
Abstract
Exercise professionals often hold anti-fat attitudes, which contribute to weight stigma and discrimination in physical activity contexts. This study examined the effects of an online weight stigma intervention on exercise professionals’ attitudes toward fatness. Participants were 105 exercise professionals who were employed at least part-time at university recreation centers in the United States. In this randomized controlled trial, participants were randomized into an intervention online course to decrease weight stigma or a control online course to learn about communication techniques to enhance motivation for physical activity. Attitudes about fatness were assessed at pre- and post-course using the Fat Attitudes Assessment Toolkit (FAAT). There were significant increases in the fat acceptance composite score in the intervention group compared to the control group, suggesting recreation center staff who completed the intervention WIT FITS course experienced more positive evaluations of fat people as a result of the intervention.
Introduction
Most college students have access to University Recreation Centers (URCs) to engage in physical activity (PA), yet students often find these spaces unwelcoming (Powers et al., 2019). While all students must pay mandatory fees that fund these facilities, not all college students use their URCs (Todd et al., 2009; Young et al., 2003). In fact, men are more likely to use URCs than women (Milton & Patton, 2011; Watson et al., 2006; Zizzi et al., 2004). Furthermore, in a 2008 study, Miller and colleagues found that women who “perceive themselves as slightly to very overweight” are less likely to use their campus recreation centers (p. 95). Likewise, Vartanian and Shaprow (2008) revealed that female college students who reported higher body dissatisfaction were more likely to avoid exercise.
Researchers have shed light on the relationship between weight stigma and exercise avoidance, highlighting the prevalence of weight stigma across the PA landscape (Panza et al., 2018; Pickett & Cunningham, 2017a, 2017b; Rich & Mansfield, 2019; Vartanian & Shaprow, 2008). Weight stigma refers to unfavorable attitudes and perceptions linked to body weight, which may manifest as stereotypes, exclusion, bias, and discriminatory actions (Hart et al., 2020). Often, exercise professionals hold anti-fat attitudes and misconceptions about the relationship between health and weight, contributing to weight stigma and discrimination in PA contexts (Lee et al., 2023; Panza et al., 2018). Weight stigma and discrimination can hinder meaningful and lifelong PA enjoyment and participation for all, especially for people living in larger bodies (Jackson & Steptoe, 2017). Further, researchers have revealed associations between weight stigma and various adverse mental and physical health outcomes, including PA avoidance (Puhl & Suh, 2015; Vartanian & Novak, 2011).
Thus, interventions designed to decrease weight stigma across PA settings are warranted. Specifically, scholars have shown the need to provide exercise professionals with educational opportunities (Souza & Ebbeck, 2018; Rote et al., 2018) to help them: (a) identify their biases, (b) reflect on their assumptions about the relationship between health and weight, and (c) apply practical strategies to create weight-inclusive climates in PA settings. While there have been few such interventions, initial outcomes have shown improvements in participants’ anti-fat attitudes (Rote et al., 2018; Rukavina et al., 2008, 2010; Wijayatunga et al., 2019)—however, previous interventions were limited to kinesiology undergraduate students rather than exercise professionals.
In a systematic review of weight bias reduction studies for healthcare professionals, Alberga and colleagues (2016) found that many of the interventions were not randomized, and overall evidence of effectiveness was poor. Moreover, those initiatives were facilitated as in-person programs, limiting their reach and scalability. To date, the available online weight stigma interventions have only targeted populations other than exercise professionals, such as nurses (Gamaly, 2022), medical staff (Sherf-Dagan et al., 2022), and health-related undergraduate students (Raffoul et al., 2023).
The present study addresses the pressing issue of weight stigma and its association with exercise avoidance, particularly within the context of college PA facilities. The existing body of research underscores the importance of implementing interventions to reduce weight stigma in PA settings. A significant research gap exists concerning the development and evaluation of online weight stigma interventions tailored specifically for exercise professionals. This study seeks to bridge this gap by developing and assessing the effectiveness of an online weight stigma intervention designed specifically for exercise professionals, with the ultimate goal of fostering more inclusive and welcoming environments within URCs. The study aims to answer the following research question: What is the impact of an online intervention on URC exercise professionals’ attitudes toward fatness and fat individuals?
