
Abstract
Background:
For children with upper brachial plexus birth injury (BPBI; C5, C6, ±C7 roots), most clinics first recommend nonsurgical treatment followed by primary and/or secondary surgical interventions in selected patients. Since 2008, we have used an infant shoulder repositioning protocol (supination-external rotation [Sup-ER]) designed to prevent shoulder internal rotation contracture and its potential effects on the shoulder joint. This study characterizes our clinic’s current choice, number, and timing of primary and secondary procedural interventions (including Botox) and compares Sup-ER protocol patients with those of our historical controls.
Methods:
The records of all patients with upper BPBI who underwent procedures from 2001 to 2018 were retrospectively reviewed and grouped into a historical (2001-2007, n = 20) and recent (2008-2018, n = 23) cohort. Patient demographics, procedure types and timing, and functional outcomes were collected and analyzed.
Results:
Since the 2008 institution of the Sup-ER protocol, fewer brachial plexus exploration and grafting (BPEG) surgeries were performed and none in later infancy, where nerve transfers were preferred. There were more and earlier Botox injections. There were fewer tendon transfers, and the preoperative indications were from a higher level of function.
Conclusions:
We now see fewer indications for BPEG surgeries overall. After the 3-month-age group, more direct nerve transfers are indicated instead of the BPEG surgery if nerve surgery is required at all. Shoulder tendon transfer rates have decreased. Humeral osteotomies are not seen in our recent group. Glenoid osteotomies within tendon transfers are rare in both groups.
Keywords
Introduction
A brachial plexus birth injury (BPBI) occurs when there is damage to the brachial plexus during infant delivery. In Canada, the incidence of BPBI is estimated at 1.24 per 1000 live births. 1 While about 66% to 95% of injuries2-4 have clinically reasonable spontaneous recovery, those with more severe injuries may have poorer recovery. These infants may experience lifelong disability or reduced function related to weakness, joint deformity, limb length discrepancy, and reduced range of motion (ROM).2,5,6
Management of severe upper BPBI is guided by the patient’s pattern of recovery and function. Treatment often begins with rehabilitative management including upper extremity stretching with or without splinting to maintain full passive ROM, avoid joint contractures, encourage active movement and age-appropriate developmental play, support strengthening, and develop sensory awareness. 3 Surgical decision-making may be challenging during a period described as the “gray zone,” when the balance of surgical timing, risks, and outcomes are hard to determine. 7 Patients with poor nerve recovery and/or shoulder joint malposition may benefit from surgical interventions such as primary nerve exploration/reconstruction, repair, grafting, and/or transfers, and/or secondarily from tendon transfers (TTs) and osteotomies.8,9 Nonsurgically, botulinum toxin type A (BTX-A) used in antagonist muscles can improve muscle balance, allow reduction of shoulder subluxation, and alleviate cocontraction.10-12 Although many different treatment options and algorithms exist, global consensus for optimal management in upper plexus injuries has not been reached. Regardless of management choice, even children with “good” recovery often experience some impairment in passive and active range of external rotation (ER) and supination (Sup), incomplete recovery from muscular imbalances, and long-standing contractures of the shoulder and elbow.13-15
Our clinic previously described an early upper extremity passive repositioning program (Sup-ER protocol) that uses an orthosis to position the forearm in Sup and the shoulder in ER with the goal of optimizing the musculoskeletal anatomy of the shoulder 16 in addition to traditional rehabilitation management. The protocol starts at 6 to 8 weeks of age, with 20 to 22 hours per day of orthosis wear during the long newborn sleep periods, and full ROM stretches during interval breaks from the orthosis. 16 This maximizes glenohumeral contact time during a period of rapid growth, conceptually akin to the Pavlik harness for hips. 17 Ultrasound confirms glenohumeral anatomy at the time of orthosis institution and at monthly clinic follow-ups. If shoulder ROM and α angles stabilize, orthosis use is reduced to nights and naps. 16 A pilot study showed that children who followed the Sup-ER protocol had better Sup and ER ROM at 2 years of age compared with a historical control group. 17 Sup-ER protocol-specific recommendations/algorithms for orthosis use, brachial plexus exploration/grafting (BPEG), Botulinum toxin/casting, nerve transfers, and suggested orthopedic considerations have evolved over time. Our initial aspiration for the Sup-ER protocol was to reduce the need for shoulder interventions, especially if we could reduce tendon transfers. Therefore, this study specifically examines the changes in the pattern of interventions and functional outcomes in a clinic population in the years following institution of the Sup-ER protocol. We hope our findings may add to the discussion of optimal management for children with BPBI, even those in the “gray zone,” with specific interest in whether TT rates or indications are affected positively.
Methods
This retrospective study was approved by the University of British Columbia Children’s and Women’s Research Ethics Board (H20-01297).
Study Patients
We reviewed the British Columbia Children’s Hospital (BCCH) Brachial Plexus Clinic database for all patients with data entered from January 1, 2001, to April 31, 2018. Eligible patients were those clinically diagnosed with injury severity greater than a neurapraxia to C5-6 ± C7, (i.e., Erb’s palsy) with or without initial neurapraxic injuries to C8-T1. Patients were included if they were initially assessed at our center before 6 months of age and received any procedural intervention including Botox treatment. Patients with pan-plexus injury or greater than neurapraxic injuries to C8 and T1, as well as patients who never had a single procedural intervention were excluded.
Study patients were divided into 2 cohorts: the historical group, patients born before the institution of the Sup-ER protocol (2001-2007), and the recent group, patients born after the institution of Sup-ER protocol (2008-2018).
Data Collection and Analysis
Data were collected from the BCCH Brachial Plexus Clinic database and patients’ complete hospital records.
