
Abstract
Background:
Radial head fractures are often associated with poor outcomes. Both open reduction and internal fixation (ORIF) and radial head arthroplasty (RHA) might be considered in operative cases. This study aimed to compare long-term patient-reported functional outcomes among patients with operatively treated radial head fractures.
Methods:
A cross sectional study conducted at a Level I trauma center was used to identify patients with a radial head fracture who underwent ORIF or RHA between 2006 and 2018, and agreed to complete a survey in 2020. The primary outcome measure was the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score.
Results:
Seventy-six patients participated in the study. No significant differences in outcomes were observed between groups. QuickDASH scores were similar for both groups (ORIF: mean = 15.7, SD = 18.4; RHA: mean = 22.8, SD = 18.6; mean difference = 0.2 [-9.0 to 9.3], P = .97). Nineteen (37%) ORIF patients and 12 (48%) RHA patients reported a need for pain medication (adjusted odds ratio [OR] = 0.8 [0.3-2.4], P = .70). Thirteen (25%) ORIF patients and 6 (24%) RHA patients required additional surgery (adjusted OR = 1.7 [0.5-6.2], P = .39). A subgroup analysis of multi-fragmentary fractures revealed similar findings.
Conclusion:
Patient-reported outcomes, which included a subgroup analysis of multi-fragmentary fractures, were similar between ORIF and RHA groups at an average of 7.5 years from surgery. Reconstructing the radial head might not result in worse outcomes than RHA when both options are employed according to the best judgment of the operating surgeon.
Keywords
Introduction
Radial head fractures represent a significant proportion of elbow injuries, and the outcome for these types of injuries are often poor. The goal of treatment is to achieve elbow stability and pain-free range of motion. In operative cases, both open reduction and internal fixation (ORIF) and radial head arthroplasty (RHA) might be considered. The choice between ORIF or RHA to optimize outcomes in radial head fracture treatment remains a topic of controversy.
Several studies1,2 report unsatisfactory function and postoperative complication rates among patients treated with ORIF particularly for multi-fragmentary fractures, which suggests that surgeons should have a low threshold for choosing RHA for patients with complex fractures over ORIF. However, a recent meta-analysis comparing ORIF and RHA cautions that long-term follow-up data are needed to determine if the ostensible benefits of RHA are counteracted by late complications.3,4
Currently, most evidence on this topic is derived from small, short- to mid-term studies, many of which lack patient-reported outcome measures. To our knowledge, no published study exists comparing long-term patient-reported functional outcome data between these 2 groups. The aim of the current study was to compare long-term patient-reported functional outcomes between patients who were treated with ORIF or RHA for a radial head fracture. We hypothesized that arthroplasty would have better long-term functional outcomes than ORIF, particularly for patients with 3 or more fracture fragments.
Materials and Methods
Study Design and Participants
We conducted a cross-sectional study at a single, urban academic trauma center after receiving institutional review board approval. Potential patients were sourced from an institutional database of operative radial head fractures, constructed by data retrieval from the hospital billing database using Current Procedural Terminology (CPT) codes and International Disease Classification, Ninth Edition codes and medical record review. Eligible patients included consecutive adult patients with a radial head fracture treated with either ORIF or RHA between 2006 and 2018. Radial head fractures with other associated injuries were included, such as terrible triad injuries. All eligible patients were attempted to be contacted to complete a patient-reported outcome questionnaire over the phone. Exclusion criteria were less than 1 follow-up visit or inability to complete the questionnaire in English.
Outcomes and Covariates
The primary outcome was patient-reported function measured using the QuickDASH questionnaire. The QuickDASH is a validated, shortened iteration of the Disabilities of the Arm, Shoulder, and Hand (DASH) outcome questionnaire used to measure self-reported disability among upper extremity injury patients. 5 The questionnaire comprises 11 items scored by patients from 1 to 5. Scale scoring from the item scores is then calculated from 0 to 100, with lower score indicating lower level of disability. The QuickDASH is validated for written and verbal administration. 6
Secondary outcomes included unplanned reoperation, range of motion, pain at last follow-up visit, and use of pain medication. Secondary outcome data and demographic data (age, sex, and body mass index [BMI]) were obtained through a retrospective chart review and through 2 additional questions added to the QuickDASH questionnaire related to use of pain medication and any additional surgery on the affected arm since the last follow-up visit at the primary treating center.
Fracture characteristics were determined by fellowship-trained upper extremity orthopedic surgeons. Radiographic evaluation and clinical notes were used to classify the fracture pattern and Mason type of each injury. Surgeons also determined radial head comminution, fragment number, and presence and direction of dislocation where applicable. Fracture patterns were classified into isolated, olecranon, terrible triad, and Monteggia subtypes. Mason type was classified as 1, 2, or 3, while Mason type 4 fractures were classified by fracture pattern in the aforementioned categories of transolecranon fractures, terrible triad fractures, and Monteggia subtypes. When classifying Mason type 2 fractures, the constant portion of the radial head was not counted as a fragment in the total accounting of fracture fragment number.
