
Abstract
Purpose:
The objective of this study was to investigate whether the outcomes of Mason type III radial head fractures (RHFs) treated by open reduction and internal fixation (ORIF) were comparable to those of Mason type II RHFs treated by ORIF.
Methods:
A total of 87 surgically treated RHF patients were reviewed. Their fractures were Mason type II in 39 patients (all treated by ORIF) and Mason type III in 48 patients (40 treated by ORIF, 7 by radial head arthroplasty, and 1 by resection). Although ORIF was preferred for Mason type III RHFs in our series, an arthroplasty was performed when the fracture accompanied severe associated injuries or multiple traumas. Radiological and functional outcomes were evaluated and complications were reviewed.
Results:
When Mason type II and Mason type III in general were compared, QuickDASH score, a shortened version of the Disabilities of the Arm, Shoulder and Hand (DASH) score, and forearm rotation were significantly worse in Mason type III. However, when comparing Mason type II and Mason type III treated by ORIF in which the proportion of associated injuries were not significantly different, there was no significant difference in QuickDASH score, range of extension/flexion, or complication rate. Forearm rotations were significantly more limited in Mason type III treated by ORIF (7° for pronation and 7° for supination), and Mason type had an independent effect on forearm rotations in multivariate analysis.
Conclusion:
ORIF for Mason type III fractures with low level of associated injury can be as good as that for Mason type II fractures, except for less forearm rotation.
Keywords
Introduction
Radial head fractures (RHFs) are common fractures, accounting for up to 4% of all fractures in adults. 1 Their incidence has been reported to be 2.8 per 10,000 inhabitants per year. 2 Mason classification is often used for RHFs: type I, a nondisplaced fracture (fissure fractures or marginal sector fractures without displacement); type II, a displaced fracture (marginal sector fractures with displacement), and type III, a comminuted fracture (comminuted fractures involving the whole head of the radius). 3 Later, Johnston added RHF with dislocation of the elbow as the fourth type. 4 However, elbow dislocation can be regarded as one of the associated injuries of RHFs. 5 While Mason type I fractures are generally treated conservatively, treatments for Mason type II fractures are inconclusive between nonoperative management and surgical treatment, although there is no disagreement about choosing open reduction and internal fixation (ORIF) as the surgical method. 6
On the other hand, there is no dispute that Mason type III fractures need surgery, 7 although the choice of surgical method for Mason type III is still a matter of debate. 8 Although it has been reported that radial head resection can produce acceptable outcomes in some limited cases, restoring radiocapitellar contact is preferred whenever possible either by ORIF or by radial head arthroplasty (RHA). 9 –12 Between ORIF and RHA, three recent meta-analyses have favored RHA over ORIF. 13 –15 However, a prosthesis may have its inherent drawbacks such as overstuffing, osteolysis, loosening, or implant dislocation. 16 –18 If we can get acceptable functional outcomes with low complication rate, ORIF is preferable to preserve normal articulation and bone stock. If ORIF fails prematurely, theoretically it can be converted into RHA.
In this context, we have been preferentially performing ORIF for Mason type III RHFs. The objective of this study was to investigate whether ORIF for Mason type III RHFs produced outcomes comparable to that for Mason type II RHFs and to identify the factors which affected the outcomes.
Patients and methods
A total of 87 patients who were treated surgically for an RHF in a single institute were reviewed after obtaining approval from the institutional review board. Pediatric cases with growth plate unfused or old RHFs and cases without sufficient data were excluded. The mean age at surgery was 45 years (range 15–77 years). There were 40 males and 47 females. Their fractures were Mason type II in 39 patients (44.8%) and Mason type III in 48 patients (55.2%). The injury was an isolated RHF in 56 patients (64.4%) and an RHF with associated injuries including elbow dislocation, fracture(s) other than RHF, or surgically treated ligament injury in 31 patients (35.6%). The surgery for Mason type II RHFs was ORIF in all cases. The surgery for Mason type III was ORIF in 40 patients (83.3%), RHA in 7 patients (14.6%), and resection in 1 patient (2.1%). Although, in general, ORIF was preferred for Mason type III RHFs, RHA was performed when the fracture accompanied severe associated injuries or multiple traumas.
