
Abstract
Ulnar-sided wrist pain can be attributed to various bony and ligamentous structures. The purpose of this review is to compare outcomes following surgical interventions for isolated lunotriquetral (LT) interosseous ligament injuries in adults. We assessed 202 procedures from 9 retrospective case series studies of low to moderate quality based on the Structured Effectiveness Quality Evaluation Scale. The comparative outcomes (ie, range of motion, pain, strength, quality of life, complications, return to work, and patient satisfaction) were aggregated and categorized under arthrodesis, capsulodesis, ligament repairs and reconstruction, and ulna shortening osteotomy procedures. Although the comparison of outcomes was largely inconclusive due to the heterogeneity and the omission of preoperative characteristic data, we did observe higher complications and reoperation rates post LT arthrodesis. It is recommended that all outcomes be standardized and presented uniformly with best practices developed to better characterize the injury’s severity and integrity in future studies.
Introduction
The lunotriquetral (LT) joint is stabilized by the intrinsic C-shaped interosseous ligament consisting of the dorsal, proximal membrane, and palmar structures. 1 Lunotriquetral interosseous ligament (LTIL) injuries mostly result from excessive ulnar axial loading, hyperextension, pronation, and radial deviation of the wrist with forearm supinated.2,3 Concomitant bony and ligamentous lesions, such as triangular fibrocartilage complex (TFCC) or scapholunate (SL) tears, are often associated with similar pathomechanics.4-9
Common LTIL injury symptoms include ulnar-sided wrist pain, weakness, diminished sensation, limited range of motion (ROM), and “clicking” during wrist lateral movements.10 -13 Arthroscopy is the most valuable diagnostic tool that allows direct visualization of the location, size, and extent of soft-tissue damage. 14 Operative management is indicated if conservative treatment fails and the symptoms persist.13,15,16 There is no agreement regarding the most effective treatment method. 14 To our knowledge, there has been no previous systematic review on this topic. Therefore, this systematic review aimed to compare patients’ outcomes following surgical interventions for isolated LTIL injuries in adults.
Methods
Data Identification
Literature searches were conducted for clinical studies related to LT instability interventions up to February 2022. Four computerized databases were searched from the earliest date using 10 search terms (listed in Supplemental Table S1). The databases that were searched are MEDLINE (OVID), Excerpta Medica (EMBASE), CINAHL, and SCOPUS.
Eligibility Criteria
Design
We included studies that were published in English without any date restriction. All study designs were included except for reviews, case reports, strictly biomechanical/cadaveric studies, and technique papers without reporting patient results.
Participants
Participants were adults with isolated LTIL injuries that have had surgical interventions. We did not include patients with concomitant injuries that were inseparable from the rest of the cohort. However, we did not exclude cases of static volar intercalated segment instability (VISI) as it arises mainly secondary to a full LTIL tear. 17
Intervention/comparator
All surgical methods were accepted, except if concomitant injuries were present or repaired simultaneously. We included studies that focused solely on surgical management.
Outcome
Any outcome measure used in the studies was included.
Time
All isolated LTIL injuries were included, regardless of their chronicity.
Study Selection
Four authors (MOH, JCKL, JM, and DR) were involved in screening titles, abstracts, and full text of all the collected journal articles. The bibliographic citation files were imported into Covidence 18 software. Two votes were required for articles to be included in the subsequent stage. All reviewers in the process were blinded to each other’s decisions. Journal articles that had conflicts were resolved by another reviewer in the research group (AD). The article’s references were also screened to find if any additional journal articles matched the inclusion/exclusion criteria that may be added to the list of included articles.
Data Extraction
All 4 reviewers (MOH, JCKL, JM, and DR) extracted data from 9 primary studies. We used a spreadsheet for organization, and the data extracted were as follows:
Information about the studies such as authors, type of study, year, interventions, and the Structured Effectiveness Quality Evaluation Scale (SEQES) score.
Information on participants such as sample size, age, gender ratio, instability, tear integrity, mean time to surgery, work, and postoperative management.
Information based on outcome measures and results used in the studies such as pain, strength, ROM, functional outcomes, patient satisfaction, return to work (RTW), and complications.
Data Synthesis and Analysis
We synthesized and analyzed our extracted data on participants, surgical interventions, and outcomes. To enable comparisons to be drawn between ROM and grip strength results, we had to recalculate and aggregate the data. We presented ROM as a percentage of the norm. Measurements provided solely in degrees were converted to percentages by using the normative data obtained from the American Academy of Orthopaedic Surgeons. 19 The following ranges were considered normal as per the reference means: flexion 75°, extension 74°, radial deviation 21°, and ulnar deviation 35°. To compare grip strength values between studies, the percentage of grip strength of the affected hand compared with the contralateral side was used. When strength measurements of the contralateral side were provided, the percentage of the affected side was manually calculated. In addition, all studies reporting in pounds were converted to kilograms. The studies that reported only absolute values without comparing with the contralateral side could not be included in the calculated means. Based on the results of the SEQES, low-quality studies with a score of 16 or lower were excluded from the analysis.
Critical Appraisal and Quality Assessment
The quality of the studies and study designs were evaluated using the SEQES (see Supplemental Table S2). 20 The SEQES is a 24-item critical appraisal tool that evaluates the methodological characteristics of the study in 7 general sorts (study questions, design, subjects, interventions, outcomes, analysis, and recommendations). Scoring includes 24 items, and each item is scored 2, 1, or 0. Each reviewer used interpretation guides presented in the article “An Introduction to Evidence-Based Practice for Hand Therapists” by Dr Joy MacDermid. 20 A quality score between 33 and 48 indicates high quality, scores between 17 and 32 indicate moderate quality, and ≤16 indicates low quality. Each reviewer’s SEQES scores were blinded to the other reviewers until the scoring process was completed based on the calibration meeting held virtually with all reviewers post screening.
