
Abstract
Emerging studies from low-and-middle-income countries (LMIC) have applied mixed methods to investigate gender-based violence (GBV) syndemics. There is currently no guidance on how to appropriately combine qualitative and quantitative methods when testing syndemic theory. This research introduces a mixed methods framework for testing GBV syndemics in LMIC. A multi-step approach was used for framework development. The framework centers on the distinct strengths of the population perspective (quantitative) and locally grounded perspective (qualitative) and informs the development of (i) measurement tools, (ii) causal models, and (iii) contextual interventions. This article contributes an application of mixed methods to inform the design of studies that robustly test theoretical constructs. Further, this article demonstrates how a sensitive/hidden exposure like GBV contributes to the patterning of chronic and infectious diseases, leading to population health disparities.
Introduction
Epidemics are partly biological, resulting in premature morbidity and mortality via physiological mechanisms at the individual level, and partly social, affecting populations organized along distinct sociopolitical dimensions. A biosocial approach integrates biological and social aspects to the study of epidemics. Since the 1990s, syndemics have emerged as one notable application of the biosocial approach in global health, integrating infectious and chronic diseases with social and political inequalities. Mixed research methods, combining qualitative and quantitative approaches, can holistically address the biological and social aspects of syndemics.
We begin by first providing an overview of syndemic theory, which we expand on in the later theory section. Syndemics are theorized to occur when inequitable sociopolitical conditions promote the clustering and interaction of two or more epidemics, yielding an exacerbated population health burden that is greater than that sum of its parts (Singer, 1996; Singer et al., 2017; Vahedi et al., 2025). The theory has made significant contributions to global health by providing a unifying biosocial framework which emphasizes the interconnection between epidemics and context. Syndemic theory has been applied to holistically investigate intersections between chronic and infectious diseases such as HIV/AIDS, depression, substance use, and diabetes within environments of structural disadvantage such as poverty, apartheid, racism.
The concept of syndemics was originally introduced by medical anthropologist Merrill Singer, who conducted ethnographic research in the 1990s. At this time, Singer used the concept of a syndemic to describe the interplay between the social, economic, and biological factors that contribute to the clustering and interaction of substance use, violence, and HIV/AIDS among urban Puerto Rican communities in northeastern United States: the substance abuse, violence, and HIV/AIDS (SAVA) syndemic (Singer, 1996).
The construct of violence has been central to the SAVA syndemic since its inception (Singer, 1996). Indeed, Singer noted that, “while violence was not a core variable in our initial design, the frequency of violence and its painful impact on the lives of our study participants has become increasingly apparent...violence must be a central focus of prevention research on drug use and AIDS” (Singer, 1996). Community-level violence (linked to criminal activity) and various forms of gender-based violence (GBV) (such as assaults against sex workers, sexual violence perpetrated by strangers, and intimate partner violence (IPV)) were featured in Singer’s original ethnographic SAVA syndemic research (Singer, 1996).
Building on Singer’s original consideration of violence within syndemics, GBV can be conceptualized as a syndemogenic exposure, meaning it frequently interacts with other major contributors of death and disability to produce syndemic clustering and interactions (Bulled & Singer, 2024; Vahedi et al., 2021, 2025). A small but growing number of research conducted in LMIC has tested and expanded syndemics that integrate GBV (Chakrapani et al., 2022; Hatcher et al., 2014, 2022; Logie et al., 2024; Mootz et al., 2018; Okafor et al., 2018; Sileo et al., 2022; Tomita et al., 2022; Vahedi et al., 2025). Quantitative approaches to investigating GBV syndemics in LMIC represent the dominant empirical approach adopted by investigators (Vahedi et al., 2025).
Quantitative methods are beneficial for understanding the population prevalence of syndemic clustering and for testing statistical interactions and mediation pathways involving multiple epidemics in LMIC (Vahedi et al., 2025). For example, using an HIV surveillance data, Chakrapani, Lakshmi, et al. (2019) reported that 3% of Indian men who have sex with men are concurrently exposed to violence (forced sex and/or physical abuse in the past year), frequent alcohol use in the past week, and any injection/non-injection drug use in the past year (Chakrapani, Lakshmi, et al., 2019). This concurrent triple exposure magnified past-month inconsistent condom use by 14%, above and beyond single and double exposure (Chakrapani, Lakshmi, et al., 2019). Other studies report similar syndemic dynamics between GBV, substance use, and depression, relative to outcomes such as condom use, HIV treatment adherence, and HIV positivity (Alvardo et al., 2020; Chakrapani et al., 2017, 2022; Stoicescu ert al., 2019; Kiene et al., 2017; Sileo et al., 2022; Tomori et al., 2018). However, quantitative analyses sometimes lack an intentional integration of physical and social aspects of the local context (Gizamba et al., 2023).
Qualitative and open-ended explorations of local context are important given the difficulty in conceptualizing, measuring, and isolating the contextual elements that lead to syndemics. Qualitative methods are beneficial for deeply investigating local perceptions, power structures, and lived experiences related to gender-based violence. For example, by interviewing Brazilian women, Hall and Evans (2020) qualitatively examined intimate partner violence alongside co-occurring social conditions, without centering the analysis on a biological health outcome (Hall & Evans, 2020). The analysis situated intimate partner violence within a context of previous exposure to adverse childhood experiences, community violence, financial dependence on abusers, and gender oppression (Hall & Evans, 2020). Further, Hatcher’s et al. (2014) interviews with rural South African men analyzed unhealthy masculinity norms that connect manhood to inequitable decision-making authority, violence, and sexual risk taking. In doing so, the analysis extended the SAVA syndemic by situating the confluence of men’s intimate partner violence, alcohol use, and HIV positivity within the context of inequitable gender norms (Hatcher et al., 2014). Yet, contextual analysis drawn from qualitative investigations with limited sample sizes are critiqued by quantitatively oriented scholars for not being sufficiently generalizable at the population level to inform action (Leung, 2015).
Review of Mixed Methods Approaches to Investigating GBV Syndemics in LMIC
The evidence base reflects the absence of a framework that leverages and integrates the distinct strengths of quantitative and qualitative methods. Mixed methods research investigating GBV syndemics in LMIC is emerging (Duby et al., 2022; Gonzalez-Nieto et al., 2023; Kohrt & Carruth, 2022; Logie et al., 2024) but remains rare. Existing mixed methods studies could benefit from clarifying the value add of integrating research methods vis-à-vis syndemic theory’s central tenets: (1) epidemic clustering, (2) interactions between epidemics, and (3) magnification of a population health burden due to inequitable sociopolitical structures.
One recently published mixed methods syndemic study, on socio economic and mental health stressors among young South African women during the COVID-19 pandemic, concurrently collected cross-sectional survey data and in-depth interviews (Duby et al., 2022). Complementary quotes and descriptive statistics (frequencies) were presented as results (Duby et al., 2022). For instance, the frequency and severity of stressors like physical, emotional, and sexual abuse during pandemic related lockdowns were presented alongside personal accounts of strained family relationships and domestic violence. However, the quantitative analysis did not test for syndemic patterns involving interactions or pathways (Duby et al., 2022). Gonzalez-Neito et al. (2023) applied syndemic theory to study a population of women who inject drugs at the US–Mexico border, using cross-sectional quantitative data and in-depth interviews (Gonzalez-Nieto et al., 2023). The authors analyzed and presented the qualitative and quantitative data sources separately (Gonzalez-Nieto et al., 2023). Descriptive statistics that were complementary to the in-depth interviews were included in the findings (Gonzalez-Nieto et al., 2023). In such mixed methods studies, it is not clear how the qualitative and quantitative data sources build on one another and how, through integration, the methods deepen the understanding of syndemic dynamics involving context, clustering, and interaction.