Demographic data and interventions
Data collected included patients’ year of birth, sex, age at visits and at interventions, and types of intervention. The interventions included Botox injections, BPEG, TT, distal nerve transfer, and osteotomy.
Age at first visit, average follow-up period, frequency of interventions, and average age at interventions were compared between the historical and recent groups.
Functional outcomes
Toronto Active Movement Scale (AMS) 18 score had been proactively recorded in the database for all patients at the time of their clinical visits. For this study, scores were collected from as close to the following time points as possible: 0, 6, 12, 18, and 24 months of age (±3 months). If there was more than 1 score or visit within a certain time period, the visit closest to the specified time point was used. If there was no visit in a specific time period, but the patient had the same score during their visits prior to and after that period, their score was assumed to remain the same. If there was no visit in a specific time period, but the patient did not have the same score during their visits prior to and after that period, no score was entered during data collection.
Data collection regarding TTs.
The rate of TT surgery was of specific interest to us. In our hospital, TTs are performed by orthopedic surgeons and over the study period, have been generally in the pattern of Hoffer, 19 but always at least including release of latissimus dorsi and transfer to the posterior shoulder capsule. For the past 10 years, our current orthopedic surgeon focuses on subscapularis slide and transfer of latissimus ± teres major to the posterior capsule, with rare release of pectoralis major. Preoperative function and indications for TT surgery and 6-month postoperative outcomes were collected from our database and orthopedic clinic notes found in the patient’s full hospital record.
(a) Interpreting different reporting methods
Orthopedic notes variously expressed results as functional descriptions, AMS scores, and/or degrees of ROM. We created a process to report them as consistent, comparable data points. There were several challenges:
The Hospital for Sick Children Active Movement Scale scores ER as starting from 0° with the hand at the abdomen, with increasing scores through a 180° range, and AMS 3 of 7 as the neutral midpoint. This differs from orthopedic ER descriptions which classically assign “0” degrees as neutral anterior midpoint and measure a 90° range into either internal or external rotation. To provide consistency in this study, we chose, in addition to AMS, to describe external and internal rotation as angles measured from that classic neutral midpoint.
When some orthopedic charts were reviewed, specific angle measurements were not recorded, nor AMS scores, but descriptive language documented the range. In those cases, 2 authors independently reviewed and converted ER functional descriptions and/or AMS scores to the closest estimated degrees of ER ROM, and vice versa. Consensus was required before each data point was assigned. For instance, an AMS score of 3 was assigned to the classic 0° and an AMS score of 2 was correlated to −45° ER. An AMS score of 7 related to 90° ER, and AMS scores of 4, 5, and 6 were estimated as incremental steps between neutral and 90°.
To complicate data collection further, in some of the early group, ER angle measurements had been routinely recorded with “0” degrees assigned to match the hand-on-abdomen AMS “0” point. For the purposes of this study, these angles were converted to reflect the orthopedic description of “0” at neutral midpoint: hand-on-abdomen would now become −90° ER. Having now learned of these inconsistencies, we now proactively also record active and passive ER and Sup range as angles measured from the orthopedic “0,” beside the AMS scores in our database.
(b) Choosing data points chronologically
If there was no 6-month postoperative clinical evaluation, the evaluation closest to this date was used.
Comparisons
Preoperative and postoperative TT ER ROM data points were compared between the historical and recent groups.
As this study included only clinic patients who had undergone any type of procedure, a change in pattern of TTs could have been confounded by a change in surgical indications in our clinic. Therefore, we additionally reviewed the rest of the clinic database for preoperative ER, shoulder flexion, and shoulder abduction of patients at the same age who had not had any procedures. External rotation AMS scores of 4 or less at the same age prompted a patient chart review to determine why no procedure was undertaken.
Results
Study Participants
A total of 264 patients diagnosed with BPBI were seen at BCCH from 2001 to 2018 and were screened for inclusion in the study. Of these 264 patients, 40 were excluded for the following reasons: first visit after 6 months of age (n = 31), pan-plexus type of injury (n = 6), first visit after 6 months of age and pan-plexus injury (n = 2), or early loss to follow-up (n = 1). The focus of this study was to look specifically at procedures, whether there were changes in timing and type in our clinic population after the institution of the Sup-ER protocol. Therefore, from the remaining 224 patients, 181 patients who did not have any procedural intervention (including Botox) were excluded. In total, 43 patients met the inclusion criteria, with 20 in the historical group (11 female, 9 male) and 23 in the recent group (16 female, 7 male). The mean age at the first visit was 2.1 months (SD = 1.3) in the historical group and 2.0 months (SD = 1.1) in the recent group. The mean follow-up period in years was 10.3 (SD = 3.9) in the historical group and 5.9 (SD = 2.5) in the recent group.
Interventions
The patients in both the historical (N = 20) and recent (N = 23) groups each had a total of 36 procedures. The recent group had significantly fewer BPEG surgeries compared with the historical group (n = 3, 13% vs n = 11, 55%), and these were performed at an earlier mean age (4.0 months vs 6.7 months). No BPEG surgeries were performed after 5 months of age in the recent group. In both groups, BPEGs were performed under general anesthetic with a resection of neuroma, usually an accessory nerve to suprascapular nerve transfer, and bilateral sural nerve harvest for grafting. Grafts were reversed and coapted to nerve roots and distal segments that were free of scar as confirmed by a pathologist, using fibrin glue. The senior author was the primary surgeon for all patients in both groups. Note should be made that in the recent group, patients with BPEG were immobilized with flexible elastic tape (with skin protected by film dressing) in the externally rotated position for 3 weeks postoperatively (Figure 1). Where “later” BPEG had been indicated by the Hospital for Sick Children algorithm in the historical group, more focused direct nerve transfers were more commonly possible in the recent group. In the historical group, nerve transfers were undertaken in 2 patients: intercostal to musculocutaneous nerve in 1 patient, and Oberlin (ulnar fascicle to biceps branch) in the other. In the recent group, 5 Oberlin transfers were undertaken, 1 in combination with an end-to-side medial head triceps branch to axillary nerve, and 1 patient had isolated medial triceps branch to deltoid branch of axillary nerve transfer. These were all performed by an experienced peripheral nerve surgeon in conjunction with the senior author and based on specific clinical weakness patterns. The recent group also had fewer TT operations (39% vs 75%), and these were performed at an earlier mean age (4.8 vs 5.6 years).

