
Abstract
The intersection of mixed methods and community-based participatory research (MMCBPR) provides a promising approach to address health inequities. Drawing from strengths of mixed methods (which provides multiple channels for individuals to share experiences) and community-based participatory research methods (which center and empower marginalized communities in research), MMCBPR allows for the development of impactful and relevant research. This article contributes to the field of mixed methods research by illustrating a novel application of MMCBPR to a pilot research study aimed at understanding community resources and needs during the COVID-19 pandemic. We demonstrate feasibility for MMCBPR methods assessing multilevel structural and social determinants of health during times of social, political, and economic uncertainty and highlight challenges experienced in adopting this approach.
Keywords
Introduction
Mixed methods research (MMR) leverages strengths of both qualitative and quantitative data collection and analysis, allowing researchers to gain better insight into contradictions and connections across data and providing participants with multiple channels to share their experiences (Creswell & Plano Clark, 2018; Teddlie & Tashakkori, 2009). MMR is particularly helpful for investigations of health inequities because this approach allows researchers to gather a range of data to provide a more comprehensive and nuanced understanding of factors that contribute to the health conditions and outcomes experienced by different groups (Badiee et al., 2012; Creswell, 2014). For example, one recent study using MMR approaches found racial and ethnic differences in digital health information access through quantitative methods, and proceeded to conduct qualitative interviews with participants across racial and ethnic groups to better understand these differences (Tappen et al., 2022). While either element of this example could have provided a compelling story for inequalities in access to digital health interventions, the joint collection and display of quantitative and qualitative findings provided a more detailed description of specific concerns across racial and ethnic groups, which could more meaningfully inform targeted interventions. In short, this example demonstrates that mixed methods approaches can be used to facilitate understanding of the needs, resources, and preferences of marginalized communities by leveraging both qualitative and quantitative methods to investigate meaningful differences in health behaviors, access, and outcomes across communities (Stewart et al., 2008).
Community-based participatory research (CBPR) is an approach which centers community partnerships at every stage of the research process, from setting investigatory priorities to analysis, interpretation, and dissemination of findings (In Minkler & Wallerstein, 2008; In Wallerstein, 2017). Similar to MMR, CBPR methods can be particularly important in investigations of health disparities because close collaborations between researchers and key stakeholders can help to ensure that research is relevant and responsive to the needs of the community (In Minkler & Wallerstein, 2008), build trust and collaboration between researchers and community members, and identify underlying social, economic, and political factors that contribute to potential disparities (Jull et al., 2017; In Minkler & Wallerstein, 2008). At its core, CBPR seeks to combine expertise and knowledge of researchers and community members to create lasting social change (Collins et al., 2018; Wallerstein & Duran, 2010).
Considering the complementary nature of these methods, the integration of CBPR and MMR (henceforth referred to as MMCBPR) has been promoted particularly when working with marginalized communities (Badiee et al., 2012; Lucero et al., 2018; Windsor, 2013). One of the earliest mentions of integrating MMR and CBPR can be traced back to Minkler and Wallerstein’s 2008 article describing the importance of incorporating MMR in collaborative approaches to research that involve community members, researchers, and stakeholders to develop a more nuanced and comprehensive understanding of issues being studied. This integration has continued to evolve over time and across disciplines (DeJonckheere et al., 2019; Plano Clark & Ivankova, 2016). Prior studies have noted that holistic investigation of a given topic can be completed through MMR, while taking a CBPR approach increases the sustainability, impact, and rigor of the overall study and associated outcomes (Balazs & Morello-Frosch, 2013; Jones et al., 2020; Upadhyaya et al., 2015). However, recent systematic reviews reveal that there is still substantial room for growth in MMCBPR methodology, noting that current MMCBPR studies inadequately describe why either approach was selected (DeJonckheere et al., 2019; Jones et al., 2020). In particular, while most MMCBPR studies provide explicit justifications for the use of CBPR, only a small fraction of studies provide rationale or detailed descriptions of MMR (DeJonckheere et al., 2019; Kaur et al., 2019), indicating a need for more detailed descriptions and justifications for the use of specific mixed methods components. Additionally, DeJonckheere et al. (2019) found that the integration of mixed methods research design into key phases of CBPR research remains underdeveloped—specifically, additional studies which offer clear explanations of how MMR are incorporated into the seven phases of CBPR are needed in order to further our understanding of real world applications of this approach. In this discussion paper, we describe the explicit intersection of MMR into each phase of a recently completed pilot CBPR project, and discuss the feasibility of these methods during the COVID-19 pandemic. First, we describe the positionality of the study team and the motivation behind this work in the context of exacerbated health inequities following the COVID-19 pandemic. Next, we provide a detailed chronicle of how MMR approaches were integrated into each phase of the CBPR process. Finally, we summarize challenges and lessons learned from this study, our contribution to the mixed methods literature, and next steps for this research.
