgery at multiple time points postoperatively. The purpose of this study is to quantify and better understand how closely patients’ preoperative and postoperative expectations align during recovery after common hand procedures as measured by their likelihood to repeat the surgery.
Materials and Methods
We developed an automated system for digitally collecting PROMs which can be integrated into a clinical practice with minimal time investment (SurgiSurvey, LLC). After undergoing surgery, patients were emailed through a Health Insurance Portability and Accountability Act (HIPAA)-compliant web server with a link to complete a brief questionnaire asking their likelihood to repeat surgery with the options of: “Definitely not,” “Probably not,” “Unsure,” “Yes-most likely,” and “Yes-definitely.” For the purposes of statistical analysis, the results were dichotomized into patients who would repeat surgery (Yes-definitely and Yes-most likely) and patients who would not repeat surgery (Definitely not, Probably not, and Unsure).
Patients were enrolled during standard preoperative clinic visits prior to procedures at outpatient surgery centers. Nurses enrolled patients using a touch-screen tablet or computer. The software was programmed to email patients at 12-, 24-, and 52-weeks from the day of surgery with a link and request to complete the questionnaire. If the patient had not completed the questionnaire within 3 days, an automatic reminder was sent followed by a second reminder 3 days afterward, with a maximum of 2 reminders. All patients that underwent outpatient upper-extremity surgery, regardless of diagnosis, were eligible to participate.
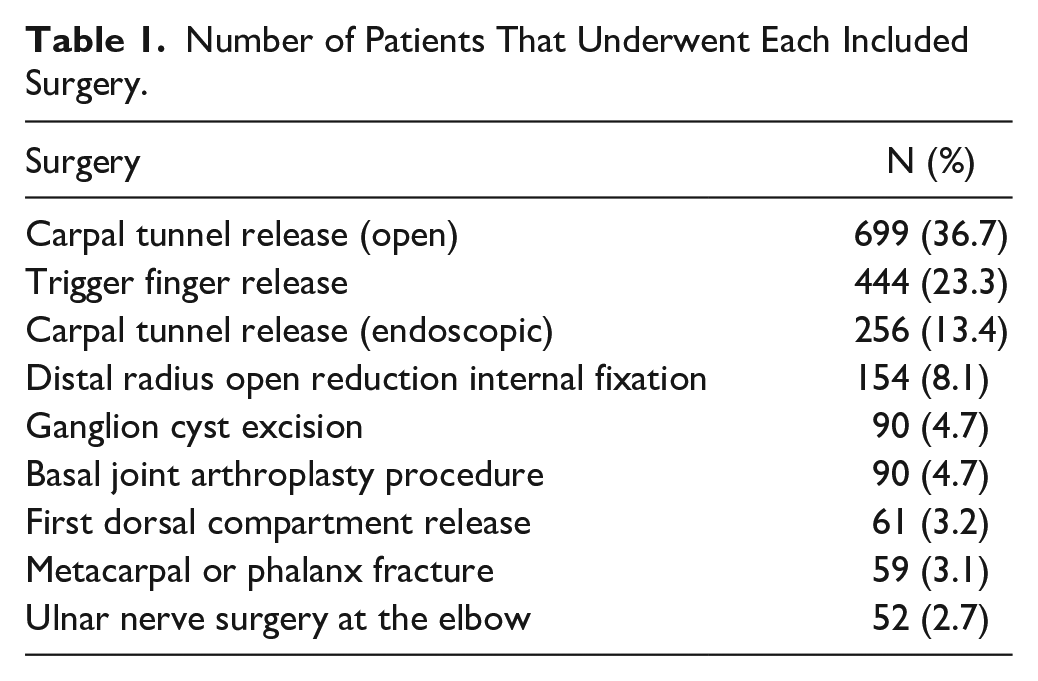
For this study, we included patients who were surgically treated for 1 of 9 common surgeries (Table 1), and who provided an answer regarding their likelihood to repeat surgery at 12, 24, or 52 weeks after surgery. Patients’ last response regarding their likelihood to repeat surgery at these 3 times determined their final satisfaction. This choice was made so as to not bias against excluding patient who would or would not choose to repeat surgery and may have stopped responding to surveys after 12 weeks. Patients with other diagnoses not listed or who underwent surgery for multiple diagnoses were excluded. Patients were enrolled at 7 hand surgery practices across 5 states (California, Ohio, Maryland, North Carolina, and Florida) comprising 14 surgeons over 42 months.
Number of Patients That Underwent Each Included Surgery.
Data Analysis
We report the overall proportion of patients who would repeat surgery stratified by common hand surgery procedures. The association between willingness to repeat surgery and diagnosis was assessed by Chi-square tests. Proportions between diagnoses were compared by z-tests with Bonferroni corrections for multiple comparisons. For the comparisons reported, post hoc power analyses demonstrated that we had greater than 94% power.
Results
Patient Characteristics
A total of 7806 postoperative patients were enrolled in the registry after routine hand surgery procedures, and 1905 met our inclusion criteria. Table 1 lists the number of patients stratified by each included surgery.
