
Abstract
Background:
Lipomas are a rare cause of posterior interosseous nerve (PIN) compression. A systematic review of predictors for motor recovery has not been performed. This study sought to evaluate whether patient or lipoma characteristics are associated with motor recovery and could be used to determine when immediate tendon transfers at the time of excision should be performed.
Methods:
Articles describing patients with forearm lipomas resulting in PIN compression with motor weakness were included. Patient age, gender, symptom duration, laterality and largest dimension of lipoma, surgical intervention, and motor recovery were identified. Article quality was assessed via the Methodological Index for Non-Randomized Studies criteria.
Results:
Thirty articles reporting on 34 patients were identified. Average age was 58.2 years. Average largest lipoma dimension was 5.7 cm. All patients underwent lipoma removal, and 2 had concomitant tendon transfers. In all, 73.5% of patients had complete motor recovery at an average of 9.7 months. Patient age and largest dimension of lipoma, and duration of symptoms were not significant predictors of motor recovery. Symptom duration was a significant predictor of motor recovery in binary regression, particularly if < 18 months.
Conclusions:
The majority of patients with PIN weakness secondary to lipoma are likely to have complete motor recovery after excision alone. Concomitant tendon transfers should be considered for patients symptomatic for greater than 18 months. Further, adequately powered, studies are required to stratify risk factors and evaluate other modalities to identify the minority of patients who would benefit from immediate tendon transfer.
Introduction
The radial nerve branches into the superficial radial nerve and posterior interosseous nerve (PIN) in the proximal forearm. The PIN then passes beneath the superficial and deep heads of the supinator to innervate the extrinsic thumb abductors and extensors, extrinsic finger extensors, and extensor carpi ulnaris. Posterior interosseous nerve palsy is uncommon but associated with significant functional impairment if left untreated. Compression of the PIN has been reported at several anatomic locations including fibrous bands between brachialis and brachioradialis, the recurrent radial vessels (vascular leash of Henry), the proximal-medial edge of extensor carpi radialis brevis, proximal supinator (arcade of Frosche), or distal supinator. Etiologies of compression are similarly numerus, including but not limited to trauma, inflammation, and iatrogenic injury. Rarely, compression can also be caused by masses such as ganglions or lipomas in the proximal forearm.1,2
Posterior interosseous nerve compression secondary to lipoma was first reported by Richmond in 1953. 3 Since then, the body of evidence has continued to be limited to case reports and case series. While lipomas themselves are not compressive, their presence adjacent to the PIN often exacerbates common points of compression. As such, concomitant PIN decompression with lipoma removal is frequently reported in the available case reports. Incidence and timing of motor recovery after lipoma removal and the benefit of concomitant tendon transfers to restore thumb and finger extension have not been evaluated. The purpose of the current study is to perform a literature review and meta-analysis of the existing literature to determine if any patient or lipoma factors are associated with complete or incomplete motor recovery.
Materials and Methods
This systematic review was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Supplementary Figure 1). A protocol for this meta-analysis was published on the International Prospective Register of Systematic Reviews (Registration number CRD42020162336). Computerized database searches of PubMed, MEDLINE, Elsevier, and the Cochrane databases were completed for the term “lipoma posterior interosseous nerve.” Inclusion criteria were as follows: (1) original reports available in English of patients with lipomas causing PIN compression; (2) patients age 18 years; or older (3) reported intervention and outcomes. After duplicates were removed, 2 reviewers independently reviewed titles of retrieved articles based on the inclusion criteria. Abstracts and full-text documents of potentially relevant reports were retrieved and independently assessed for inclusion. The Methodological Index for Non-Randomized Studies (MINORS) criteria were utilized to assess quality of included articles. 4
Motor recovery, time to motor recovery in months, and surgical complications were extracted from included reports. Additional data collected included patient age, gender, hand dominance, largest lipoma dimension, laterality of the lipoma, symptom duration, and surgical procedure. Logistic regression models were created to characterize determinants of motor recovery. Coefficients with P-values less than or equal to .05 were considered to be statistically significant.
Results
Initial query yielded 160 citations. After duplicates were consolidated and articles screened for relevancy, 30 articles comprising 34 patients met inclusion criteria and were included in the analysis (Supplementary Table 1).3,5-35 Studies comprised of case series and reports dating from 1953 to 2019. Each study included 1 to 4 patients, 31 of which described 1 patient. Average MINORS score was 6.1/16. Average patient age was 58.2 years (range: 39-83). 44.1% (15/34) of patients were male. In all, 47.1% (16/34) of lipomas were in the right forearm. Hand dominance was reported for 5 patients of which 3 had lipomas affecting their dominant forearm. The average duration of symptoms was 8.6 months (range: 1-60). The average largest dimension of the lipoma was 5.7 cm (range: 3-20). All patients underwent lipoma removal and 2 had immediate tendon transfers. Twenty-five (73.5%) were noted to have complete motor recovery at an average of 9.7 (range: 1.5-60) months. No surgical complications or lipoma recurrences were reported. The average follow-up was 15.8 (range: 4-72) months.