Theoretical Framework
Similar to previous weight stigma reduction interventions (e.g., Wijayatunga et al., 2019), our weight stigma intervention course was informed by attribution theory (Gerend et al., 2020). Attribution theory suggests one's attribution of events influences one's subsequent affective responses, attitudes, and behaviors (Weiner et al., 1988). When applied to weight stigma, attribution theorists explain that one's attribution of fatness has a subsequent impact on one's attitudes and behaviors (Täuber et al., 2018; Wijayatunga et al., 2019). For example, if one attributes fatness to internal and controllable factors such as self-discipline, one is more likely to hold negative attitudes towards fat people and feel shame about their own fatness. Thus, through our weight stigma intervention course, we aimed to retrain participants’ attributions toward fatness by summarizing research on the complex relationship between health and weight and explaining that fatness and ill health cannot be attributed solely to internal and controllable factors.
Methods
Study Design
This study followed a randomized controlled trial (RCT) design, as described by Kendall (2003). Participants were randomized into the intervention online course to decrease weight stigma or into a control online course to learn about communication techniques to enhance motivation for PA. All participants completed a pre- and a post-course survey to assess their attitudes towards body size.
Participants
Participants were 105 exercise professionals who were employed at least part-time at URCs in the United States. Participants’ mean age was 33.77 (sd = 11.29) years old. Participants were majority female (59.0%) and white (74.3%; See Table 1). Of the 105 participants, 68 (64.8%) held managerial positions (e.g., directors, coordinators, or managers), 14 (13.3%) were class instructors or personal trainers, 9 (8.6%) identified as staff, 9 (8.6%) were interns or graduate assistants, and 1 (0.9%) identified as professor and their position in the campus recreational center was not clear. Four participants did not answer this question.
Participants’ Demographics.
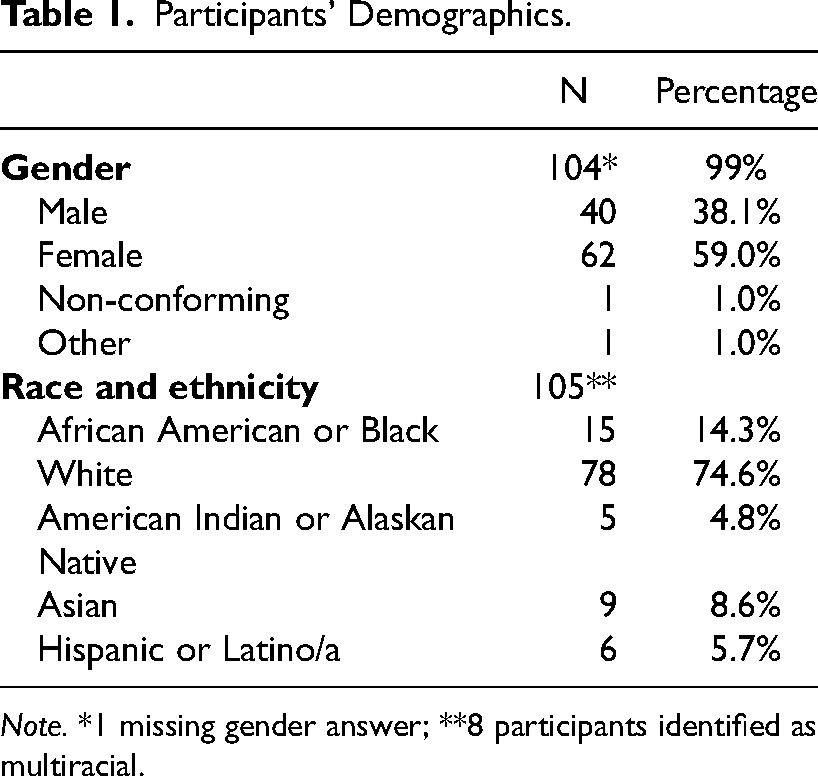
Note. *1 missing gender answer; **8 participants identified as multiracial.
Upon approval from the second author's institution's ethics review board, recruitment emails were sent out to campus members of the National Intramural-Recreational Sports Association (NIRSA): Leaders in Collegiate Recreation organization. Participants were also recruited through convenience and snowball sampling, with members of the research team sending the recruitment email to colleagues. In the recruitment email, participants were asked to complete the study and forward it to others working in campus recreation centers.