Results
Search and Selection of Studies
A total of 1297 journal articles were sourced from the 4 databases. After removing 719 duplicates, 578 were screened for eligibility. Eventually, 9 primary articles were included in this systematic review (Figure 1). 21
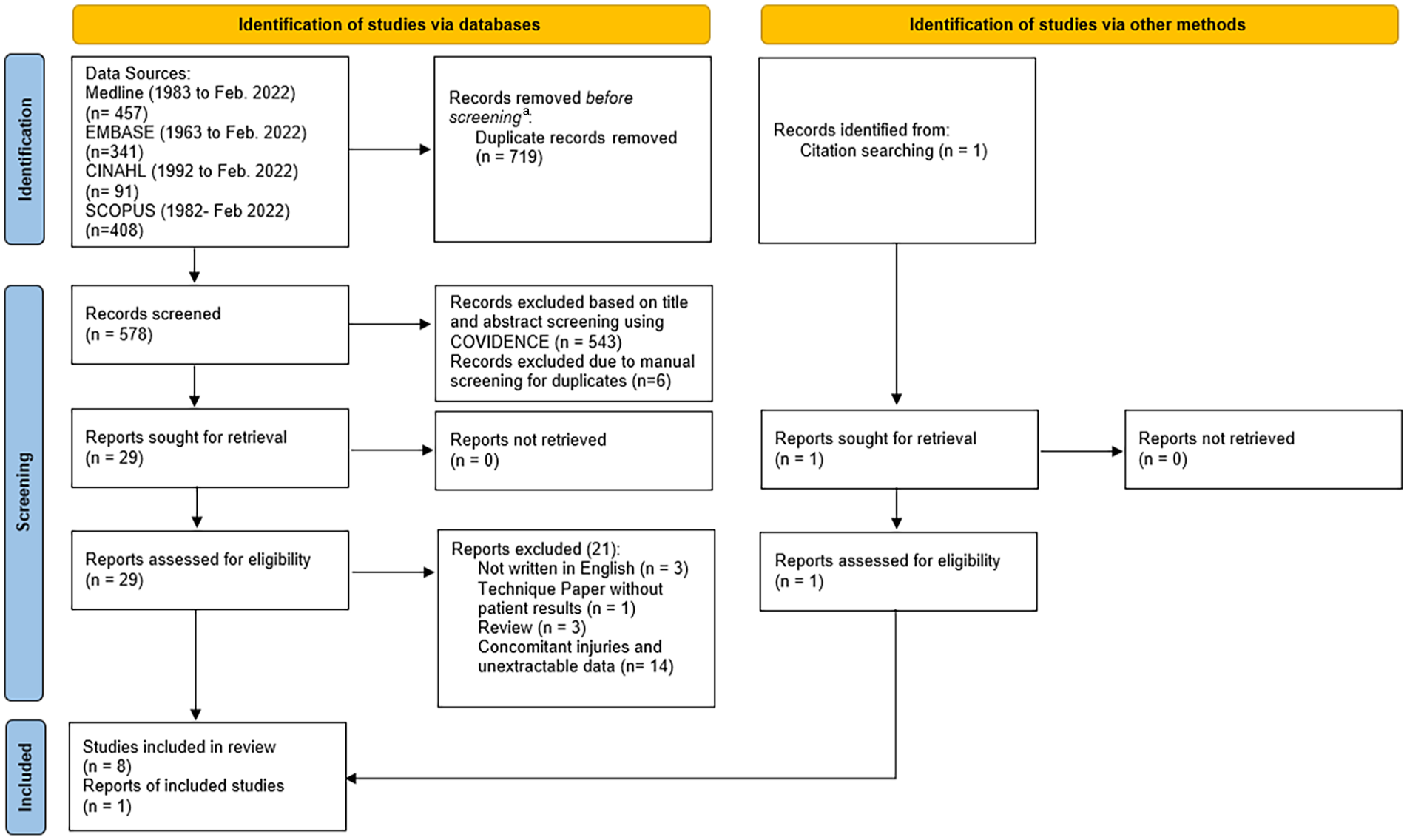
Diagram for literature search presented according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 21
Studies’ Quality
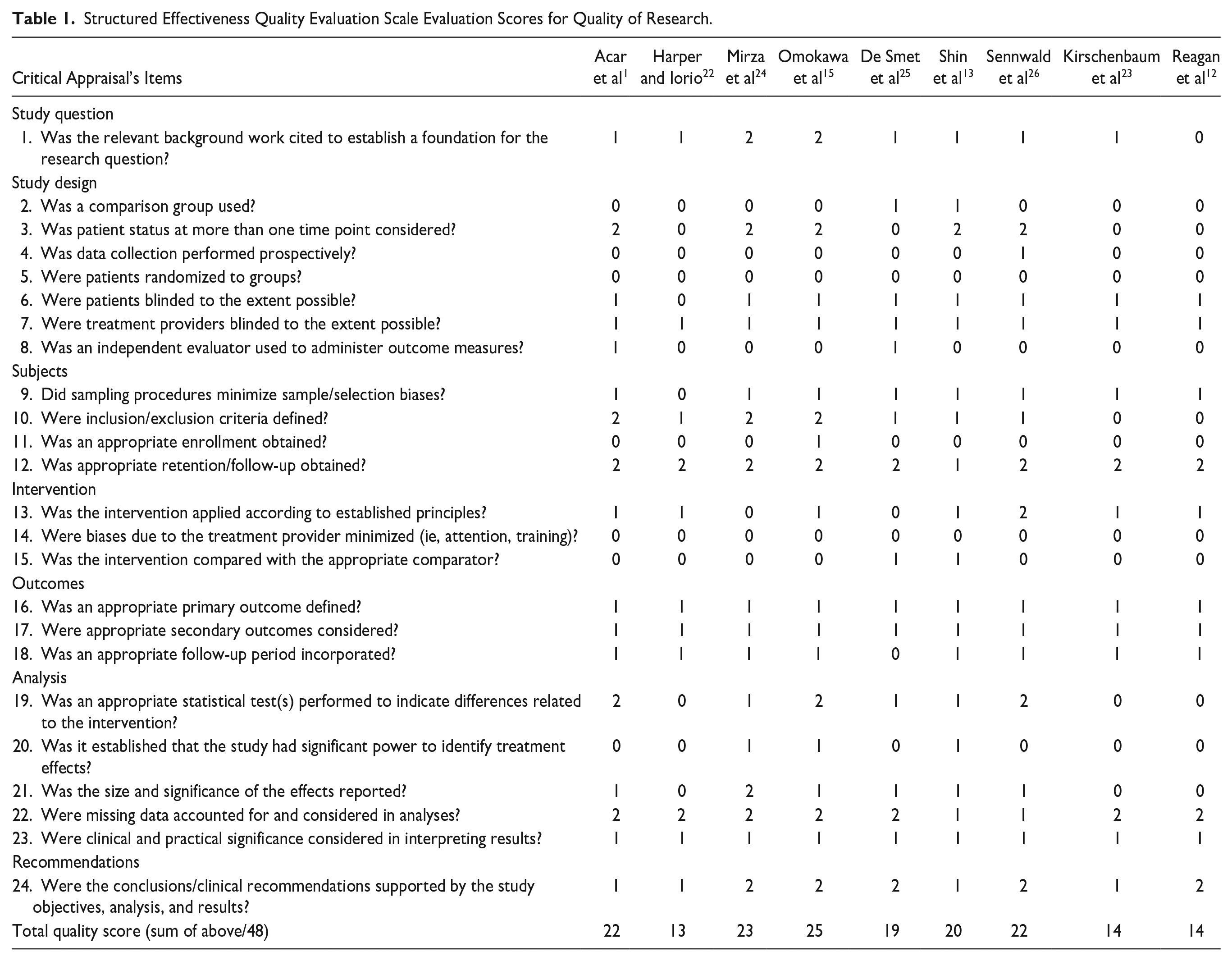
The overall scores for all selected studies range from 13 to 25, out of 48, with an average cumulative score of 19.1 (Table 1). Most studies were deemed to have moderate quality (6/9), while 3 studies, by Reagan et al, 12 Harper and Iorio, 22 and Kirschenbaum et al, 23 obtained 14/48, 13/48, and 14/48, respectively, which were classified as clinically insignificant low-quality studies. This was secondary to not having an adequate control group, collecting prospective data, and its lack of ability to randomize and perform blinding (in either subjects, surgeons, or assessors).
Structured Effectiveness Quality Evaluation Scale Evaluation Scores for Quality of Research.
Participants’ Characteristics Extracted From Selected Studies
There were 201 patients with 202 procedures performed in the 9 studies. Eight out of the 9 primary studies provided a male-to-female ratio. Overall, 56% were men. The median of all the average age provided in all the studies was 32 years old, ranging from 15 to 60 years old. Six studies reported the mean time to surgery, ranging from less than 1.5 to 96 months. In the selected studies, Acar et al 1 mentioned the patient’s profession, such as industrial worker, chemist, or bus driver. Most studies were inconsistent in providing the characteristics of the LT instability and its tear integrity (Table 2).
Summary of Characteristics and Quality Assessments.