Further, Logie et al., 2024 conducted a study among youth refugees from the Bidi Bidi refugee settlement in Uganda wherein a qualitative phase was followed by a quantitative phase (Logie et al., 2024). Qualitative themes derived from in-depth individual interviews and focus groups discussions with refugee youth, elders, and service providers represented the nexus between (1) poverty and GBV, (2) poverty and transactional sex, and (3) substance use and GBV (Logie et al., 2024). During the second stage, researchers implemented a cross-sectional survey among 115 refugee youth that quantified the constructs of poverty, GBV, and condom engagement motivation (Logie et al., 2024). Stratified quantitative analyses revealed that the relationship between GBV exposure and reduced condom engagement emerged under the condition of poverty (Logie et al., 2024). Logie et al.’s (2024) research presents separate qualitative and quantitative findings that are relevant for GBV syndemics in LMIC. Yet, it is not clear to what degree the qualitative insights intentionally informed second quantitative phase and how the integration of the separate phases, in a distinct temporal order, advanced the theoretical testing and application of GBV syndemics.
Current Limitations in Mixed Methods Research
Syndemic informed global health action requires a robust evidence base. Empirically engaging with syndemic theory necessitates the use of interdisciplinary approaches, involving distinct ontologies, epistemologies, methods, and analytical approaches, that bring inferences closer to causality. Although syndemic theory has been recognized as a promising and important strategy for recognizing systemic causes and mechanisms of inequality (Mendenhall, 2017, p. 890), empirical research falls short of pragmatically testing all theoretical features in a manner that compels the redesign of global health programs and policies.
Research Aim
Mixed methods investigators face distinct challenge engaging with multiple dualities: top-down versus bottom-up, emic versus etic, epidemiological versus anthropological, generalizable versus contextualizable (Pirrone et al., 2021). This research aims to develop an integrated research framework to provide guidance on robustly and intentionally integrating qualitative and quantitative approaches in syndemic science. The framework has implications for how global health researchers measure sensitive and hidden epidemics, such as gender-based violence, and integrate such epidemics with other major causes of morbidity and mortality (including chronic and infectious diseases) in resource limited contexts.
Organization and Structure
The next section further explains the theoretical tenets of syndemic theory. Following a detailed theoretical explanation, qualitative and quantitative approaches to investigating the theoretical tenets of syndemic theory are then presented in the results, followed by a thematic synthesis of expert opinions concerning mixed methods syndemic research in LMICs. The novel mixed methods framework, detailing the strategic and intentional integration of qualitative and quantitative methods, is presented visually in the discussion, with implications for future research.
Theory
As we have highlighted in similar publications (Meinhart et al., 2021; Stark et al., 2020; Vahedi et al., 2021, 2025, 2026), syndemic theory is a useful framework for situating GBV alongside other health burdens. The concept of a “syndemic,” derived from the combination of “synergy” and “epidemic,” underscores the idea that adverse health conditions co-occur and interact in ways that perpetuate health inequities, particularly in settings marked by structural disadvantage (Singer et al., 2017). The term was introduced by medical anthropologist Merrill Singer in the 1990s as a means of capturing how multiple health problems are simultaneously shaped and intensified by social, economic, and political inequalities (Singer, 1996). Central to syndemic theory is the recognition that large-scale economic, environmental, and political forces foster the emergence of interrelated epidemics, which interact through biological, behavioral, and social mechanisms to amplify the overall population health burden, often leading to health inequities (Outram et al., 2024; Singer et al., 2017).
Since syndemic theory explicitly attends to these biosocial interactions, syndemics differ from concepts such as comorbidity and multimorbidity, which describe the coexistence of multiple conditions without necessarily accounting for their interactive effects or related mechanisms of interactions (Singer et al., 2017). Rather than being limited to a fixed set of variables, syndemic theory is intentionally flexible and can be applied across diverse contexts and health issues, provided that three core criteria are satisfied: (i) multiple diseases, health conditions, or epidemics co-occur within a defined population; (ii) interactions among these conditions, whether biological, psychological, behavioral, or social, produce an intensified population-level health burden; and (iii) political, social and contextual forces facilitate both the clustering of conditions and their interaction (Outram et al., 2024; Mendenhall et al., 2021).
Applying a syndemic lens to GBV allows for empirical examination of how particular constellations of violence, health adversities, and sociopolitical environments combine to generate disproportionate and costly harms (Vahedi et al., 2025). Identifying these synergistic mechanisms can help clarify how GBV contributes to compounded health inequities and can reveal critical public health intervention points, such as modifiable contextual factors, mediators, or exposures (Vahedi et al., 2025). Targeting these leverage points can inform the design of more efficient and contextually appropriate interventions and policies, particularly in resource-constrained settings, including low- and middle-income countries (LMICs), where disrupting harmful syndemic interactions may yield substantial public health gains (Vahedi et al., 2025).
Methods
Though there is no formal definition of a methodological framework that experts across disciplines agree on, McMeekin et al. (2020) developed a three-step process to develop a methodological framework based on a broad scoping review of existing methodological frameworks. The three-step approach for developing methodological frameworks (McMeekin et al., 2020), was used to develop the mixed methods framework: (1) Identify evidence to inform the methodological framework, (2) Conduct data extraction and synthesis to develop the methodological framework, and (3) Evaluate and/or refine the methodological framework by consulting with experts. This step process is a robust approach for methodological framework development as it is based on a consensus of reported approaches.
Part 1: Identifying the Evidence
The first phase involved conducting a mixed methods methodological review of empirical GBV syndemics research conducted in LMIC (as identified by the World Bank) (World Bank, n.d.). Both qualitative and quantitative articles were included. A systematic search of the qualitative and quantitative peer-reviewed literature was first conducted on May 16th, 2023, and updated on February 26th, 2024. Three researchers conducted the scoping review based on Preferred Reporting Items for Scoping Reviews (Page et al., 2021). This scoping review steps from a related review on quantitative methods used to test syndemic theories (Vahedi et al., 2025). Here, we deepen the previous quantiative review by considering qualitaitve methods for testing syndemic theory.
The following research question guided the methodological review: What quantitative and qualitative study designs and analyses have been adopted to test GBV syndemics in LMIC? The present research compares the strengths and limitations of the qualitative and quantitative evidence base for the purpose of developing a mixed methods framework.
In collaboration with a librarian, we developed a search strategy (see Supplemental Appendix A), that included the domains of (1) syndemic theory and (2) GBV. For each domain, we located relevant keywords and index-specific terms (ex. Medical Subject Headings). The lead researcher reviewed existing reviews concerning syndemic theory to identify search terms and databases (Singer et al., 2020; Tsai and Burns., 2015). The search strategy was implemented in several databases: Gender Watch (ProQuest Interphase), Medline (Ovid interphase), Anthropology Plus (EBSCO interphase), Global Health (Ovid interphase), Anthro Source, Web of Science Core Collection (1990-), Scopus, and PsychInfo (Ovid Interphase). We included English peer-reviewed empirical research that employed qualitative or quantitative methods to apply or test syndemic theories that incorporated GBV in LMIC.
Similar to our review on quantitative methods (Vahedi et al., 2025), Covidence was used as a screening and data extraction tool and eliminated duplicates prior to screening (Covidence, 2023). Prior to screening, the co-researchers were trained on systematic review methods. Selection of articles occurred in two sequential stages (with two screeners assigned per article): (1) screening of titles and abstracts and (2) full text review. Articles that met the inclusion criteria after full text review were included in the methodological review and subsequently extracted and synthesized. Discordant votes during title/abstract and full text screening were resolved during consensus meetings.
Part 2: Synthesis
The included articles were charted and synthesized separately based on research approach (qualitative or quantitative). Information was charted using standardized extraction forms (separate for qualitative and quantitative designs) that were pilot tested using a sub-sample of articles (5 quantitative and 5 qualitative articles). The extraction forms were then refined for greater ease of use and all articles were charted using the same standardized form. Several domains were included in the standardized data extraction form which are summarized in the Supplemental Appendix B. For qualitative studies, excerpts pertaining to methodological details/approaches were also extracted using a codebook of a priori codes that corresponded to the three tenets of syndemic theory (clustering, interaction, and context).