Patient Likelihood of Repeating Surgery
Overall percentage of patients that indicated they would repeat surgery was 81.6%. Average likelihood to repeat surgery at 12, 24, and 52 weeks were 80.0%, 82.9%, and 80.2%, respectively, with no statistically significant differences between timepoints. Breakdown by procedure performed is provided in Table 2. There was a significant association between procedure and patient willingness to repeat surgery (χ2: 76.0, df = 8, P < .05). Willingness to repeat surgery was significantly higher for carpal tunnel releases, trigger finger release, and distal radius open reduction and internal fixation when compared to satisfaction rates for ulnar nerve surgery at the elbow, basal joint arthroplasty procedures, and metacarpal and phalanx fractures (P < .05 with Bonferroni corrections).
Percentage of Patients That Would Repeat Surgery by Procedure Performed.
Loss to Follow-up
Of the 1905 patients that met inclusion criteria, 851 (44.7%) were lost to follow-up by the 52-week timepoint. Among these patients lost to follow-up, 632 patients responded at the latest time point available that they would repeat surgery and 219 responded that they would not. Of the patients lost to follow-up, 381 responded at only the 12-week timepoint. Additionally, 206 patients (10.8%) reported data at the 52-week timepoint, but not at 1 or 2 of the earlier timepoints.
Discussion
In this study, we describe a prospective, long-term assessment of patient willingness to repeat surgery after routine hand surgeries. We found that at patient’s final response, the overall proportion of patients that would repeat surgery after common hand surgery procedures is 81.6%. Importantly, even routine, presumably low-risk, high-success procedures range in patient desire to repeat surgery from 52% to 88%. This relatively high rate of not wanting to repeat surgery is higher than what is traditionally quoted during preoperative counseling in our experience. Providing accurate information on the general patient experience is essential for setting patient’s expectations and promoting shared decision making.
When presented with a surgical option, patients frequently ask what the “success rate” of the operation is. This can be a difficult question to answer, as a successful outcome means different things to different patients depending on their preprocedure pain and function, as well as expectations and other psychosocial factors. There are also situations where a surgeon and patient may differ in their perspective of a successful surgical outcome. Routine hand surgeries are often described as “highly successful” with “few complications” but few studies have published quantifications of patient satisfaction after these procedures.8,9 In many cases, a few case series have been published, but these generally involve small numbers of patients from a single surgeon.
Among common hand procedures, the greatest quantity of data available is for open carpal tunnel release. As far back as 1969, Semple and Cargill 10 performed open carpal tunnel release on 150 hands and reported 75% symptom resolution with an average follow-up of 3.3 years. In 1995, Nancollas et al 11 published long-term results of carpal tunnel release in 60 patients an average of 5.5 years after surgery and found that 87% reported “good” or “excellent” overall outcomes. Katz et al 12 published the Maine Carpal Tunnel Study in 1998, which analyzed 188 patients after carpal tunnel release and found a satisfaction rate of 66% at 18 months postoperatively. More recently, Kouyoumdijian et al 13 in 2003 studied 114 patients with an average follow-up time of 71 months and found that 78% of patients rated themselves as “cured” and 13.6% as “much better.” For endoscopic carpal tunnel releases, there is comparatively less published data on satisfaction rates. Erhard et al 14 in 1999 studied 95 hands in 86 patients and reported 72% were “free of symptoms” at a mean follow-up of 4.5 years. Hansen and Larsen 15 published a series of 101 patients who underwent endoscopic carpal tunnel release and found a 62% satisfaction rate 2 months after surgery. Our data show slightly higher rates of patients who would repeat surgery for these procedures but still lower than what may be shared with patients.
For carpometacarpal (CMC) arthroplasty, Barron and Eaton 16 in 1998 published a series of 21 patients who underwent ligament reconstruction and tendon interposition (LRTI) with minimum 1-year follow-up and reported that 91% were “completely satisfied.” Following this, Roberts et al 17 published a series of 14 patients who underwent CMC arthroplasty and reported that 93% of patients were “very satisfied” with a mean follow-up of 21 months. Interestingly, a simple web search at the time of publication reveals at least 4 different hand surgeon websites which cite a 96% success rate for LRTI, although there is no reference or apparent source for this number. Our data suggest that willingness to repeat surgery for CMC arthroplasty may be lower than what is commonly being advertised to patients.
In the treatment of wrist fractures, Chung et al 9 in 2019 published an analysis of 296 geriatric patients with distal radius fractures from The Wrist and Radius Injury Surgical Trial (WRIST), of which 22% were treated with volar locking plate systems, 21% with external fixation, 20% with pinning, and 37% with casting. The Michigan Hand Questionnaire (MHQ) was used to measure patient satisfaction with respondents selecting from very satisfied, somewhat satisfied, neither satisfied nor dissatisfied, somewhat dissatisfied, or very dissatisfied. The MHQ is unique in that its assessment of satisfaction is directly related to satisfaction regarding hand function. Responses were dichotomized into satisfied and dissatisfied. Overall, they reported a 74% satisfaction rate for grip strength and 81% satisfaction rate for wrist motion at 12 months after injury, but they did not break down satisfaction by treatment method, making it difficult to directly compare to our data.
