
Abstract
Little is known about how New Zealand men understand their health and wellbeing as they age and what are the determinants of their healthy ageing. Contiguous and exploratory sequential mixed methods study were conducted with the collection of both focus group and survey data. Methodologically, this abductive process was incorporated within an intersectional framework, providing a comprehensive picture of healthy aging in men across life stages and socioeconomic statuses. Integrated results revealed that for respondents the most significant factors influencing their healthy aging were, life engagement purpose, substance misuse, and masculinity norms. This article contributes to mixed methods research by providing practical applications of incorporating the intersectional model to enhance rigor in designing, conducting, and interpreting mixed methods research.
Introduction
In Aotearoa New Zealand (NZ), the number of NZ men over the age of 45 years is projected to increase by nearly 60% by 2048 (1320K) from 2022 (824K), with an almost two times increase (from nearly 394K to over 645K) in the number of men over the age of 65 years of age (Statistics NZ, 2022). This substantial demographic shift in this age population will bring additional health challenges as the health status of ageing males has far-reaching consequences for families, societal health and social care services and the country as a whole (Collaborators, 2022). In addition, the soaring ageing male population will have a marked effect on the socio-economic and political infrastructure developments, which are traditionally more focused on the older female population (Xiao et al., 2022). Such complexity of the ageing trajectory among males in NZ is ideally suited through the employment of an intersectional, mixed methods research approach.
The importance of “healthy ageing” has become recognized globally in response to the challenges associated with ageing societies (Sowa et al., 2016). It is now commonly defined by WHO: “As the process of developing and maintaining the functional ability that enables wellbeing in older age” (Fallon & Karlawish, 2019; Rudnicka et al., 2020). In NZ, ageing well/healthy ageing was adopted as the term by the Ageing Well National Science Challenge, one of 11 challenges established to undertake mission-led research on the biggest science-based challenges facing NZ. If models of healthy ageing are to be promoted and to be effective, there needs to be a good evidential base of understanding factors that influence the health and wellbeing of this rapidly ageing population and to address inequalities across different social contexts.
So far, what is known from government level and previous studies is that in NZ, the life expectancy for men at birth is three-four years less than that of women (Ministry of Health NZ, 2018). It has long been recognized that the overall burden of disease is higher for men than for women, in both developed and developing countries (Hawkes & Buse, 2013). Data from the NZ Ministry of Health also shows for those 50–75 years old, overall mortality for men is 30% higher than that of women (Ministry of Health NZ, 2016). Men are more likely to experience heart disease, chronic liver disease, and cirrhosis of the liver at an earlier age than women and are more likely to suffer premature death (White et al., 2013). Previous studies also show that there are amplifying factors influencing the health challenges facing ageing males relating to their lifestyle, risk-taking behaviors, and poorer engagement with healthcare services and preventive public health measures (Gebhard et al., 2020; Rubin et al., 2020; White, 2020; Wu et al., 2021). In keeping with this, the contemporary global Coronavirus Disease (COVID-19) outbreak has further highlighted men’s vulnerability with the disproportionately higher death rate and lower immune response among men compared with women (Betron et al., 2020).
Compounding those gender inequalities highlighted in the literature, the health of the ageing male population has also received relatively little attention as an area of public health concern (Baxter et al., 2017; McKinlay, 2005). There is limited recognition of the importance of men’s health within NZ, including how to ensure older men age well and enjoy an extended healthy life span. In research terms, the area is broad but empirical evidence related to NZ men’s health is sparse; this is especially the case for the experiences of ageing and aged men, in part due to a dearth of population-level information. Most research studies in this area are either qualitative studies with limited sample size or comparative studies using gender as a social demographic factor and seeking to quantitatively analyze differences between men and women in certain health indices (Lohan, 2007; Xiao et al., 2022). In contrast, data using mixed methods approaches regarding what factors are associated with healthy ageing in the special context of NZ males remain scarce, particularly among Māori men (Indigenous people of NZ). To address this gap, this study—as one of the few mixed methods study on men’s healthy ageing in NZ—aims to provide holistic insights into factors that influenced men’s ability to age well. Methodologically, by employing the empirical study, it also aims to make contributions to mixed methods research.
Methodology Orientation
Mixed Methods and Abductive Approach
This exploratory-sequential mixed methods study incorporated an abductive approach and was framed by an intersectional framework. Since men’s healthy ageing is relatively a broad and under-explored concept, a pluralistic approach is better suited to answer the primary research question “What factors influence men’s healthy ageing in NZ.” This research question adheres to the fundamental principle of mixed methods research, which emphasizes the collection of diverse data through various strategies, approaches, and methods (Johnson et al., 2007). Both qualitative and quantitative approaches were used as the former approach enabled a better understanding of men’s healthy ageing, and the latter tested suppositions using the hypothetico-deductive model and quantify various aspects of men’s health themes (Gunter, 2013). Such a combination ensures that the strengths of each approach complement one another while minimizing any overlapping weaknesses.
The abductive approach has been defined as “the operation of adopting an explanatory hypothesis” (Peirce, 2009). It is interpreted as giving reasons for pursuing a hypothesis, which is associated with the purpose of this mixed methods design (Wheeldon & Ahlberg, 2011). It is regarded as a fundamentally creative, fruitful alternative to the induction/deduction dichotomy and addresses weaknesses associated with both approaches by allowing interactions between them (Lipscomb, 2012; Svennevig, 2001). This approach allows for generating theoretical themes from focus groups (inductively) and then being tested by establishing a conceptually connected hypothesis through a larger sample survey (deductively). It was chosen here as it has been used successfully by others exploring men’s health experiences (Robertson, 2006), and is consistent with the previously completed study in this region (University of Otago, 2017).