Upper limb positioning postbrachial plexus exploration (Right) to mimic preoperative positioning in the supination-external rotation splint (Left).
Where Botox was indicated, 10 units/kg were shared between pectoralis major and subscapularis via muscle stimulation injection. Botox injections were performed more commonly (65% vs 25%) and at an earlier age (10.5 months vs 24.2 months) in the recent group compared with the historical group (Figure 2) but appear to be reduced toward the end of the recent group study period. We instituted a functional elbow constraint device limiting the elbow forward habit around that time, in 2015 (Figure 3).
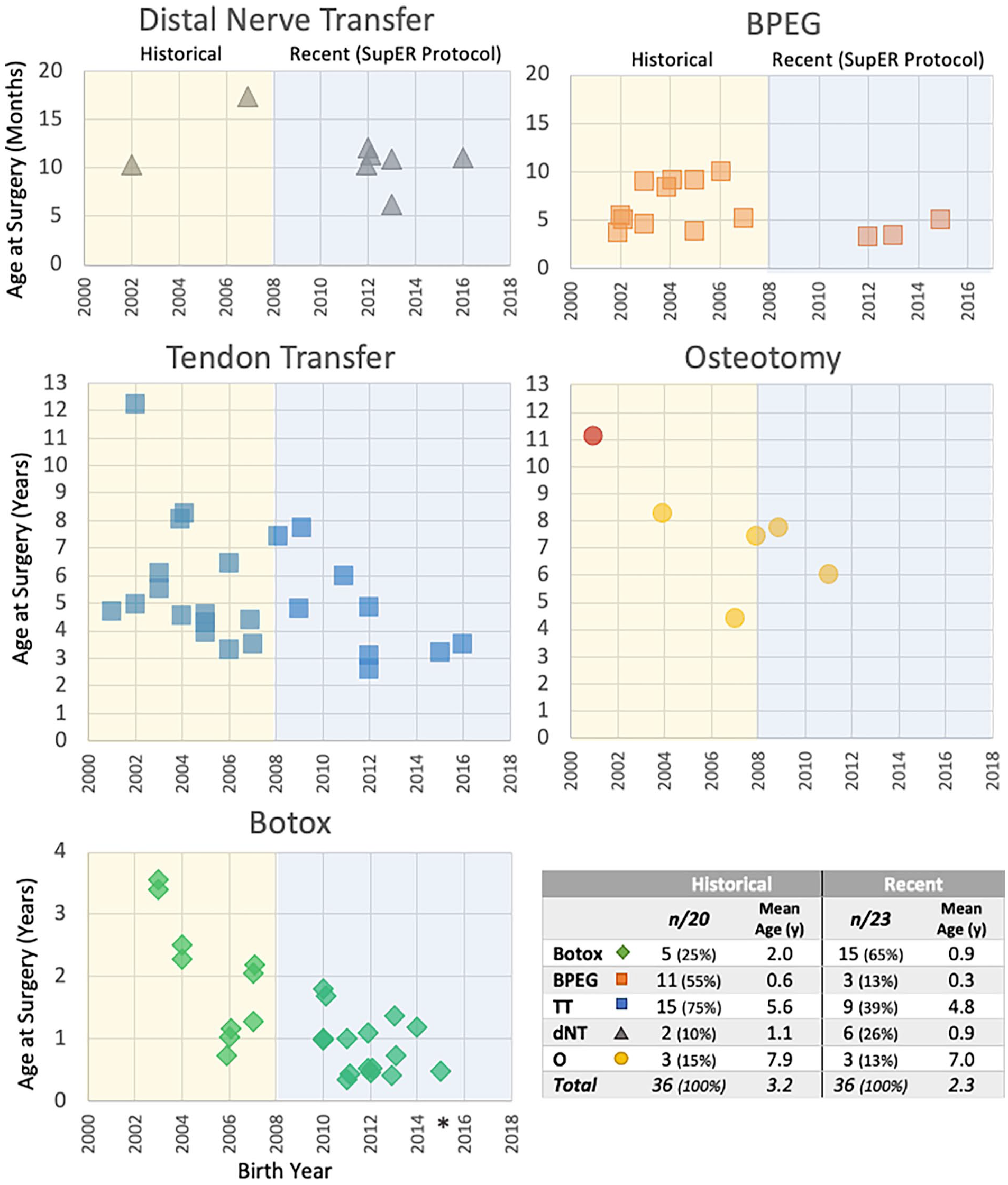
All interventions on study patients by birth year.