Example Study: A Racial Equity Response Team for the COVID-19 Pandemic Related Recession
In response to the COVID-19 pandemic, a study team comprised of researchers at the University of California, San Francisco (UCSF), San Francisco State University, Streetwyze, and Roots Community Health Center (Roots) conceptualized and designed a MMCBPR research study to understand the impacts of the pandemic on three racially and economically diverse counties in Northern California (San Francisco, Alameda, and Contra Costa). The huge wealth gap that exists in each of these counties made this geographic region a prime area for studying the impacts of the pandemic on economic marginalization. Streetwyze is a mobile mapping and SMS platform, which was founded with the intention of allowing community members to share local knowledge and real-time data on their experiences in and perceptions of their neighborhood (Akom, 2017). Streetwyze has been recognized nationally as a platform that successfully engages and empowers residents of low-income communities and communities of color to promote positive change in their neighborhood environments (Akom, 2016; 2018). Roots is a community-based healthcare organization dedicated to providing comprehensive, culturally competent care and addressing health disparities in underserved populations (Roots Community Health Center, 2014).
The primary purpose of this project was to utilize real-time neighborhood and epidemiologic feedback to identify resource gaps (such as food, housing, and healthcare) and describe the impacts of the COVID-19 pandemic and concurrent economic recession on residents’ well-being.
Study Context
The COVID-19 pandemic highlighted and amplified health inequities generated by persistent structural racism and inequities in the social and structural determinants of health (e.g., economic stability, neighborhood environment, health care, social circumstances, and education) (Dorn et al., 2020; Gauthier et al., 2021; Koh et al., 2011; Perry et al., 2021; U.S. Department of Health and Human Services, 2010). Prior to the pandemic, racially and economically marginalized communities were already burdened by limitations of services and resource infrastructures (e.g., food banks) (Anthony, 2020; Karlis, 2020; Katoni & Rusch, 2020). These challenges were exacerbated by shelter-in-place policies, which made critically important resources even less accessible (Chang, 2020; Gilligan, 2020). Throughout the pandemic, communities of color were disproportionately burdened by COVID-19 infection, hospitalizations, and mortality as well as by consequences of shelter-in-place ordinances and the pandemic-related economic recession (California Department of Public Health, 2020). These same communities were at the center of increased activism in response to police brutality against the Black community, which, while representing positive collective action and support, may have been accompanied by re-lived racial trauma and discriminatory backlash (Taylor, 2021). Further compounding existing infrastructure issues and the new burden of COVID-19 disease, the pandemic will have long-lasting harmful impacts to economic conditions (Anthony, 2020; Arango & Fuller, 2020; Flaming & Burns, 2020; Larsen, 2020; UCLA Anderson Forecast, 2020).