Intervention and Control Courses
Two online courses were developed for this study. The intervention course, “Weight-Inclusive Thinking for Fitness Spaces” (WIT FITS), was an approximately a 2-hour, self-paced, interactive online course on weight inclusivity for fitness professionals. This course was developed based on the results of a needs assessment survey of URC leaders (Lee et al., 2023; Zuest et al., 2021) and the Health at Every Size® (HAES®) paradigm. The HAES® approach, as trademarked by the ASDAH (2023), advocates for dismantling sizeism and healthism. Through the intervention course, we introduced the HAES® approach and each of its five principles: weight inclusivity, health enhancement, respectful care, eating for well-being, and life-enhancing movement. We also introduced weight stigma reduction strategies participants could implement at intrapersonal, interpersonal, and structural levels (Cook et al., 2014; Zuest et al., 2022). In a single-arm pilot study of the intervention course, Zuest et al. (2023) found that the online course significantly decreased exercise professionals’ anti-fat attitudes from pretest to posttest. Minor changes were made to the course to address participants’ feedback.
The control course was an approximately 2-hour, self-paced online course on communication strategies for fitness professionals. This control course, titled Motivation to Move, taught participants how to assess an individual's stage of change for increasing physical activity and provided specific strategies to enhance motivation through concepts such as autonomy support and exploring intrinsic motivation for change. The course adapted concepts from the transtheoretical model (TTM; Prochaska & DiClemente, 1983), self-determination theory (SDT; Deci & Ryan, 1985), and motivational interviewing (Miller & Rollnick, 2013) and touched on aspects of inclusivity without directly addressing weight stigma. Specifically, we informed participants that SDT posits that motivation ranges from controlled to autonomous, with more long-term changes occurring with higher levels of autonomous motivation (Ryan & Deci, 2000). We also informed participants about communication techniques derived from motivational interviewing. This communication approach honors autonomy and helps strengthen peoples’ reasons for change and how they could integrate these skills into their work (Miller & Rollnick, 2013). Both courses were developed by an interdisciplinary faculty and student research group and were interactive in nature. Courses included a mix of short videos, text, infographics, and quizzes.
Instruments
Demographics
Demographic questions included questions about participants’: age, gender, race, ethnicity, job title, length of time working in the fitness industry, state where their campus recreation center was located, and highest degree earned.
Fat Attitudes Assessment Toolkit (FAAT)
We used the Fat Attitudes Assessment Toolkit (FAAT; Cain et al., 2021) to examine participants’ attitudes toward body size before and after completing the intervention or control courses. The FAAT is a validated questionnaire comprising 49 statements that are rated on a Likert scale of 1 (strongly disagree) to 7 (strongly agree). It contains nine subscales: empathy (7 items; e.g., “fat people face discrimination in many areas of life”), activism orientation (7 items; e.g., “discrimination due to fatness leads to a denial of human rights”), size acceptance (6 items; e.g., “size acceptance should be encouraged”), attractiveness (5 items; e.g., fat people are attractive”), critical health (5 items; e.g., “fat people are not necessarily unhealthy”), general complexity (6 items; e.g., “there are biological factors that result in people being fat”), socioeconomic complexity (3 items; e.g., “there are economic factors that contribute to people being fat”), responsibility (6 items; e.g., “fatness is the result of lifestyle factors”), and body acceptance (4 items; e.g., “I feel good about my body”). The total score is calculated by summing all items’ scores after reversing the responsibility subscale scores.
In addition to the total score, the score from five subscales is added to calculate an overall fat acceptance composite score, which assesses participants’ alignment with “critical fat perspectives, and higher scores on these scales indicate more positive evaluations of fat people” (Cain et al., 2021, p. 20). The scores from two subscales (general complexity and socioeconomic complexity) are added to calculate an attribution complexity composite score, which assesses the controllability of participants’ attributions about fatness. In other words, the score indicates whether the participant attributes fatness as within or outside one's control, with higher scores indicating external attributions (Cain et al., 2021). The responsibility subscale also measures the degree to which participants attribute fatness to internal factors such as self-control or willpower (Cain et al., 2021). Finally, the body acceptance subscale assesses “how respondents appraise their own bodies within the broader social context” (e.g., “I do not feel defined by my weight”) (Cain et al., 2021, p. 20). Higher scores indicate that participants’ self-concepts are not dependent on their weight. In this study, the internal consistency in the nine subscales pre-and post-intervention were all at least acceptable (2 acceptable, 7 good, and 9 excellent), with Cronbach's alpha reliability ranging from .77 to .98.