Following data charting/extraction, the lead author developed an inventory of methods employed. Further, the strength and limitations of the qualitative and quantitative methodological approaches were compared relative to the theoretical tenets of clustering, interaction, and context. Creswell and Plano Clark’s mixed methods study designs were used to organize and combine the qualitative and quantitative research approaches that appeared in the syndemics evidence base (Creswell & Plano Clark, 2018).
Part 3: Refinement Using Expert Opinions
The Delphi technique was employed to obtain a consensus of syndemic experts’ perspectives regarding the utility and application of mixed methods research designs as well as current gaps and best practices (Okoli & Pawlowski, 2004). Experts’ opinions were used to (1) ensure the mixed methods framework addressed the needs of its target users and (2) refine practical research applications of the framework. The Delphi technique uses a series of cross-sectional surveys to gather the perspectives of an expert group, with the goal of reaching consensus on a complex problem or objective (Okoli & Pawlowski, 2004). Experts are asked to share their opinions on a particular topic/issue. Subsequent survey rounds are based on the findings from previous rounds; experts’ previous opinions are contrasted against those of the group (Okoli & Pawlowski, 2004).
Participants
Experts were recruited using purposeful sampling. All recruited experts had to have at least one first-authored peer-review publication whose primary focus was testing or applying GBV syndemics in LMIC. A contact list of 60 experts was created based on all corresponding and/or first authors from the sources included in the methodological review. To participate in the study, the researchers/scholars were contacted using publicly available emails. The recruitment email included an invitation to participate in the study, a description of the study design, the first survey round, and an information sheet. The Washington University Institutional Review Board considered this study exempt from ethical review.
Procedure
The Delphi design with two successive rounds was employed to obtain consensus of expert views/experiences concerning GBV syndemics research in LMIC (Okoli & Pawlowski, 2004). The Delphi method structures communication by allowing experts to express and refine their views while maintaining anonymity. In this study, the Delphi technique involved two sequential cross-sectional surveys. Although additional rounds would likely result in greater consensus, the two-round design mitigated attrition. The survey was administered using Qualtrics.
Round 1
Experts were invited to answer demographic information, followed by the main survey questions. The first round elicited open-ended responses using text boxes and the second round involved rating the relative importance of responses from the first round to build consensus. Open text responses from the first round focused on potential applications of mixed methods designs, methodological/analytical gaps, good research/analytical design practices, theoretical tenets that are the most difficult to demonstrate empirically and why, and challenges encountered (refer to Appendix). Responses of any length were accepted.
When Round 1 data collection was complete, responses from each open-ended question were collected and organized using inductive thematic analysis (Williamson, 2022). In our case (using open-ended responses) this data-driven analytical approach consisted of reading the open-ended responses and identifying commonalities that were then grouped into codes and later themes. Regarding theme creation, the lead author analyzed the coded statements in relation to one another and noted where statements could be conceptually grouped into themes that captured the main essence of linked statements. For each open-ended question, all statements were organized their respective themes. This approach enabled the efficient identification of overlapping viewpoints. Following this analysis, the lead author reduced the responses into a comprehensive list of unique statements. If multiple experts shared the same opinion or view, one statement was created to capture to idea using the phrasing of the expert who was most clear. All unique statements for each open-ended question were reviewed a second time to ensure they were exhaustive of all unique views/opinions, to maximize clarity of wording, and remove any redundancies.
Round 2
Experts were invited to participate in the second round, regardless of whether they responded to the first round. The master statement list from Round 1 was converted into the Round 2 survey. Experts were asked to consider the statements and rate their level of importance using a 5-point Likert scale. Depending on the statement type, experts were asked to rate (i) the level of importance of promising strategies for improving future research (very important, somewhat important, neutral, not that important, not important) and (ii) the extent to which gaps/challenges hinder research progress (strongly hinders progress, hinders progress, neutral, facilitates progress, strongly facilitates progress). Experts were also provided with an optional open text box to elaborate on their rating.
Final Analysis