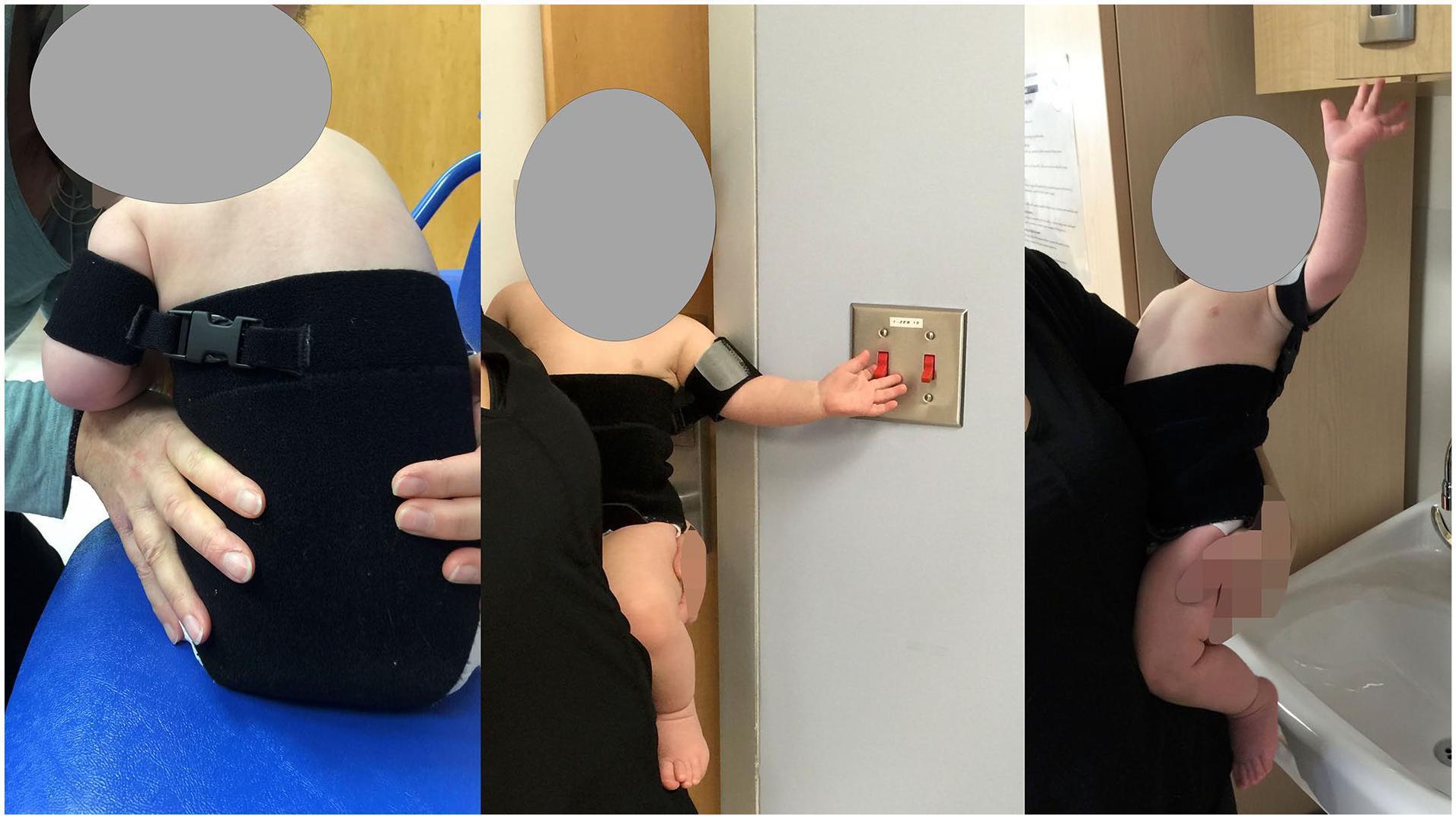
Elbow forward constraint band.
Six patients had upper extremity osteotomies, 3 in each study group. Five were glenoid osteotomies, and the only humeral osteotomy was performed on a patient in the historical group.
Functional Outcomes
Patients in the recent group had consistently better functional outcomes at 24 months than patients in the historical group in both active ER and Sup (Figure 4). The mean ER and Sup at 24 months were each 1.3 AMS units better in the recent group than in the historical group. The difference in mean ER between the historical and recent groups was statistically significant at 12 (P = .002), 18 (P = .003), and 24 months (P = .009). The difference in mean Sup AMS scores between the historical and recent groups was statistically significant at 6 (P = .004), 12 (P < .001), 18 (P < .001), and 24 months (P = .009). Mean elbow flexion at 12 months was 1.2 AMS units better (P = .031) in the recent group, but by 2 years of age, the scores were similar (P = .142).