Procedures
Once participants completed the pre-test, they were randomly assigned to either the intervention or control course through a final Qualtrics survey question that randomized instructions to enroll in the control or intervention course. The final sample included 50 participants in the intervention and 55 in the control group. As part of the last step of the course, participants were instructed to complete the post-test. Once participants completed the pre-test, online course, and post-test, they received a $40 electronic gift card. Although 212 people completed the pre-test, only 125 people completed the course. Of those, 121 completed the post-test, which shows a 41% attrition rate. Additionally, 17 participants did not correctly fill in their identification numbers, which prevented the researchers from including them in the final data analysis. A series of five independent samples t-tests comparing the participants who completed the study with those who did not, show no significant differences between the two groups in the five dependent variables at pre-intervention (see Table 2).
Comparison of the Five Dependent Variables Between Participants who Finished or Dropped the Study at Pre-Intervention.
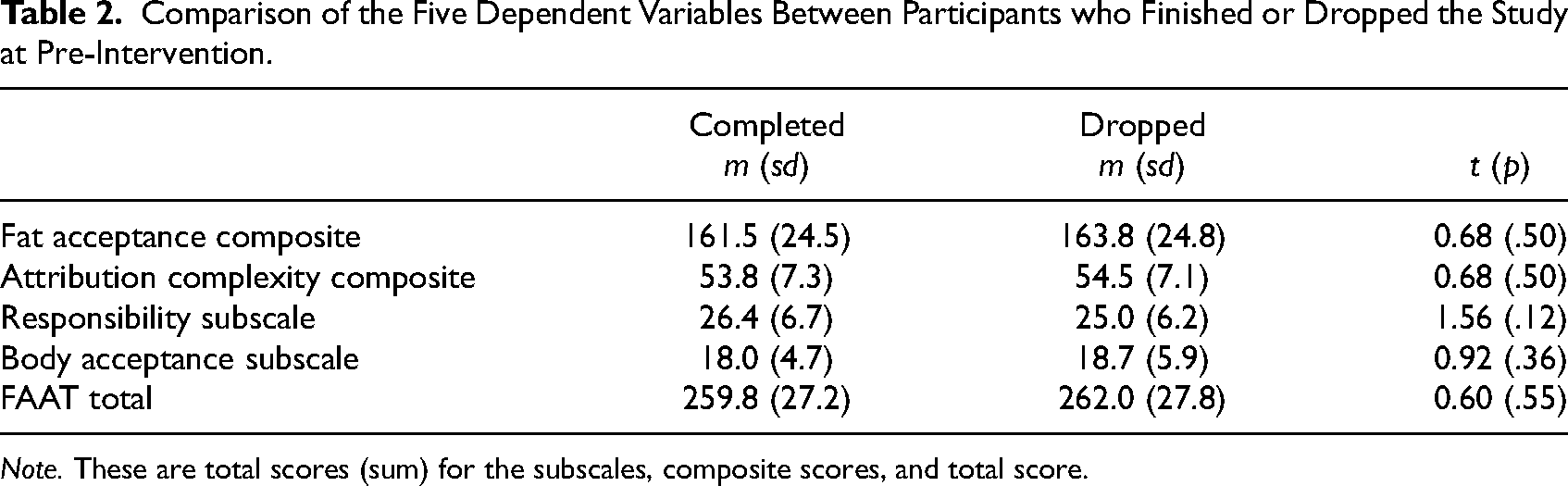
Note. These are total scores (sum) for the subscales, composite scores, and total score.
Data Analysis
The IBM Statistical Package for the Social Sciences (SPSS, Version 28) was used to analyze data. First, mean, standard deviation, and frequencies were calculated for the participants’ demographics. Following, three Independent Samples t-tests identified that there were no significant differences between the intervention and control groups for pre-intervention FAAT score, t(103) = 0.38, p = .708, fat acceptance composite score, t(103) = 0.19, p = .847, attribution complexity composite score, t(103) = 0.67, p = .492, responsibility subscale, t(103) = 0.32, p = .749, and body acceptance subscale, t(98.3) = 1.74, p = .085.