Two descriptive statistics were used to compute degree of consensus (Bennouna et al., 2017). First, clear consensus was defined as at least 90% of participants agreeing or strongly agreeing with a statement (Bennouna et al., 2017). Statements that 80% and 89% of participants agreed or strongly agreed with were deemed as approaching consensus (Bennouna et al., 2017). Second, among all agreeing experts (strongly agree or agree), we also calculated the proportion of experts who strongly agreed (the agreement intensity). An agreement intensity above 0.50 indicates that experts were more likely to strongly endorse a statement than they were to moderately agree with it.
Results
We present the results according to the McMeekin et al. (2020) three-step process for developing a methodological framework. First, we outline results from the evidence identification and synthesis phases. Second, we outline results from the expert refinement/consultation phase.
Part 1: Evidence Identification and Synthesis
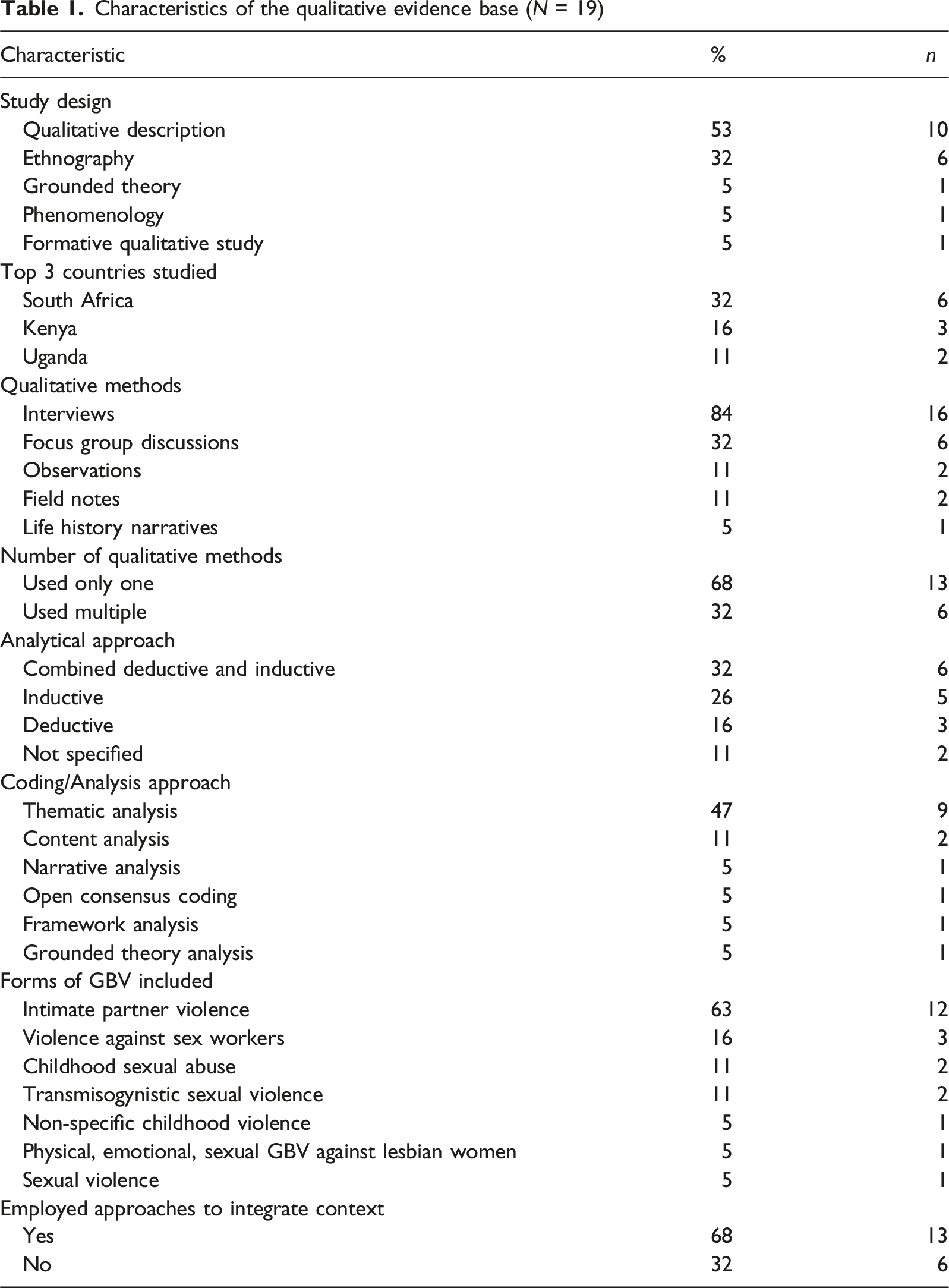
Characteristics of the qualitative evidence base (N = 19)
Characteristics of the quantitative evidence base (N = 45)
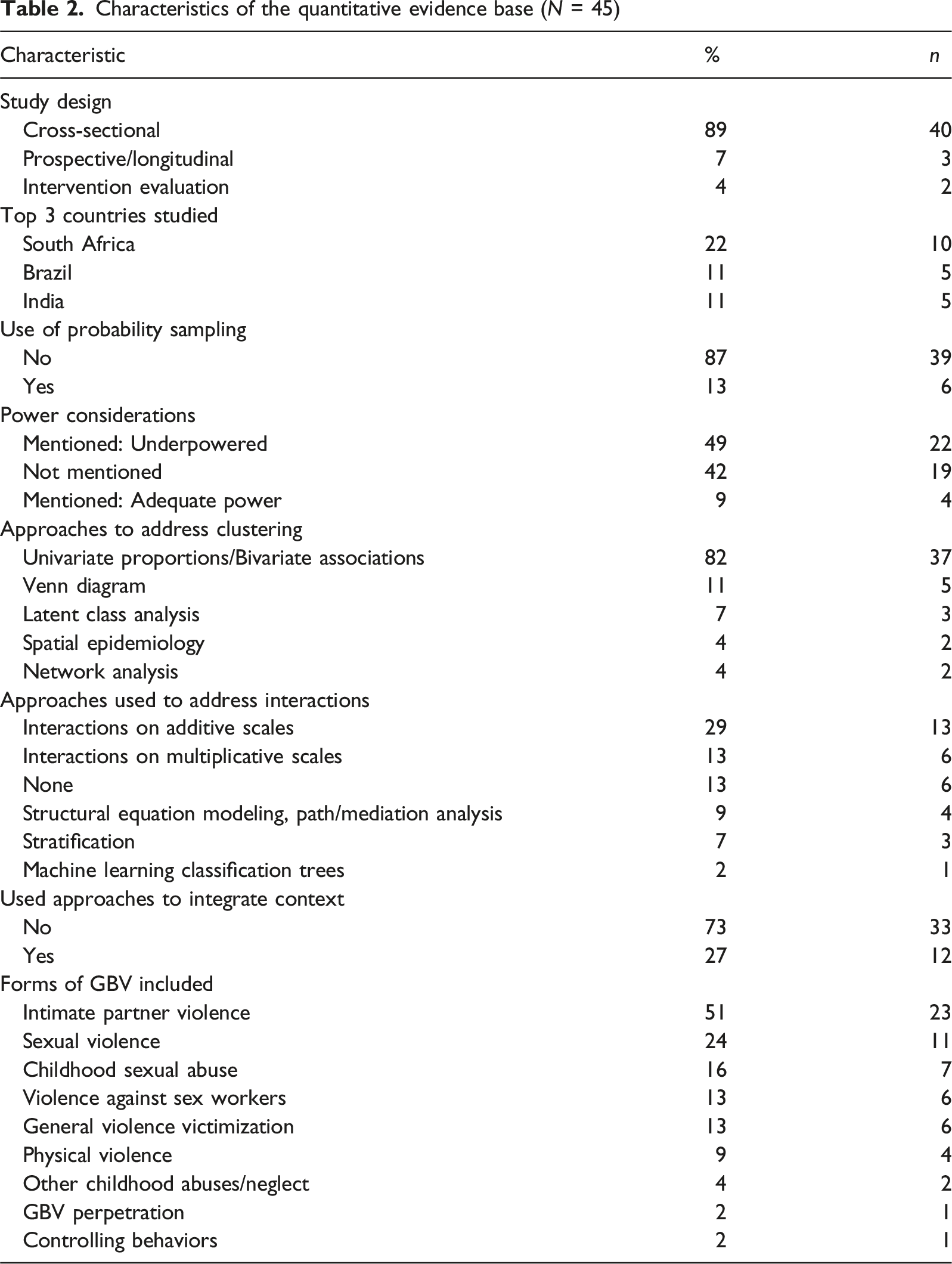
Important for the development of a mixed methods framework is a synthesis of how each evidence base (quantitative and qualitative) approached the three theoretical tenets. For this reason, we focus the presentation of findings from the methodological review on how and to what degree the quantitative and qualitative evidence base tested the tenets of syndemic theory.
Theoretical Tenets 1 & 2: Epidemics Cluster and Interact to Magnify the Population Health Burdens
Quantitative Evidence Base
A detailed analysis of quantiative syndemic methods used to test clustering and interaction is given in Vahedi et al., (2025); here we provide an overview of quantiative approaches in contrast to qualitative methods. Different statistical approaches were used to test for clustering and interaction in the quantitative evidence base. For example, approaches to quantitatively test for clustering were descriptive in nature and involved reporting the degree to which the sample was exposed to each syndemic condition (i.e., using frequencies or proportions), the syndemic score count (i.e., the number of syndemic exposures a sample is exposed to), and denoting all unique permutations of syndemic exposures in the sample (Vahedi et al., 2025). Some authors illustrated syndemic clustering using Venn Diagrams (Vahedi et al., 2025). Other approaches that were leveraged to illustrate clustering/co-occurrence included geospatial analyses (Sileo et al., 2022; Tomita et al., 2022), network analysis (Lee et al., 2023; Choi et al., 2019), and latent class analysis (Brown et al., 2023; Chakrapani, Willie, et al., 2019; MacLin et al., 2023), Clustering provides a measure for the burden of co-occurring epidemics. Thus, the utility of clustering analysis for global health action is maximized when using probability samples and minimized for nonprobability sampling methods, like convenience sampling.
Syndemic interaction analysis is distinguished from clustering in the quantitative evidence base. Syndemic interactions were analyzed using additive and multiplicative interactions involving fully saturated regression models, structural equation modeling and path analysis, stratification, and machine learning. The goal with such approaches was to demonstrate that the probability of an adverse health outcome was greater when the epidemics occur simultaneously, compared to singularity. In other words, the magnification of harm is greater than the sum of its parts (Vahedi et al., 2025). For this reason, testing for statistical interactions on additive scales provides the clearest evidence for syndemic interactions. However, structural equation models with path analysis and mediation models can illustrate how epidemics influence one another, analogous to a “chain of risks” with singular or bidirectional relationships.
Qualitative Evidence Base
Distinguishing between the theoretical tenet of clustering and interaction was more difficult in the qualitative evidence base, as these were presented as interrelated. It was common for qualitative studies to purposively recruit participants based on the presence of one or more syndemic conditions (e.g., having been diagnosed with diabetes, screening positive for IPV, and binge drinking, orphans, HIV positive, etc.). Thus, it is less appropriate to assess the degree to which epidemics cluster among participants using such purposively selected data. Rather, in such cases qualitative data sources can be used to understand how persons experiencing syndemic clustering understand interrelated epidemics.
For example, Duby et al. emphasized contextual specificity in South Africa by including the original language/phrases used by adolescent girls/young women to describe their mental health (Duby et al., 2021). Mendenhall and Norris (2015) noted that South African women communicated multilayered syndemic suffering involving HIV/AIDS and chronic diseases by invoking accounts of everyday/ordinary suffering that were separate from biomedical disease nomenclature. Qualitative data may also examine the life histories of persons living multiple epidemics to understand trajectories leading to syndemic clustering. Studies using key informant interviews are suited to inductively investigate syndemic clustering by conducting a content analysis of which epidemics were most often described in combination, while also considering how participants interrelations and interactions between epidemics. Qualitative research may strike a balance between including probes that provide participants opportunities to fully develop their perceptions, without influencing participants’ schemas of specific combinations of epidemics or ways they interact.