Statistical Analysis
A power calculation determined that at least 17 patients were required in each treatment arm to have at least 80% power to detect a 15-point difference in the QuickDASH, assuming a standard deviation of 15 points and an alpha of 0.05. The mean outcome difference of 15 was chosen to reflect the minimum clinically important difference for the QuickDASH. 7 Our study is powered for the primary analysis of difference in QuickDASH scores of 15 points between all study participants. Subgroup analyses are underpowered and exploratory should be considered as exploratory.
Patient demographic and injury characteristics were analyzed using Student’s t-test for continuous variables, Pearson’s chi-square test for categorical variables, and Fisher’s exact test for variables with 20% of expected cell counts fewer than 5 observations. To adjust for potential treatment biases between patients who underwent ORIF and those who underwent RHA, association between treatment and study outcomes was analyzed with a regression model that included Mason type and soft tissue injury.
We performed 3 subgroup analyses, stratifying the sample based on age (<55 years vs ≥55 years), BMI (<30 km/m2 vs ≥30 km/m2), and in a subset of patients with 3 or more fracture fragments. Among the subgroup of patients with 3 or more fracture fragments, we had an insufficient number of patients with supination <85 degrees, flexion <145 degrees, extension >0 degrees, and pain measures at last follow-up and were, therefore, unable to calculate between-treatment differences in this subgroup. Association of outcomes between treatment group by fracture type could not be analyzed with regression modeling because of insufficient numbers of patients with each fracture type. Instead, outcomes by fracture type were analyzed with Fisher’s exact test for categorical outcomes (reoperations, arc of motion above or below 100 degrees, and pain at last follow-up) and student t-test for continuous outcome (QuickDASH). Neck, neck only, and Monteggia variants were too small to be included in the subgroup analysis.
Results
Three hundred eligible patients were identified (Figure 1). Three patients were deceased and 2 lacked mailing address information. The remaining 295 patients were sent an opt-out letter in the mail. Those patients who did not opt-out were approached via phone to complete the QuickDASH.
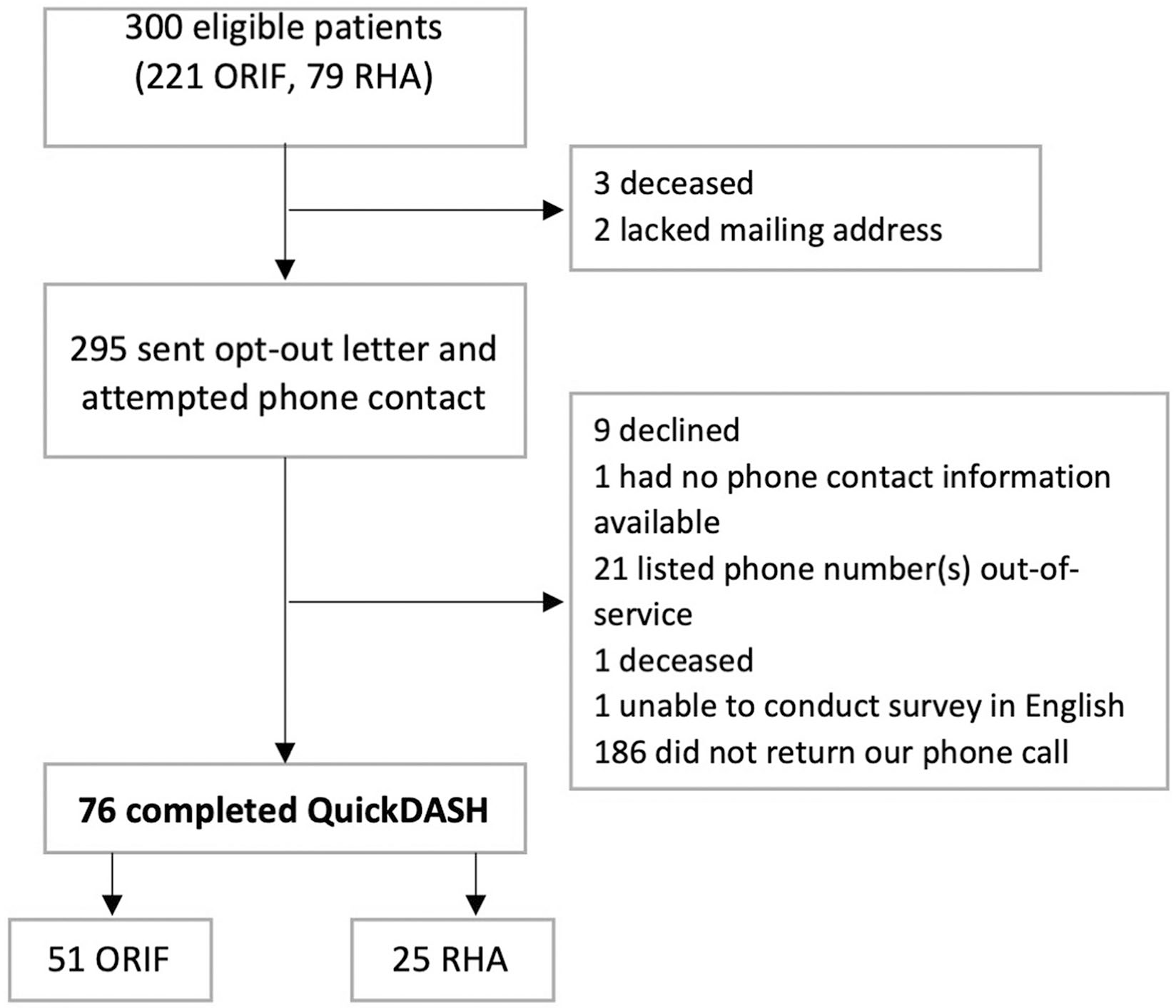
CONSORT diagram.