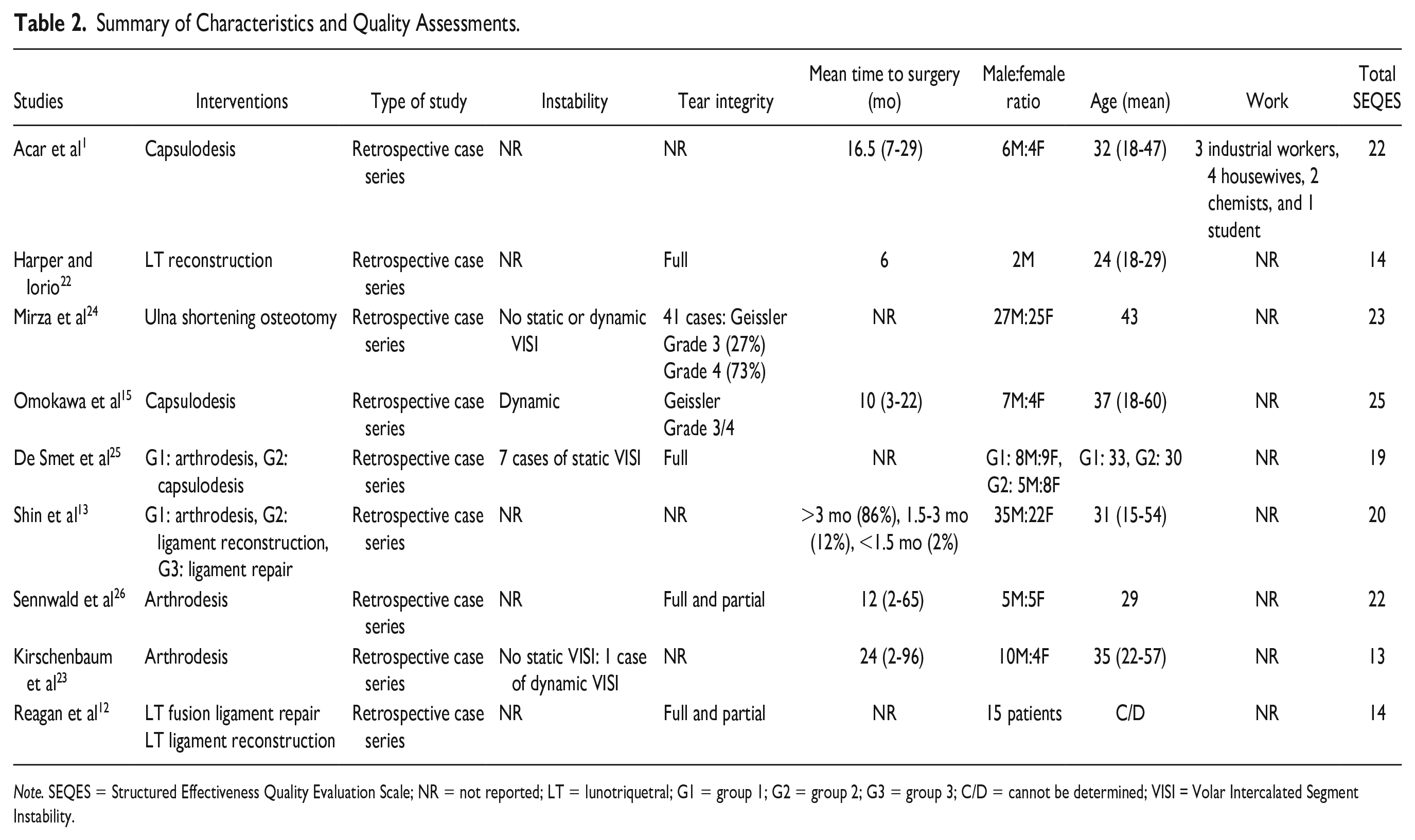
Note. SEQES = Structured Effectiveness Quality Evaluation Scale; NR = not reported; LT = lunotriquetral; G1 = group 1; G2 = group 2; G3 = group 3; C/D = cannot be determined; VISI = Volar Intercalated Segment Instability.
We eliminated individual data points from our selected studies if specific data points were not solely an isolated LTIL injury. In the study of Sennwald et al, 26 13 out of the 23 patients were eliminated due to concomitant injuries such as primary distal radius fractures and chondromalacia. 26 Similarly in the article of Reagan et al, 12 7 out of 22 patients were excluded because of concomitant injuries such as SL ligament disruption and procedures such as proximal row carpectomy and intercarpal fusion of several carpal bones. 12 The outcomes were extracted individually from the studies, and a mean was generated accordingly.12,26
Surgical Procedures
Five surgical techniques were included in this systematic review (Tables 3 and 4). Lunotriquetral arthrodesis is a surgical method that attempts to minimize movement between the lunate and the triquetrum as in congenital carpal coalition.8,27 Dorsal capsulodesis is used to reinforce the dorsal aspect of the ulnar carpus. 28 This procedure was rationalized based on previous kinematic studies17,29,30 showing that the dorsal radiocarpal ligament contributes to LT joint stability and plays a key role in preventing VISI collapse. 29 Lunotriquetral ligament repairs were performed by reducing the LT joint with Kirschner-wire fixations and suturing the LT ligament into the triquetrum through drilled holes.12,13 Lunotriquetral reconstruction is a surgical technique in which a tendon strip is used to correct the subluxation of the triquetrum, thereby permitting increased anatomical movement between the proximal row of the carpal bones and maintaining LT movement.22,31 This procedure reestablishes typical carpal kinematics but does not necessarily recreate the anatomy of the LT joint.13,22,31 Ulna shortening osteotomy is a technique that alleviates symptoms by placing the distal part of the TFCC and ulnolunate and ulnotriquetral extrinsic ligaments under tension, and consequently, reduces motion at the lunate and triquetrum.6,32 -34 In the study of Mirza et al, 24 no previous or other concomitant procedures were performed alongside the ulna shortening osteotomy in the included patients. Within the included studies, 44% (88 out of 202 procedures) failed conservative management before surgery,1,13,23,24 and the rest did not report if and how patients were conservatively managed before surgery.
Summary Outcomes for Arthrodesis, Capsulodesis, Ligament Repair, Ligament Reconstruction, and Ulna Shortening Osteotomy.