Theoretical Tenet 3: Inequitable Sociopolitical Contexts Promote Clustering and Interactions
Quantitative Evidence Base
Only 27% of the quantitative evidence base analyzed how the sociopolitical environment affected the clustering and interaction of epidemics, compared to 68% of the qualitative evidence base. Quantitative approaches used to integrate context include (i) spatial epidemiology to identify geographical hotspots of epidemic clustering, (ii) purposively recruiting participants from geographical regions with different armed conflict exposure, (iii) positioning contextual variables (gender inequitable views, HIV stigma, and armed conflict exposure) as exogenous variables in structural equation modeling, (iv) integrating contextual variables (e.g., social support, resilience, education, and income) into quantitative modeling to test for moderation or changes in main effects, and (v) latent class analysis to develop typologies of access to resources/assets. Only the two studies that used spatial methods included group/aggregate level measures of context. In all other studies, context was measured at the individual level using survey questions or tools.
Qualitative Evidence Base
The qualitative evidence base engaged more deeply with local LMIC contexts through open-ended approaches such as ethnographic field work, inductive thematic analysis, grounded theory, and life history narratives. In doing so, the qualitative research revealed latent aspects of the local sociopolitical environment that affect syndemic dynamics. For example, investigators adopted a deductive approach wherein a priori syndemic constructs (substance use, GBV, HIV/AIDS) were used as codes and were combined with other theory-driven codes to capture contextual complexity (e.g., codes pertaining to the socioecological model or social determinants of health framework) (Hall & Evans, 2020; Kibicho & Campbell, 2019).
The qualitative evidence base extended beyond identifying a contextual aspect to holistically describing the economic and power systems that create sociopolitical inequities and lead to syndemic clustering and interaction. Rich qualitative data sources were beneficial in developing a causal story detailing the relationship between context, clustering, and interaction, often incorporating multiple ecological levels (systems, institutions, and individuals). Qualitative data from in-depth interviews, observations, and field notes enabled investigators to flexibly develop mechanisms through which macrolevel inequities adversely affect meso-level institutions, norms, and industries and microlevel families and indices. Eight articles (42%) visually depicted the causal syndemic conceptual model that emerged from the qualitative data using a figure. Most figures (n = 7) included considerations for clustering, interaction, and context. Articulating the processes and pathways through which excess population disease burdens are produced in a particular place and time is a cornerstone of syndemic theory; qualitative methods can develop and refine such conceptual models in a more flexible manner than quantitative methods, which may be limited by temporality, the availability of measurement tools, or computational efficiency. As Horan et al. described in their study of the intersecting factors leading to poor maternal and infant health outcomes in Puerto Rico: While sociopolitical elements are commonly integrated into syndemic models, factors like colonization or globalization are typically considered as components of a cluster of interactions, rather than as the foundation, the precondition, from which the syndemic emerges or manifests. (Horan & Holly, 2021, p. 10).
Mendenhall’s in-depth interviews with women living with diabetes in Soweto, South Africa linked the physiological and cognitive manifestations of everyday stress and suffering to the legacies of apartheid’s structural violence (Mendenhall, 2014; Mendenhall & Norris, 2015). Disproportionate AIDS mortality in Soweto, the restructuring of families, food insecurity, depression, and interpersonal violence, were common stressors and inhibited women’s health promoting behaviors related to diabetes management. Further, Montesi conducted 1 year of fieldwork in Southern Mexico to understand local drinking patterns and their relationship with diabetes (e.g., abusive drinking and diabetes syndemic) (Montesi & Laura., 2018). This deep field engagement illuminated complex linkages between larger economic systems (colonialism and capitalism) and intensification of alcohol production, exchange, and consumption in Mexico. These linkages negatively impacted men and boys, resulting in intensified alcohol use and financial precarity. Women’s economic dependence on husbands who engage in heavy episodic drinking and intergenerational histories of intimate partner and domestic emerged when conducting interviews with diabetic women (Montesi & Laura., 2018). The feminization of poverty emerged as an important element of the sociopolitical context (Backe et al., 2022; Hall & Evans, 2020; Joshi et al., 2021; Shah et al., 2023; Winchester, 2015). The widening poverty gap between men and women combines both patriarchal power systems and capitalism. Poverty feminization shapes women and girls’ financial dependency on men, which can in turn alters experiences violence as well as communicable and noncommunicable disease.
Synthesis Summary and Conclusions
To date, empirical quantitative and qualitative approaches to testing syndemic clustering, interaction, and context pose distinct benefits and limitations. As demonstrated by the studies from the methodological review, the strategic temporal separation of qualitative and quantitative phases can draw on the advantages of each empirical approach relative to syndemic theory. For this reason, the convergent mixed methods design wherein qualitative and quantitative sources of data are collected and analyzed in tandem is not recommended. Rather, an approach wherein qualitative data addresses the shortcomings of initial quantitative insights and qualitative data addresses the shortcomings of initial quantitative insights is recommended. The (1) exploratory sequential and (2) explanatory sequential mixed methods designs are better suited to holistically test syndemic theory because they separate the quantitative and qualitative phases temporally, using insights from the first phase to guide the second phase (Creswell & Plano Clark, 2018).
Part 2: Expert Consultation
Out of 60 invited experts, 21 syndemic experts completed at least one round of the Delphi surveys (response rate of 35%). Nineteen respondents participated in Round 1 (31% response rate), resulting in 74 unique statements. Eleven respondents participated in Round 2 (18% response rate). In Round 2, 47% of statements reached clear consensus and 25% approached consensus. Additionally, 39% of statements reached clear consensus with agreement intensity at or above 0.50. All statements with their level of consensus and agreement intensity are presented the Supplemental Appendix D.
Potential Uses of the Exploratory Sequential Mixed Methods Design
Experts reached consensus on several applications of the exploratory sequential mixed methods design, which begins with a qualitative phase followed by a quantitative phase. One statement that reached clear consensus noted an important value add of the exploratory mixed methods design: “the second quantitative phase allows researchers to move beyond individual experiences and assess broader population patterns/trends” (consensus 100, agreement intensity 0.60).
Experts also reached consensus on using the exploratory mixed methods design to first develop locally informed syndemic theories that are quantitatively tested in the second phase. This application was reflected in different statements that reached consensus: (1) “If the first qualitative phase is used to develop a theoretical model of the syndemic, the second quantitative phase can be used to test this theoretical model” (consensus 100, agreement intensity 0.90), (2) “If the qualitative phase investigated whether participants perceived they were affected by syndemics, the second quantitative phase could assess the prevalence of multiple diseases, severity of disease, and the trajectory of the disease” (consensus 100, agreement intensity 0.80), (3) “The qualitative data in the first phase is useful in informing the specification of the quantitative models” (consensus 90, intensity agreement 0.78), and (4) “The second quantitative phase can be used to measure/quantify constructs that originated from the qualitative themes” (consensus 100, intensity agreement 0.90). A second application of the exploratory sequential design was measurement tool development: “the second quantitative phase can develop local measurement instruments for syndemic measures” (consensus 100, agreement intensity 0.70).
Potential Uses of the Explanatory Sequential Mixed Methods Design
Experts reached consensus on several applications of the explanatory sequential mixed methods design, which begins with a quantitative phase followed by a qualitative phase. This design begins with quantitatively testing syndemic theory and collecting follow-up qualitative data in the LMIC context. The second qualitative phase can extend and deepen the initial qualitative results in several ways. Stated simply, in the explanatory sequential design “the second qualitative phase can contextualize the results from the quantitative models” (consensus 100, agreement intensity 0.70).
