
Abstract
Background:
Posterolateral rotatory instability (PLRI) results from lateral ulnar collateral ligament (LCL) deficiency. The lateral pivot shift test is used to diagnose PLRI but can be difficult to perform and is poorly tolerated. We present a new maneuver, the Posterior Radiocapitellar Subluxation Test (PRST), that we believe is easier to perform. The purpose of this study was to compare the efficacy and reproducibility of the PRST with the lateral pivot shift test.
Methods:
We obtained 10 cadaveric upper extremity specimens, performed a Kocher approach on each, released the LCL origin in 5, then closed. The specimens were randomized, and 3 attending orthopedic surgeons and 1 resident blindly performed the PRST then the lateral pivot shift test after re-randomization and assessed presence or absence of PLRI. This process was repeated the following day. The data for each test were analyzed for sensitivity, specificity, and accuracy.
Results:
For the blinded testing when comparing PRST with the pivot shift test, overall accuracy was 77.5%, compared with 67.5% (P = .03), sensitivity was 75.0%, compared with 50.0% (P = .003), and specificity was 80.0%, compared with 85.0% (P = .55).
Keywords
Introduction
O’Driscoll and Morrey described posterolateral rotatory instability (PLRI) of the elbow in 1991 and clarified the stages of elbow instability, progressively from PLRI to dislocation.1,2 The common mechanism of elbow dislocation, of which PLRI is the first stage, became better elucidated, with improved understanding of the ligamentous anatomy, especially the importance of the lateral ulnar collateral, or synonymously, the ulno-humeral ligament.1-3 The ulno-humeral ligament was determined to be an essential stabilizer, without which PLRI occurs.1-4 Along with their recognition of PLRI, O’Driscoll and Morrey described a physical examination maneuver (lateral pivot shift test) to aid in diagnosis, and, subsequently, several other provocative tests have been proposed. 1 ,4-7 The original, and still probably the most used, is the lateral pivot shift test. It entails placing the patient supine with the shoulder flexed 90° with the examiner at the head of the table. The forearm is supinated, and the elbow is extended and axially loaded in valgus. In this extended position, the radiocapitellar joint subluxates posteriorly if there is PLRI. As the elbow is flexed, there is a clunk as the radiocapitellar joint reduces, usually when about 40° of flexion is reached. 1 The drawbacks of this test are: (1) inconvenience of patient positioning; (2) the challenge of assessing the amount of pathologic joint translation while concomitantly moving the elbow (limiting the ability to assess subtle degrees of instability); and (3) patient trepidation, limiting sensitivity and the ability to perform the test (generally not more than once in the office due to apprehension in an awake patient).6-8
The senior author devised a simple and versatile test for PLRI, which was named the Posterior Radiocapitellar Subluxation Test (PRST). The PRST is performed with the patient either sitting, standing, or supine with the examiner standing or sitting on the same side of the patient as the injured arm. Facing the patient, with the patient’s injured elbow flexed no more than 90° and the forearm in neutral rotation, the examiner grasps the patient’s wrist using the same sided hand as the patient’s injured elbow (eg, examiner’s right hand for right elbow injury). The examiner’s opposite thumb is placed into the lateral elbow soft spot (bordered by the radial head, capitellum, and olecranon) to palpate the posterior aspect of the radiocapitellar joint. A valgus load is applied to the elbow, as the forearm is passively supinated. If there is PLRI, posterior radiocapitellar subluxation can be palpated, often accompanied by a sulcus sign in the soft spot. The supination maneuver can be done multiple times to confirm findings, as in the senior author’s experience, awake patients will allow several tests without undue complaints of pain (Figure 1).

Visualization of the examination set up.
The purpose of this study was to evaluate the accuracy, sensitivity, specificity, and reliability of the original lateral pivot shift test compared with the PRST.