A series of five ANCOVAs, one for each dependent variable (total FAAT score, Fat Acceptance, Attribution Complexity, Responsibility, and Body Acceptance), was used to compare post-intervention scores between groups with their pre-intervention score as a covariate. As such, the pre-intervention questionnaire scores for each dependent variable were entered as covariates in each ANCOVA, and group assignment (intervention x control) was entered as a fixed factor. Effect size categories for eta squared were set at .02 (small), .13 (medium), and .26 (large), as suggested by Harlow (2014).
Results
FAAT Total Score
An ANCOVA revealed that the intervention group had a significantly higher mean score on the FAAT questionnaire than the control group after the intervention, after controlling for their pre-test scores, F(1,102) = 34.39, p < .001, with medium effect size, η2 p = .25. For pre- and post-course mean scores, see Table 3.
ANCOVA Results.
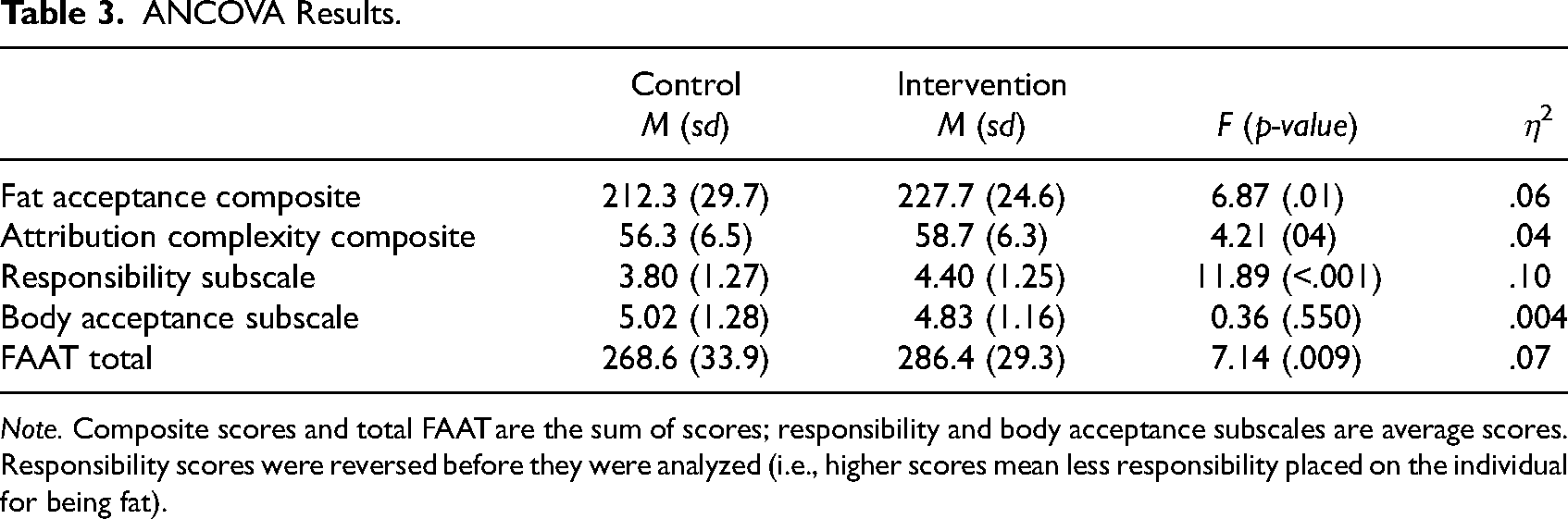
Note. Composite scores and total FAAT are the sum of scores; responsibility and body acceptance subscales are average scores. Responsibility scores were reversed before they were analyzed (i.e., higher scores mean less responsibility placed on the individual for being fat).
Fat Acceptance Composite Score
An ANCOVA with the Fat Acceptance Composite Score as the dependent variable showed that the intervention group had significantly higher fat acceptance than the control group at the end of the intervention period, after controlling for their initial Fat Acceptance Composite Scores, F(1,102) = 25.29, p < .001. The effect size of the intervention was medium, η2 p = .20.