Experts reached consensus that “by understanding lived experiences and the cultural context in the second qualitative phase, researchers can develop intervention strategies that prevent/mitigate the GBV syndemic” (consensus 100, agreement intensity 0.90). Integrating local perspectives can test the interpretations and conclusions drawn from the quantitative data: (1) “In the second qualitative phase, researchers can return to the community and conduct focus group discussions where participants discuss, critique, and explain the quantitative syndemic findings” (consensus 90%, agreement intensity 0.78) and (2) “In the second qualitative phase, researchers can conduct ethnographic research or in-depth interviews to examine whether the quantitative findings align with social experiences” (consensus 90%, agreement intensity 0.56). The second qualitative phase also presents an opportunity to further investigate new hypotheses that emerged from the quantitative analysis (Statement Q6_4, consensus 90%, intensity agreement 0.67) and further explain any unexpected findings (Statement Q6_7, consensus 90%, intensity agreement 0.67).
Research Gaps
Four statements reached clear consensus with agreement intensity and three statements were approaching consensus. Key methodological and analytical gaps pertained to the themes of (1) funding, (2) quantitative approaches, (3) qualitative approaches, (4) measurement and (5) causality.
Funding
Importantly, “limited funding for GBV syndemics research in LMIC” emerged as an important gap (100% consensus, 0.73 agreement intensity). The importance of designated funding for GBV syndemics research was further raised by two experts in the optional open text box, noting that with increased funding, the methodological/analytical gaps would improve. In line with funding, experts also agreed that it is challenging to “practically articulating syndemic findings to policymakers and program designers (who want easy solutions)” (consensus 100%, agreement intensity 0.60).
Gaps for Quantitative and Qualitative Approaches
Beyond funding, experts noted that for quantitative research, “It is difficult to disentangle the comorbid conditions, adverse interactions, and advanced disease progression in quantitative modeling” (91% agreement, 0.70 intensity agreement) and that there are a “lack of prospective studies with larger samples” (100% agreement, 0.64 agreement intensity). “Disagreement in the field and lack of guidelines regarding best analytical practices for the quantitative modeling of syndemics” approached consensus (82% consensus, 0.56 agreement intensity). Related to qualitative research, experts agreed there is a “lack of qualitative research investigating syndemic mechanisms/pathways and their population effects” (91% consensus, 0.50 agreement).
Gaps in Measurement
Two measurement gaps approached consensus. First, experts noted there is “limited consideration of bidirectional violence perpetrated by women against men (among couples)” (consensus 82%, agreement intensity 0.44) and that “due to measurement limitations (stigma, underreporting, and lack of standardized measures), it is difficult to assess the prevalence of GBV and its true co-occurrence with other epidemics/health conditions” (consensus 82%, agreement intensity 0.22).
Gaps in Causal Inference
Experts noted distinct challenges in the ability to elucidate causal syndemic effects. For example, experts reached consensus that (1) “it is often difficult to explain causality when testing interactions. For example, are the adverse disease interactions occurring because of the syndemic? Is the magnified health burden due to the syndemic or because of another factor?” (consensus 100%, agreement intensity 0.60) and (2) “biological mechanisms and the bidirectional relationships are challenging to demonstrate empirically, and greater theoretical/conceptual development is needed” (consensus 90%, agreement intensity 0.56). Further, causality involving GBV syndemic pathways was noted as a challenge: “GBV can be defined and experienced in different ways and thus causes harm through different pathways, which are difficult to concurrently analyze” (consensus 100%, agreement intensity 0.60).
Good Research and Design Practices
Experts generally endorsed all statements of good research/design practices, with the exception that “best quantitative approaches to analyzing syndemic interactions already exist in the literature and are outlined by Tsai and Burns (2015) and Tsai and Venkataramani (2016)” (consensus 70%, agreement intensity 0.43). However, experts agreed that “standardized approaches to measuring and analyzing syndemics need to be developed” (80% agreement, 0.22 agreement intensity). One way to expand the application of quantitative methods is to use “structural equation modeling, mediation analysis, or path analysis to quantitatively assess syndemic pathways” (consensus 90%, agreement intensity 0.22). This view reflects a growing interest and need to build and expand upon using statistical interaction to test syndemic theory, particularly when understanding how, why, and under what conditions syndemics occur. Notably, experts endorsed the need to “conduct mixed methods research, combining quantitative and qualitative methods” (100% agreement, 0.80 agreement intensity). Syndemic researchers can draw on a variety of recommended qualitative and quantitative research and design practices to improve the GBV syndemics evidence base in LMIC. Good research and design practices pertain to the themes of (1) measurement, (2) local engagement, and (3) integration of context.
Measurement
Good measurement practices involve “using ethnographic research to create new and local GBV measurement tools based on context, culture, beliefs, experiences, idioms, and language” (90% agreement, 0.67 agreement intensity) as well as “adapting and validating existing measurement tools for specific contexts” (consensus 100%, agreement intensity 0.40). Experts also agreed that measuring GBV in LMIC introduces complexity in GBV syndemics research: “GBV is a multidimensional concept that encompasses multiple forms of violence with varying severities; researchers should use formal assessments that capture this complexity” (consensus 100%, agreement intensity 60%). Experts concurred (although with less relative intensity and consensus) that “the field should consider whether GBV should include and be sensitive towards male victimization” (consensus 80%, intensity agreement 0.50). Last, there was approaching consensus for “improving the conceptualization and measurement of all components of a syndemic, rather than just focus on the comorbid conditions” (consensus 80% agreement intensity 0.63).
Local Engagement
Experts agreed that (1) “Use of community-based participatory research and involving community members in data collection improves cultural sensitivity and ensures that GBV syndemics research addresses local needs” (consensus 100%, agreement intensity 80%), (2) “Researchers should conduct formative qualitative work and ethnographic field research to understand local perspectives of GBV” (consensus 100%, agreement intensity 60%), and (3) “Researchers should engage with local government and community-based organizations to codevelop research designs and capitalize on existing GBV infrastructure” (consensus 100%, agreement intensity 0.50).
Integration of Context
Various statements addressed integration of the LMIC context in GBV syndemics. For example, syndemics researchers could “integrate other theoretical frameworks which explore how broader socioeconomic conditions perpetuate the clustering of conditions in marginalized populations” (consensus 100%, agreement intensity 0.50). Another consideration of local context involved “identifying and measuring social support networks, which may prevent or mitigate GBV syndemics” (consensus 100%, agreement intensity 0.70). Regarding contextual aspects of GBV, “researchers could analyze culturally and socially relevant factors that shape GBV (e.g., local gender ideologies, role expectations, family composition, and gender roles)” (consensus 90%, agreement intensity 0.67). Last, spatial epidemiology had approaching levels of consensus: “Spatial epidemiological approaches using georeferenced spatial data and graphical information systems (GIS) are useful when analyzing GBV syndemics” (consensus 80%, agreement intensity 0.63).
Discussion
Over the past three decades, syndemic science has expanded both in terms of populations and regions studied but also methodological practices. Several published reviews and frameworks have guided the quantitative evidence base and improved research quality (Batchelder & Lounsbury, 2016; Shrestha et al., 2022; Tsai & Venkataramani, 2016; Vahedi et al., 2025). Although there is a growing recognition of the utility in merging qualitative and quantitative approaches in syndemic science (Bulled & Singer, 2024; Himmelgreen et al., 2022; Kohrt & Carruth, 2022; Pirrone et al., 2021) there is less guidance on best practices for the integration of qualitative and quantitative methods. This study integrated a methodological review alongside a Delphi consensus of expert researchers to develop a mixed methods framework for GBV syndemics research in LMIC.