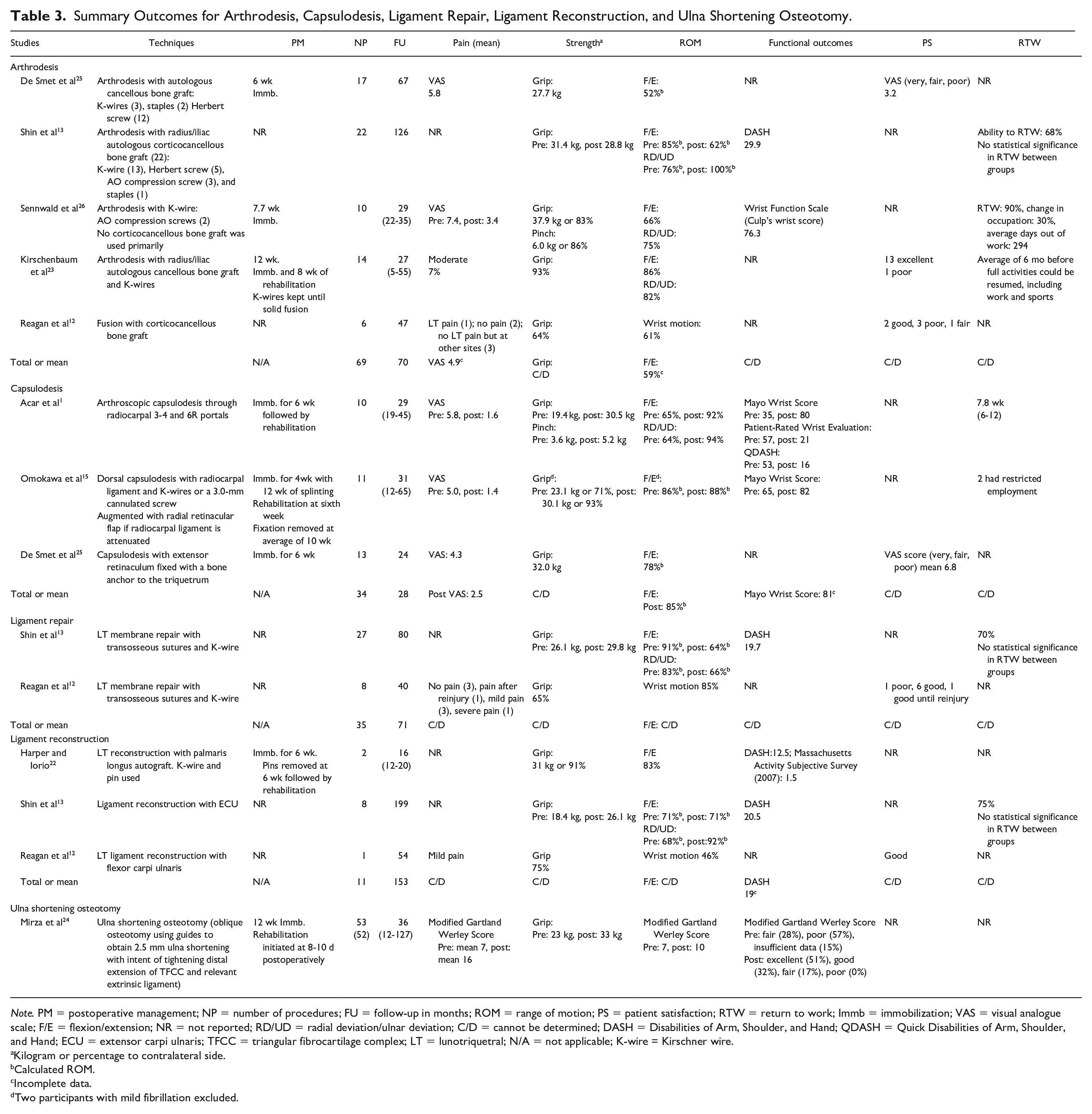
Note. PM = postoperative management; NP = number of procedures; FU = follow-up in months; ROM = range of motion; PS = patient satisfaction; RTW = return to work; Immb = immobilization; VAS = visual analogue scale; F/E = flexion/extension; NR = not reported; RD/UD = radial deviation/ulnar deviation; C/D = cannot be determined; DASH = Disabilities of Arm, Shoulder, and Hand; QDASH = Quick Disabilities of Arm, Shoulder, and Hand; ECU = extensor carpi ulnaris; TFCC = triangular fibrocartilage complex; LT = lunotriquetral; N/A = not applicable; K-wire = Kirschner wire.
Kilogram or percentage to contralateral side.
Calculated ROM.
Incomplete data.
Two participants with mild fibrillation excluded.
Summary of Complications, Reoperation, and Additional Notes.