Materials and Methods
We obtained 1 fresh cadaver upper extremity from shoulder girdle to fingers after completing the Anatomical Material Request Application required by our institution. As a preliminary study, we took fluoroscopic lateral images of the elbow in 90° of flexion, and then while performing the PRST. Then we did a lateral approach through the Kocher interval, 9 exposing the lateral collateral ligament complex (LCL; consisting of the ulno-humeral ligament, radial collateral ligament, and the annular ligament). First, we detached the entire LCL origin from the lateral epicondyle and repeated the fluoroscopic images in 90° of flexion, and then while performing the PRST. This sequence was repeated after releasing the ulno-humeral ligament from its insertion on the crista supinatoris, and then cutting the annular ligament. Fluoroscopic images were analyzed for differences in radiographic stability.
For the second part of the study, 1 investigator exposed the lateral elbow through the Kocher approach in 10 additional fresh cadaver specimens. We defined PLRI in our study as having the LCL humeral origin released. Therefore, in the 5 PLRI specimens, the entire LCL was freed from the humerus, and the incision closed with a running 2-0 nylon stitch. In the other 5 control specimens, the LCL was left intact, and the incision closed similarly. The 10 specimens were then randomized for instability testing.
On day 1, the blinded participants, including 3 hand surgery fellowship-trained attending orthopedic surgery faculty members, and 1 junior resident, performed the standard lateral pivot shift as described by O’Driscoll on each of the 10 specimens. The supine shoulder flexed overhead position was simulated by manually stabilizing the scapula to a heavy table. If PLRI was detected via palpable subluxation, the examiner recorded a “yes,” and a “no” if they did not detect PLRI. 1 The examiners then left the room, and the specimens were re-randomized and renumbered by the investigator who performed the initial dissections. Each participant then performed the PRST test as previously described. “Yes” or “no” was recorded depending if PLRI was detected. On day 2, the 10 specimens were re-randomized and numbered, and the tests were repeated. The participants were unaware how many of the 10 specimens had PLRI.
The data for each test were analyzed for accuracy, sensitivity, specificity, as well as interobserver and intraobserver reliability. A χ 2 test was used to assess statistical differences between the accuracy, sensitivity, and specificity of the tests. Statistical difference was associated with a P value of .05 or less. Kappa values were calculated using SPSS version 26 software to assess the interobserver and intraobserver reliability of the tests. Specifically, intrarater reliability was assessed for each tester on 2 separate days for each test yielding a kappa value for each tester. Interrater reliability was assessed using values from 1 single test day among all 4 testers yielding a Fleiss kappa value for each test.
Results
The fluoroscopic images of the unaltered preliminary specimen showed no radiocapitellar subluxation with the PRST (Figure 2b) compared with the unstressed elbow flexed to 90° (Figure 2a). With the disruption of the LCL origin, we saw moderate radiocapitellar subluxation with the PRST, and the degree of subluxation increased after releasing the insertion of the ulno-humeral ligament from the crista supinatoris (Figure 2c and 2d). However, it was not until the annular ligament was cut that we saw full radiocapitellar dislocation and perching of the coronoid process with the PRST (Figure 2e).