Introducing the New Mixed Methods Framework for GBV Syndemics in LMIC
The framework (presented in Figure 1) addresses syndemic experts’ opinions on gaps in measurement and causal inference and reflects experts’ views on the utility of mixed methods designs. Figure 1 centers the distinct ontological and epistemological positions of quantitative and qualitative research relative to syndemics, GBV, and LMIC. In Supplemental Appendix E, we provide a simplified version of the framework for further application and adaptation. Mixed methods framework for investigating GBV syndemics in LMICs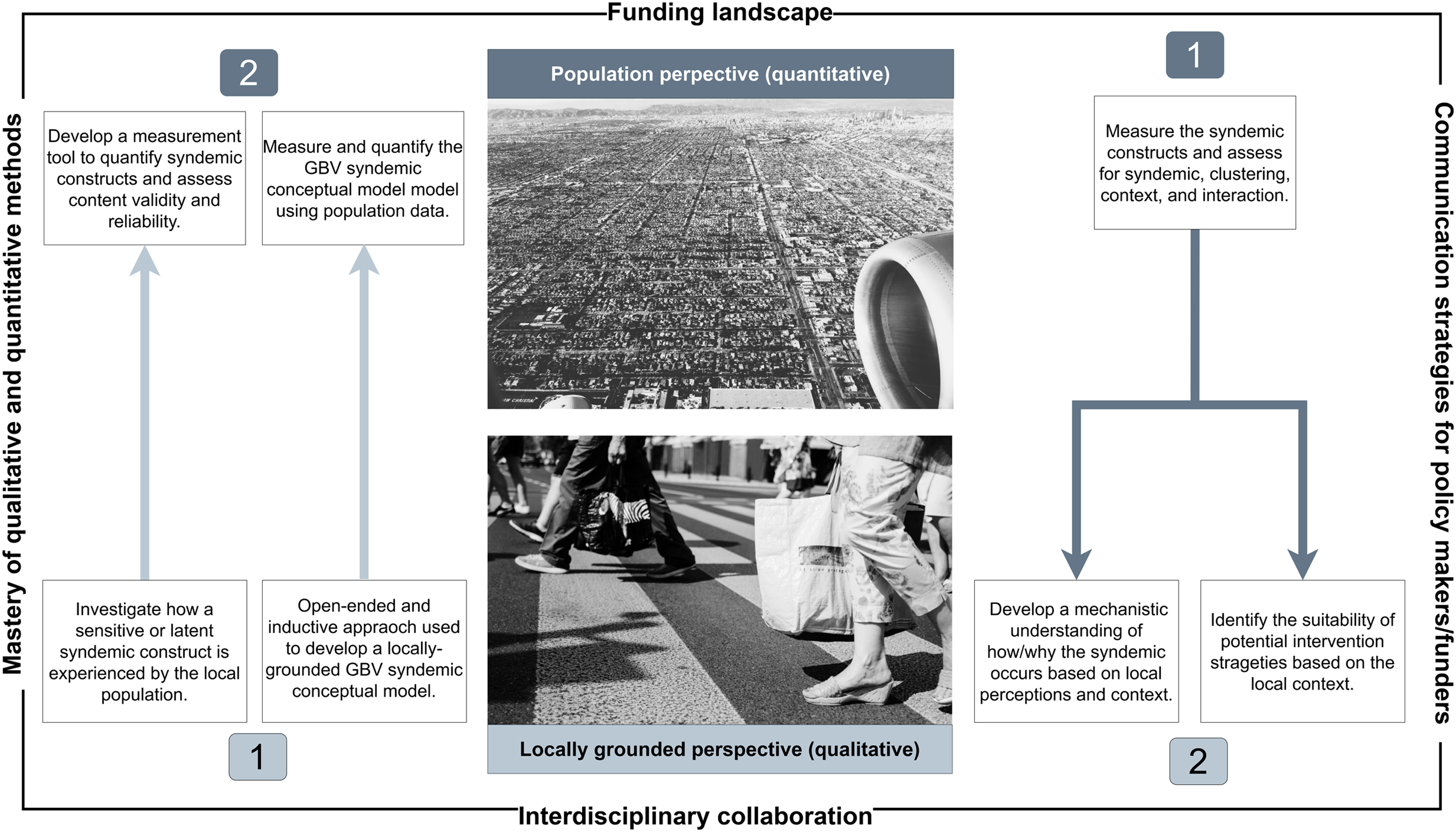
Quantitative methods are depicted at the top using an aerial view of the target population, like gazing from an airplane window after its ascent. This population perspective positions the researcher as an external observer of the syndemic phenomenon at the population level. Using appropriately large probabilistic samples and distinct statistical methods for testing clustering, interaction, and context, the population perspective permits the identification of deductive syndemic patterns (particularly clustering and interaction). The population perspective moves beyond individual experiences to broader population patterns. Important applications of the population perspective include (1) determining the population prevalence of syndemic clustering, (2) identifying clustering hotspots using geospatial methods, (3) quantifying the excess health burden risk due to synergistic interactions, and (4) isolating which causal biosocial pathways explain the most variability in the health burden.
Qualitative methods are depicted at the bottom of Figure 1 using a ground view of a small population segment, like crossing the street with members of the target population. This locally grounded perspective recognizes the researcher’s identity relative to the realities, dynamics, and norms of the LMIC setting. By analyzing the lived experiences of purposively selected individuals, observing the physical places where people interact, and sociopolitical norms that shape behavior, the investigation centers on understanding the physical and social contexts that shape syndemic clustering and interaction and can be sites for intervention. The locally grounded perspective permits the investigation of constructs that are not readily quantifiable or that emerge through a complex process of meaning creation within the norms of the local context. This perspective is open-ended and inductive, allowing salient aspects of the macro-, meso-, and microlevels to guide the investigation. The locally grounded perspective emphasizes that syndemics are not global; syndemic vulnerability emerges from distinct sociopolitical drivers of inequality that are woven the fabric of a local context in a particular point in time (Singer et al., 2022; Weaver & Kaiser, 2022).
Using the Mixed Methods GBV Syndemics Framework to Guide Research Inquiry
The mixed methods investigator must first decide which perspective (population or locally grounded) to begin with. Experts noted that (1) beginning with qualitative inquiry can develop a syndemic conceptual model of GBV that is later quantitatively tested and that (2) the initial qualitative data can guide the specification of quantitative models. Thus, beginning with a locally grounded (qualitative) perspective and transitioning to a population perspective (quantitative) is well suited when applying GBV syndemics to a new LMIC context/population where the syndemic dynamics are less known and a causal syndemic conceptual model needs to be developed. The exploratory sequential mixed methods design can also address challenges encountered by syndemic researchers. For example, initial qualitative investigations can clarify the concepts of comorbidity, interaction, and disease progression prior to quantitative modeling, identify endogenous/bidirectional relationships, and isolate syndemic mechanisms/pathways involving GBV. For example, investigators may be unaware of what GBV forms are the most common, the local phrases or idioms denote experiences of GBV and related distress, the degree to which GBV is normalized as part of everyday life, and through what pathways/mechanisms GBV interacts with other epidemics. Inductive investigations of GBV can inform more complex syndemic models that quantify complex and sensitive social experiences, thus moving the investigation from individual interviews or observations to generalizable population patterns.
Mendenhall et al.’s mixed methods population-based study in Soweto, South Africa focuses on syndemics of stress and multimorbidity (Mendenhall et al., 2021). Although not focused on GBV, their study can be analyzed as a case study of how to conduct an exploratory sequential design. Investigators began with an ethnographic stage that explored local perceptions of stress. The initial ethnographic phase shaped the study questions and developed a local measurement instrument (the 21 item Soweto Stress Scale) (Mpondo et al., 2022) employed in the second quantitative phase Mendenhall et al. noted that “using a generic life events scale could have missed what people in this context themselves define as most critical for determining quality of life” (Mendenhall et al., 2021). The second phase adopted a population perspective: using a probability sample, investigators quantified stress, multimorbidity, and quality of life. Interaction analysis revealed lowered quality of life when individuals experienced multimorbidity and were in the highest stress quintile (Mendenhall et al., 2021).