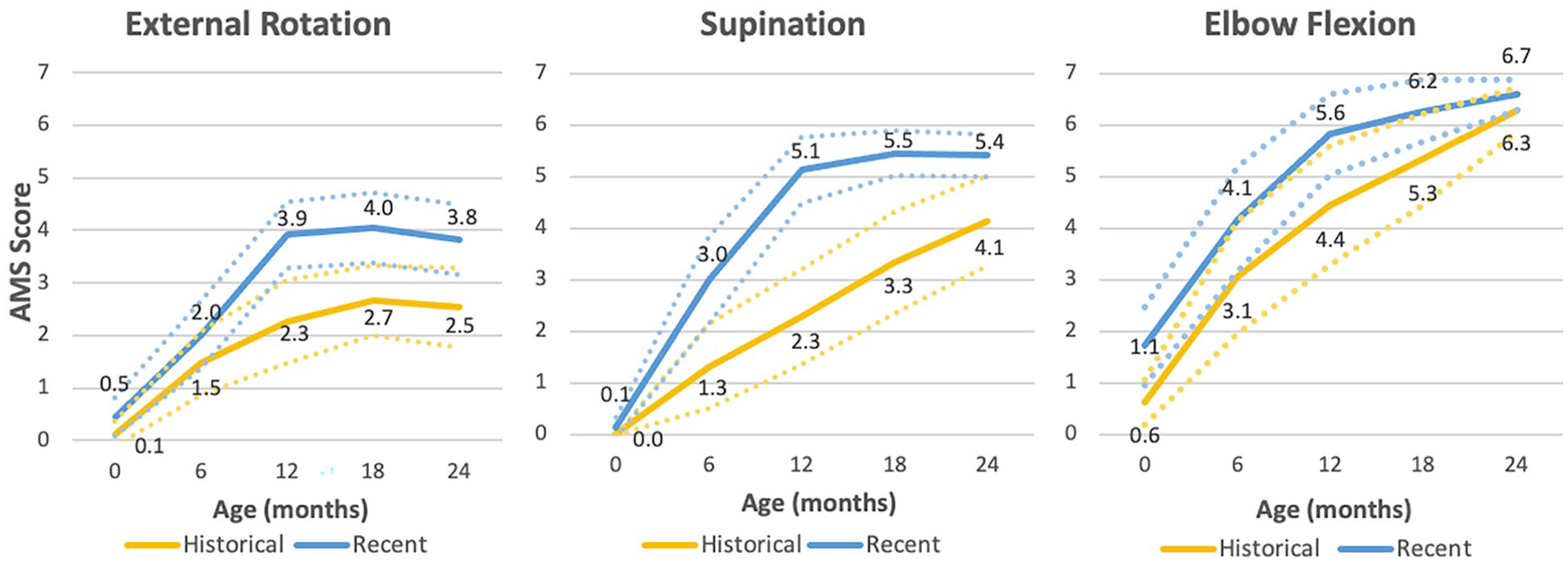
Active Moment Scale (AMS) scores by age and by group for external rotation (ER), supination (Sup), and elbow flexion.
Tendon Transfers
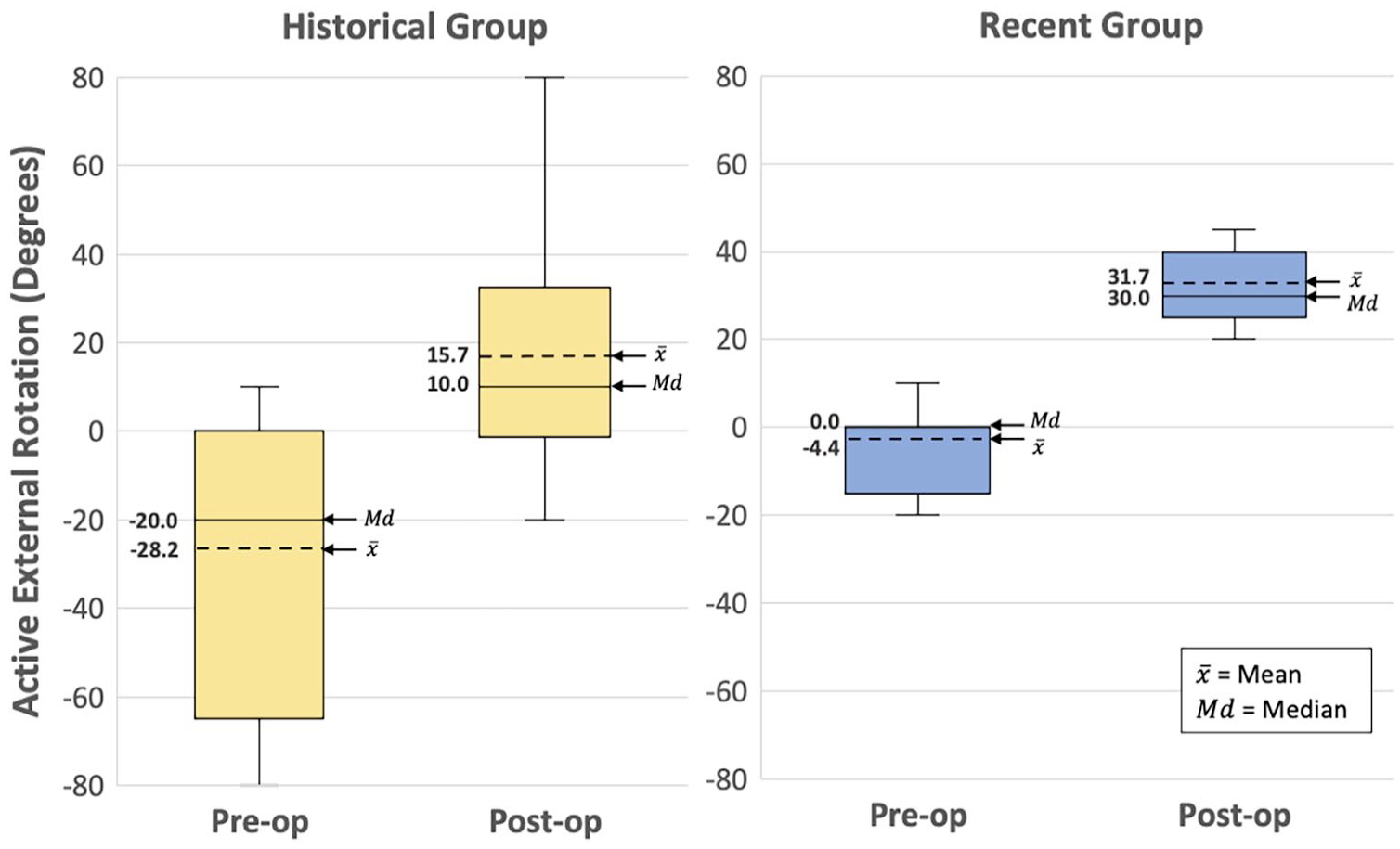
Compared with the historical group, fewer patients in the recent group had TTs (9 vs 15), and patients in the recent group started with 24° greater (P = .0135) preoperative ER ROM and ended with 16° greater (P = .0255) 6-month postoperative ER ROM compared with those in the historical group (Figure 5). In the recent group, there was less intragroup variability of preoperative and postoperative ER ROM compared with that in the historical group (Figure 6).