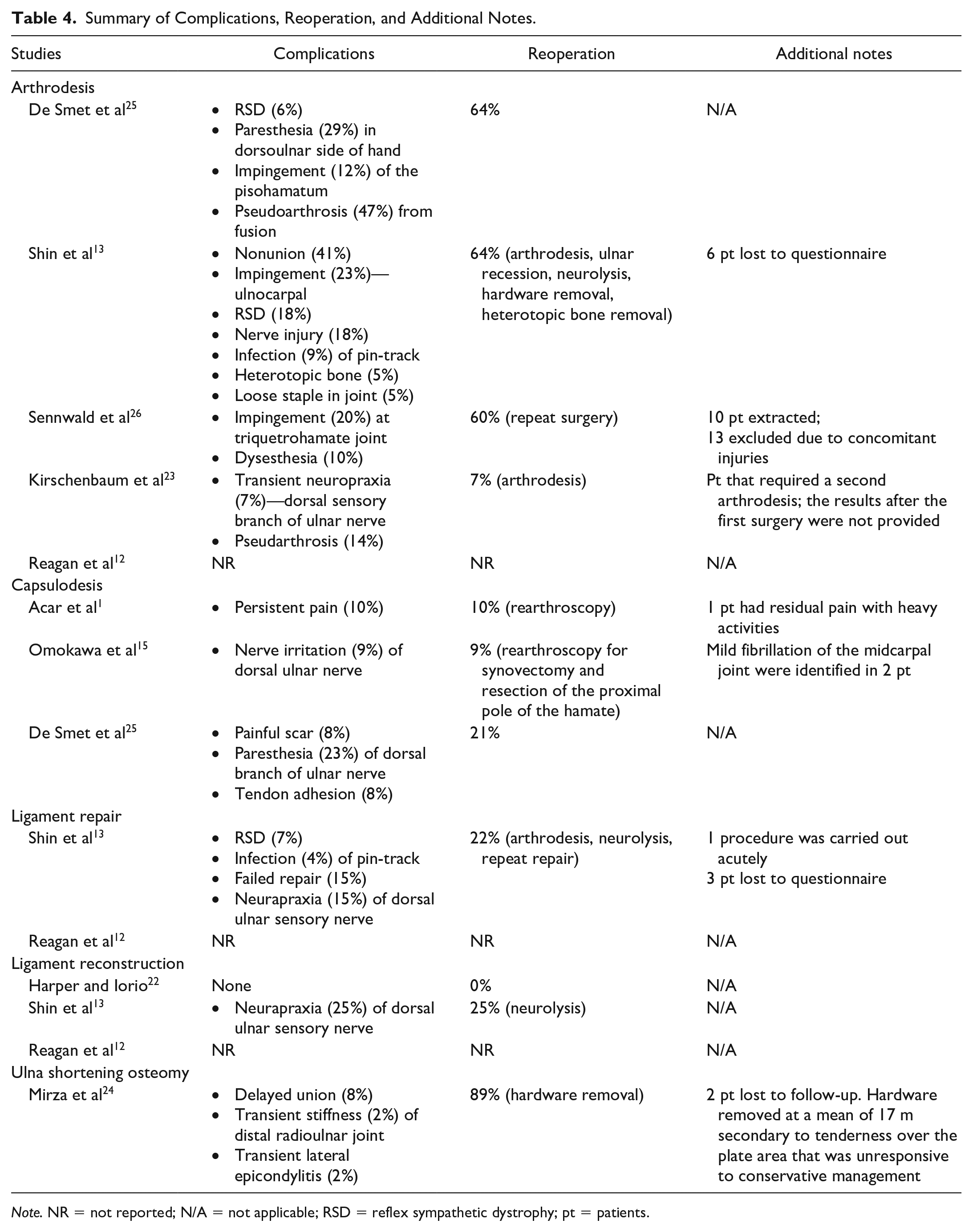
Note. NR = not reported; N/A = not applicable; RSD = reflex sympathetic dystrophy; pt = patients.
Outcomes
Means were generated per outcome and surgical procedure only when identical scales were used by 2 or more studies; however, low-quality studies were excluded in this process.
Range of motion
Range of motion data were presented either in degree measurement or percentage of the contralateral side, except for the study of Mirza et al, 24 where the Modified Gartland Werley Score (MGWS) was used instead. 24 All 9 studies included wrist flexion and extension ROM, 3 included radial and ulnar deviations, and Reagan et al 12 reported wrist motion in percentage without specifying the direction of the movement. Preoperative ROM measurements were only included in 3 studies. De Smet et al 25 and Sennwald et al 26 provided absolute values, which had to be converted to percentage.26,25 The mean percentage of postoperative ROM for flexion/extension in arthrodesis ranged between 52% and 86%, capsulodesis between 78% and 92%, ligament repair between 64% and 85%, and ligament reconstruction between 46% and 83%. Patients who underwent ulna shortening osteotomy obtained an MGWS of 10 ± 2. A score of 10 indicates that the motion is “same as the contralateral side,” and 7.5 indicates that motion is “limited but more than functional wrist motion.” 35
Pain
Seven studies reported pain as an outcome measure. Shin et al 13 and Harper and Iorio 22 did not include pain as an outcome measure in examining their results. Forty-four percent of the primary studies measured pain with the visual analogue scale (VAS). In the arthrodesis group, De Smet et al 25 reported a mean VAS postoperative score of 5.8 out of 10. Sennwald et al 26 reported a reduction in pain of 40% from prearthrodesis and postarthrodesis procedures. 26 Kirschenbaum et al 23 reported that 7% of the participants continued to report moderate pain. 23 Reagan et al 12 continued to have 1 participant out of 6 report persistent pain following arthrodesis, and 2 other participants reported pain at a different location (ie, carpometacrapal joints). 12 In the capsulodesis group, Acar et al 1 and Omokawa et al 15 reported a reduction in VAS scores in precapsulodesis and postcapsulodesis of 42% and 36%, respectively.1,15 De Smet et al 25 reported a 4.0 score on the VAS scale following capsulodesis. 25 In the ligament repair group, Reagan et al 12 reported that 1 out of 9 participants continued to report severe pain. Reagan et al 12 reported mild pain following the procedure for the ligament reconstruction group. Mirza et al 24 obtained a postoperative subjective pain mean score of 16 over the MGWS, where a score of 15 indicates “occasional pain, no compromise in activities, and mild discomfort with strenuous use” and a score of 20 indicates “no pain.” 35
Strength
Grip strength was reported in all the studies included in this review. Three of the 5 studies that carried out arthrodesis had grip strength ranging from 64% to 93%. In 3 of the studies where capsulodesis was performed, only data from one study by Omokawa et al 15 were presented as a percentage of the contralateral side with an average grip strength of 93%. In 2 studies where LTIL repair was done, Reagan et al 12 had average grip strength of 65% of the contralateral side, whereas Shin et al 13 gave absolute values of 29.8 kg. 12 Grip strength in the studies where ligament reconstruction was done ranged from 75% to 91%. In the ulna shortening osteotomy study by Mirza et al, 24 an absolute postoperative value of 33 kg was provided without comparison with the contralateral side.