Surgical procedure
For ORIF of the radial head, a Kocher approach between the extensor carpi ulnaris and the anconeus muscles, an extensor digitorum communis-splitting approach, or a Kaplan approach between the extensor digitorum communis and the extensor carpi radialis brevis muscles were used. 19,20 The annular ligament and the joint capsule were transected in line with the plane between muscles split. After removing hematoma, all fractured fragments were identified with a special concern for articular fragments. All articular fragments were put together anatomically and fixed temporarily with K-wires. These K-wires sometimes were used as drill for mini-screws or guide pins later. After identifying the safe zone for proximal radioulnar articulation, 21 fragments were fixed with mini-screws, mini-plates (DePuy Synthes GmbH, Solothurn, Switzerland and Jeil Medical Corporation, Seoul, Korea), Mini-Acutraks (Acumed, Hillsboro, Oregon, USA), or K-wires. Plates were placed in the safe zone, while the head of a fixation device was buried below the articular surface when the entry of a fixation device was beyond the safe zone. 22 The annular ligament was securely repaired with nonabsorbable sutures or polydioxanone sutures.
For radial head replacement arthroplasties, a bipolar prosthesis (RHS™, Tornier Inc., Montbonnot-Saint-Martin, France) was used. A posterolateral approach was performed with the annular ligament transected. The radial neck was osteotomized 5 mm proximally to the biceps tuberosity. The proximal medullary canal of the radius was prepared with a burr or a rasp. After ensuring a good fit in the medullary canal and the joint space with trial prostheses, the stem and the prosthetic head were inserted. The annular ligament was securely repaired with nonabsorbable sutures or polydioxanone sutures.
Postoperatively, a long arm splint was applied with 90° of elbow flexion for 2 weeks. A hinged brace was then applied for 4 weeks. Increasing the range of motion (ROM) was allowed.
Outcome evaluation
The mean follow-up period was 29 months (range 6–98 months) for all patients. Radiological and functional outcomes at final visit were evaluated, and complications were reviewed. Radiological evaluations were performed by two board-certified orthopedic surgeons with a subspecialty certificate in hand surgery, for secondary displacement, osseous union/nonunion, avascular necrosis of the radial head, and post-traumatic arthrosis after ORIF. Joint space narrowing, osteolysis, loosening, and implant dislocation were evaluated after RHA. Post-traumatic arthrosis was graded according to Broberg and Morrey system, 23 as grade 0 (absent; normal elbow), grade 1 (mild changes), grade 2 (moderate changes), and grade 3 (severe degenerative changes).
Functional outcomes were evaluated by board-certified orthopedic surgeons as ROM and QuickDASH, a shortened version of the Disabilities of the Arm, Shoulder and Hand (DASH) score. ROM was measured with a goniometer as range of extension, flexion, pronation, and supination. Flexion–extension examinations were performed with neutral forearm rotation. Pronation–supination examinations were measured with the elbow flexed to 90°. In QuickDASH, the score ranged from 0 to 100, with higher score indicating greater level of disability and severity.
Complications other than radiological changes or functional deficit were also reviewed for hardware-related complications, heterotopic ossification, and infection.
Statistical analysis
All statistical analyses were performed using SPSS 24.0 (IBM Corp. Armonk, New York, USA). Differences between groups were compared by Mann–Whitney U test and χ 2 test. To compare the effect of factors on outcome, multiple linear regression analysis was used. In all cases, a p value of ≤0.05 was used to indicate statistical significance.
Results
Mason type II versus type III in general
Outcomes of Mason type II and III RHFs are summarized in Table 1. Age at surgery, gender, or follow-up period was not significantly different between Mason type II and III. The proportion of associated injury was significantly higher in Mason type III than that in Mason type II. Regarding ROM, extension/flexion was not significantly different between Mason type II and III. However, pronation/supination was significantly worse in Mason type III (p = 0.007 for pronation and p = 0.001 for supination). QuickDASH score also was significantly worse (higher) in Mason type III than that in Mason type II (p = 0.016).
Outcomes of Mason type II and type III radial head fractures.

DASH: Disabilities of the Arm, Shoulder, and Hand.
