
Abstract
Traumatic thumb injuries often result in significant functional disability. With segmental bone loss, reconstructive options include antibiotic cement with delayed bone graft, revision amputation with webspace deepening, metacarpal distraction osteogenesis, index pollicization, bone flap, and free toe transfer. We present a case of a subtotal thumb amputation just distal to the metacarpal phalangeal joint resulting in loss of both soft tissue and a segmental bone defect of the proximal and distal phalanx. Reconstruction was initially performed with a chimeric bone free flap from the medial femoral condyle with a vastus medialis muscle cuff to provide soft tissue coverage. A revision soft tissue coverage procedure was required and a radial forearm free flap was utilized. His reconstruction restored his missing bone and soft tissue, and provided stability with sufficient grip strength and metacarpophalangeal function resulting in a satisfactory functional outcome.
Keywords
Introduction
The thumb is the most critical digit in hand function and reconstructive goals include providing length, stability, mobility, sensibility, and appearance. 1 A multitude of surgical options exist for thumb reconstruction which are best addressed by dividing the first ray into proximal, middle, and distal thirds. Middle third injuries typically result in functional deficits, including loss of fine pinch and strong grasp. Reconstruction should aim to add bone length and/or to create relative ray length. Common reconstruction options include antibiotic cement with delayed bone graft, revision amputation with webspace deepening, metacarpal distraction osteogenesis, index pollicization, bone flap, and free toe transfer.
Doi and Sakai first demonstrated the use of a bone flap from the supracondylar region of the femur with vascular supply via the descending genicular artery (DGA). 2 The DGA is a branch of the superficial femoral artery and provides the greatest vascularity of the medial femoral condyle. 3 As a result, this bone flap has a robust perfusion and is versatile, reliable, and has minimal donor site morbidity. 4
In this case report, we describe a thumb reconstruction for a subtotal amputation just distal to the metacarpal phalangeal (MCP) joint with a medial femoral condyle free flap with successful bone transfer that resulted in satisfactory function and grip strength.
Case Report
A 49-year-old right-hand dominant male sustained a left thumb partial amputation with a router saw at work (Figure 1). The patient was an active smoker but otherwise healthy with no previous thumb injuries. He was not taking any medications and had no known drug allergies. The saw entered the thumb at the level of the proximal phalanx, just distal to the MCP joint.

Middle third left thumb router injury distal to metacarpal phalangeal joint. Far right: Plain radiograph of thumb at time of emergency department presentation.
This resulted in segmental bone loss of the proximal phalanx, with an additional open comminuted fracture of the distal phalanx, while preserving a skin bridge on the radial aspect of the thumb. Upon physical examination, the radial perfusion and sensation of the thumb remained intact with the skin bridge. There was segmental loss of thumb flexor pollicis longus tendon, extensor pollicis longus tendon, and ulnar neurovascular bundle. Plain film radiograph demonstrated significant proximal phalanx bony loss and comminuted open distal phalanx fracture. However, the proximal metacarpophalangeal joint remained intact.
After adequate debridement and irrigation, the wound was found to involve a 4.5 cm long bony segmental defect, ulnar digital nerve defect, tendon laceration, and significant missing volar-ulnar soft tissue. Unfortunately, the distal phalanx also had significant segmental bone loss, and intra-operative exploration revealed that it was so highly comminuted (including the radial half, which appeared potentially useful in pre-operative x-rays) that it precluded successful salvage and would not have contributed any meaningful structural integrity toward arthrodesis. With a non-salvageable interphalangeal joint, it was felt that the best option would be to reconstruct both the distal and proximal phalanx with a 5 cm x 1 cm x 1 cm medial femoral condyle osteocutaneous free flap (MFCFF). The ulnar digital nerve was reconstructed with an interpositional saphenous nerve branch graft from the thigh by coapting it to a small terminal nerve branch at the tip of the finger. This was performed to provide a distal target for the ulnar digital nerve, minimizing the risk of painful neuroma formation at the injury site. Moreover, although the ulnar aspect of the middle third of the thumb was devoid of skin, successful nerve regeneration could provide meaningful sensation to the ulnar tip of the thumb. For soft tissue coverage, a chimeric vastus medialis muscle flap was harvested via a perforator from the free medial femoral condyle pedicle (Figure 2). The MFCFF was carefully trimmed to size and fixated to the proximal phalanx base with crossing k-wires (Figure 3). Arteriovenous loops using volar forearm veins were created from the level of the anatomical snuff box and connected to the chimeric free flap to facilitate inset. Bright red bleeding from both free flaps was confirmed with the tourniquet down. The extensor pollicis longus was attached to the MFCFF using a bone anchor to improve postoperative motion. Finally, the vastus medialis muscle flap was covered with a split thickness skin graft (Figure 4).