Seventy-six patients completed the QuickDASH, including 51 who underwent ORIF and 25 who underwent RHA. The mean age of the participants was 50.2 ± 14.4 years, 51% were male, and the mean BMI was 30.4 ± 6.4 km/m2. The mean time between surgery and QuickDASH completion was 7.5 ± 2.7 years (range: 2-13 years). Among the 33 participants with 3 or more fragment fractures, 21 underwent ORIF, and 12 underwent RHA.
Both treatment groups demonstrated differences. ORIF patients compared with arthroplasty patients were younger (mean age 45.8 years vs 59.1 years), less likely to be female (29% vs 88%), lower BMI (28.2 kg/m2 vs 34.9 kg/m2), less comminution (29% vs 64%), and less soft tissue injury (39% vs 68%) (Table 1). There were also differences among Mason types among patients (Table 1). Mason type 4 fractures were more common in RHA than ORIF (32% vs 14%).
Patient Demographics and Injury Characteristics.
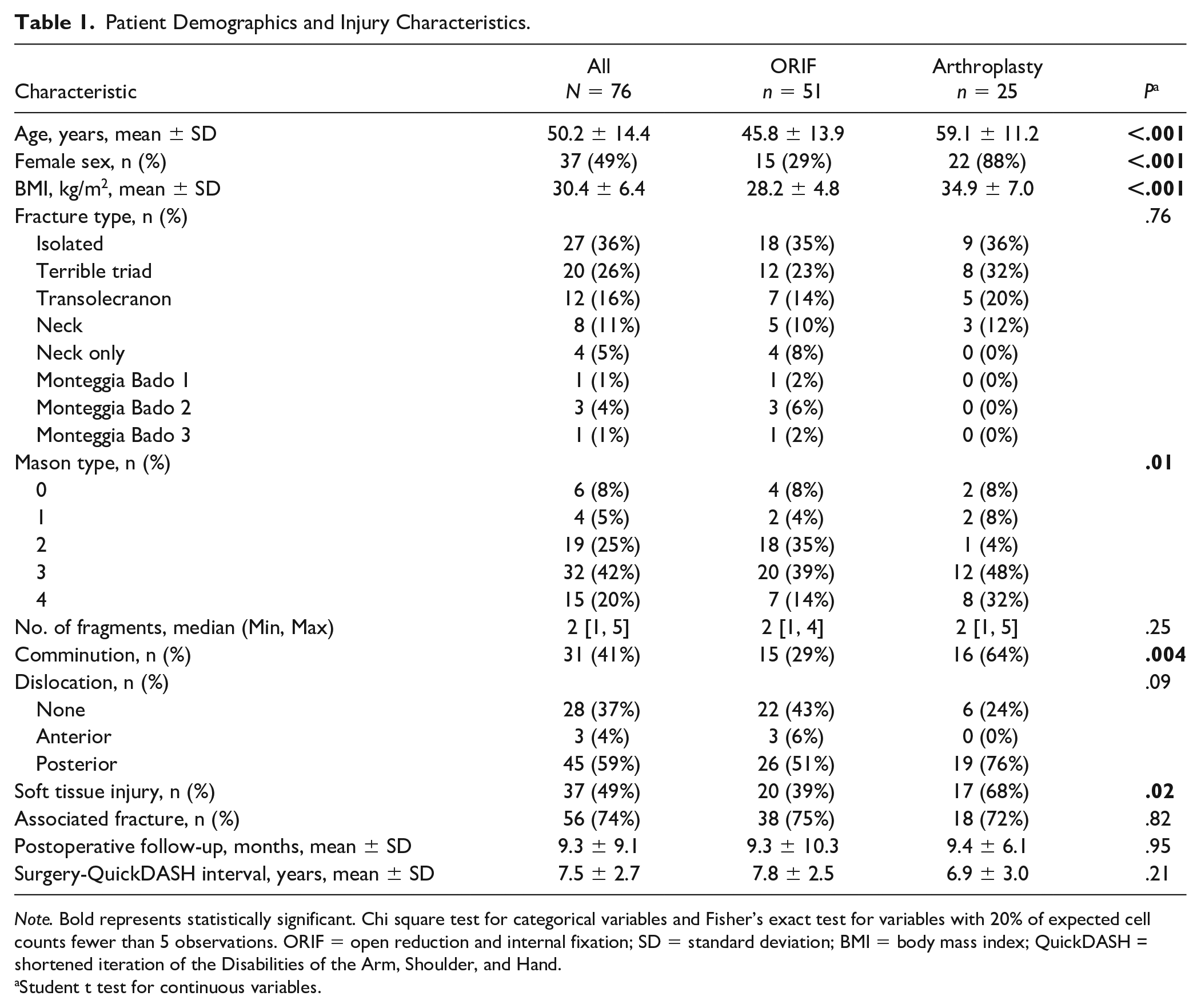
Note. Bold represents statistically significant. Chi square test for categorical variables and Fisher’s exact test for variables with 20% of expected cell counts fewer than 5 observations. ORIF = open reduction and internal fixation; SD = standard deviation; BMI = body mass index; QuickDASH = shortened iteration of the Disabilities of the Arm, Shoulder, and Hand.
Student t test for continuous variables.