Attribution Complexity Composite Score
The ANCOVA with Complexity Composite Score as the dependent variable showed that the intervention group had a significantly higher Complexity Composite Score than the control group at the end of the intervention period after controlling for their initial Complexity Composite Score, F(1,102) = 4.21, p = .043. However, the intervention's effect size was small, η2 p = .04.
Responsibility Subscale
The ANCOVA with the Responsibility Subscale as the dependent variable showed that the intervention group placed significantly less responsibility on the individual for their weight than the control group at the end of the intervention period, after controlling for their initial Responsibility Subscale score, F(1,102) = 11.89, p < .001. However, the intervention’s effect size was small, η2 p = .10.
Body Acceptance Subscale
The ANCOVA with the Body Acceptance Subscale as the dependent variable showed that the intervention group did not have significantly different acceptance of their own body than the control group at the end of the intervention period, after controlling for their initial Body Acceptance Score, F(1,102) = 0.36, p = .550, η2 p = .004.
Discussion
Given the exercise avoidance patterns of college students who experience body dissatisfaction (Vartanian & Novak, 2011; Vartanian & Shaprow, 2008), high-reach interventions are needed to enhance weight-inclusivity in fitness center spaces located in university settings and beyond.
The FAAT was recently designed to measure “the effectiveness of weight-stigma reduction interventions” (Cain et al., 2021, p. 20) and, with robust reliability and validity scores, was selected to measure changes in attitudes surrounding fatness of participants completing our 2-hour online course. URC employees assigned to the WIT FITS course experienced significantly improved total FAAT scores from pre- to post-course compared to those assigned to the control course.
Anti-fat attitudes also improved in the pilot study of the WIT FITs curriculum from pre to post-intervention in a small sample of 36 recreation center employees; however, given the single-arm study design, a more rigorous study design was needed to show causation [Authors blinded]. The present study is the first known RCT aimed at addressing attitudes about fatness among fitness professionals.
Our research findings suggest that a two-hour highly interactive online course informed by attribution theory and the HAES® paradigm provides an adequate dose to impact attitudes about fatness. Previous research with shorter technology-based high-reach interventions has been well-received but not always effective (Raffoul et al., 2023; Sherf-Dagan et al., 2023). Students reported preferring interactivity and engagement with online educational content (Raffoul et al., 2023). Working professionals may have limited time to complete educational courses, which may have contributed to the 41% attrition rate for the 2-h intervention and control. While completion rates may be lower in longer self-paced interventions, the in-depth and interactive nature of the WIT FITS modules sustained the majority of users and positively influenced attitudes about fat acceptance, weight, and health. In the present study, participants received payment for completing the courses, and it is unknown if completion rates would be as high for a 2-h course without incentives or mandating course completion, as is common in worksite training.
In the present study, there were significant increases in the fat acceptance composite score in the intervention group compared to the control group, suggesting recreation center staff who completed the WIT FITS course experienced more positive evaluations of fat people as a result of the intervention. No other studies have measured how interventions aimed at addressing attitudes about fatness have specifically measured changes in fat acceptance.
There were also improvements in the attribution composite score and the responsibility subscale from pre- to post-course in the intervention group compared to the control group. This indicates that URC employees who completed the WIT FITS course were less likely to attribute fatness to internal factors such as self-control or willpower and more likely to attribute fatness as a factor outside one's control. Wijayatunga and colleagues (2019) also noted improvements in weight control/blame as a result of their classroom-based intervention on kinesiology students.
Attribution theory informed the development of the WIT FITS course, and therefore, modules were aimed at retraining participants’ attributions towards fatness by describing contributors to body weight that go beyond personal responsibility and by debunking the notion that body weight is an appropriate measure for assessing individual health status. Furthermore, the course included information on the prevalence and negative health implications of weight stigma and provided specific examples of strategies to improve weight inclusivity within fitness spaces. The control course was aimed at training recreation staff in communication strategies that can enhance participant motivation. The control course was informed by the TTM (Prochaska & DiClemente, 1983) and the SDT (Deci & Ryan, 1985) and included communication concepts adapted from motivational interviewing (Miller & Rollnick, 2013). Course content described methods to communicate with recreation center participants in a way that supports autonomy and enhances motivation; therefore, participants may have viewed behavior change as something that is within the control of the individual. These differences could explain the significant findings related to attitudes about fatness.