Vastus medialis (left) and medial femoral condyle free flap (right) prior to dividing from donor site.
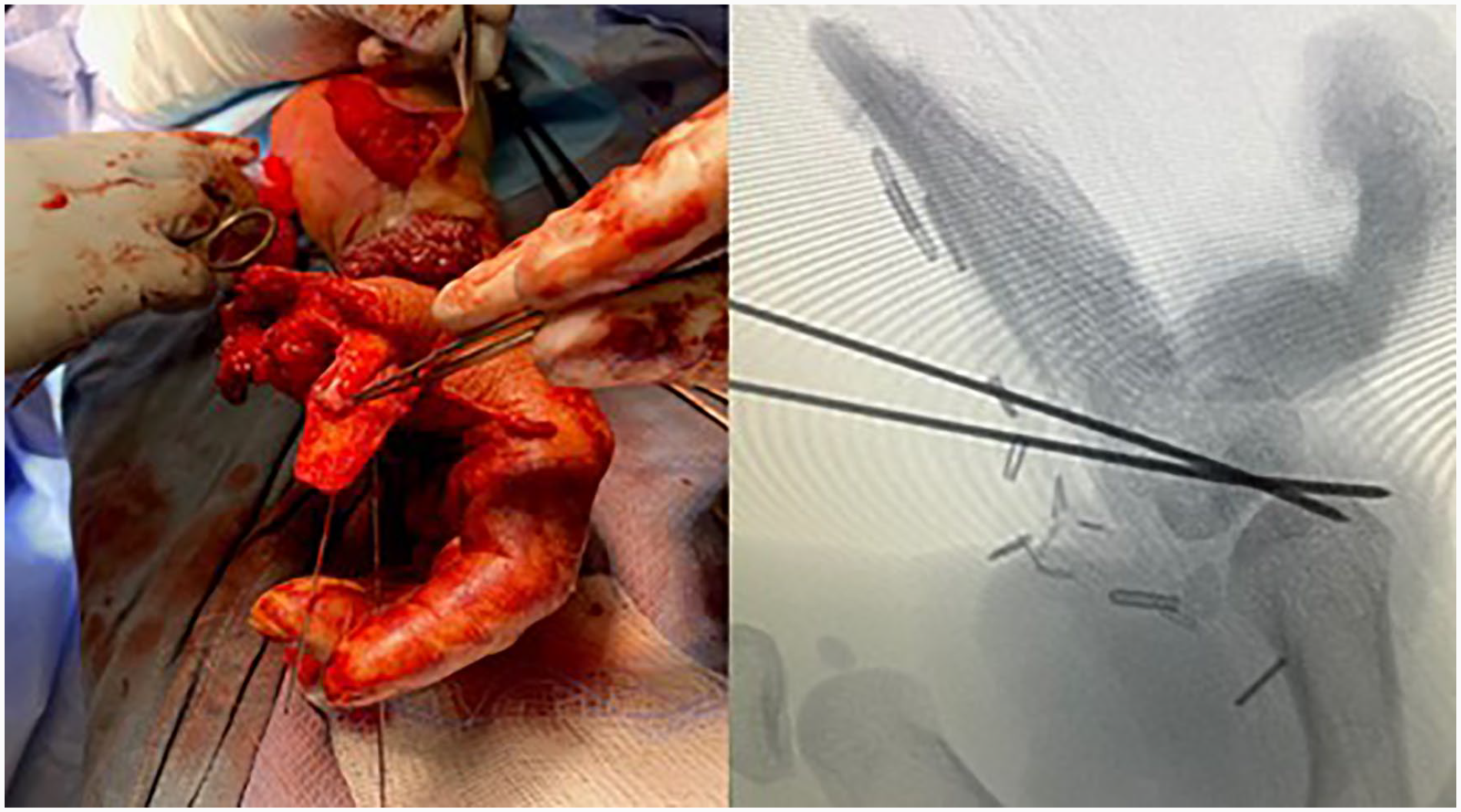
Left: Intraoperative fixation of contoured medial femoral condyle free flap. Extensor pollicis longus (EPL) tendon secured with a mini-mitek bone anchor. Right: Plain radiographs immediately post-fixation of contoured medial femoral condyle osteocutaneous free flap to thumb.