Overall, no statistically significant differences in study outcomes were observed between the two treatment groups in both unadjusted and adjusted models (Table 2). QuickDASH scores were similar for both ORIF and RHA (mean difference = 0.2; 95% confidence interval [CI]: -9.0 to 9.3; P = .97). QuickDASH scores for both ORIF (15.7 ± 18.4) and RHA groups (22.8 ± 18.6) indicated a low level of disability. On average, the patients in both treatment groups included in this study recover to a level of function that is within 1 standard deviation of the general population, reported to be 10.1 ± 14.68. 8 Twenty-five percent of patients in the ORIF group and 40% of patients in the RHA group reported a need for pain medication (mean difference = 0.8; 95% CI: 0.3-2.4; P = .70). Thirteen (25%) patients in the ORIF group and 6 (24%) patients in the RHA group required reoperation on the affected arm after definitive treatment (mean difference = 1.1; 95% CI: 0.4-3.3; P = .89).
Association Between Treatment and Study Outcomes.
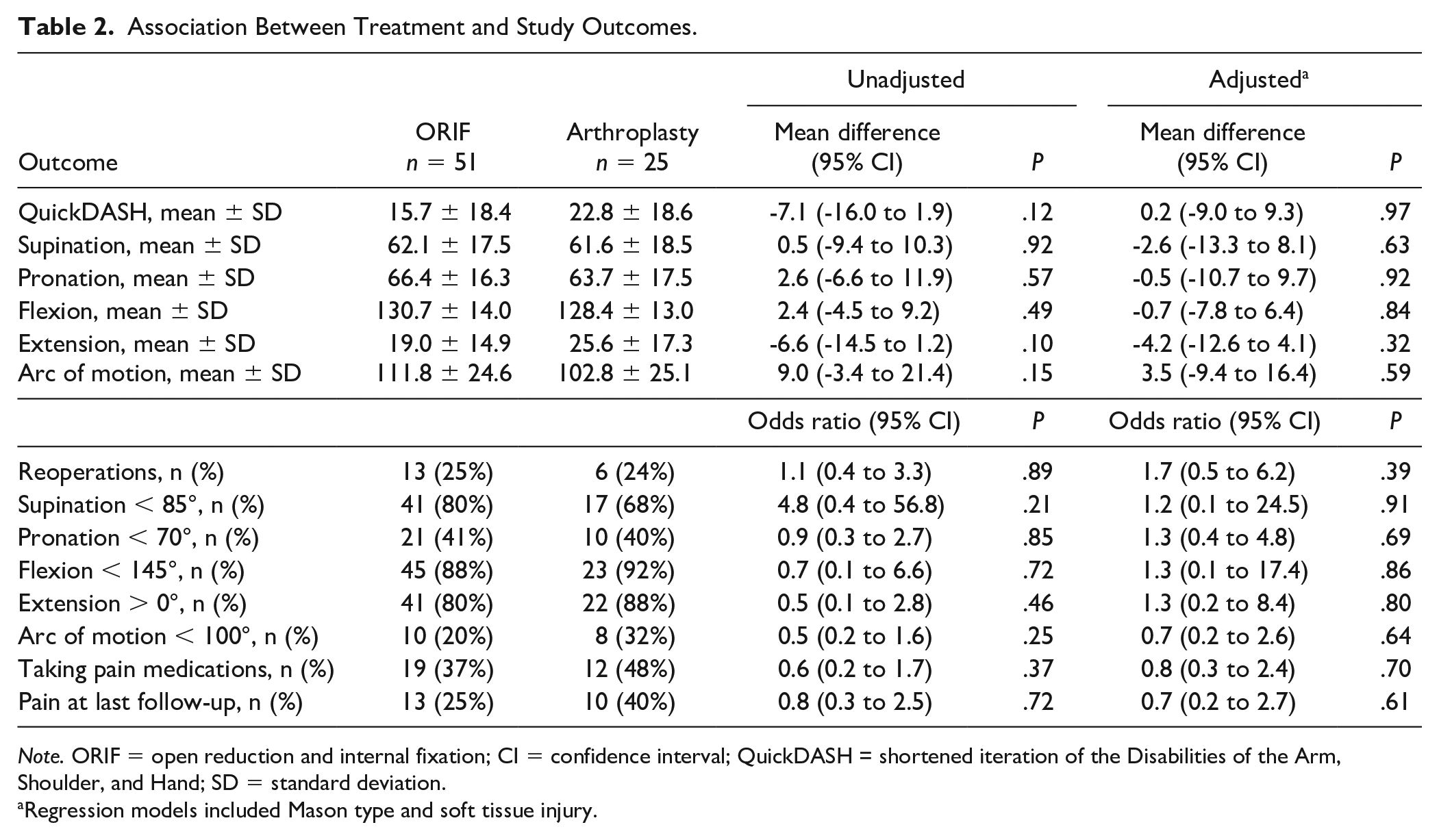
Note. ORIF = open reduction and internal fixation; CI = confidence interval; QuickDASH = shortened iteration of the Disabilities of the Arm, Shoulder, and Hand; SD = standard deviation.
Regression models included Mason type and soft tissue injury.
In a subset of patients with 3 or more fracture fragments, no statistically significant differences in study outcomes were observed between both treatment groups in both unadjusted and adjusted models (Table 3). As in the main group, QuickDASH scores were similar for ORIF patients (18.7 ± 17.2, n = 21) and RHA patients (26.1 ± 19.0, n = 12; mean difference = -4.4; 95% CI: -19.0 to 10.2; P = .54).