Influence of Mason type and surgery type
To evaluate the influence of Mason type and surgery type to outcomes, patients were divided into three groups: Mason type II RHFs (II-ORIF), Mason type III RHFs treated by ORIF (III-ORIF), and Mason type III RHFs treated by RHA (III-RHA).
When comparing group II-ORIF and group III-ORIF (Table 2), there was no significant difference in age, gender, the proportion of associated injury, or follow-up period. Regarding outcomes, no significant difference was observed in extension, flexion, or QuickDASH score (p = 0.408, p = 0.740, and p = 0.082, respectively), although pronation/supination was significantly worse in III-ORIF (p = 0.030 and p = 0.003, respectively).
Outcome comparison between Mason type II radial head fractures and type III fractures treated by open reduction and internal fixation.

ORIF: open reduction and internal fixation; DASH: Disabilities of the Arm, Shoulder, and Hand.
When comparing group II-ORIF and group III-RHA (Table 3), the proportion of associated injury was significantly higher in III-RHA (p = 0.001), suggesting that the injury was more severe in III-RHA. Follow-up period was significantly longer in III-RHA (p = 0.039). Regarding outcomes, QuickDASH score was significantly worse (higher) in III-RHA compared to that in II-ORIF (p = 0.006). ROMs in flexion, pronation, and supination were also significantly worse in III-RHA compared to those in II-ORIF (p = 0.009, p = 0.006, and p = 0.006, respectively).
Outcome comparison between Mason type II radial head fractures and type III fractures treated by radial head arthroplasty.

RHA: radial head arthroplasty; DASH: Disabilities of the Arm, Shoulder, and Hand.
Influence of associated injuries
To evaluate the influence of associate injuries, cases were divided into isolated RHF group and RHF with associated injury group including elbow dislocation, fracture(s) other than RHF, or surgically treated ligament injury. When comparing isolated RHF and RHF with associated injury (Table 4), there was no significant difference in age, gender, or follow-up period. Regarding outcomes, QuickDASH score was significantly worse (higher) in RHF with associated injury compared to that in isolated RHF (p = 0.048) and ROM in pronation was also worse in RHF with associated injury (p = 0.008). ROMs in extension, flexion, or supination was not significantly different between two groups.
Outcome comparison according to the presence of associated injuries.
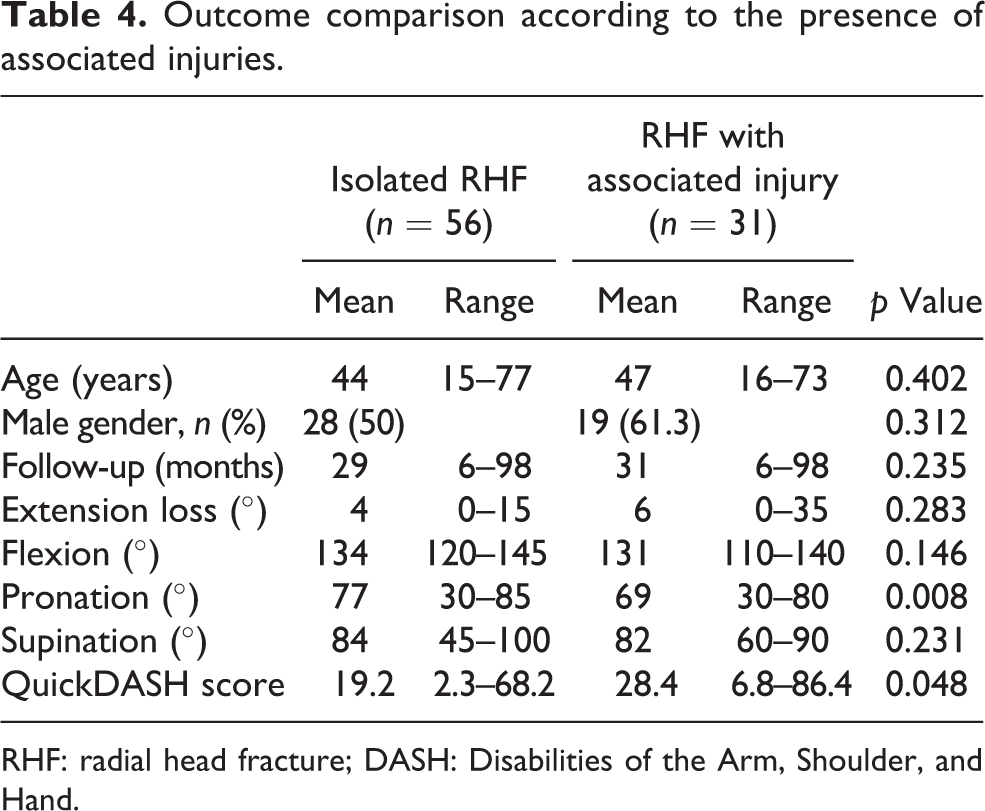
RHF: radial head fracture; DASH: Disabilities of the Arm, Shoulder, and Hand.