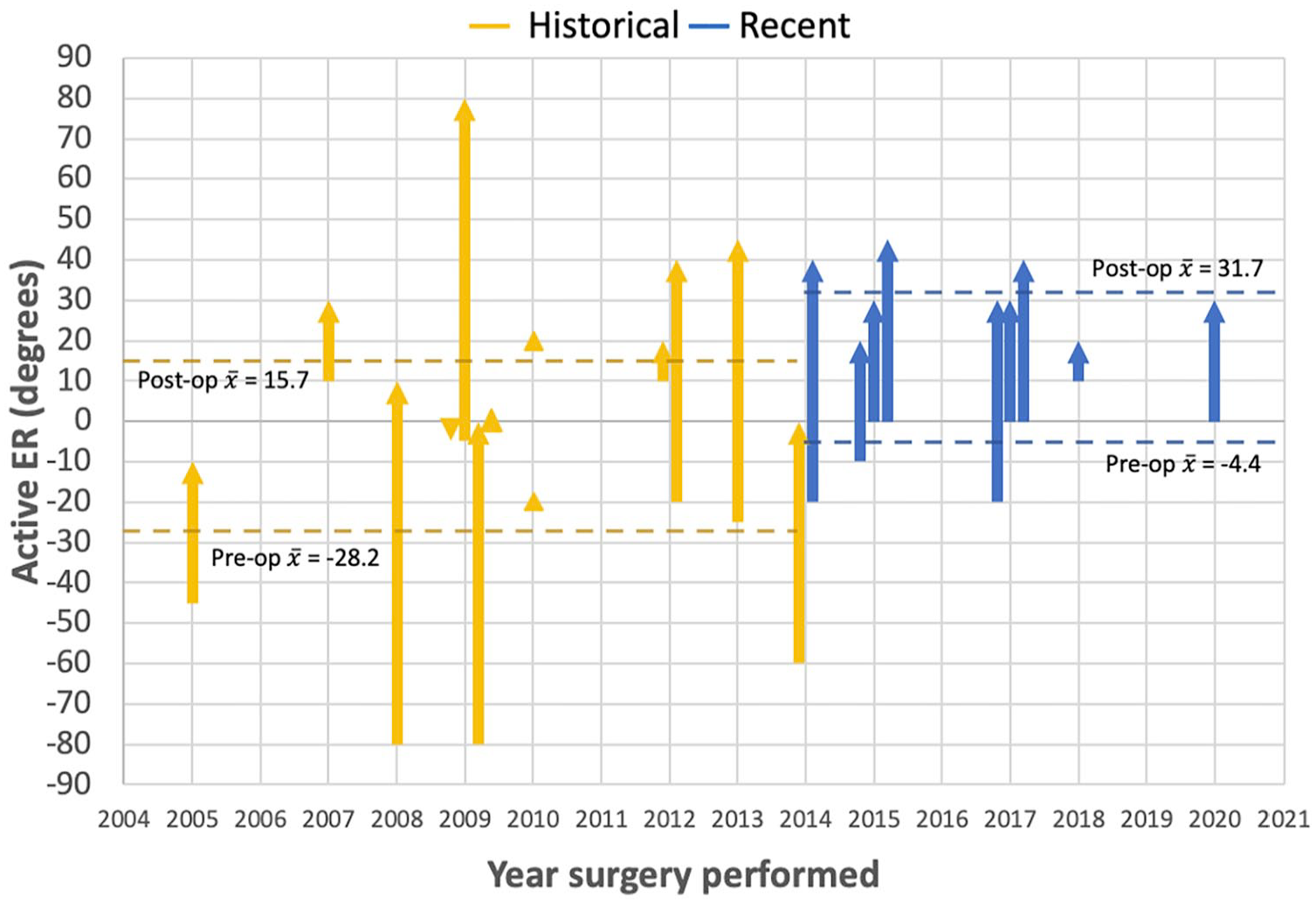
Changes in ER from tendon transfer surgeries of individual patients.
Intragroup variability of active preoperative and postoperative external rotation in patients with tendon transfer surgeries.
We wanted to reassure ourselves that the decrease in TTs did not simply reflect a change in surgical indications between the groups. Thus, we returned to our complete database to find whether there were patients at 5 years of age with ER scores of less than or equal to AMS 4 (which reasonably might have led to a recommendation of TT) who had been excluded from the study group because they had not undergone at least 1 procedure. We identified 12 such patients in the excluded historical group and 8 in the excluded recent group, prompting review of their charts to determine why they did not undergo TT. Despite their ER scores, all these patients had excellent shoulder flexion and shoulder abduction (AMS ≥ 6), considered a relative contraindication for TT by the orthopedic surgeon at that time (Figure 7). There were 2 patients in the historical group and 0 in the recent group for whom TT had been recommended but declined by the family.