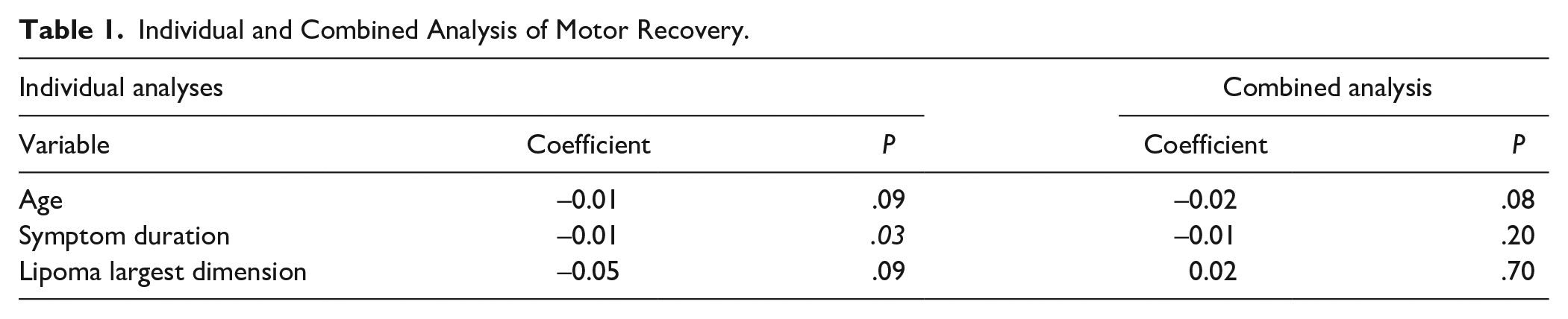
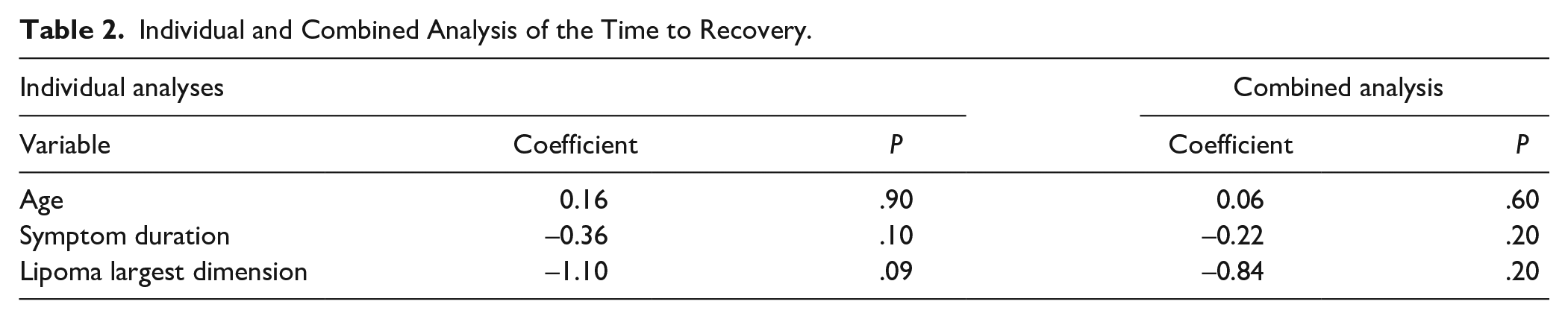
The effects of patient age, duration of symptoms, and largest lipoma dimension on motor recovery and time to recovery were evaluated in univariate and multivariate regression models. Complete data for motor recovery and patient age was available for 34 patients; motor recovery and duration of symptoms for 28 patients; and motor recovery and largest lipoma dimension for 24 patients. In individual binary logistic regression models predicting motor recovery, duration of symptoms was the only significant predictor (coefficient = -0.01, P = 0.03). The same effect was not reproduced however when independent variables were combined (Table 1). None of the primary predictor variables determined time to recovery in individual or combined regression models (Table 2).
Individual and Combined Analysis of Motor Recovery.
Individual and Combined Analysis of the Time to Recovery.