Functional outcomes
A detailed comparison between the different studies could not be effectively made due to the heterogeneity of the scales. In the studies where arthrodesis was done, Shin et al 13 reported an average Disabilities of Arm, Shoulder, and Hand (DASH) score of 29.9, and Sennwald et al 26 used the Wrist Function Scale and reported an average score of 74.82.13,26 Two of the 3 studies that reported on capsulodesis presented functional outcomes. Acar et al 1 used 3 scales, the Mayo Wrist Score, the Patient-Rated Wrist Evaluation (PRWE), and the Quick Disabilities of Arm, Shoulder, and Hand (QDASH) questionnaire, with preintervention scores of 35, 57, and 53 and postintervention scores of 80, 21, and 16, respectively. 1 Omokawa et al 15 used only the Mayo Wrist Score with a preoperative score of 65 and a postoperative score of 82. Of the 2 studies reporting ligament repair, only Shin et al 13 reported functional outcomes using the QDASH with an average score of 19.7. Two of the 3 studies that reported on ligament reconstruction had functional outcomes with Harper and Lorio 22 using the QDASH with a score of 12.5 and also the Massachusetts Activity Subjective Survey with a score of 1.5 and Shin et al 13 using the QDASH with a score of 20.5. 22 In the ulna shortening osteotomy study, the functional outcome scale used was the MGWS with a preoperative score of 7 and a postoperative score of 10.
Patient satisfaction
Three studies reported on patient satisfaction. De Smet et al 25 used the VAS scoring system to determine patient satisfaction under the terms very satisfied, fair, and poor. In group 2, the capsulodesis group had a greater mean score than the arthrodesis group 1; the scores were 6.8 and 3.2, respectively. Kirschenbaum et al 23 stated that 92% of the participants reported excellent satisfaction following their arthrodesis procedure. Reagan et al 12 broke down their patient satisfaction into good, fair, and poor. In the LT fusion group, 50% reported poor satisfaction following the procedure. For LT membrane repair, only 1 participant reported their satisfaction as poor, and for ligament reconstruction, 1 participant reported their satisfaction as good.
Return to work
Only 5 studies reported on RTW. None were used as primary outcomes. In the capsulodesis group, Acar et al 1 reported an average RTW of 7.8 weeks postsurgery, and Omokawa et al 15 had 2 participants with restricted employment following the procedure. In the arthrodesis group, Shin et al 13 and Sennwald et al 26 reported RTW rates of 68% and 90%, respectively. Krishenbaum et al reported an average of 6 months before full activities could be resumed, including work. Shin et al 13 found no significant differences between the 3 groups. They reported a RTW rate of 70% in the ligament repair group and 75% in the ligament reconstruction group.
Discussion
This systematic review compares the outcomes following surgical interventions for isolated LTIL injuries in adults. We decided to isolate LTIL injuries as clinical outcomes could be affected by concomitant injuries. Most studies do not have a standardized classification for chronicity and did not provide an inclusion criterion for preoperative characteristic data. Only 3 studies from our review defined injuries as chronic when acquired at least 3 months before surgery.13,23,26 Only 3 of the included studies reported a minute number of patients with persistent symptoms for less than 3 months.13,22,26 In the study of Shin et al, 14 only 1 out of 27 ligament repairs was carried out acutely. The scarcity of literature related to the management of acute LTIL injuries can be attributed to late diagnosis as radiological imaging is typically normal. 36 As in the article by Omokawa et al, 15 LTIL injuries were often overlooked and diagnosed as a wrist sprain until the patient develops “persistent pain and functional impairments.” Furthermore, magnetic resonance imaging (MRI) was shown to have a specificity of 76% to 100% and a sensitivity of 0% to 82%. 37 According to Andersson et al, 37 “negative results of MRI or provocative clinical tests are unable to safely rule out the possibility of clinically relevant tears to the TFCC or the SL and LT ligaments.”
A complication during data extraction is the heterogeneity of outcome measures reported in different studies, which makes comparison difficult. All studies that reported on patient satisfaction did not report on functional outcomes. This may be due to a change in practice and a newer trend shifting from solely using patient satisfaction toward standardized patient-rated outcome measures. We suggest using an established, well-validated tool such as the PRWE or the DASH questionnaires for future research. This aligns with the recommendations by the International Consortium for Health Outcomes Measurement Hand and Wrist Working Group. 38 This will make interpreting and replicating data and literature more streamlined. Similarly, returning to work is an outcome that should be of high consideration. As per the available results, more than 2/3 of patients RTW following operative intervention for LTIL injury. A direct comparison between the surgical techniques could not be made as results were either presented in RTW rates, time out of work, or employment restriction.
Most of the included studies, regardless of the procedure, reported reduction of pain postsurgery. A direct comparison between the techniques was inconclusive due to the heterogeneity of the pain scales and data omission in 29% of the procedures. Pain is reported in a numerical scale in slightly less than a third of the procedures. A true postoperative VAS mean of 2.5/10 could only be generated for the capsulodesis group based on 34 procedures, while the arthrodesis group obtained a higher mean at 4.9/10 based on incomplete data pertaining to 27 procedures. Grip strength and ROM were measured inconsistently in percentages and/or absolute units. As grip strength norms are dependent on a variety of factors such as gender, age, hand dominance, arm support, and wrist and forearm position, 39 it is only through the provision of preoperative and postoperative values for both the affected and nonaffected hands that meaningful comparisons on this important outcome can be made. With less than half of the subgroups providing grip strength as a percentage of the contralateral side, surgical outcomes that provided better grip strength could not be effectively determined.