Intersectional Framework
So far, what is known from previous studies is that older men’s health and help-seeking behaviors appear to be inextricably linked to traditional notions of hegemonic masculinity (Duncanson, 2015; Smith et al., 2007) and that such masculine ideologies and expectations are context-specific. In NZ, young Pacific male athletes were very willing to seek help for mental distress whereas older men with prostate cancer displayed negative views of seeking medical help (Marsters et al., 2021; Medina-Perucha et al., 2017). Similarly, studies have found that men’s help-seeking behaviors are germane to age (Wang et al., 2013), cultural influences (Galdas et al., 2007), and the self-perceived severity of their symptoms (Douglas et al., 2013). Thus, it is important to recognize health behaviors and as a consequence, health outcomes for men are also determined by age, race, ethnicity, culture, sexual identity and orientation, and disability and economic status (Griffith, 2012; Griffith et al., 2011). Such aspects of intersectionality were acknowledged in trying to better understand men’s health and health disparities in this study (Merlino et al., 2020) (Figure 1). Intersectional framework of exploring healthy ageing determinants.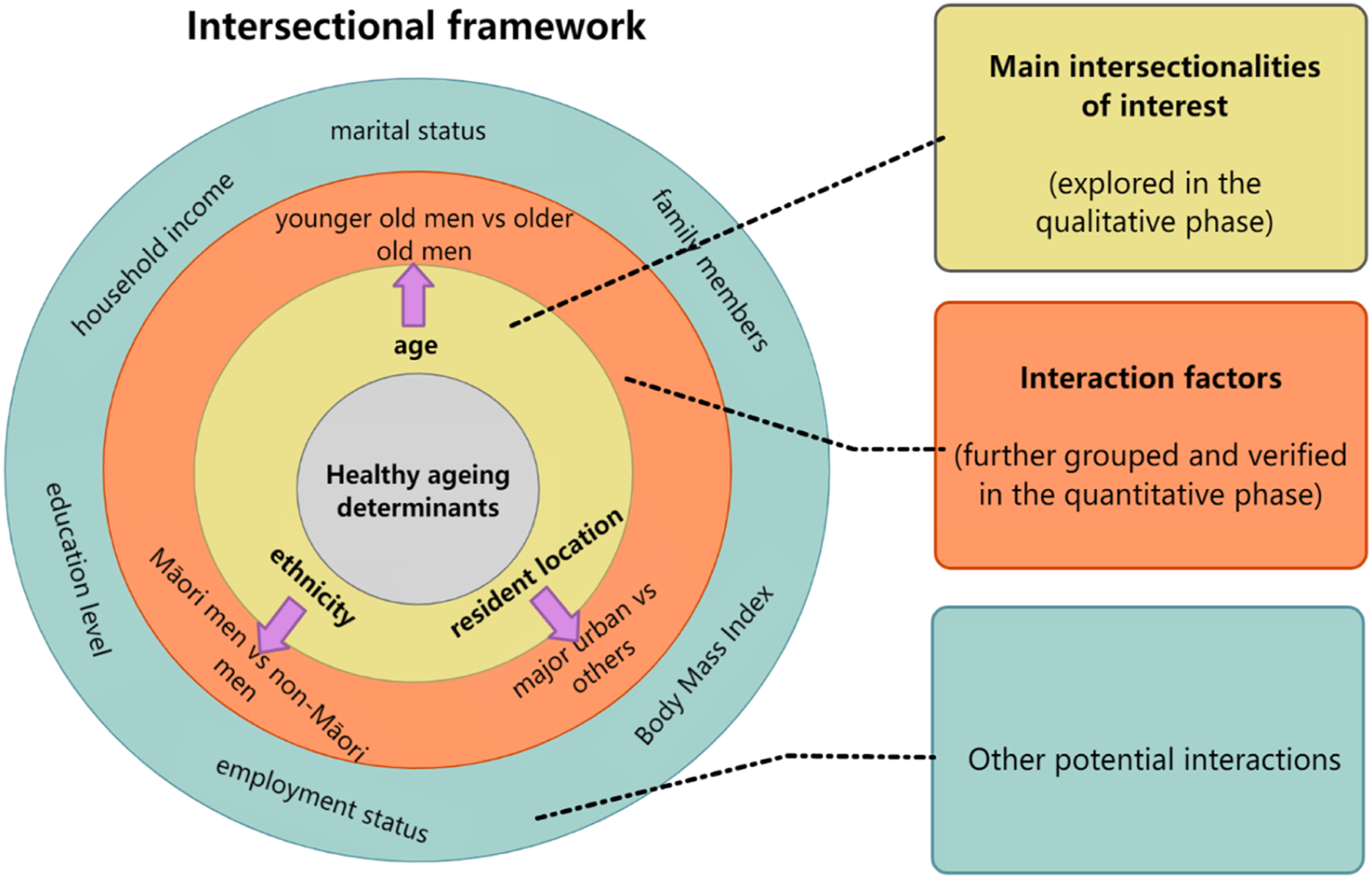
Intersectionality is a framework that recognizes how different social categories (such as ethnicity, age, class, sexual orientation, and ability) intersect and interact, leading to a comprehensive understanding of men’s healthy ageing issues (Cole, 2009). Addressing intersectionality in this mixed methods study involves incorporating multiple dimensions of identity and social categories into the research design, data collection, analysis, and interpretation. As shown in Figure 1, the inner most circle is the primary research question. Age, ethnicity, and resident location are the three intersections of interest, which were firstly incorporated into the qualitative study design and data collection. Then these interacting factors were further grouped into binary variables and their interacting effects have been tested in the quantitative phase. Such framework enables a close focus on significant transitions across different life stages and socioeconomic statuses for men and emphasizes the interplay between various factors, rather than seeing these in isolation (Gunnarsson, 2009). Exploring how men understand and interpret their experience within this framework has significant implications for explicitly addressing men’s health issues and how best to support men to age well and have positive wellbeing.
Aims and Research Questions
The primary aim of the qualitative phase study was to explore older men’s (≥45 years) beliefs and understanding about their health and wellbeing and healthy ageing. The secondary aim was to identify what aspects they considered important. These findings were then to be used to inform the design of the questionnaire for the quantitative component of this mixed methods study. As key elements, determining older men’s preferences for survey administration (online vs. paper), considering potential biases that could arise from using these methods, and identifying possible strategies for improving response rates. Given the lack of NZ research on ageing and men, our principal research questions in the qualitative phase were designed to capture a range of participants’ perspectives across multiple domains.