Multivariate analysis
To compare the effect of factors on outcome, multiple linear regression analyses were performed for 86 cases except for the radial head resection case, using age, gender (male > female), Mason type (III > II), associated injury (present > none), and surgery type (RHA > ORIF) as independent variables (Table 5). For QuickDASH score, surgery type was the only significant factor (standardized coefficient = 0.265, p = 0.029), suggesting that RHA produced worse (higher) QuickDASH score. For ROM in extension loss, age was the only significant factor (standardized coefficient = 0.395, p = 0.006), suggesting that older patients had more extension loss. For flexion, surgery type was the only significant factor (standardized coefficient = −0.335, p = 0.006), suggesting that RHA resulted in more flexion loss. For pronation/supination, Mason type was the only significant factor (standardized coefficient = −0.222, p = 0.050 and standardized coefficient = −0.312, p = 0.006, respectively), suggesting that Mason type III left more deficit in pronation/supination. Gender and associated injury had no significant effect on outcomes in multiple linear regression analysis.
Factors analyzed for outcomes of radial head fractures by multiple linear regression analysis (n = 86).
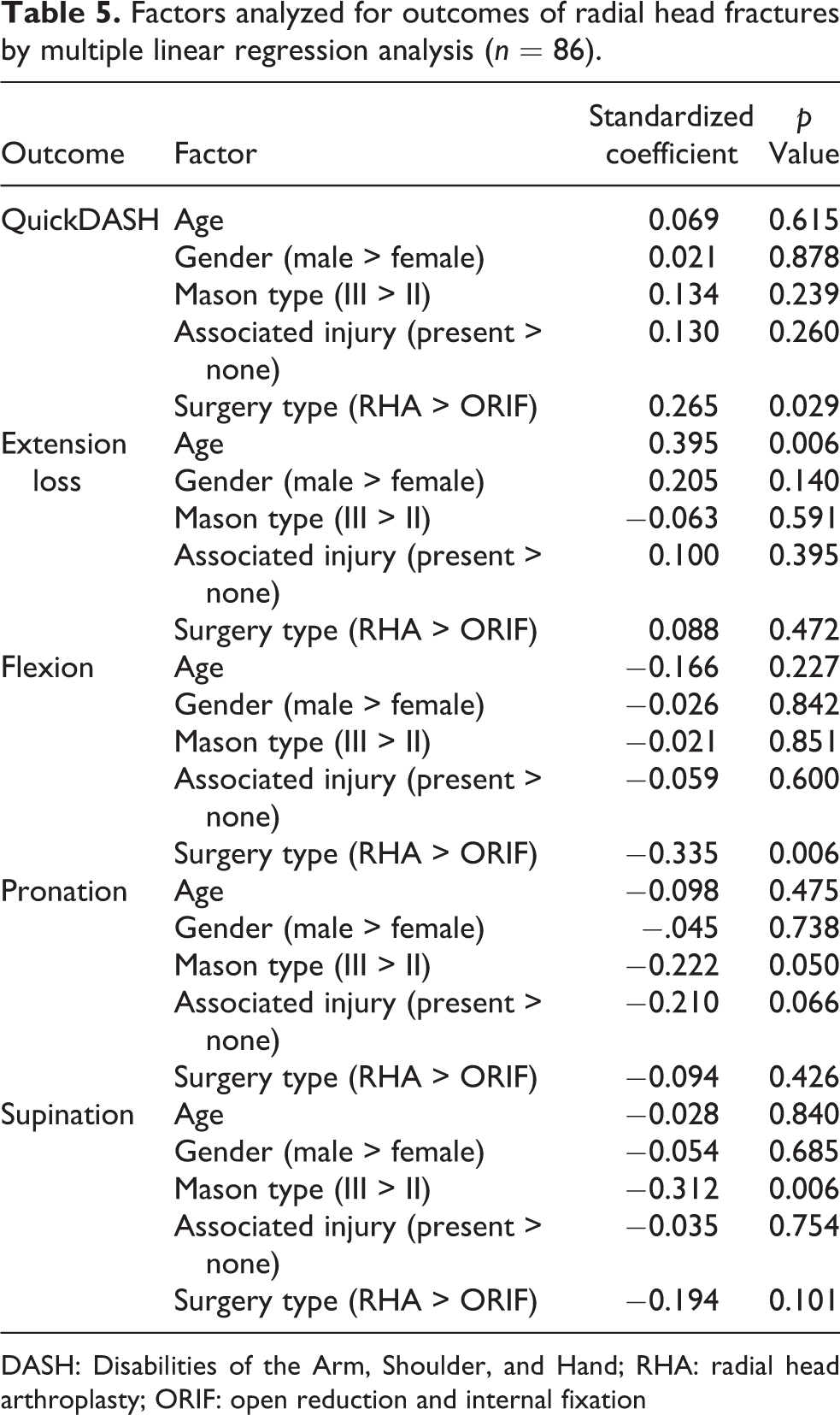
DASH: Disabilities of the Arm, Shoulder, and Hand; RHA: radial head arthroplasty; ORIF: open reduction and internal fixation
Complications
When complications were compared between group II-ORIF and group III-ORIF (Table 6), no significant difference in complication rate was found in terms of secondary displacement, nonunion, avascular necrosis, hardware breakage, hardware irritation required a removal surgery, heterotopic ossification, or radiological arthrosis.
Complications of Mason type II radial head fractures and type III fractures treated by open reduction and internal fixation.
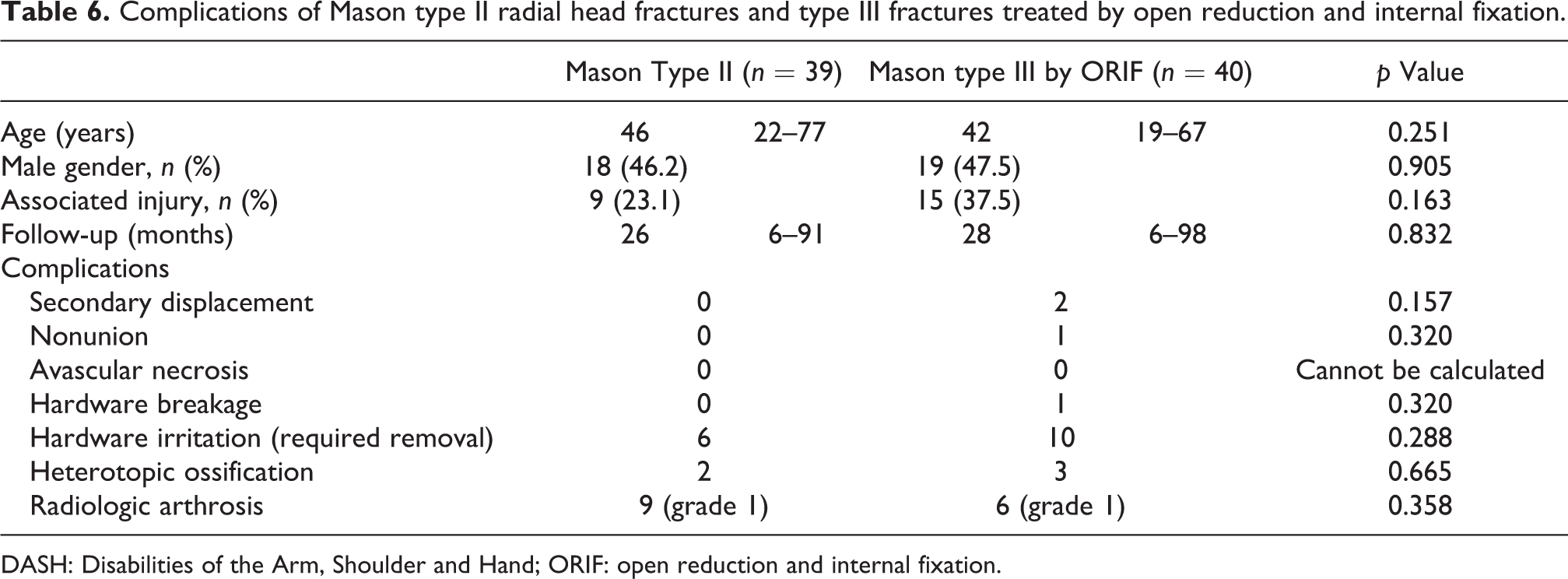
DASH: Disabilities of the Arm, Shoulder and Hand; ORIF: open reduction and internal fixation.