There is an abundance of evidence that structural and social determinants of health have real and long-lasting effects on individuals’ health and life expectancy (Braveman et al., 2011; Koh et al., 2011; U.S. Department of Health and Human Services, 2010) (Figure 1). For instance, within racially and economically marginalized communities, it is highly likely that worsening structural and social determinants of health bring about even more severe long-term adverse health outcomes than the COVID-19 disease itself (Abrams & Szefler, 2020; Webb Hooper et al., 2020). Thus, our proposed project addressed the mitigation of adverse structural and social determinants of health as experienced by racially and economically marginalized communities during the COVID-19 pandemic and aimed to provide tools to support these communities beyond the pandemic. Our approach was embedded within a racial equity framework which acknowledged the structural racism and class oppression that led to a disproportionate burden of stress and poor health, gave voice to those experiencing inequity, and consciously supported the health of racially and economically marginalized communities (Gray et al., 2020). This approach is unique in its integration of multiple forms of qualitative and quantitative data (i.e., individual and household survey data; crowd-sourced, local neighborhood data; and population-level neighborhood data). Structural and Social Determinants of Health, adapted from Healthy People (2020) (U.S. Department of Health and Human Services, 2010).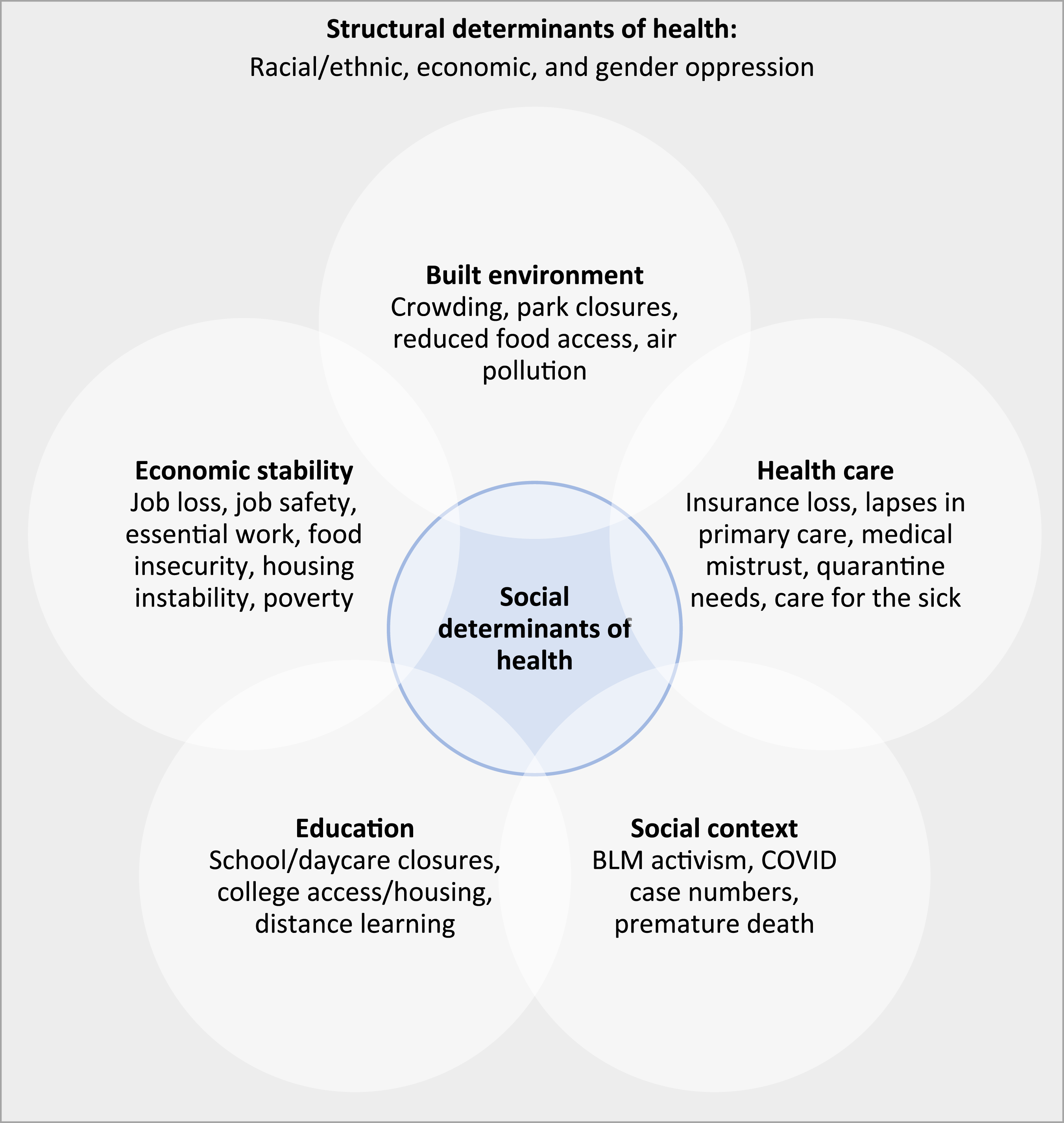
We implemented several recruitment strategies, including engaging with existing users of the Streetwyze platform, partnering with Roots to share flyers/postcards and attending existing virtual support groups, posting weekly on social media platforms (i.e., Instagram and Twitter), and sustaining interactions with participants through text and email. Participants were invited to engage in the study in whatever capacity they preferred (including completing quantitative surveys, submitting neighborhood reports, or both). Between September 2020 and December 2021, we received 51 baseline survey responses and 236 qualitative neighborhood reports from 19 unique respondents (94.7% of whom also completed the baseline survey), and ongoing follow-up surveys, which was made possible by the recruitment and outreach efforts of Roots, our trusted community partner on the ground. We received ethical approval from the Institutional Review Board of the senior author’s home institution.