The quantitative phase aimed to explore the generalizability of the themes identified from the focus group analysis within a wider population. An appropriate survey instrument based on pre-existing validated questionnaires was developed to explore the specific research questions as listed below.
Research question one: What is the status of healthy ageing and HRQoL among male residents in Otago and Southland regions, and how does it differ between Māori and non-Māori men?
Research question two (main research question): What are the factors (men’s healthy ageing risks and challenges) influencing each domain of healthy ageing and HRQoL amongst NZ men?
Research question three: How are these factors differentially related to healthy ageing and HRQoL across ethnicity-specific, age-specific, and location-specific interactions?
Methods
Study Design
The design of this study was based on the methodology and framework indicated above. Semi-structured focus groups employing reflexive thematic analysis narratives were chosen for the qualitative phase (Braun & Clarke, 2019), and a cross-sectional survey (larger component) that encompassed both online and postal questionnaires was chosen for the quantitative phase. The University of Otago Ethics Committee (reference code H19/150 for the qualitative component; H20/165 for the quantitative component) approved this mixed methods study. Qualitative data were reported as per the Consolidated Criteria for Reporting Qualitative Research (COREQ) statement (Tong et al., 2007). Quantitative data were reported as per the Reporting of Studies Conducted using Observational Routinely-collected Health Data (RECORD) statement (Benchimol et al., 2015).
Focus Group Procedure
According to our study protocol (Xiao et al., 2021), six focus groups were conducted in both urban and rural areas of Southern NZ. A pilot focus group was conducted first among a group of researchers currently working with older adults at the University of Otago. Each focus group was conducted by one moderator (DB), and two recorders (HX) and (LL) with experience in talking with men in the age group. The moderator first elicited participant accounts of their understanding of men’s healthy ageing, with emphasis on how each participant conceptualizes and understands their health and wellbeing. This was followed by exploring specific issues of interest. Underpinning the discussion around each question was gaining participants’ thoughts about underlying gender differences. The question sequence involved drilling down ideas and comments from general to specific. Detailed field notes were recorded to complement the audio recordings. Each focus group lasted for between 50 and 80 minutes and was recorded digitally via three audio recorders. Audio recordings were transcribed verbatim by a transcription service and checked for accuracy by the moderator.
Survey Sample Source
Access to the database of men residing in Otago and Southland was obtained from the NZ Electoral Roll (February 2021), which included information about the name, gender, date of birth, and address. Participants were screened and randomly selected from the list. Stratified random sampling was used to recruit equal numbers of men into each of four 10-year age bands (45–54, 55–64, 65–74, and 75+ years) (Lee et al., 2009).
The sample size was determined according to Dillman’s criteria for survey sample size estimation (Dillman, 2011; Needham et al., 2008). For a total population of (110,970 + 48,705) × 41.3% = 65,946 men 45 years and over resident in Otago and Southland, with a confidence level set at 95% and a ±5% margin of error, 381 participants were required. Furthermore, the sample size of 381 was also considered to be sufficient to detect over 30 independent variables in logistic regression analysis according to Peduzzi’s theory (Peduzzi et al., 1996). Assuming a 40% response rate to previous similar survey studies (Lee et al., 2009), it was estimated that the final sample would need to consist of at least 953 (381/40%) male participants.
To ensure sufficient numbers of men who indicate Māori descent, we purposively sent culturally appropriate invitation letters to Māori men. Additionally, allowing for a lower response rate from this group, we over-sampled men who indicate Māori descent in the Electoral Roll by boosting their total number by 25% of the overall sample size (Baxter et al., 2006; Clark et al., 2011). Thus, we targeted a sample of 1500 men in our study, with n = 300 for each 10-year age group, and an additional group of Māori men (n = 300). All the measures used to collect data in this survey were from standardized, validated, and commonly used instruments. The final instrument, “Men’s Health and Healthy Ageing Survey” is listed in Table S1a (supplementary document one).
Survey Pilot and Administration
Study questionnaires went through two stages of piloting including 1) expert consultations and 2) face-to-face questionnaire completion (Sørensen et al., 2013). The expert consultations ensure all the questions are culturally appropriate to both non-Māori and Māori men. In stage two, eight men were recruited to read and complete the questionnaires under the observation of three research team members. Any questions, hesitations, or mistakes were recorded. This stage was designed to examine participants’ willingness and acceptance to respond to a questionnaire of this length and help discover potentially inappropriate questions from the participants’ lens. It also ensured that the questionnaires were as relevant, concise, and clear as possible, and established the face validity of the instrument.
Participants who received the survey invitation could choose to either enter the online survey or request the paper-based questionnaires by contacting the research team. The online survey was administered using Qualtrics (Qualtrics, 2021). The mailing survey included a paper-based package of survey questionnaires, a participant information letter, a consent form, and a return prepaid envelope. Following this strategy, nonrespondents were re-contacted by sending follow-up reminders within four weeks after they received the first invitation.
Data Analysis
Qualitative data were analyzed using the reflexive thematic analysis across six stages (Braun & Clarke, 2019), and it has been published elsewhere (Xiao et al., 2021). Survey data analysis was conducted using Stata 16.0 (StataCorp LLC, 2021). Recruitment and nonrespondents were reported, and post-stratification weights were calculated based on the survey, along with the sampling weights, all analyses were weighted to be reflective of the NZ population for men. The mean substitution was used as our data was Missing Completely at Random (MCAR). Descriptive statistics in terms of means and standard deviations (SD), medians and interquartile ranges (IQR), and frequencies and percentages as appropriate were reported, along with 95% confidence intervals.
To determine the association between the men’s health themes developed from the qualitative phase and healthy ageing, multivariate regression analyses (linear for continuous outcome successful ageing; logistic for binary outcomes HRQoL) employing multivariate hierarchical models were undertaken by adjusting control variables in different models. The basic model included all men’s health themes collectively assessed individual associations of each predictor with the outcome while accounting for the potential confounding effects of other themes. The adjected model further added demographic control variables. The interaction model tested the moderating effects of men’s age (younger old vs. older old), ethnicity (Māori vs. non-Māori), and residential location (major urban vs. others) on significant associations based on the adjusted model. Likelihood ratio tests were employed to compare two models (adjusted model vs. interaction model). As a result, regression coefficients (β), p values, and confidence interval (CI) were obtained. Statistical significance was determined by two-sided p < .05.