In RHFs treated by RHA (n = 7), there were three cases of joint space narrowing, two cases of heterotopic ossification, one case of osteolysis, one case of loosening, and one case of implant dislocation. There was no postoperative infection.
Illustrative case
A 67-year-old woman fell backward on an escalator and sustained a comminuted elbow fracture (Figure 1(a)). Her RHF was classified as Mason type III and her radial head was broken into at least five pieces (Figure 1(b), articular fragments were put together for the photo although the fracture involved the entire radial head and the fragments were scattered before the photo). Her fractures were treated by ORIF using plates and screws (Figure 1(c)), some of which were removed later because of skin irritation. At postoperative 34 months, no radiological arthrosis was evident around the radial head (Figure 1(c)). She did not want removal of radial hardware because it did not cause any irritation. Her final QuickDASH score was 4.5.

(a) A Mason type III radial head fracture with associated proximal ulnar comminuted fracture in a 67-year-old woman. (b) The radial head was broken into at least five pieces (scattered articular fragments were put together in the photo). (c) These fractures were treated by open reduction and internal fixation using plates and screws. (d) At postoperative 34 months, no radiological arthrosis was evident around the radial head. She did not want the removal of radial hardware which did not cause any irritation.
Discussion
The principal result of our study is that the outcomes of Mason type III RHFs treated by ORIF were comparable to those of Mason type II RHFs. Although the mode of surgery for Mason type III RHFs has been controversial, recent trends have led to RHA. There have been three recent meta-analyses favoring RHA over ORIF for Mason type III RHFs. 13 –15 All of them reported that RHA was superior in terms of satisfactory rate and complication rate. However, evidence was of low quality in general, as mentioned in one of these meta-analyses. 15 In addition, in a recent retrospective study that included isolated RHFs only, ROM and functional score were not significantly different between ORIF and RHA for Mason type III and IV RHFs. 24 Therefore, it may still be a hasty conclusion to say that RHA is better than ORIF for Mason type III RHFs, and it might be necessary to choose a surgical option taking into account factors other than Mason type such as the degree of associated injuries, bone quality, age, and functional requirements.
In our series in which ORIF was preferred for Mason type III RHFs, outcomes of group III-ORIF were similar to those for group II-ORIF. ROM except for pronation/supination, QuickDASH score, or complications showed no significant difference between those two groups. Although forearm rotations were significantly worse in group III-ORIF, the mean difference was relatively small: 7° for pronation and 7° for supination. These results can be attributed to the fact that there was no significant difference in the proportion of associated injury in both groups. We chose RHA when the fracture accompanied severe associated injuries or multiple traumas. Although this indicates that our study has bias in the treatment method, our results at least may suggest that it may not be necessary to give up ORIF merely because the fracture is Mason type III, if associated injuries are not severe.