MMCBPR Integration and Research Methods
In the sections below, we will specifically describe ways in which MMR was integrated into each of the seven core phase of the CBPR research process (DeJonckheere et al., 2019; In Israel, 2013) (Figure 2): (1) forming a CBPR partnership, including establishing relationships between community members, stakeholders, and researchers; (2) identifying priority issues and research questions that are mutually beneficial to all partners involved in the research; (3) designing and conducting research, including discussing and making decisions about appropriateness of research methods; (4) feeding back and interpreting findings, by engaging all research partners in developing analytic approaches and interpretation; (5) disseminating and translating findings to community members, including making decisions about the results to be published and identifying appropriate channels for dissemination; (6) assessing community strengths and dynamics, including discussions about strategies to best engage with community members who have been historically marginalized; and (7) maintaining, sustaining, and evaluating the CBPR partnership, by having open and honest conversations about the facilitators and barriers of effective collaboration and ongoing acknowledgment of existing power dynamics. Intersecting processes of mixed methods and community-based participatory research.
Forming a CBPR Partnership
Our interdisciplinary research team comprised of academic researchers and community partners from UCSF, San Francisco State University, Streetwyze, and Roots. Our team had combined expertise in racial equity research; direct service; community engagement and outreach; use of technological interventions to harness community resources and social resilience; social epidemiology; mixed methods research; and harmonization of complex, multilevel data. Specifically, this partnership formed from a shared interest in exploring the neighborhood space as a determinant of health and well-being and a shared goal of using this research to inform neighborhood-level solutions that were relevant for the immediate needs of communities. This interest was at the core of the UCSF principal investigator’s research portfolio and the foundation and mission of Streetwyze as a platform (which focuses on resident powered solutions and mobilization). This interest also fundamentally reflected the historical investments that Roots has made to creating healthier local neighborhoods, bolstering its reputation as a critical, trusted, and well-established community organization. This partnership was fostered through weekly meetings with a core interdisciplinary team, in which we discussed issues related to participant recruitment and engagement during a pandemic. Additionally, ongoing conversations between UCSF, Streetwyze, and Roots ensured that data collection and analysis efforts centered community needs and solutions. The nature of remote work during the pandemic helped to strengthen these partnerships, as it became easier for the team to schedule and engage in discussions about shared interests and priorities.
Identifying priority issues and research questions
The priority research agenda for this study was to develop a data model for rapidly responding to the needs of local communities. Specifically, we wanted to understand the extent to which the pandemic impacted structural and social determinants of health, as well as identify barriers and facilitators of overall health and well-being. An MMR approach was critical for us to accomplish this objective because the pandemic uncovered emergent needs for local communities that would have been insufficiently captured by any singular data source. Thus, in order to comprehensively understand and monitor participants' social and material conditions, a combination of qualitative, quantitative, and geospatial data was most appropriate and allowed for participants to engage with the research process more flexibly.
Additionally, our team acknowledged that decades of academic interest and involvement in low-income and communities of color in the San Francisco Bay Area have contributed to research fatigue (Ashley, 2021; Patel et al., 2020). Thus, to ensure that our priority research question would truly benefit the local community, our existing CBPR partnership provided guidance on how to meaningfully engage with community members to prioritize responsiveness to needs. Specifically, at its core, Streetwyze was developed to focus on identifying scalable solutions and Roots emphasized fostering community solutions rather than focusing on deficits. Thus, the team prioritized understanding and building community cohesion and solutions.