Results
Focus Group: Themes, Subthemes, and the Integration With Survey Development
Twenty-eight men participated in the focus group study. Five face-to-face and one online focus group (two participants dropped out as they did not have access to the internet) were conducted. Participants’ ages ranged from 45 to 92 years. The sample of men (67.4 ± 11.4 years) comprised two age groups and two location groups: 15 participants were between 45–69 years (younger group; most are urban residents), and 13 were aged ≥70 years (older group; most are rural residents). Additional demographic information can be found in Table S1a of supplementary document one. While participants were largely ethnically homogenous (26 were NZ European, and two were Māori), they were heterogeneous in other ways, as they were inclined to explicitly position themselves by emphasizing their experience or age, living environment, or cultural background.
Themes and Subthemes Identified From the Qualitative Phase.
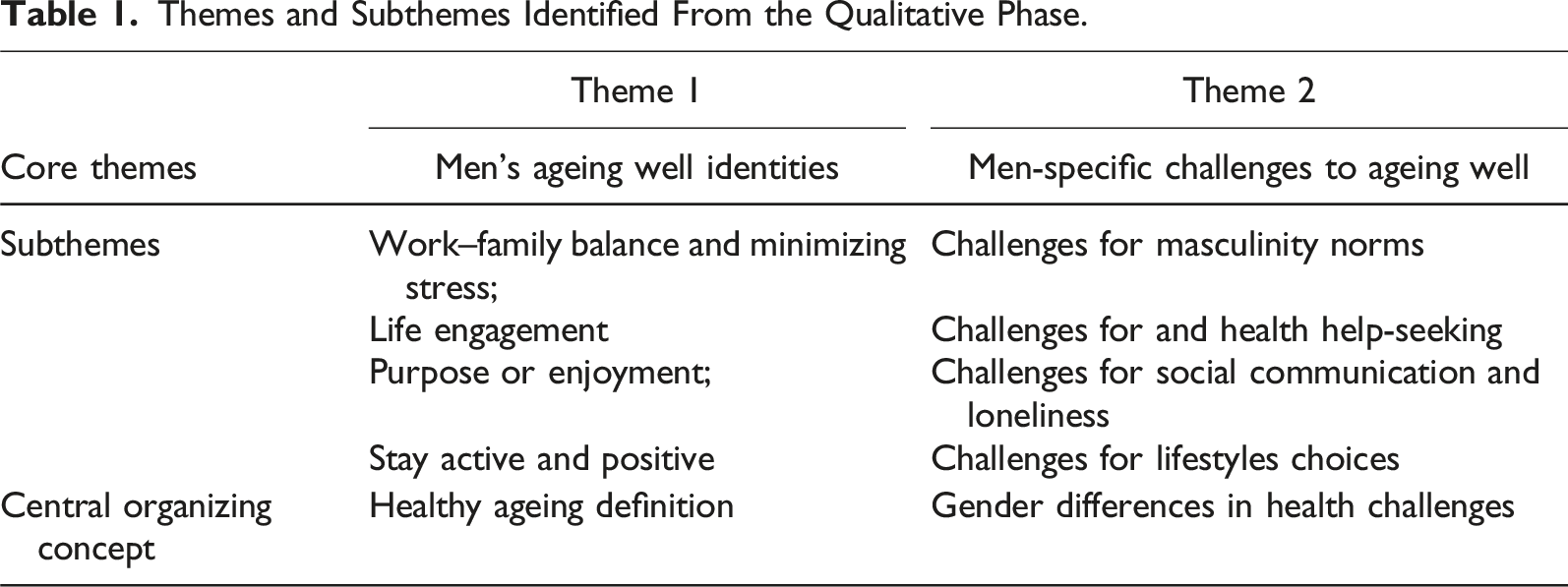
Overall, most men in the qualitative phase appeared to already have a basic understanding of the challenges to their health and wellbeing as they got older, with slightly different views across the different age and location groups, that is, beyond the simplistic view of “absence of any disease or impairment”; both older and younger men believed that life satisfaction and engagement are more important considerations. Men also understood they could lack social interaction, which may lead to both mental and physical health problems. Even so, they were not necessarily committed to developing and maintaining social engagement, or to seeking support from health services, especially in relation to their chronic health conditions and mental health issues. These participants tended to have excuses for not seeking help with their health and for their unhealthy lifestyle choices. Our findings highlight a range of health challenges and health risks that men face across the subthemes. This is instructive for indicating potential strategies to address the challenges of healthy ageing for men, as well as exploring universal and country-specific public health practices to support healthy ageing.
Survey Data: Descriptive and Inferential Statistics
Sample Characteristics
A total of 434 out of 1500 eligible responses (response rate 28.9%) were included in the final analysis. The ethnicities reported are in accordance with standard NZ ethnicity reporting (Ministry of Health NZ, 2021). Most study participants were NZ European (70.97%), and most were married (71.89%). Despite the high proportion of NZ Europeans, this was slightly lower compared to the proportion in the overall population of Otago and Southland regions (89%) - and the whole of NZ (74%) (Statistics NZ, 2015). To compensate for deficiencies in Māori men recruitment and ethnicity interactions in the qualitative phase, we oversampled Māori men. The proportion of Māori participants in our study (17.74%) was higher than the distribution of Māori at the population level (9%) (Statistics NZ, 2015). Participants’ demographic characteristics are presented in Table S1b of supplementary document one. Comparisons of the above demographic characteristics between Māori men and non-Māori men are also listed in Table S1b of supplementary document one. For the purposes of comparison, we grouped NZ European, Samoan, Chinese, Indian, and Others into the non-Māori group.