For surgical excision of primary wrist ganglia, Craik and Walsh 18 studied 44 patients with mean follow-up of 44 months and found a 98% overall satisfaction rate. Patients in this study were asked to rate their satisfaction on a numerical scale from 1 to 5 and responses were dichotomized into dissatisfied (1-3) and satisfied (4-5). Singhal et al 19 similarly reported 92% satisfaction 6 weeks postoperatively from surgical excision of wrist ganglia among 26 patients. Satisfaction was assessed using a questionnaire asking patients to select from low, moderate, or high satisfaction. The satisfaction rates in both these studies are higher than the willingness to repeat surgery found in our data.
For De Quervain’s release, Scheller et al 20 published a study of 94 patients followed for an average of 15.7 years and reported a 100% success rate, defined by an absence of triggering and pain subjectively, as well as by physical examination. A study by Ta et al 21 reported a “full satisfaction” rate of 88% in 43 patients followed for an average of 3 years after De Quervain’s release. These satisfaction rates are both higher than the willingness to repeat surgery reported in our study.
Similarly, surgical trigger finger release has a wide range of reported success rates. In 1988, Thorpe 22 reported a 60% “success rate,” as defined by a lack of triggering, in 43 patients followed for an average of 47 months. This was followed by a 1997 report from Turowski et al 23 of a 97% success rate in 75 patients who underwent surgical trigger finger release and were followed for an average of 48 months. Satisfaction was defined as complete resolution of symptoms, while dissatisfaction was defined as partial or lack of improvement in symptoms. The 84% willingness to repeat surgery rate in our study population fell in between the reported satisfaction rates of these 2 studies.
Overall, there is a lack of consensus on how to measure satisfaction after many common hand procedures, leading to wide variability in quoted rates. The data available arealso not generalizable, as most studies are based on a small cohort with procedures performed by a single surgeon. As a result, surgeons may either share estimates of satisfaction rates hindered by their own recall and recency biases, or instead they may discuss complication rates as a surrogate for satisfaction. Complication rates do not tell the whole story, however, as patients can be unsatisfied for numerous reasons which may not be clear to the surgeon despite not being considered to have any identifiable complication. A recent study of wrist arthroplasty found that the procedure had a high satisfaction rate (87%) despite also having a high complication rate (29%). 24 Studies in plastic surgery have further demonstrated this lack of correlation between complication rate and patient satisfaction. 25
Our study has several limitations. These data reflect the experiences for patients of 14 hand surgeons at 7 hand surgery practices in the United States and may not necessarily be generalizable to other patient populations. Another limitation of this study is that preoperative patient-surgeon discussions were not standardized. These discussions prior to surgery shape patients’ expectations and therefore may have influenced their postoperative satisfaction. Additionally, surgical techniques were not standardized and were at the discretion of the participating surgeon. Our study is also limited by a high rate of loss to follow-up at the 1-year mark, although many of these were patients who underwent minor procedures such as carpal tunnel and trigger finger releases which typically do not require follow-up all the way to 1 year. We also found that of the patients lost to follow-up, far more patients indicated at their latest response that they would repeat surgery than those who would not. Furthermore, we included responses from patients who did not respond at all time points. This could lead to a lack of data dis-proportionately representing either satisfied or unsatisfied patients. It is also important to note that our survey used a surrogate question for satisfaction by asking for a patient’s likelihood of repeating surgery, rather than explicitly asking about satisfaction. However, we feel this is justified because the decision to repeat a surgery indicates that the outcome was satisfactory to the patient. Finally, our use of electronic data-collection for patient reported outcomes may not provide adequate representation from populations with limited access to, or difficulty with, electronic devices.
It is not in the best interest of either the patient or the surgeon to undergo a surgery that will ultimately result in patient dissatisfaction. Future studies will be necessary to further ascertain the reasons for patient dissatisfaction, including analysis of ongoing symptoms, complications, and unmet expectations. Comparing patients treated nonoperatively and operatively may also yield further insights. This knowledge could provide insight into improving preoperative counseling, selecting better candidates for surgery, as well as finding ways to identify dissatisfied patients early in the postoperative course and potential offer an early intervention.
This study represents an important first step toward this goal by providing data which can be shared with patients during preoperative conversations. It is clear, however, that we still do not understand dissatisfied patients well enough. There is ample opportunity for qualitative research efforts to better determine what is driving this group of patients and why they are dissatisfied. Being able to accurately quantify patient satisfaction within a given setting is the important first step toward recognizing deficiencies and areas for improvement, understanding how to improve satisfaction, and ultimately increasing the value provided to patients through hand surgery.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author O.F. is the owner of SurgiSurvey LLC, the database used for this study. The other authors declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.