Designing and conducting research
Due to the pandemic, all data were collected remotely, through online surveys and the Streetwyze mobile application. We selected a convergent mixed methods design for data collection, which is an approach that uses strategic integration of qualitative and quantitative data to triangulate findings across data sources and yield a more comprehensive and nuanced understanding of participants' experiences (Creswell & Plano Clark, 2018). A convergent design was the most appropriate choice for this study given this was a pilot research project and the flexible nature of data collection in a convergent design allowed us to ensure that relevant themes we “discovered” in any type of data collected could be used to inform other elements of data collection. Specifically, because we anticipated that the pandemic would result in emergent needs that were not anticipated by the research team, the simultaneous collection, analysis, and iteration of qualitative and quantitative data collection materials was the most appropriate approach.
We collected qualitative neighborhood reports using Streetwyze. Specifically, on the Streetwyze platform, participants were asked to indicate the location (on a map) of an experience/resource they wanted to share, rate the experience/resource, and share qualitative descriptions via text/audio/video-based stories (see supplemental materials for full list of prompts). This collection of real-time, location-based data on users’ experiences in and perceptions of their neighborhoods through a mobile data collection platform has been found to be a promising avenue for residents to share their lived experiences (Galea et al., 2020). Importantly, the Streetwyze mobile platform also allowed for participants to view other community members’ stories and data points. Therefore, while the use of this platform provided an avenue for ongoing engagement between participants and researchers, it also served as a real-time resource network for community members to learn about resources in their communities and monitor changing circumstances of the pandemic (Gamache et al., 2018; Zhang et al., 2017). Additionally, as mobile platform-based data collection was not limited to single points in time, this allowed for on-going monitoring of circumstances within communities as the pandemic and recession continued. Furthermore, as the fundamental goal of this pilot study was to identify solutions and needs that were meaningful for communities, leveraging the existing, engaged community of Streetwyze users allowed for an efficient “boots on the ground” approach for identifying relevant issues. Finally, as participants were able to share their experiences while actively interacting with their environments rather than in interview settings, qualitative and geospatial data collected from Streetwyze reflected social and economic determinants which were relevant to the community.
We simultaneously collected baseline epidemiologic surveys which assessed participants’ changing circumstances before and after the start of the pandemic (March 2020). In addition to collecting sociodemographic and geographic data, themes for the baseline survey were selected based on the structural and social determinants of health, which have been documented to be impacted by the pandemic. Specifically, our quantitative surveys included questions related to employment, housing, health insurance, transportation, well-being (e.g., stress, discrimination, and health), and COVID-19 illness. All questions were taken or adapted from validated instruments (e.g., the everyday discrimination scale (Williams et al., 1997), two-item PROMIS (Patient-Reported Outcomes Measurement Information System) global physical and mental health scales (Hays et al., 2017), and the Perceived Stress Scale (Cohen et al., 2014)) and modified to assess for potential changes to a participant’s circumstances prior to and following February 2020 (when the counties in the study were subject to widescale pandemic restrictions). Participants were also asked to complete repeated follow-up surveys every two months, which were designed to assess individual changes within each domain of the baseline survey. Following the convergent mixed methods design, we added and edited questions to the follow-up survey in response to content from neighborhood reports.