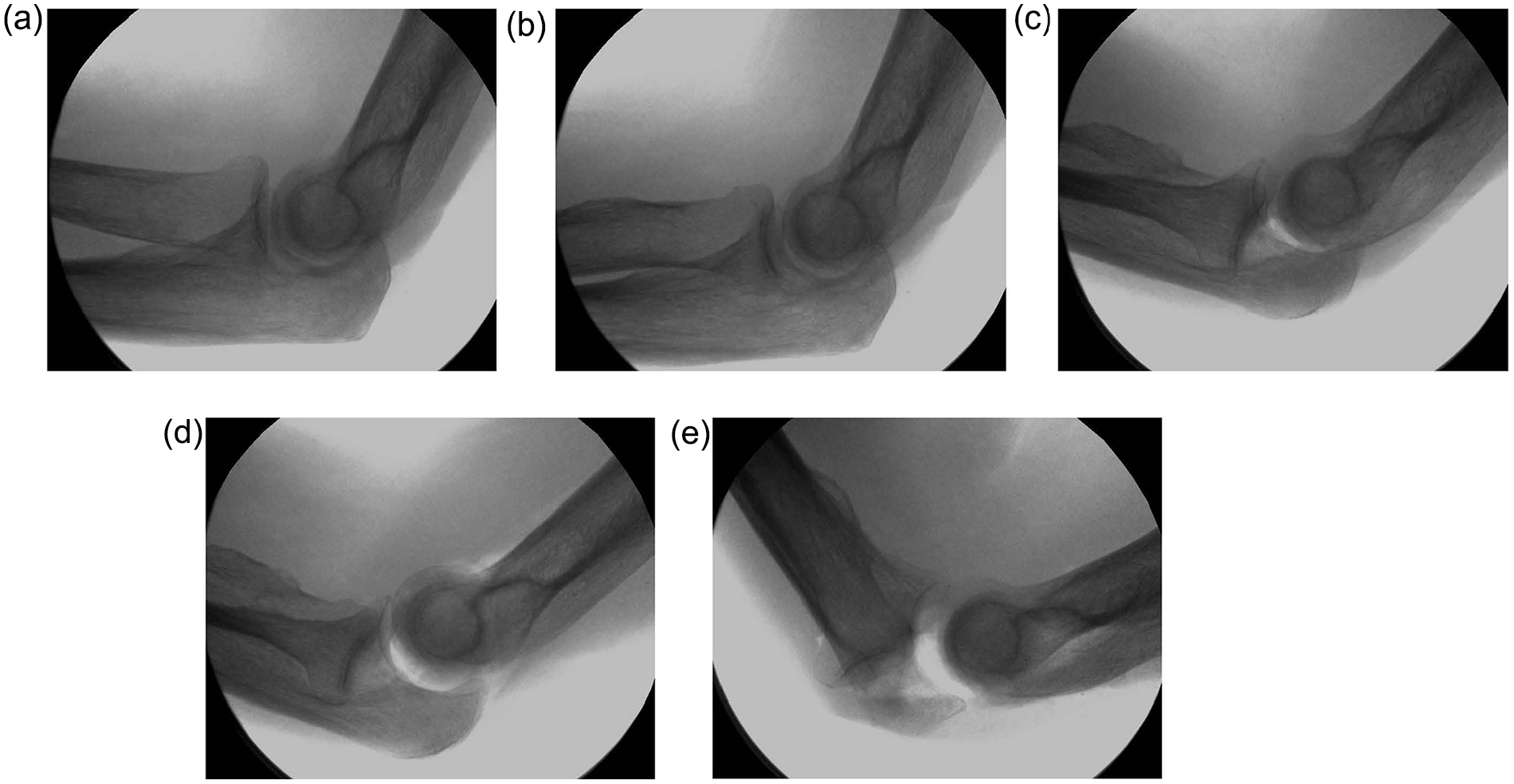
Fluoroscopic imaging with the PRST.
The overall accuracy of the PRST for detecting PLRI caused by detachment of the LCL origin was 77.5%, compared with 67.5% for the pivot shift test. There was no statistical difference in accuracy between the tests for each examiner (Table 1). The overall sensitivity of the PRST test was 75.0%, while the sensitivity of the pivot shift test was 50.0%. The overall specificity of the PRST was 80.0%, and the specificity of the pivot shift test was 85.0%.
Accuracy, Sensitivity, and Specificity for the PRST Versus the Pivot Shift Test in 10 Cadaver Elbows to Detect Posterolateral Rotatory Instability.