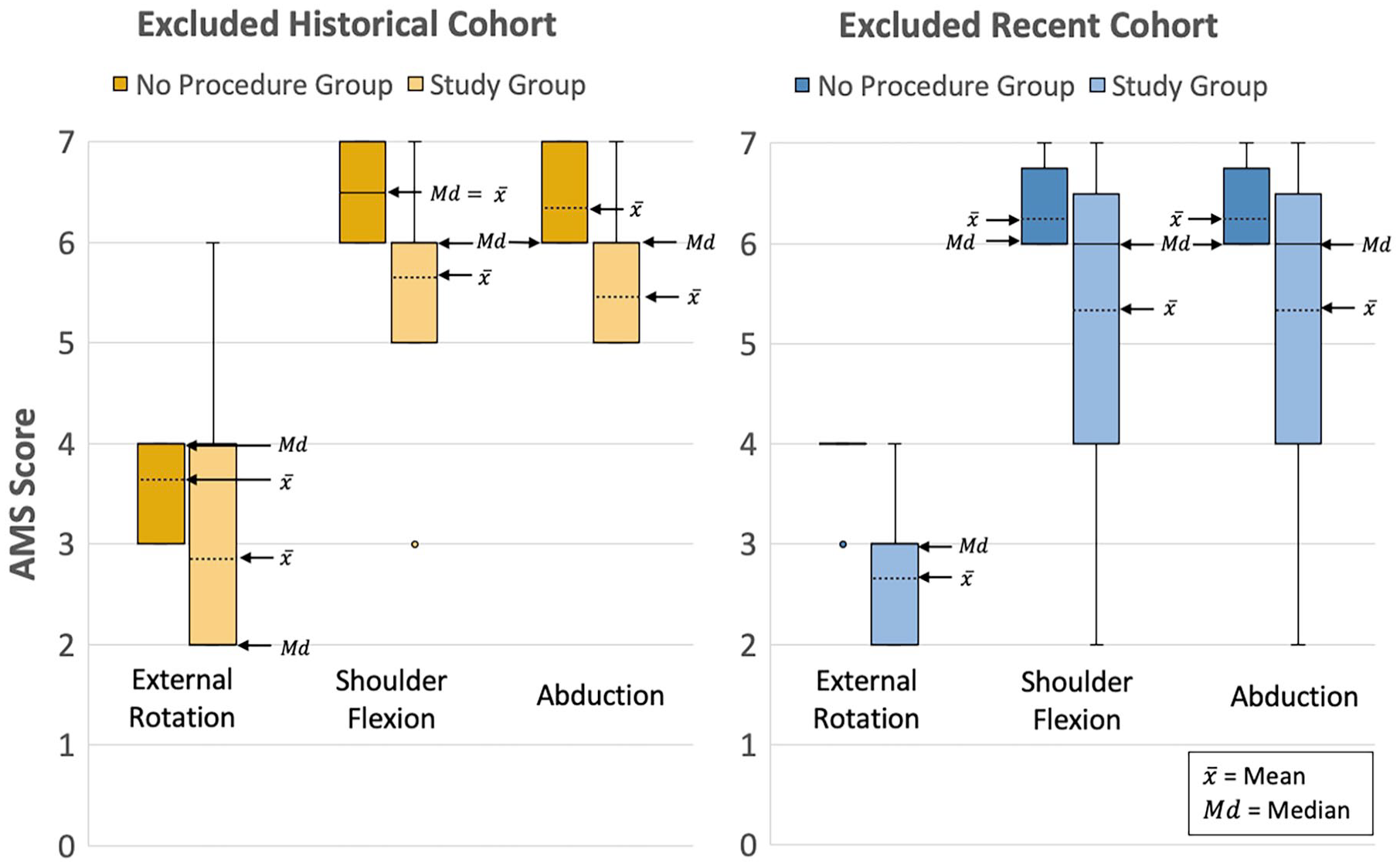
Shoulder AMS scores of patients who underwent tendon transfer surgery compared with patients who had last recorded ER ≤4 but underwent no procedures.
Discussion
The objective of this project was to examine how the pattern of interventions evolved in the decade after the institution of the Sup-ER protocol in a brachial plexus clinic population.
BPEG/Nerve Transfer
In our clinic, the indications for BPEG were formerly based on the Hospital for Sick Children algorithm, 20 including the “cookie test” at 9 months. Children with the most severe brachial plexus injuries still had indications for early BPEG at 3 months, but after institution of the Sup-ER protocol, far fewer Erb’s type patients failed the 9-month “cookie test.” We posited that the improved position and function of the shoulder optimized elbow flexion mechanics, allowing the elbow movement to more accurately reflect the degree of nerve recovery. The hand and forearm raising a cookie to the mouth while in a position of shoulder internal rotation are often restricted by the abdomen and trunk, making “failure” a more likely outcome. Better growth and congruency of the glenohumeral joint similarly allows the testing of shoulder abduction and flexion to more accurately reflect nerve recovery rather than having results confounded by shoulder mechanical restriction. At the 9-month visit, if we found elbow flexion weakness, it was more certainly nerve recovery related and usually more isolated, prompting a decision to offer nerve transfers instead of BPEG. Our results show an absolute decrease in the number of BPEGs and the age at which they were performed. In the recent group, no BPEG was performed after 5 months of age, and the tripling of nerve transfers reflects the change in preferred interventions, when nerve surgery was indicated at all, for these patients.
Botox
The recent group had 3 times more and earlier Botox injections, as it was used preventively in conjunction with the Sup-ER protocol to improve shoulder imbalances. We recommended Botox when there was evidence of a mild recurrence of internal rotation tightness or elbow forward habit, as early as 4 months of age. Although our data are not robust enough yet to confirm a causal relationship, the decrease in Botox use in the latter part of the recent group reflects increasing use of a functional elbow constraint device, which appears to show at least some promise in reducing the elbow forward habit. Anecdotal evidence suggests that functional internal rotation may have at least some habitual component. Preventing the ability to bring the elbow fully forward during active use has resulted in correction of this habit sometimes within a month. Our clinic volumes cannot allow us to determine whether this is a direct cause-and-effect relationship, but it is our impression that patients improve their functional ER after wearing the device, and Botox is less indicated.