A procedural diagram depicting different components of data collection and integration are presented in Figure 3. Procedural diagram illustrating mixed methods data collection and integration.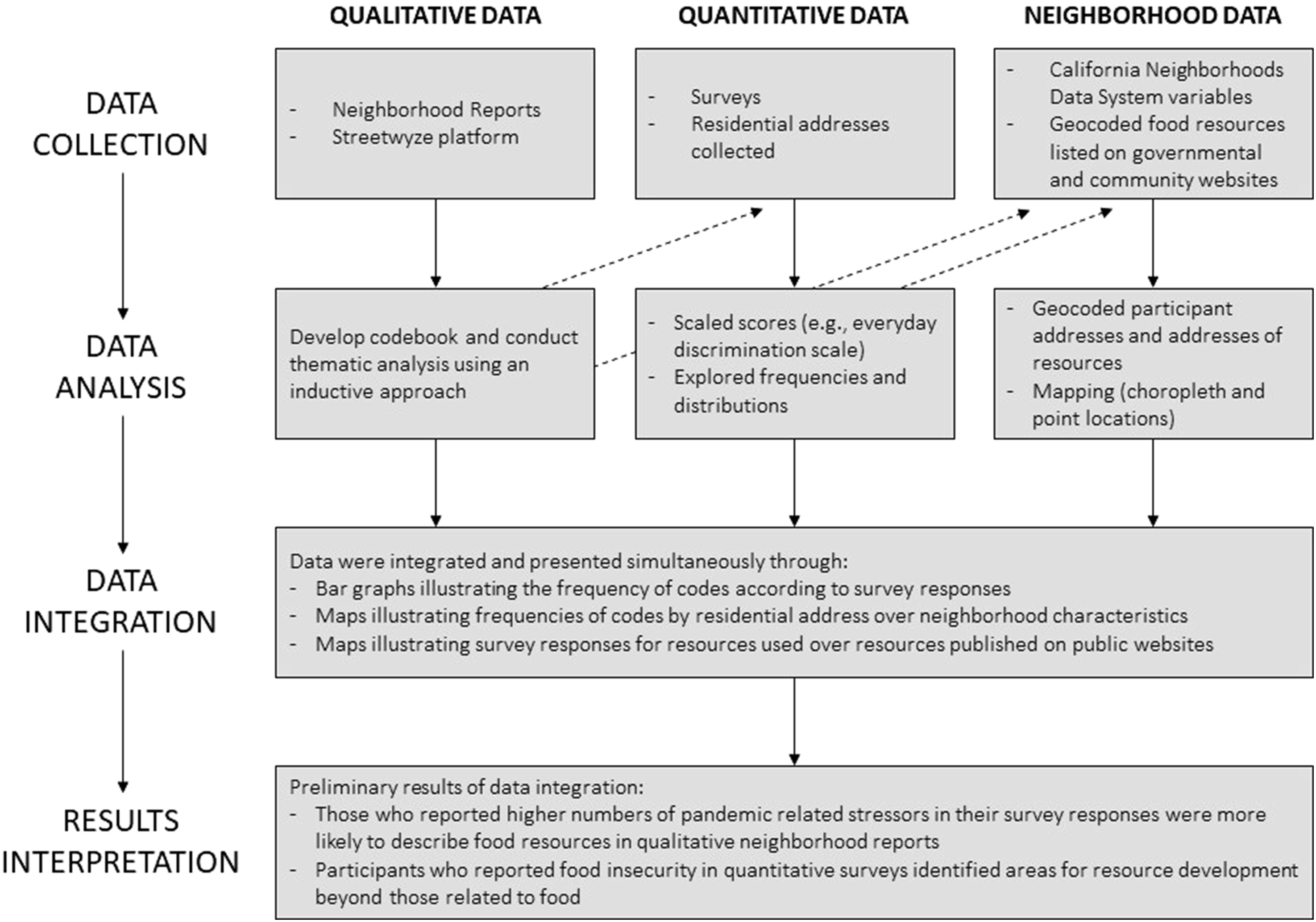
Feeding back and interpreting findings
Throughout the data collection process, we iterated upon our quantitative and qualitative data collection materials based on feedback from preliminary findings. Specifically, priority issues that emerged from the qualitative neighborhood reports that were not hypothesized by the social determinants of health framework were used to modify our follow-up survey. For example, preliminary analysis of neighborhood reports revealed that participants expressed strategies for coping, resilience, and neighborhood perceptions as relevant topics in their daily lives. Though survey items pertaining to these themes were not included in our baseline survey, the preliminary analysis of our qualitative data prompted us to add new questions to capture these topics in our follow-up surveys.
In addition to the data analysis and interpretation that informed and refined our data collection processes, findings were also presented to our community partners to solicit feedback and ensure that our strategies remained relevant. We disseminated these findings to food banks and relevant local organizations through flyers and over social media, and to state policy experts and community leaders who offered feedback and guidance on appropriate entities to target and priority domains of interest.
Disseminating and translating findings
We developed an integrated data analysis model to describe groups of individuals (e.g., by income level, pandemic-related employment changes, and mental well-being) for whom qualitative themes (e.g., food resources and healthcare access) were most frequently mentioned. Specifically, we employed a stepwise approach to integrating our multiple data sources to describe food insecurity and resource needs, which will be reported (Tashakkori & Teddlie, 2010) in a forthcoming manuscript. In short, we first transformed qualitative data into quantitative form, wherein an indicator was devised to discern codes that surpassed the average mentioned frequency at the participant level. Then, because participants provided residential addresses through the survey and all qualitative neighborhood reports are geolocated, we integrated the transformed qualitative data with quantitative data or geospatial data to describe participants’ food experiences. For example, we illustrated the prevalence of “above average” mentions of food resources in qualitative data by participant's self reported food insecurity in the quantitative survey. As another example, we mapped the locations of food resources that participants reported using during the pandemic (e.g., food pantries and food banks) to total food resources per capita at the census tract level as an illustration of resource use. These analyses provided a glimpse into specific neighborhoods where resources were being heavily used, and geographic areas with unmet needs. In addition to oral and written presentations that have been delivered to community members, community-based organizations, and policy stakeholders, we intend to disseminate findings from our data integration model and qualitative data analysis through academic journals.