Immediate postop with vastus medialis muscle flap with overlying split thickness skin graft.
At 2 weeks postop, the procedure was complicated by complete vastus medialis flap loss (Figure 5). Subsequent debridement and coverage with a contralateral radial forearm free flap was performed. Intraoperatively, the MFCFF pedicle was checked and confirmed to have flow on Doppler. The radial forearm free flap anastomosis was performed end to side to the radial artery at the level of radiocarpal joint.

Two weeks postop demonstrating epidermolysis with vastus medialis free flap necrosis (volar) despite audible Doppler signal and palpable pulse involving his first webspace related to the vein graft.
Postoperatively, there was no further complications encountered. The patient underwent Exogen device therapy at 4 weeks postop to encourage bony union. At the 14 weeks follow-up, he had minimal tenderness, maintained a supple MCP joint, and bony union was confirmed on both CT scan and x-ray (Figure 6). At 6 months postop, soft tissue coverage, and bony construct remained stable (Figure 7). Patient was able to fully abduct his first webspace, perform pincer grasp, and had no difficulty with power grip and fine motor skills, such as opening bottles. At 1-year postoperative, Semmes-Weinstein monofilament (SWM) testing demonstrated that the patient obtained slightly diminished light touch on the ulnar tip of the thumb with a SWM score of 3.61. He has no protective sensation within most of the flap (SWM 4.56) and has diminished protective sensation (SWM 4.56) at the base of the flap. He has normal sensation on the radial aspect of his thumb (SWM 2.83). He also has no pain within his thumb at rest, with movement, or with firm palpation. Grip strength was 21.4 kg and 31.4 kg for his left (injury side) and right hand, respectively.
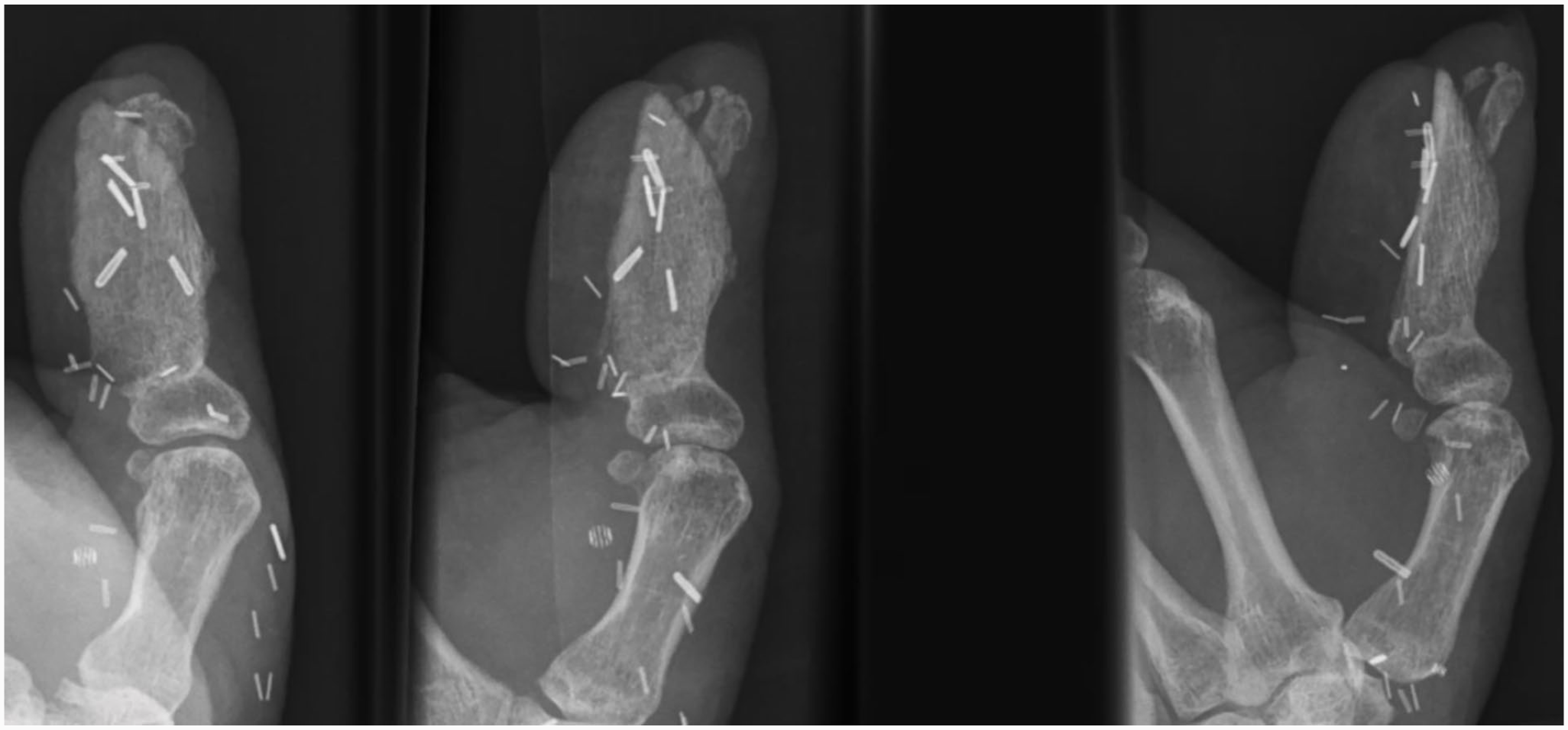
Posteroanterior, oblique and lateral (left to right) radiographic views of left thumb injury 14 weeks postop.
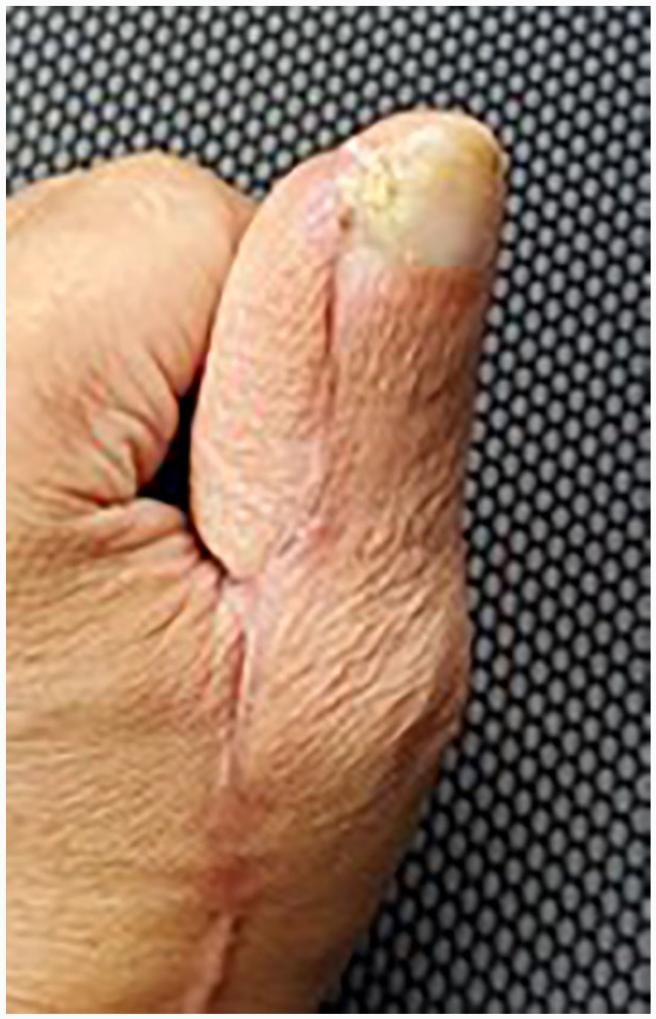
Photo of thumb reconstruction 6 months post-reconstruction demonstrating ample soft tissue based on the radial forearm free flap.