Association Between Treatment and Study Outcomes in Subset of Patients With 3 or More Fragments.
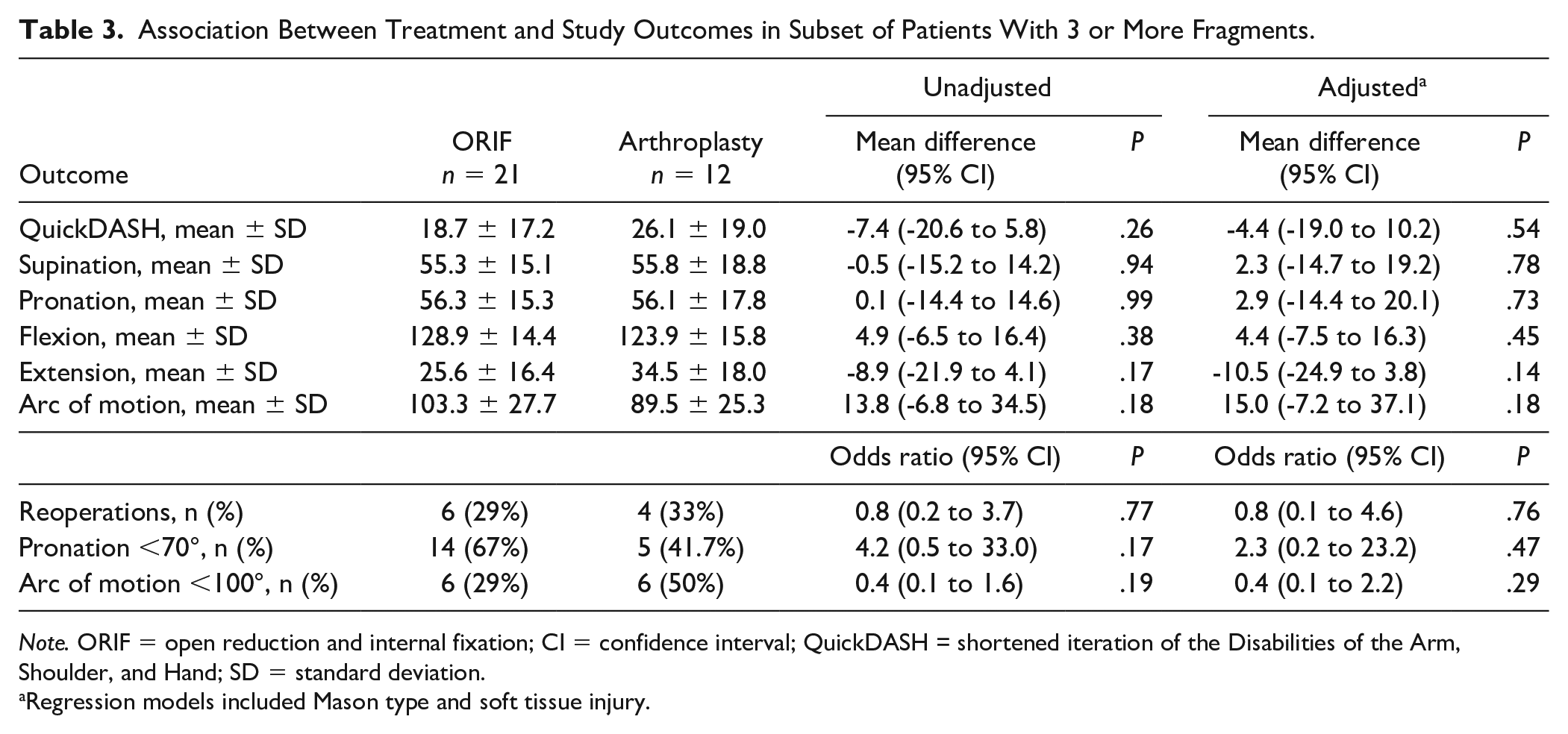
Note. ORIF = open reduction and internal fixation; CI = confidence interval; QuickDASH = shortened iteration of the Disabilities of the Arm, Shoulder, and Hand; SD = standard deviation.
Regression models included Mason type and soft tissue injury.
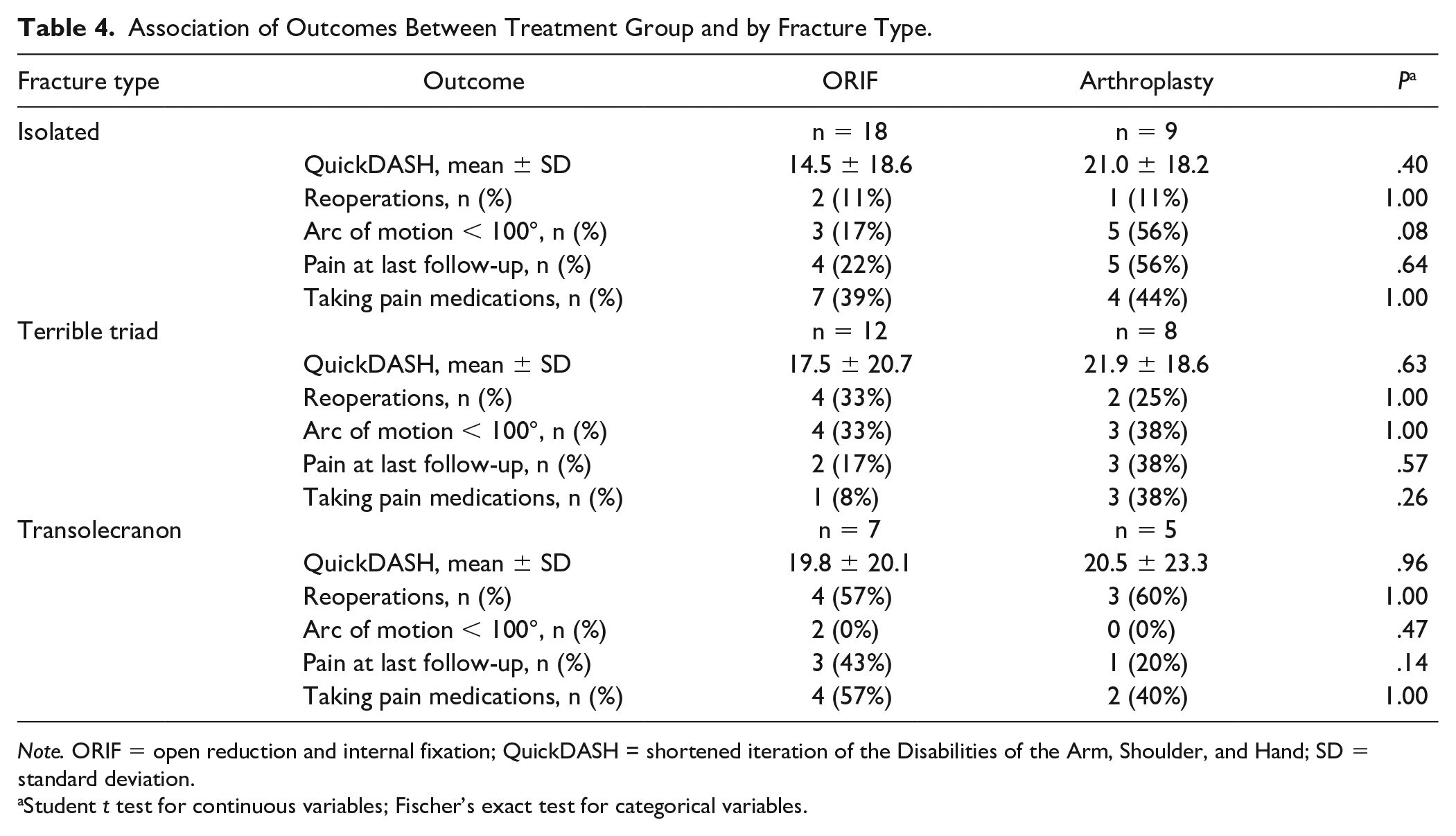
No statistically significant differences were observed in study outcomes between treatment groups by fracture types (Table 4). Isolated fractures represented 18 patients who underwent ORIF and 9 who underwent arthroplasty, with no significant difference in QuickDASH scores (ORIF 14.5 ± 18.6; RHA 21.0 ± 18.2, P = .40), pain medication (ORIF 39% vs RHA 44%, P = 1.0), or reoperation (ORIF 11% vs RHA 11%, P = 1.0). Terrible triad fractures represented 12 ORIF and 8 RHA cases, with no significant difference in QuickDASH scores (ORIF 17.5 ± 20.7 vs RHA 21.9 ± 18.6, P = .63), pain medication (ORIF 8% vs RHA 38%, P = .26), or reoperation (ORIF 33% vs RHA 25%, P = 1.0). Transolecranon fractures represented 7 ORIF and 5 RHA, similarly with no significant difference in QuickDASH scores (ORIF 19.8 ± 20.1; RHA 20.5 ± 23.3, P = .96), pain medication (ORIF 57% vs. RHA 40%, P = 1.0), or reoperation (ORIF 57%, RHA 60%, P = 1.0). There were not enough patients with neck, neck only, and Monteggia variants to perform these analyses.