The second mixed methods approach begins with the population perspective (quantitative) and is followed by a locally grounded perspective (qualitative). Experts noted that follow-up qualitative data can aid in contextualizing quantitative syndemic results patterns, particularly regarding the development of intervention strategies for the local context. Thus, the initial quantitative phase requires that investigators approach the quantitative phase with deductive justification/hypotheses that (1) certain forms of GBV cluster and interact with other epidemics at the population level and (2) GBV and other constructs are appropriately measured using existing tools. Investigators follow best analytical practices for assessing syndemic clustering, interaction, and context. For example, quantitative approaches could involve latent class analysis of syndemic exposures, descriptive analysis of comorbidity, testing additive statistical interactions, mediation/path analysis, structural equation modeling with or without bidirectional relationships, and spatial epidemiology to identify hotspots of epidemic clustering. A follow-up qualitative phase is then implemented to better understand how and why syndemics patterns emerged in the quantitative data and to identify how to disrupt the harmful synergies. The second locally grounded phase also presents an opportunity for investigators to share the quantitative results with participants and relevant stakeholders. Further, the qualitative phase can address limitations in quantitative explorations and assessments of the sociopolitical context. Such an approach parallels experts’ views that engaging with the local community can improve the degree to which GBV syndemics research addresses local needs and can capitalize on existing GBV infrastructure for developing public/global health response.
Mendenhall et al.’s mixed methods, population-based study in Soweto, South Africa provides a case study for understanding how to implement the explanatory sequential design (Mendenhall et al., 2021). Building on the population-based quantitative findings, investigators implemented a third qualitative phase. In-depth interviews were conducted with a subsection of the participants who completed the epidemiological survey (Mendenhall et al., 2021). Investigators purposively selected participants based on membership in the comorbidity and stress cluster groups (Mendenhall et al., 2021). Inductive analysis revealed that the high stress and multimorbidity group experienced constant fear, financial burdens, and family conflict (Mendenhall et al., 2021). In contrast, the multimorbidity low stress group described social experiences that were more like participants without multimorbidity: adequate social support, less difficulty managing medications, and acceptance/positive view of their illness trajectory (Mendenhall et al., 2021).
Adopting a Mixed Methods Investigation of GBV Syndemics in LMIC
Four factors can increase our ability to integrate the population and locally grounded perspective when conducting GBV syndemic science. These factors are represented in Figure 1 as modifiable context. Based on the Delphi surveys with syndemic experts, funding opportunities for GBV research in global health and the ability to communicate with policy makers/funders the value add of syndemics have potential to improve mixed methods applications. Further, in terms of research capacity, the framework also requires a strategic integration and mastery of methodological approaches. Lastly, successfully working with terms of experts trained in population and locally grounded perspectives requires both interdisciplinary collaboration and mastery of multiple methods.
Contributions to the Field of Mixed Methods Research
The proposed framework deepens mixed methods research by providing guidance on how to (1) strategically position two important global health research perspectives (population and locally grounded perspectives), (2) increasing congruency between mixed methods integration and theoretical advancement, and (3) designing research studies that pragmatically address complex dynamics involving sensitive and hidden constructs like GBV. The framework has applications for engaging with biosocial perspectives on global health and investigating global health inequities. The mixed methods framework strikes a balance between the need to provide guidance based on existing evidence and expert consultation and the importance of not being overly prescriptive and inflexible. The framework also centers an intuitive understanding of the distinct ways in which the population and locally grounded perspectives enrich the investigation of GBV syndemics in LMIC. Strategically positioning qualitative and quantitative research phases will improve the emerging evidence base on GBV syndemics in LMIC, which is dominated by convergent mixed method designs, and challenge other investigators to empirically test biosocial theories using mixed methods.
Although the framework presented in Figure 1 may also apply to syndemics research outside of GBV and LMIC, it was developed for the purpose of expanding research inquiry on GBV syndemics in LMIC. In comparison to syndemics involving biological interactions between infectious diseases (e.g., hepatitis C and HIV, tuberculosis, and HIV) (Singer, 2010), GBV syndemics invoke additional layers of social and behavioral complexity. For example, GBV syndemics often incorporate both communicable (e.g., HIV/AIDS and sexually transmitted infections) and noncommunicable diseases/disorders (e.g., substance use disorders, depression, diabetes, etc.). GBV syndemic pathways/mechanisms extend beyond pathogen–pathogen interactions and involve pathways of appraisal, traumatic stress, and coping behaviors that intersect with contextual factors such as gender inequitable social norms. LMIC contexts also differ from high income countries in what macrolevel factors drive syndemic vulnerability. Thus, the framework presented focuses on leveraging mixed methods to improve GBV measurement and testing empirically informed GBV syndemic pathways/mechanisms.
Recommendations for Future Mixed Methods Inquiry
The mixed methods framework, research synthesis, and Delphi expert consultation raise several research recommendations. First, qualitative data can be more robustly leveraged to develop causal GBV syndemic conceptual models that can be subsequently tested using quantitative population data. Second, qualitative data can develop local measurement tools to quantify latent and sensitive constructs such as GBV. Importantly, local GBV measurement tools can address aspects that may be overlooked: bidirectional IPV, male victimization, cultural and social factors that shape GBV, and severity. Third, the toolkit of quantitative methods relevant for syndemics research (latent class analysis, descriptive statistics, additive interactions, spatial epidemiology) can elucidate GBV syndemic patterns at the population that require follow-up local knowledge contextualization for public/global health action. Understanding local infrastructure barriers and facilitators relative to GBV syndemic spatial hotspot areas requires follow-up qualitative work with communities and governments. Fourth, investigators can draw on the framework presented in Figure 1 to develop prospective mixed methods studies. For example, repeated follow-up qualitative interviews can be integrated a cohort study (Houghton & Paniagua-Avila, 2023). Fifth, the mixed methods framework also provides flexibility in incorporating other theoretical frameworks GBV syndemics. This may be particularly beneficial for developing and testing mechanisms which explain how socioeconomic conditions lead to endemic clustering and interactions. Theories related to gender power hierarchies, fundamental causes of inequality, and stress can enrich the investigation of GBV syndemics.
Limitations
This research is not without limitations. Although reminder emails were sent to the invited experts to complete the first and second round of the Delphi surveys, only 11 experts responded to the second round (response rate of 18%). A greater number of respondents may have led to greater levels of consensus. A third Delphi survey round could not be accommodated due to high attrition. Further, the framework developed did not address one expert opinion that emerged from the Delphi. The experts agreed that there is disagreement in the field regarding best quantitative analytical approaches. The mixed methods framework presented in Figure 1 does not prescribe specific quantitative approaches to modeling syndemics. Rather, based on the evidence synthesis, we provide a toolkit of possible quantitative approaches that can be used to investigate syndemic clustering, interactions, and context.
Conclusion
This research presents the first methodological framework detailing how to integrate qualitative and quantitative approaches when testing GBV syndemics in LMIC. The framework presents two perspectives that are important for syndemic science, the integration of GBV, and understanding LMIC contexts: (1) the population (quantitative) and (2) locally grounded (qualitative) perspective. A strategic mixed methods design requires that investigators determine with which perspective to begin the research process with and how to leverage the second perspective to deepen and expand insights from the first phase, relative to syndemic theory’s theoretical tenets. The framework is intended for syndemic scholars, GBV researchers, global health experts, epidemiologists, scholars investigating complex and hidden constructs, and investigators seeking congruency between mixed methods and theory.
Supplemental Material
Supplemental Material - Mixed Methods to Advance Global Health Research on Gender-Based Violence Syndemics: A New Research Framework
Supplemental Material for Mixed Methods to Advance Global Health Research on Gender-Based Violence Syndemics: A New Research Framework by Luissa Vahedi, Ilana Seff, Alexander C. Tsai, and Lindsay Stark in Journal of Mixed Methods Research
Footnotes
Acknowledgments
The authors would like to acknowledge the librarian, Ms Melissa Vetter, who supported the creation of the search strategy.
Ethical Considerations
This research was exempt from ethical approval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Vahedi’s doctoral research and studies were supported by the Social Sciences and Humanities Research Council of Canada Doctoral Fellowship and the Philanthropic Educational Opportunities Scholars Award. Dr Tsai acknowledges salary support from U.S. National Institutes of Health K24DA061696-01.
Declaration of Conflicting Interests
Dr Tsai reports a financial honorarium from Elsevier for his work as Co-Editor in Chief of the Elsevier-owned journal SSM – Mental Health. The other authors declare no competing interests.
Data Availability Statement
All data can be made available upon request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.