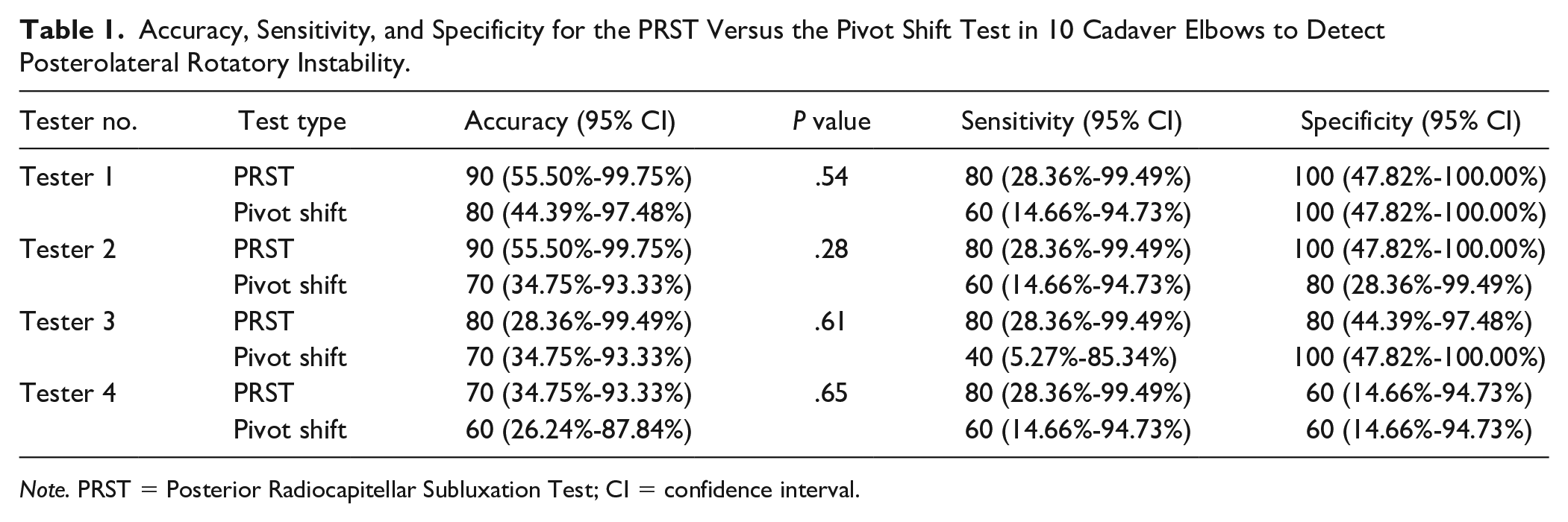
Note. PRST = Posterior Radiocapitellar Subluxation Test; CI = confidence interval.
The kappa values for intraobserver reliability, comparing day 1 with day 2 for each of the testers, ranged from 0.17 to 0.58 for the PRST and –0.15 to 0.74 for the pivot shift test. The number of unstable specimens identified correctly by each tester on each day can be seen in Table 2 along with their individual intrarater reliability and years of practice experience. The average intraobserver reliability for each test was 0.28 and 0.24 for PRST and pivot shift, respectively. For interobserver reliability, the Fleiss multirater kappa values were 0.43 for the PRST, and 0.19 for the pivot shift test.
Number of Accurately Identified PLRI Specimens by Each Tester and Test Type (PRST and Pivot Shift) and Their Individual Intrarater Reliability.