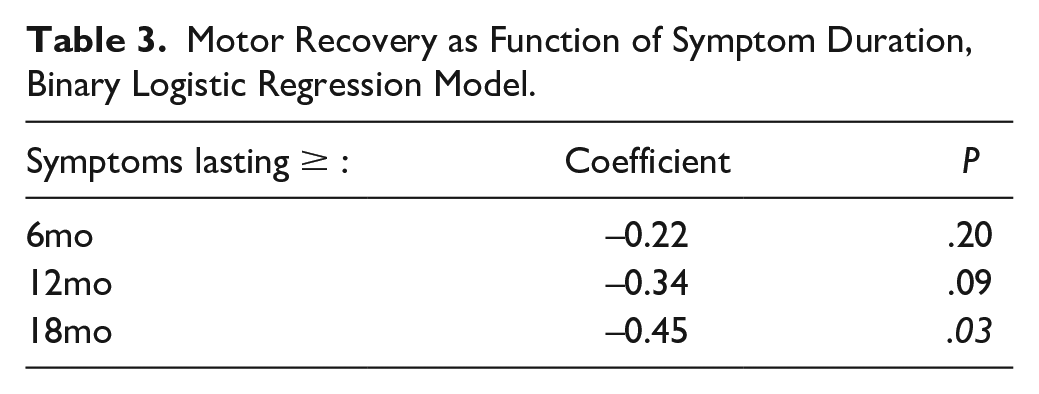
Symptom duration at which motor recovery becomes significantly less likely was also examined. Binary logistic regression models for patients with complete data for symptom duration and motor recovery revealed no statistically significant difference at 6 months (coefficient -0.22; P = .20) and 12 months (coefficient -0.34, P = .09). The chance of recovery was statistically significantly higher for patients with fewer than 18 months of symptoms (coefficient -0.45, P = .03) (Table 3).
Motor Recovery as Function of Symptom Duration, Binary Logistic Regression Model.
Discussion
Injury of the PIN in the proximal forearm results in significant functional deficits due to limitations in finger extension, thumb extension and abduction, and wrist extension. Lipomatous compression is an infrequently reported etiology, limited solely to case reports and small case series. No large studies presently exist in the literature evaluating their incidence and time to spontaneous motor recovery. This meta-analysis sought to determine whether patient or lipoma characteristics could potentially be used to predict motor recovery and secondarily identify patients who may benefit from primary tendon transfer.
In this study, multivariate regression models including patient age, duration of symptoms, and largest lipoma dimension did not significantly correlate with or predict motor recovery or time to motor recovery. Seventy-four percent of patients had full motor recovery at an average of 9.7 months, suggesting that observation and serial examination may be sufficient for most patients. Univariate analysis did reveal symptom duration, specifically greater than 18 months, as a possible negative predictor of motor recovery. Based on the studies included in this analysis, spontaneous recovery was seen in 76% (19/25) of patients with less than 18 months of symptom duration compared to 33% (1/3) of patients with greater than 18 months of symptoms. Irreversible motor end-plate degeneration due to prolonged nerve compression is a possible explanation for this finding.36,37 Clinically, these patients may benefit from immediate tendon transfers at time of lipoma excision. Unfortunately, like other forms of compressive neuropathy, symptom onset is typically insidious thus confounding the accurate reporting of symptom duration.38,39
There are several limitations to the current study. Foremost, the rarity of this condition resulted in the use of low evidence (level IV) studies, resulting in an average MINORS criteria score of 6.1/16. Selection and publication biases are notable confounders for this type of analysis, comprised of mainly case reports. Though this analysis is the largest study to-date on this condition, the sample size limitations precluded power calculations and limit the conclusions drawn from the regressions. Due to this small sample size, our data may be underpowered to determine independent predictors of motor recovery. This may explain why symptom duration predicted poorer motor recovery in univariate but not multivariate regression. Outliers may have inordinate influence on findings. While age is known to impact recovery after nerve injury and transfers, this was not seen in our study and may also be a result of an underpowered study. 40 While this meta-analysis sought to identify relationships in an otherwise very uncommon disease, ultimately larger, more standardized, cohorts will be required to validate the trends identified with adequate statistical power. Finally, other potentially prognostic modalities such as preoperative electrodiagnostic studies were not available for review.
Conclusions
This meta-analysis suggests that recovery from PIN palsy caused by lipoma compression should be expected. Symptom duration greater than 18 months is a possible risk factor for motor recovery, however. Patients with such longer duration of symptoms may be considered for concomitant tendon transfer. Future multi-center studies could help elaborate on the risk factors for incomplete recovery and those who would benefit from immediate tendon transfers in this rare condition.
Supplemental Material
sj-doc-1-han-10.1177_15589447221096710 – Supplemental material for Forearm Lipoma Causing PIN Compression: Literature Review and Meta-Analysis of Predictors for Motor Recovery
Supplemental material, sj-doc-1-han-10.1177_15589447221096710 for Forearm Lipoma Causing PIN Compression: Literature Review and Meta-Analysis of Predictors for Motor Recovery by Christopher Cheng, Ayesha Punjabi, Sven Gunther and Kyle Chepla in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447221096710 – Supplemental material for Forearm Lipoma Causing PIN Compression: Literature Review and Meta-Analysis of Predictors for Motor Recovery
Supplemental material, sj-docx-2-han-10.1177_15589447221096710 for Forearm Lipoma Causing PIN Compression: Literature Review and Meta-Analysis of Predictors for Motor Recovery by Christopher Cheng, Ayesha Punjabi, Sven Gunther and Kyle Chepla in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Not applicable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KC is a consultant for Checkpoint Surgical. Cleveland, OH. CC, AP, SG declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.