Additional strengths of this study include the RCT design and national recruitment efforts. Another strength of this study is that we used the FAAT, which is a new questionnaire that addresses limitations of previous measurements such as the Anti-Fat Attitudes instruments (AFAT; Lewis et al., 1997). AFAT instruments focus on the negative aspects of fatness and fat individuals, reinforcing stereotypes and contributing to weight stigma (Cain et al., 2021). However, utilizing a new instrument makes it challenging to compare current research findings to previous studies, garnering it as both a strength and a limitation. Other limitations of this study include the homogeneous nature of participants (primarily white females) and the relatively small sample size with low course completion rates, which may be related to the relatively long course length. Follow-up data are also needed to determine if changes in attitudes that occurred from pre- to post-course were maintained long-term. In this study, participants completed the post-test immediately after completing the course. Nevertheless, a follow-up test could show whether participants’ attitude changes were sustained.
As for future directions, this study should be replicated in other fitness settings, such as in public or private gyms. Physical education teachers in both elementary and secondary school settings would also be an interesting population to replicate this study with, as body dissatisfaction from weight-based anxiety starts as young as ten or twelve years (Wang et al., 2019). Future researchers would also do well to gather feedback from either the fitness professionals involved in the study(ies) or their clients/students on how they felt about the care they received, especially with regard to messaging around their bodies.
Conclusion
This study examined the effects of a novel online course aimed at addressing exercise professionals’ attitudes toward body size, e.g., fatness. One hundred and five exercise professionals employed at least part-time at university recreation centers in the U.S. were randomized into the WIT FITS intervention course or a control course. Attitudes toward body shape and size were measured pre- and post-course using the Fat Attitudes Assessment Toolkit (FAAT; Cain et al., 2021). We found significant improvements in FAAT scores among participants who took the intervention course compared to those who participated in the control course. Furthermore, significant improvements were witnessed in the fat acceptance and attribution complexity composite scores and the body acceptance and responsibility subscales.
Our findings suggest that university recreation staff who engaged with the WIT FITS intervention course improved their attitudes about fatness. Specifically, intervention participants experienced shifts in their thinking from weight being a matter of personal responsibility towards a deeper understanding of the complex contributors of body weight. Participants were taught the importance of promoting size diversity and advocating to reduce weight stigma and discrimination. Their improved attitudes towards body size can result in a more welcoming and inclusive campus recreation environment that attracts students from a wider range of backgrounds and body types. Creating a more inclusive campus recreation environment can result in increased use of the facility by the student body, ultimately enhancing physical activity engagement, which is linked to improved physical and emotional health. Furthermore, weight bias training may reduce incidences of weight stigma on campus, thereby supporting the mental health needs of university students. Weight-inclusive educational opportunities and programming across campus can support the diversity, equity, and inclusion initiatives instigated by university administrations.
The results from this study show a promising path forward to both reducing weight stigma and improving attitudes towards fat people among fitness professionals. In the future, university administrators and major campus recreation stakeholders can standardize weight stigma training as part of the onboarding process for new campus rec employees. Ideally, online courses like WIT FITS would be supplemented with in-person staff discussions to explore tangible ways to make individual recreation centers more inclusive. In addition, campus recreation center leaders could assess the individual inclusivity concerns of their student body so that they can adequately address those specific needs to promote size diversity in their recreation spaces.
Footnotes
Acknowledgements
This study was funded by the 2022 NIRSA Research Grant and by the 2022 Association for Applied Sport Psychology (AASP) Collaborative Research Grant. Thank you to the WIT FITS course reviewers: Sookie Bardwell, MA, OCT (Body, Sex & Relationship Coach and Consultant of Shamefree) and Christine Hsu, OCT (Anti-Oppression Sports Inclusion Consultant & Healing-Centered Movement Coach). Thank you to the WIT FITS instructional and web designers: Kari Word (InstructionalDesign Studio LLC) and Dee Word (Tiger-Phoenix LLC).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIRSA Foundation, Association for Applied Sport Psychology (AASP), (grant number 2022 Research Grant, 2022 Collaborative Research Grant).