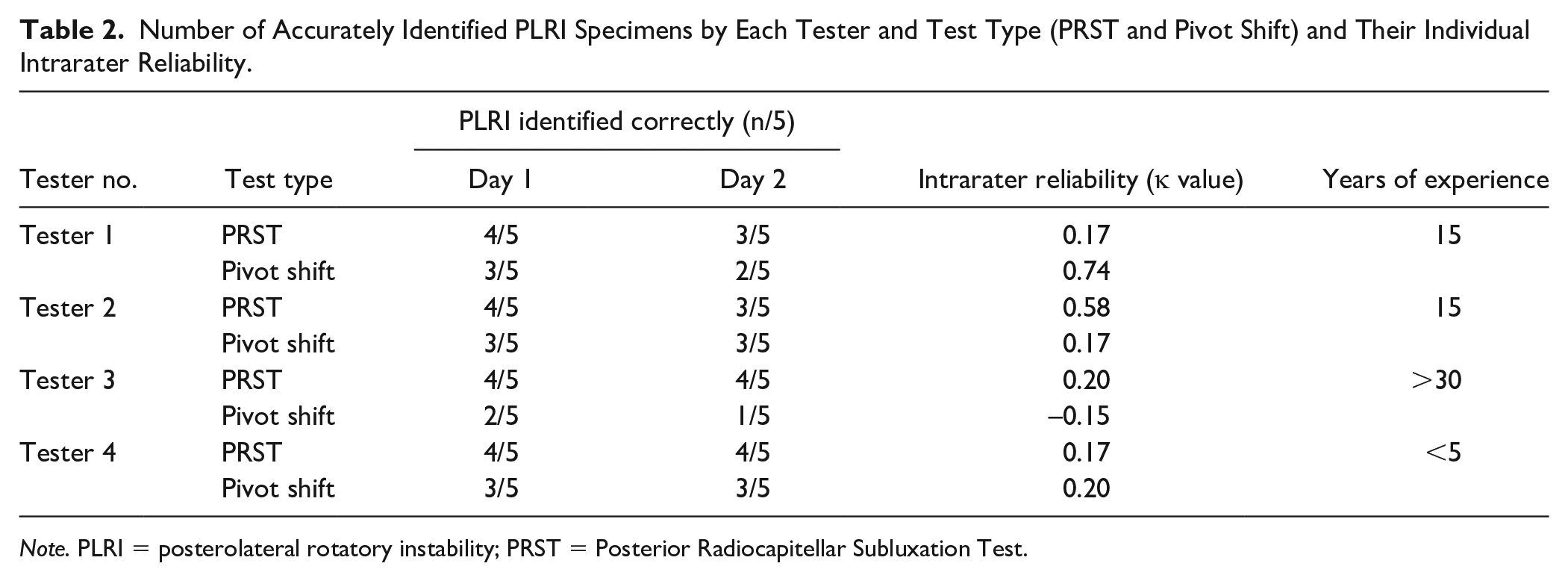
Note. PLRI = posterolateral rotatory instability; PRST = Posterior Radiocapitellar Subluxation Test.
Discussion
Physical examination for detecting PLRI can be challenging, and several tests have been described. These include the lateral pivot shift, the lateral pivot shift apprehension test, the posterolateral rotatory drawer test, tabletop relocation test, chair push-up test, and prone push-up test. The lateral pivot shift was described earlier in this article. The lateral pivot shift apprehension test is performed similarly as the pivot shift except a positive response is apprehension as opposed to instability. 7 The posterolateral rotatory drawer test is better tolerated in an awake patient and is performed in the same position as the pivot shift with a similar axial valgus load. A posterior rotatory drawer maneuver is performed at various positions of elbow flexion assessing degrees of instability, with maximal instability perceived at 20° to 40° of flexion. 10 The tabletop, chair, and prone push-up tests are all similar, with the patient pushing up with elbows pointing laterally and forearms supinated. As patients push up, apprehension indicates a positive test. In the tabletop relocation test, after first experiencing apprehension with an initial push-up, the patient tries pushing up again with the examiner placing thumb pressure on the posterior radial head preventing subluxation. If there is apprehension with the initial push-up that is prevented by stabilizing the radial head, PLRI is likely. If the stabilizing thumb is subsequently removed during the push-up, and apprehension is again manifest, this is even more confirmatory. 5 In a study by Arvind and Hargreaves of 8 patients diagnosed with PLRI by a positive pivot shift test, the tabletop test was also positive, indicating similar sensitivity of the tabletop push-up test as the pivot shift test. 5 In Regan and Lapner’s series of 8 patients, all diagnosed with PLRI, 38% had a positive pivot shift test when awake, 100% had a positive test when under anesthesia, and the chair and prone push-up tests were positive in 88% of the patients. 6 Ultrasonography has also been used to help in the office diagnosis. 11
A criticism of available clinical studies comparing and assessing the efficacy of provocative tests is that patient numbers were small and all patients in the studies were diagnosed with PLRI, with no real criterion standard, other than a diagnosis based on clinical grounds or a positive pivot shift test as the reference. 12 Studies performed in patients predetermined to have PLRI can lead to a high bias and potentially an abnormally high sensitivity and positive predictive value of the diagnostic test. 12 Test accuracy, however, cannot be determined. Our study eliminated these problems by randomization and an equal number of lesioned and unaffected limbs.