Tendon Transfer
We were very interested in whether the number of TTs would change in the group exposed to the Sup-ER protocol.
Almost half as many TTs were documented in the recent group and those were performed on patients with better preoperative ER scores and resulted in better postoperative ER scores. With that, we recognize that our recent goals for TTs have evolved from salvaging severe IR/ER imbalance to proactively aiming to achieve ROM closer to normal.
The range of preoperative ER scores for patients undergoing TTs was much narrower in the recent group, which we feel is a result of the closer monitoring we now practice.
By examining the chart details of patients in the expanded recent and historical groups who did not undergo TT surgery with ER less than or equal to AMS 4, we confirmed that a change in indications between time periods was likely not a confounding factor. In all groups, orthopedic surgery notes consistently documented a relative contraindication for surgery if shoulder abduction and flexion was excellent.
Two patients in the historical group had been recommended to have TT but declined, while none declined in the recent group, thus eliminating another potential confounding factor.
Osteotomy
Osteotomy was historically considered to be a salvage procedure where the humerus was rotated to centralize the rotational arc of motion to fall within the most functional range. More recently, our osteotomy of choice is of the glenoid in conjunction with TTs, and is used proactively to attempt to normalize rotational ROM and shoulder anatomy.
Supination and Elbow Flexion
The recent group also showed better functional outcomes for Sup, consistent with our previous pilot study. No interventions for Sup were documented in either group. Elbow flexion at 2 years in both groups was similarly good, providing reassurance that early splinting in elbow extension did not negatively affect elbow flexion outcome.
Management Guidelines
There are few studies that examine timing and patterns of interventions in BPBI. General principles of management in most centers are widely accepted, including early diagnosis and assessment of function, intensive physical therapy, early nerve surgical intervention where indicated, and secondary reconstruction for residual deformities if needed. 21 The first decision for nerve surgery often takes place at around 3 months of age.20-22 At that age, exploration and nerve grafting is usually recommended for children with absent biceps function, evidence of significant root avulsion, or lower brachial plexus injuries. Brachial plexus exploration has also been recommended for children approximately 6 to 9 months of age who have regained limited elbow flexion strength in the context of an upper brachial plexus injury. 20 Incomplete nerve recovery, with or without nerve surgery, often leads to predictable joint growth abnormalities and permanent shoulder imbalance issues.21,23,24
In our clinic, we had initially followed these general recommendations, but patterns of practice gradually evolved after the institution of the Sup-ER protocol in 2008, including the following:
a. We stopped performing later BPEG in upper plexus injuries. Instead, where elbow flexion was weak enough at 9 months, more focused direct nerve transfers were possible and usually performed between 10 and 12 months of age.
b. We do fewer TTs on patients, with better preoperative ER indication scores, and an expectation of better postoperative results. Tendon transfer is no longer salvage; instead, it is considered a proactive step that may achieve closer-to-normal function.
c. We have a tendency toward more frequent and earlier Botox treatment.
d. We have changed our method of documenting ER and Sup to provide more consistently comparable data than AMS scores alone provide.
e. The institution of the Sup-ER protocol did not result in any unfavorable trends in intervention patterns or worsening of measured outcomes.
Current Canadian national clinical practice guidelines for BPBI 5 have been established. Consideration could be given to add early Sup-ER protocol implementation as a baseline recommendation in these guidelines.
The Canadian guidelines recommend using common data sets such as AMS for baseline and outcome measures. We should work toward universal agreement on the vast expression of ER scores. AMS scores alone are often not specific enough to allow meaningful clinical comparisons, and we would support an agreement to express ER and Sup as angles from neutral midpoint.
Limitations
As a retrospective study, there were limits to the quality and comprehensiveness of the available data. Some of the recorded ER ROM measurements were available only as degrees or only as AMS scores, so 2 researchers independently converted them for comparison. While we followed consistent conversion rules and achieved consensus, there may still be room for a degree of conversion error. Statistically significant conclusions about the timing and frequency of distal nerve transfers and osteotomies could not be drawn due to the infrequency of both procedures. Especially in the historical group, our follow-up was less frequent and consistent after 2 years of age, and there were insufficient data to plot comparative outcomes beyond 24 months of age. Our more recent protocols involve more frequent follow-up. Finally, the pattern, frequency, compliance, and accurate timeline of individual Sup-ER splint use were inconsistently recorded, limiting our ability to make strong conclusions relating patterns of Sup-ER splint use to specific requirements for surgical procedures or to functional outcomes.
Conclusion
Following institution of the Sup-ER protocol in our clinic, we performed fewer BPEG surgeries and only those indicated at 3 months of age. We now perform the more predictable direct nerve transfers instead of the BPEG surgery that had previously been recommended at 9 months of age. Our rate of shoulder TTs has decreased, and the procedure is used to more proactively achieve closer-to-normal range rather than as a salvage technique. Humeral derotational osteotomies have decreased and are not seen in our recent group. Glenoid osteotomies within TTs are rare in both groups.
We believe that institution of the Sup-ER protocol in our clinic has resulted in positive changes to patterns of intervention compared with historical practice and improved outcomes for our patients.
Footnotes
Ethical Approval
This study was approved by the University of British Columbia Children and Women’s Research Ethics Board (H20-01297).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
A waiver of informed consent was obtained from our ethics board to collect data for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: V.C.Y.W. was awarded a Summer Student Research Program grant from the University of British Columbia for this study.