Assessing community strengths and dynamics
An ongoing priority of our interdisciplinary research team was to highlight community resources that supported participants through the pandemic and related recession. Descriptions of such resources were made possible through qualitative and geospatial data, which included descriptions of resources that organically emerged within communities. For example, participants described community initiatives and resources such as online/no-contact library borrowing, well-maintained outdoor spaces, and high quality or comforting food resources as helpful for coping and maintaining resilience. These findings informed the addition of survey instruments related to coping and resilience in subsequent surveys and allowed us to advocate for the support of these resources in presentations to community-based organizations and policymakers. A full manuscript documenting emergent resources and coping strategies was published for academic audiences earlier this year (https://link.springer.com/article/10.1007/s40615-023-01824-x).
Maintaining, sustaining, and evaluating CBPR partnerships
Following this project, our team will continue to identify opportunities to utilize the MMCBPR approach to inform local policies and recommendations. We are in the process of evaluating our partnership, engaging new institutions and individuals to participate, and discussing the priority issues and design of the mixed methods approach. Additionally, we are continuing to seek government and foundational funding for ongoing efforts to support the research goals and needs of participating communities.
Conclusion
In this study, we presented a novel adaptation of the MMCBPR approach to develop a data model to rapidly assess and understand the needs of racially and economically marginalized communities during the COVID-19 pandemic-related recession. This work is at the leading edge of new approaches to data collection, racial equity, and community-centeredness. The CBPR component directly engaged racially and economically marginalized communities, and allowed for individuals most likely to be affected by recession to articulate their needs directly, while MMR methods assured that individuals’ lived experiences were meaningfully captured and contextualized. Furthermore, our use of mobile technology for real-time collection of neighborhood data allowed for rapid and repeated assessment of on-the-ground circumstances for communities. Although MMCBPR approaches have been well utilized by researchers across disciplines, to our knowledge, they have not been described in the context of the rapidly changing social, political, economic, and medical landscape following the COVID-19 pandemic. We demonstrate that this method was feasible, and allowed for the provision of community-generated, relevant data on critical resources and services that were used by racially and economically marginalized communities during the pandemic.
Our approach can be adapted to establish measures for ongoing monitoring of structural and social determinants of health within communities at risk, including monitoring interventions, programs, or policies. We intend to incorporate this design into future studies with the hopes of providing ongoing and sustainable tools for communities. Specifically, methodologies used in this work are well-positioned to service community-based organizations, foundations, and governments to provide high priority resources in an equitable and accessible manner to whom and to where they are most needed. Our ultimate, long-term goal is to provide communities with evidence to adjust hyper-local tactical programs and policy recommendations and, to the degree possible, to scale recommendations at regional and statewide levels.
Contribution to the Mixed Methods Literature: Challenges and Lessons Learned
There were several key challenges that we faced in this study. First, the time commitment that we were asking of participants was substantial, which is a known difficulty that has been documented by other studies utilizing MMCBPR approaches. Similarly, while we were able to leverage existing virtual community spaces to recruit participants, we were unable to utilize in-person recruitment strategies due to pandemic restrictions, which could have helped to expand our participant pool. In our initial proposal, we had intended to collect both quantitative surveys and qualitative neighborhood-level reports from all participants. When this approach proved to be misaligned with the needs and interests of the participants, we modified our original plans to instead offer multiple channels to participate, enabling participants to provide both qualitative and quantitative data, or either individual component. Additionally, many community members had pandemic-related critical needs that required immediate attention throughout our study, which required additional time and labor for our community partners to onboard and consent individuals and maintain their engagement in the study through the year and a half. As with any CBPR study, we adapted our research protocols to ensure that participant engagement was as easy as possible, thus shifting to electronic and verbal consent forms to reduce the amount of effort needed to onboard participants.