Several studies reported only postsurgery ROM measurements, which is inadequate as we are unaware of the participants’ preoperative values. A numerical analysis could not be performed for the study of Mirza et al 26 for ulna shortening osteotomy as the MGWS only provides a descriptive range. From the available aggregated data, the capsulodesis group obtained a higher postsurgery wrist flexion and extension ROM with a calculated mean at 85% based on 34 procedures compared with the arthrodesis group who obtained 59% based on incomplete data from 47 procedures. This lower wrist flexion and extension ROM rate in the arthrodesis group may be attributed to altered carpal kinematics. 13 Secondary to the data’s paucity and heterogeneity, we cannot conclude gains and deficits. Considering this is often a salvage procedure with significant functional limitations, LT operative interventions, regardless of type, still result in at least 50% return to wrist flexion/extension ROM.
A variety of complications were reported in most studies in this review (Table 4). Differences in procedures, follow-up times, and reporting details in the included articles limited the ability to make comparisons around complications. Across the treatment subgroups, patients who underwent arthrodesis had the highest complication rates varying between 5% and 47% with a high reoperation mean rate of 51%. Given the midcarpal joint discongruency 25 and altered carpal kinematics induced 13 by the arthrodesis, the wrist joint is susceptible to ulnocarpal and midcarpal impingement. 13 The site of impingement varied across the studies, with Sennwald et al 26 reporting impingement at the triquetrohamate, Shin et al 13 at the ulnocarpal joint requiring ulnar recession, and De Smet et al 40 at the pisohamatum. Reoperation rates were higher than other techniques secondary to the significant risk of nonunion or pseudoarthrosis. For example, Shin et al 13 reported 41% nonunion and a reoperation rate of 64% in the arthrodesis group. In contrast, they had 22% and 25% reoperation rates in the ligament repair and ligament reconstruction subgroups, respectively. A similar observation was reported by Grift and Ritt 14 in their literature review about the management of LT instability. They reported up to 57% rates of nonunion in the arthrodesis procedure of the LT joint, and that indication for surgery should be very clear. 14 Other surgical techniques showed comparable complication and reoperation mean rates that ranged between 14% and 22%. Ulna shortening osteotomy presented few transient complications; however, hardware removal is almost a requisite due to a high 89% removal rate secondary to tenderness over the plate area. 24
Limitations
None of the studies included a control group, and only 2 had comparative treatment groups. All our studies were retrospective case series. Therefore, there was no randomization of groups. These factors cause selection and reporting bias. There were methodological issues, such as lack of inclusion and exclusion criteria reported.23,25 Furthermore, many of the included studies did not specifically indicate when concomitant injuries were present and if it was included or excluded per their exclusion criteria. Thus, it is difficult to assert that concomitant injuries were completely absent. The lack of consistent and meaningful evidence weakens the strength of our interpretation drawn for the interventions, even though there is evidence supporting the use of the interventions in current clinical practice. With inconsistent reporting, biases to internal validity and a level of uncertainty were introduced when aggregating and interpreting the data.
Conclusion
This systematic review synthesized the evidence of surgical interventions and management outcomes for isolated LT instabilities. Current available studies are of poor to moderate quality, mostly retrospective case series with poor internal validity based on the aggregated data from this review. Although the comparison of outcomes was largely inconclusive due to the heterogeneity and the omission of preoperative characteristic data, we did observe tendency of higher complications and reoperation rates post LT arthrodesis. There is still no ideal surgical method for isolated LT injuries that could be advised after this review; however, our analysis indicates that LT capsulodesis tends to yield a higher postoperative wrist flexion and extension ROM rate and a lower postoperative pain score compared with LT arthrodesis. It is recommended for future studies that all outcomes be standardized and presented uniformly with best practices developed to better characterize the injury’s severity and integrity in future studies.
Supplemental Material
sj-docx-1-han-10.1177_15589447231198268 – Supplemental material for Outcomes Following Surgical Interventions for Isolated Lunotriquetral Interosseous Ligament Injuries: A Systematic Review
Supplemental material, sj-docx-1-han-10.1177_15589447231198268 for Outcomes Following Surgical Interventions for Isolated Lunotriquetral Interosseous Ligament Injuries: A Systematic Review by Mohanad Omar-Hossein, Jacob C. K. Leung, Joyce Munaku, Danielle Rodzik, Armaghan Dabbagh and Mike Szekeres in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447231198268 – Supplemental material for Outcomes Following Surgical Interventions for Isolated Lunotriquetral Interosseous Ligament Injuries: A Systematic Review
Supplemental material, sj-docx-2-han-10.1177_15589447231198268 for Outcomes Following Surgical Interventions for Isolated Lunotriquetral Interosseous Ligament Injuries: A Systematic Review by Mohanad Omar-Hossein, Jacob C. K. Leung, Joyce Munaku, Danielle Rodzik, Armaghan Dabbagh and Mike Szekeres in HAND
Footnotes
Acknowledgements
The authors would like to thank Dr Paul Parikh for his guidance in this research.
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This article does not contain any human participants from whom informed consent would be required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.