Figure 2 addresses research question one and presents the comparisons of the healthy ageing and HRQoL variables between Māori men and non-Māori groups graphically. The average score of cognitive functions was 3.12 (ranging from 1.00–5.00), with a standard deviation of .87. Men participating in our study tended to report relatively high scores for successful ageing (mean = 7.70, SD = 1.41), physical capabilities (median = 11.00, IQR = 10.00–11.00), and metabolic and physiological health (mean = 5.76, SD = 1.17). The CESD 10 Boston score was low (median = 1.00, IQR = 1.00–5.00), which suggested there was no great severity of depression symptoms among the participants. This was also reflected by the MSC score. Statistically significant differences were found between Māori men and non-Māori men in five of the six outcome variables. Overall, non-Māori men have higher scores for self-reported HRQoL, successful ageing, cognitive functions, physical capabilities, and metabolic and physiological health than Māori men. Distribution of outcome variables of statistical significance between Māori and non-Māori groups. Comparison of healthy ageing outcomes between Māori men and non-Māori men. Æ Two-sample T-tests: mean ± SD (minimum-maximum) values were reported. § Mann-Whitney U tests: median (Interquartile Range, IQR) was reported.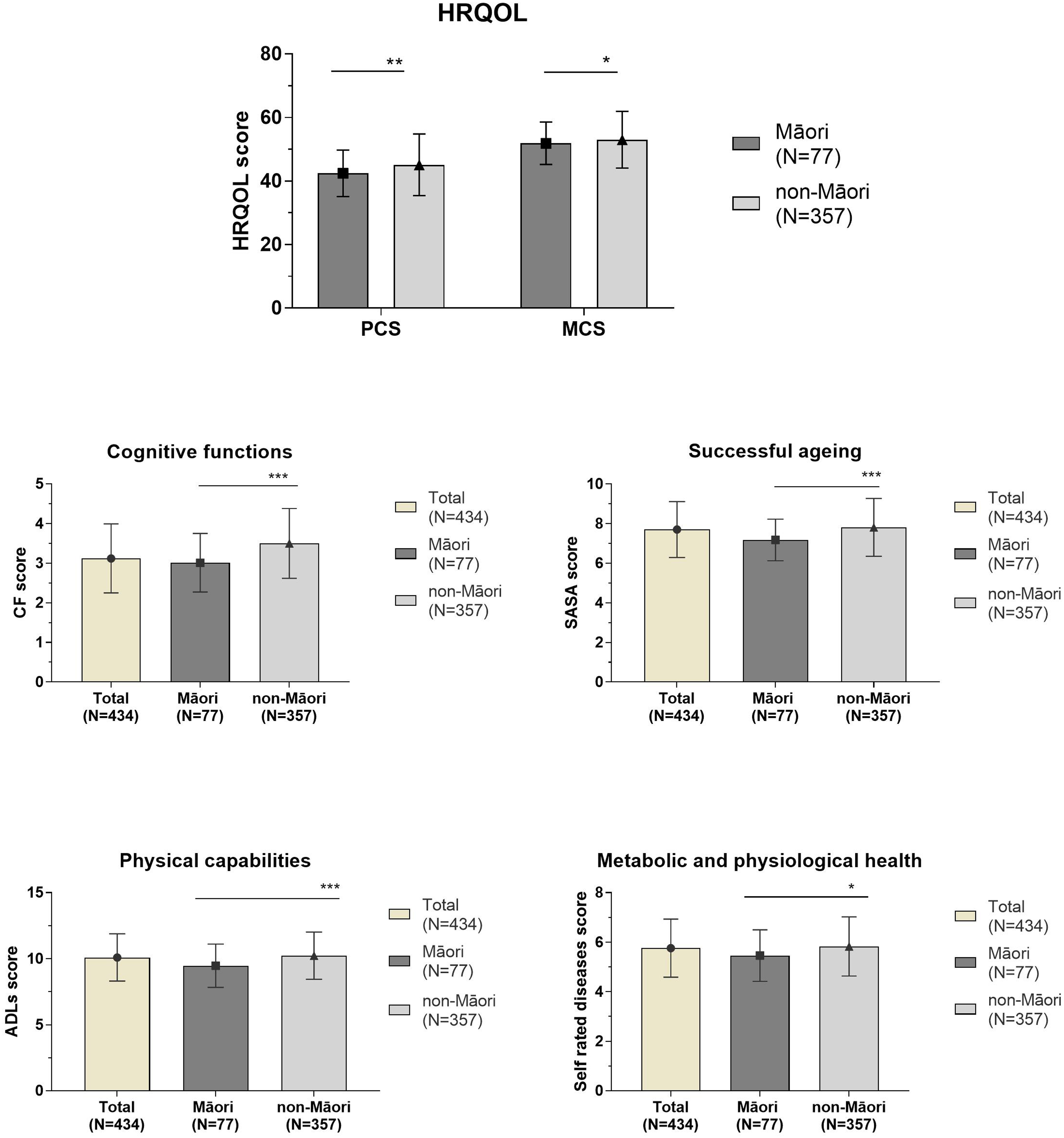
Multivariate Models
Hierarchical Regression Models for SRSA
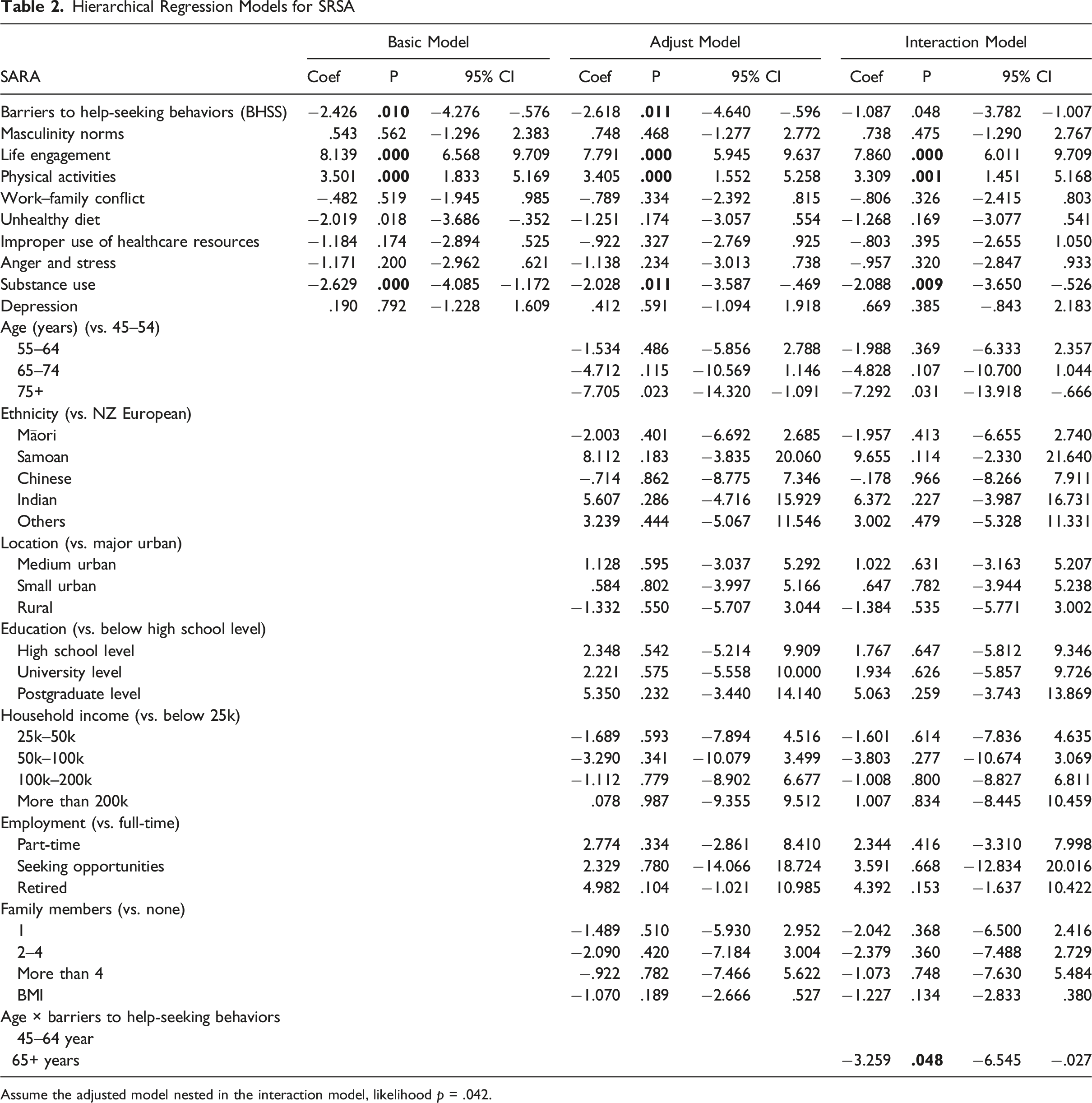
Assume the adjusted model nested in the interaction model, likelihood p = .042.
Hierarchical Regression Models for HRQoL (PCS).
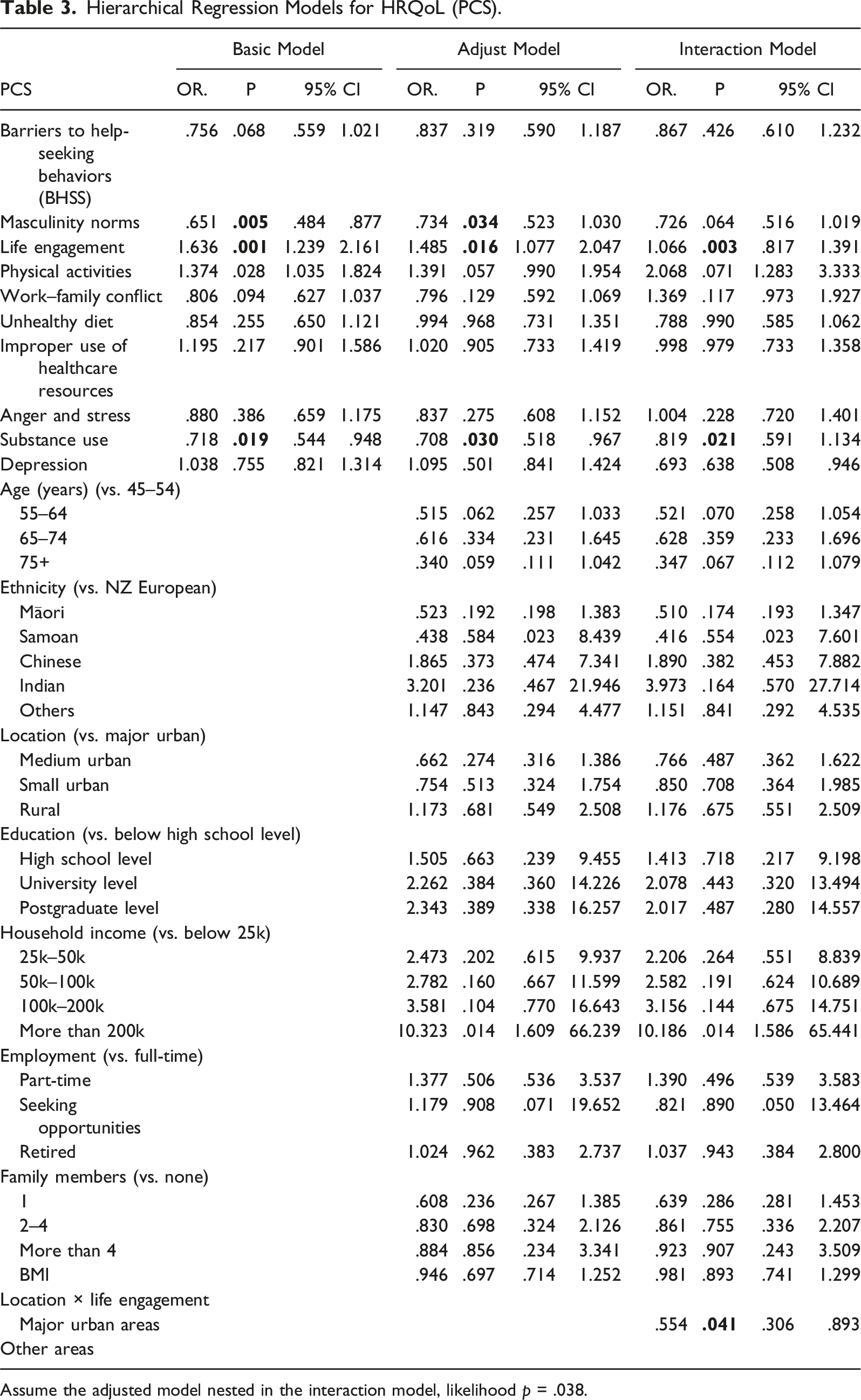
Assume the adjusted model nested in the interaction model, likelihood p = .038.