Association of Outcomes Between Treatment Group and by Fracture Type.
Note. ORIF = open reduction and internal fixation; QuickDASH = shortened iteration of the Disabilities of the Arm, Shoulder, and Hand; SD = standard deviation.
Student t test for continuous variables; Fischer’s exact test for categorical variables.
Among patients younger than 55 years of age, no statistically significant differences were observed in study outcomes between treatment groups (Supplemental Table 1). Among patients 55 years and older (Supplemental Table 2), QuickDASH scores were 13.7 points lower (95% CI: -25.9 to -1.4, P = .03) and arc of motion 14.7° higher (95% CI: 0.4 to 29.0, P = .04) in the ORIF group compared with the arthroplasty group. However, these differences were not statistically significant when adjusted for Mason type and associated soft tissue injury.
In subgroup analyses of patients stratified by BMI ≥30 km/m2 (Supplemental Table 3), patients who underwent RHA had significantly higher supination range of motion than ORIF patients (ORIF: 59.9, SD = 21.7; RHA: 64.2, SD = 13.8; mean difference, -19.8; 95% CI: -38.9 to -0.7; P = .04). This subgroup had no other statistically different outcomes between treatments. Among patients with BMI <30 km/m2, no statistically significant differences between treatments were observed.
Discussion
We compared ORIF and RHA and found no difference in QuickDASH scores at an average of 7.5 years from surgery, even among patients with comminuted, multi-fragmentary radial head fractures. Among our secondary outcomes, patient-reported need for pain medication did not differ between groups, nor did range of motion or unplanned reoperation.
Although not statistically significant, we found that RHA patients reported a slightly higher average level of functional disability when compared to ORIF. However, findings from nonrandomized retrospective studies comparing ORIF and RHA should be interpreted with caution because of treatment bias. In our study in particular, the RHA population was older, had a higher BMI, and had more concurrent soft tissue injury.
Among our multi-fragmentary subgroup, QuickDASH scores were also similar between treatments. This was also true among patients with complex fracture patterns. This was not a randomized study, and therefore, these findings should be viewed as indicative of the treatment strategy employed at our trauma center to reconstruct the radial head when possible, despite the increased technical difficulty and time of the procedure; ORIF confers the theoretical benefit of restoring native anatomy, which is especially important for the younger patient who might outlive their implant. 9 As we were underpowered to detect the minimal clinical important difference (MCID) of the QuickDASH in this subgroup, these results should be considered exploratory only.