Though the cyclical nature of both mixed methods and CBPR processes was inherently challenging, we embraced this pilot study as an opportunity to iterate our approach to data collection and continually evaluate the data we collected. For example, in the later stages of the CBPR process (feeding back and interpreting findings, disseminating and translating findings, and assessing community strengths and dynamics), we relied on consistent communications within our interdisciplinary partnership to ensure that the research process remained faithful to our primary objectives. Additionally, throughout the mixed methods research process, we used our quantitative and qualitative data collection and analysis efforts to complement and co-inform each other. With the integration of both processes, feedback and dialogue in our interdisciplinary team was critical to iterate data collection and analysis. The findings emerging from both quantitative and qualitative data sources were used to inform relevant partnerships that we should approach in future studies to respond to the needs of the community. For instance, food needs and resources quickly emerged as an important theme across qualitative, quantitative, and geospatial data. Because of this, we developed an infographic for local food resource organizations, highlighting our data collection approach and extending opportunities for data use and partnership. Additionally, we presented our work to a program which bridges researchers with policymakers, to develop strategies for identifying policy-relevant partnerships and messaging. Altogether, this iterative and cyclical process allowed us to be dynamic and responsive in our approach to further advance equity among local communities which have experienced racial or economic marginalization.
Some important lessons that we believe can be further explored in future studies implementing these methods are (1) building in strategies for ensuring participant engagement and (2) interpretation of neighborhood reports to ensure that residents’ lived experiences are meaningfully leveraged for position change. For example, while we did not have the resources to do so in this study, future projects could leverage the multiple sources of data to conduct targeted follow-ups with select participants to provide immediate feedback about concepts and themes that emerged from their reports (e.g., communicating the researcher interpretations of concepts emerging from qualitative or quantitative reports to participants to assess consistency and provide opportunity for direct feedback on findings).
The advantage of intersecting MMR and CBPR in the context of our research agenda is clear. Because our study goal was to understand community-level impacts of the pandemic on racially and economically marginalized individuals, CBPR approaches were necessary to frame the overall study design and questions, identify strategies for recruiting communities of interest, and to develop a dissemination plan which ultimately benefited the targeted community. Additionally, due to the unprecedented nature of the COVID-19 pandemic, a mixed methods research approach was critical for the identification of emergent needs and to monitor changes in theorized needs. The integration of MMR and CBPR allowed for the collection of multiple data sources (qualitative, quantitative, and geospatial) to provide a more complete picture of research questions that were relevant to racially and economically marginalized individuals and to ensure that findings would be relevant and useful for community-based organizations and policy makers. MMCBPR methodology has been widely utilized in the context of health education interventions (Christopher et al., 2008; Wiggins et al., 2014) and to explicate nuances in CBPR partnerships for the advancement of social justice (Bellows et al., 2015; Lucero et al., 2018; NeMoyer et al., 2021). Our study suggests that the intersection of these two approaches to research was feasible in the context of the COVID-19 pandemic and can be applicable to future studies which require rapid response to research.
In conclusion, our project offers an example study on how the MMCBPR approach can be effectively used to respond to community needs during times of social, economic, and political uncertainty and informs an approach for continued, rapid monitoring and feedback. In the long-term, we intend this study to provide a proof-of-concept, processes, and tangible support for enabling rapid assessment of multilevel structural and social determinants of health. Through our community-based participatory research practice, we hope to establish long-term and meaningful connections which will offer a symbiotic exchange of resources. This is critical for an evidence-based response to ongoing and future public health challenges, particularly those that are driven by structural and social inequities.
Supplemental Material
Supplemental Material - Combining Mixed Methods and Community-Based Participatory Research Approaches to Identify Neighborhood-Level Needs During the COVID-19 Pandemic
Supplemental Material for Combining Mixed Methods and Community-Based Participatory Research Approaches to Identify Neighborhood-Level Needs During the COVID-19 Pandemic by Alice Guan, Tessa Cruz, Jamaica Sowell, Brenda Mattias, Aekta Shah, Analena Hope Hassberg, Salma Shariff-Marco, Antwi Akom, and Mindy C. DeRouen in Journal of Mixed Methods Research
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of California Office of the President, California Breast Cancer Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.