Our findings in the preliminary cadaver elbow specimen showed that with detachment of the LCL origin, the PRST maneuver revealed radiographic posterior radiocapitellar subluxation. Incremental increasing radiographic instability occurred with the PRST maneuver after subsequently detaching the ulno-humeral ligament from the crista supinatoris and then cutting the annular ligament. The radiographic changes coincided with the tactile feel of posterior radiocapitellar subluxation and the sulcus sign. We felt it was important to perform radiographic analysis in a preliminary specimen, to clarify what we meant by PLRI. We defined PLRI in our study as posterior radiocapitellar subluxation following LCL humeral origin release, which was confirmed radiographically on our preliminary specimen as a reference and detectable by the PRST.
As the focus of our investigation, we found the PRST was no less effective in identifying PLRI than the well-established pivot shift test in cadavers as performed by 3 attending staff and 1 orthopedic resident. There were no statistical differences in the accuracies of the PRST from the pivot shift test, and sensitivity and specificity of the tests were comparable.
While the range of the kappa values for intraobserver reliability was slightly better for the PRST than the pivot shift test, and the Fleiss multirater kappa value for interobserver reliability was closer to 1 for the PRST than the pivot shift test (0.43 vs 0.19); overall, the kappa values for intraobserver and interobserver reliability were low for both examinations for testers with all years of experience. We were surprised that intraobserver and interobserver agreement was low for both tests in our study, especially because others have shown that most of the mechanics for the pivot shift test were repeatable for a given surgeon. 13 One possible explanation for this could be that while our testers were shown how to do each test as previously described, there was no specific standardization on performance methods and what constitutes a positive test, which could be noted as a weakness in our experimental design.
As a cadaver study, the conditions for assessing elbow instability were ideal insofar as there was no confounding influence of patient apprehension, resisting the examination maneuvers. Thus, the comparison of our PRST maneuver and the pivot shift tests is as if we were comparing them in anesthetized patients. It is well known there is significant apprehension and diminished sensitivity performing the pivot shift test in the awake patient. 6 It has been the lead author’s experience that the PRST can be performed relatively comfortably and repeated for confirmation of findings by the examiner in most awake patients. Although not proven in this study, we think the PRST could be more accurate than the pivot shift in awake patients.
Understandably, there are drawbacks to extrapolating a cadaver study to the live patient. Cadaver extremities have different compliance, and the simulated lesion may not be the same as the true traumatic lesion. That the specimen was only an upper extremity from fingertips to scapula, the elbow may have behaved differently during testing than if it was attached to an entire body. However, despite these limitations, the authors believe the findings of the study are worthwhile and believable.
We have proposed and tested a new simple and versatile provocative test for PLRI that is at least as accurate and reproducible as the well-accepted lateral pivot shift test. Its benefits are that it is convenient, easily performed, and is not significantly painful (in the author’s experience) to be associated with apprehension in the awake patient. The ability to perform the test in virtually any patient position allows the test to be used in the operating room to assess PLRI intraoperatively, before and after ulno-humeral ligament repair or reconstruction. It is perhaps in this setting where the PRST sets itself apart from the other tests. This can be visualized in the supplementary video.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not required for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.T.L. has received payment for a DJO educational event. R.A.A. has received consulting fees from the American Board of Orthopedic Surgery, TriMed, Inc., Auxilium Biotechnologies Inc., Johnson & Johnson (Synthes), payment for a TriMed, Inc. educational event, and payment for expert testimony. S.R.W. has grants with the National Institutes of Health, the Department of Defense, NuVasive, and the Wu Tsai Foundation, and has leadership roles in the San Diego Spine Foundation and Operation Walk. The remaining authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.