Our results agree with several recent studies, which are short- to mid-term in duration. In a multicenter retrospective European study of 40 patients with Mason types 2 and 3 fractures treated with ORIF or RHA, no significant differences were found in patient-reported outcome scores including the QuickDASH. 10 The average age of participants was 47 years, similar to that of our cohort, but had a shorter average follow-up duration of 48 months. Ryu et al conducted a similar retrospective patient-reported outcomes study in Korea among 42 patients with modified Mason types 3 and 4 fractures, finding no significant difference in Patient-Rated Elbow Evaluation or DASH scores between ORIF and RHA patients. 11
On the other hand, a randomized controlled trial published in 2011 found opposing results. This trial randomly allocated 45 Mason type 3 fracture patients to either ORIF or RHA, finding that RHA patients had significantly better Broberg and Morrey scores at a mean of 2.8 years follow-up. 12 However, Broberg and Morrey scores include a combination of physician-reported and patient-reported measures, compared with the QuickDASH, which is scored entirely on patient report. In a similar vein, the largest available retrospective review included 7520 patients in these treatment groups and found higher reoperation rates and greater costs associated with ORIF as compared to RHA in short-term follow-up, although patient-reported functional outcomes were not collected in this study. 13
Strengths of this study include its sample size and duration of follow-up. Our cohort of 76 patients is larger than previous studies comparing patient-reported outcomes between these 2 treatment groups. The average time from surgery to completion of the QuickDASH was 7.5 years in our study, which is several years longer than most similar studies and allows ample time to observe long-term loss of function.10 -13 Our single-center design also provided a consistently applied surgical approach to these injuries.
A main limitation of our study is the specialized upper extremity surgical experience of our team. This study therefore might not yield generalizability of our surgical algorithm to other centers. We are also limited by suboptimal response rates, introducing potential bias to our study. However, respondents included similar proportions of ORIF and RHA in the patient pool as a whole, and demographics were similar between treatment groups. Since we were only powered to detect the MCID for the QuickDASH in the full pool of participants, our subgroup analyses were underpowered and findings should be interpreted as exploratory only. This study also did not explicitly account for the specific features of associated soft tissue injuries, which is known to affect functional outcomes, 14 though it is likely that this was factored into patient selection.
Conclusion
This study represents one of the largest cross-sectional cohort studies with long-term follow-up comparing patient-reported functional outcomes between ORIF and RHA for radial head fracture. We find that QuickDASH scores, unplanned reoperation rates, range of motion, and pain are similar overall between groups, including subgroup analysis of fractures with >3 parts and in patients >55 years old. These findings are in contrast to much of the doctrine on radial head fractures, and demonstrate that reconstructing the radial head may not result in worse outcomes than RHA when both options are employed according to the best judgment of the operating surgeon. For selected patients, even those with multi-fragmentary radial heads, ORIF is a reasonable option based on our data.
Supplemental Material
sj-docx-1-han-10.1177_15589447221109631 – Supplemental material for Association of Radial Head Fracture Treatment With Long-Term Function
Supplemental material, sj-docx-1-han-10.1177_15589447221109631 for Association of Radial Head Fracture Treatment With Long-Term Function by Cynthia E. Burke, Phillip C. McKegg, Alison L. Wong, Genaro A. DeLeon, Jayesh Gupta, Kathleen Healey, Blessing Enobun, Nathan N. O’Hara, Robert V. O’Toole, Raymond A. Pensy, Christopher G. Langhammer and W. Andrew Eglseder in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447221109631 – Supplemental material for Association of Radial Head Fracture Treatment With Long-Term Function
Supplemental material, sj-docx-2-han-10.1177_15589447221109631 for Association of Radial Head Fracture Treatment With Long-Term Function by Cynthia E. Burke, Phillip C. McKegg, Alison L. Wong, Genaro A. DeLeon, Jayesh Gupta, Kathleen Healey, Blessing Enobun, Nathan N. O’Hara, Robert V. O’Toole, Raymond A. Pensy, Christopher G. Langhammer and W. Andrew Eglseder in HAND
Supplemental Material
sj-docx-3-han-10.1177_15589447221109631 – Supplemental material for Association of Radial Head Fracture Treatment With Long-Term Function
Supplemental material, sj-docx-3-han-10.1177_15589447221109631 for Association of Radial Head Fracture Treatment With Long-Term Function by Cynthia E. Burke, Phillip C. McKegg, Alison L. Wong, Genaro A. DeLeon, Jayesh Gupta, Kathleen Healey, Blessing Enobun, Nathan N. O’Hara, Robert V. O’Toole, Raymond A. Pensy, Christopher G. Langhammer and W. Andrew Eglseder in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not required for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NNO reported receiving stock or stock options from Arbutus Medical, Inc. unrelated to this research. RVO reported receiving royalties from Lincotek, serving as a paid consultant for Smith & Nephew and Stryker, receiving honorarium from Zimmer, and receiving stock options from Imagen, all unrelated to this research. CGL reported serving as a paid consultant for DePuy Synthes unrelated to this research. WAE reported receiving royalties from and serving as a paid consultant for Globus Medical unrelated to this research. Dr. O’Toole reported receiving royalties from Lincotek, serving as a paid consultant for Smith & Nephew and Stryker, receiving honorarium from Zimmer, and receiving stock options from Imagen, all unrelated to this research.The remaining authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.