Hierarchical Regression Models for HRQoL (MCS).
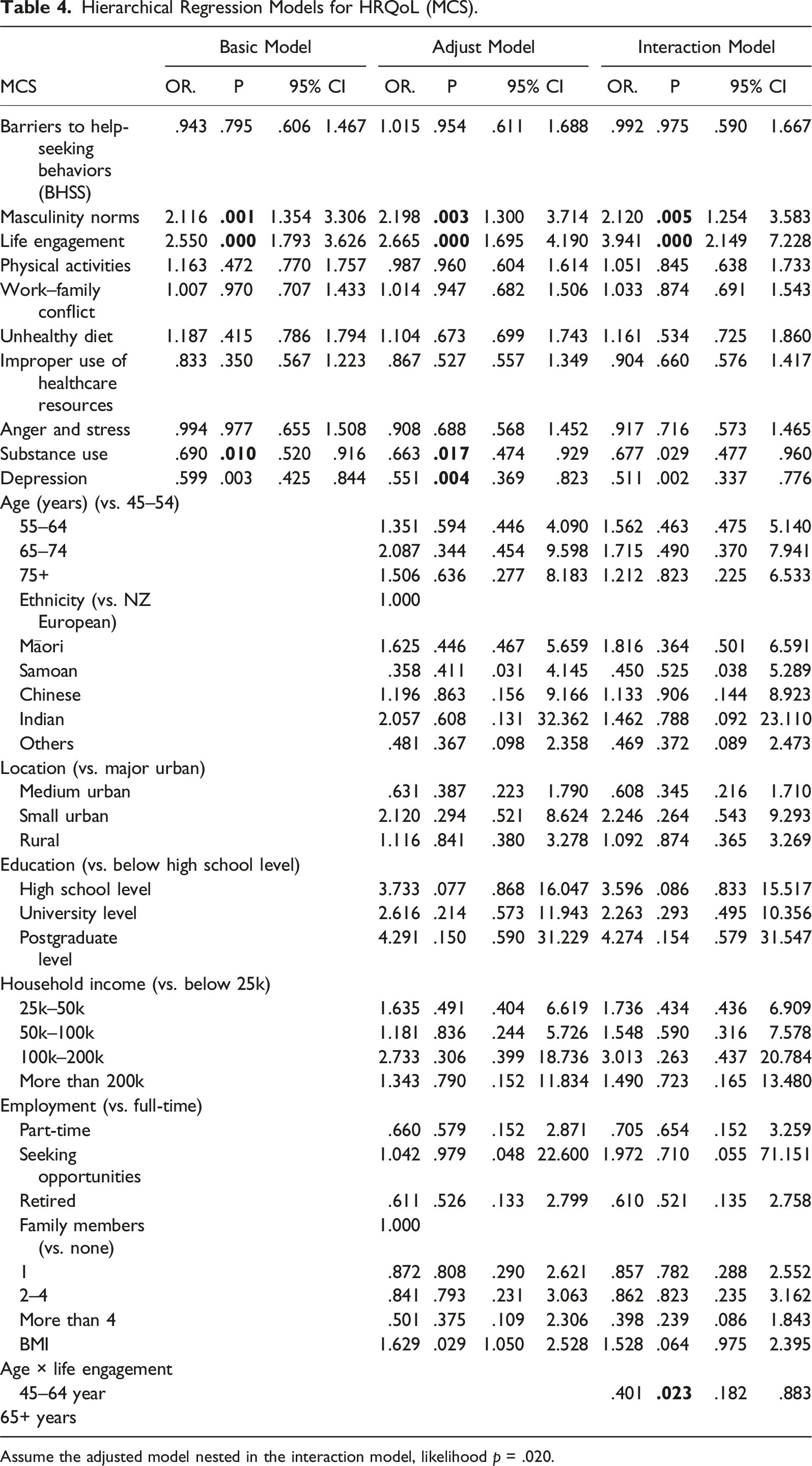
Assume the adjusted model nested in the interaction model, likelihood p = .020.