Discussion
A useful algorithm for assessing traumatic thumb defects is to divide the thumb into proximal, middle, and distal thirds. Goals of reconstruction are stable wound healing with early active use, soft tissue stability, and preservation of functional length. In this case, the injury is focused on the middle and distal third of the thumb. Traumatic bony loss resulting in poor functional length was a significant concern. Possible reconstructive alternatives for this patient included antibiotic cement with delayed bone graft, first dorsal metacarpal artery flap, or cross-finger flap, revision amputation with webspace deepening, metacarpal distraction osteogenesis, index pollicization, bone flap, and free toe transfer. The Masquelet technique, while simple and elegant in surgical principle, still would have required vascularized soft tissue coverage and necessitated a multi-stage operation and long period of immobilization preventing early return to function. 5 Revision amputation with webspace deepening would have resulted in a very short thumb with significant functional deficit and also discarded the sensate radial soft of the thumb, likely decreasing tip sensation and increasing the chances of a painful neuroma. While delayed metacarpal distraction osteogenesis after amputation can be effective, it requires a prolonged period of distraction, consolidation, and patient cooperation with risks of significant stiffness. 6 Index pollicization was felt to be contraindicated given the presence of preserved first metacarpal bone and metacarpophalangeal joint. A first dorsal metacarpal artery flap with antibiotic cement spacer, yet another reasonable option, would require at least 2 stages and can have additional complications with nonunion of non-vascularized bone graft. The cross-finger flap with antibiotic spacer for this patient would have also been a 2-stage operation, and would likely not have provided sufficient soft tissue bulk for the defect. After the first stage, it would have left the antibiotic spacer slightly exposed at the base of the flap, thus increasing the risk of contamination/infection. The patient declined any consideration of great toe transfer. Wearing “flip-flop” sandals was routine in his cultural background, and he could not accept the associated donor defect. A radial forearm osteocutaneous flap would likely have been the best alternative option that would have provided vascularized bone and potentially a single stage reconstruction, barring any complications.
In this case, MFCFF provided the benefit of stable vascularized bony tissue that bridged the bony defect while having minimal donor site morbidity. While the preoperative plan was to potentially utilize a second free flap for soft tissue coverage, the intra-operative finding of a perforator entering the vastus medialis from the same pedicle supplying the MFCFF appeared to be a reasonable option. Although the muscle appeared to be perfused after flap inset, it did not survive despite vein grafts that were patent during the takeback operation. As such, a second free flap for soft tissue coverage was performed.
Medial femoral condyle osteocutaneous free flap is a well-described free flap for avascular necrosis, bony nonunion, osteoradionecrosis, and osteomyelitis.7-12 The MFCFF is supplied by the DGA alongside 2 concomitant veins. 13 The DGA provides the greatest vascularity of the medial condyle of the femur.3,14 Pedicle length in the literature is reported between 6 and 13 cm with a mean of 8 cm15 and cadaveric studies have shown its diameter at the origin to be 1.5 to 3.5 mm, which is suitable for microsurgery. 15 Furthermore, donor site morbidity is low, which is consistent with the patient in this case who has no subjective lower extremity complaints. 16 The flap can also be harvested as an osteocutaneous flap if a skin paddle is desired. 11
Conclusion
Thumb injuries can be divided into proximal, middle, and distal thirds to better determine appropriate surgical management. Trauma resulting in soft tissue envelope and segmental bone loss are significant injuries often resulting in major functional impairment. Goals of reconstruction should aim to achieve length, stability, mobility, sensibility, and cosmesis. In this case report, we demonstrate that a medial femoral condyle free flap can be utilized for phalangeal thumb reconstruction. Our reconstruction preserved MCP mobility allowing for early range of motion, achieved bony and soft tissue stability, preserved sensation, and resulted in satisfactory grip strength and thumb mobility.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from the patient included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.