One of the probable reasons for similar outcomes of group III-ORIF and group II-ORIF in our study could be meticulous repair of the annular ligament. The main mode of failure in ORIF for Mason type III RHFs has been reported to be fixation loss and painful nonunion that may lead to insufficient stability of ORIF, especially when the fracture consists of more than three fragments. 25 Although Hotchkiss et al. has described that the annular ligament does not usually require repair as a separate structure, 22 we have repaired it as a separate structure whenever possible to provide additional stability and facilitate rotational gliding of the radial head (Figure 2). One study has reported that Mason type III RHFs do not even require fixation to the shaft when performing ORIF. 26 They described that factors that could influence rotatory stability were an intact periosteal sleeve across the fracture, ragged fracture lines that could facilitate interlocking of the fracture fragments, and stable soft-tissue repair. We believe that annular ligament repair is especially helpful for stability in cases as those shown in our illustrative case, in which some fracture fragments are fixed by only one screw.

Annular ligament repair during an open reduction and internal fixation for a Mason type III radial head fracture. Three horizontal mattress-type sutures were placed before approximating the ligament. They were then tied one by one to secure the repair. Additional sutures were applied to enhance the repair.
Associated fractures or soft tissue injuries in RHFs have been reported to be as frequent as 39%. 5 In general, the more severe the associated injury, the worse the outcomes are expected to be. Indeed in our comparison according to the presence of associated injuries, RHF with associated injury group showed significantly worse QuickDASH score and pronation than isolated RHF group. However, in multiple regression analysis, associated injury itself had no independent effect on outcomes, and surgery type was the only significant factor for QuickDASH score. This may be because Mason type and associated injury were already reflected in the selection of surgery type.
Regarding the results of multiple regression analysis on ROM, each motion had significant factor for it. For extension, age was the significant factor. Older patients had more extension loss. For flexion, surgery type was the significant factor. Although this also may have been influenced by the preference of surgical method, it may be due to overstuffing of the radial head prosthesis, a well-known complication of RHA. 27 For pronation/supination, Mason type was the significant factor. As Mason type III showed significantly worse forearm rotations within cases treated by ORIF, it appears that Mason type certainly affects pronation/supination. This is probably due to the need for larger hardware for fixation in Mason type III RHFs as compared to Mason type II RHFs.
Regarding complications, there was no significant difference in complications between group II-ORIF and group III-ORIF. Although there are reports comparing complications ORIF and RHA within Mason type III, complication types can be completely different in ORIF and RHA. For example, secondary displacement which can happen only in ORIF may not progress after bone union and nonunions of small fragments can be asymptomatic, 20 causing no substantial functional deficit. Whether a hardware removal surgery after ORIF should be regarded as a complication is also controversial. On the other hand, complications such as osteolysis, loosening, and implant dislocation are relatively specific for RHA. Therefore, it is more objective to compare Mason type II RHFs and Mason type III RHFs treated by ORIF than to compare the number of complications. Our result regarding complications additionally supports that ORIF in Mason type III RHFs with low level of associated injury can be as good as that in Mason type II RHFs.
Our study has limitations. First, this is a retrospective study with small number of cases. However, most studies for Mason type III RHFs have reported less than 40 cases for each type of surgical method. 13 –15 Although there are a few prospective studies on Mason type III RHFs favoring RHA over ORIF, 28,29 none of them have reported long-term outcomes, and one of them mentioned that the radial head should be preserved for relatively stable RHFs with less associated injuries. Second, our study showed results of preferentially performed surgeries. Because RHA was performed in cases with more severe injury levels, our study has bias in the treatment method. However, our result that the outcomes were similar between group II-ORIF and group III-ORIF can support that ORIF for Mason type III RHFs with low level of associated injury may produce good outcomes as that for Mason type II RHFs. Third, only one type of prosthesis was used for RHA. However, it has been reported that monopolar and bipolar fixed-neck prosthetic radial head implants have similar biomechanical effects in a terrible triad. 30 Fourth, follow-up period was variable. Although we used data from the final visit to see possible long-term results, some patients had lost follow-up early.
In conclusion, ORIF can be a good option for Mason type III RHFs with low level of associated injury, which may produce comparable outcomes to that for Mason type II RHFs. It may not be necessary to give up ORIF merely because the fracture is Mason type III. Although Mason type III results in less forearm rotations after ORIF, substantial amount of the deficit is small. Future studies with a greater number of cases and a longer follow-up period are needed to further strengthen our conclusion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.