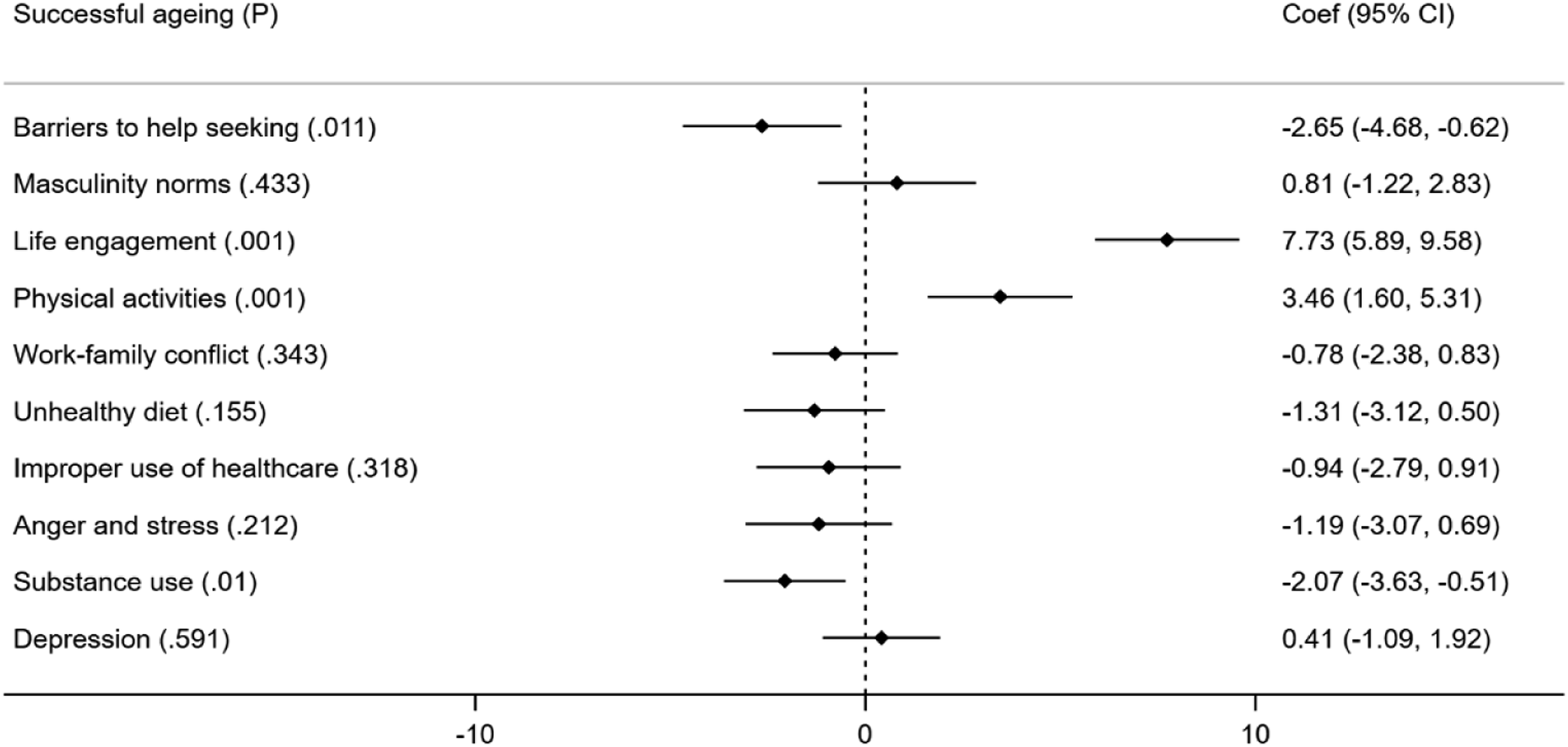
Factors influencing successful ageing.
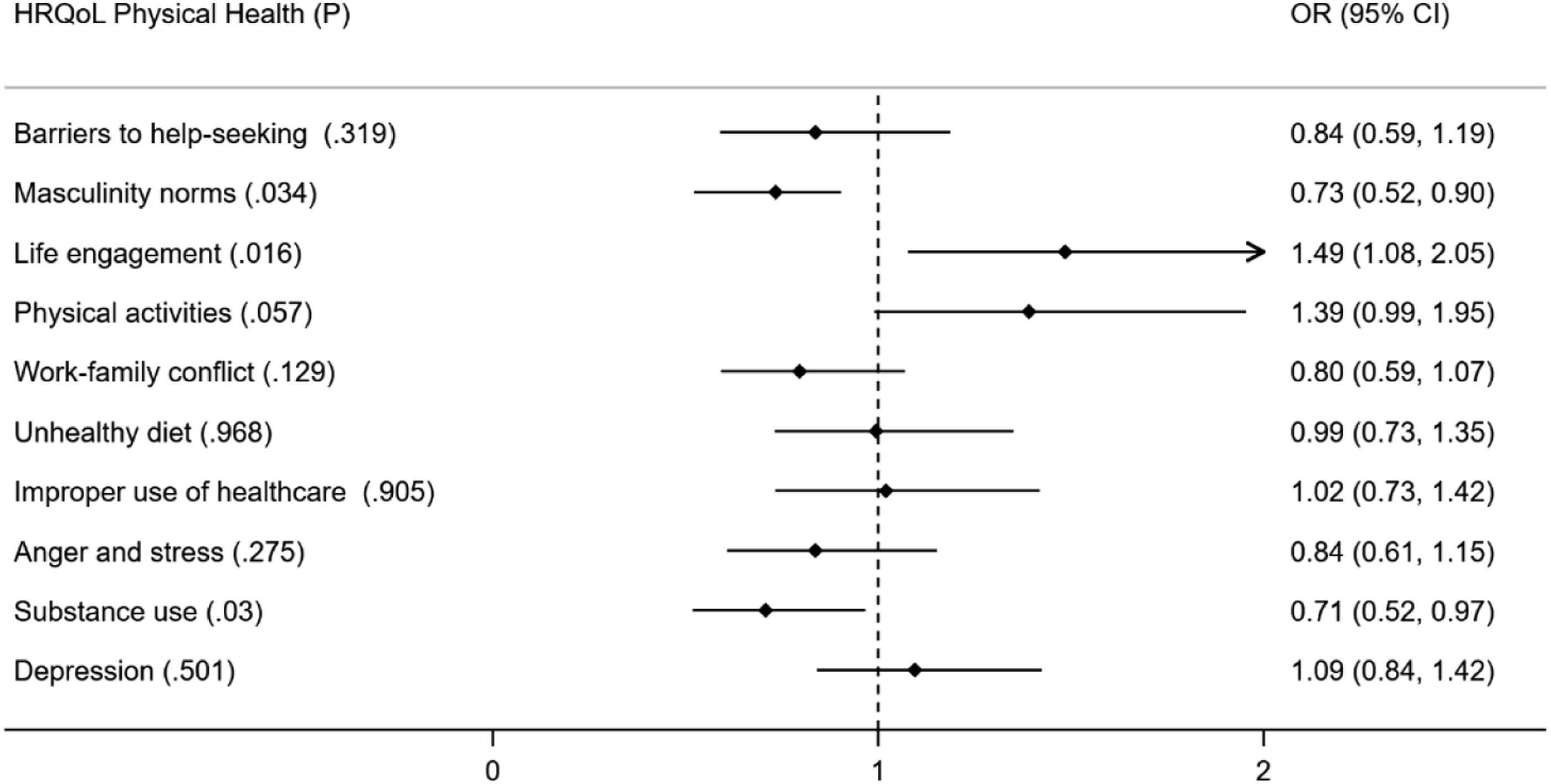
Factors influencing physical health.
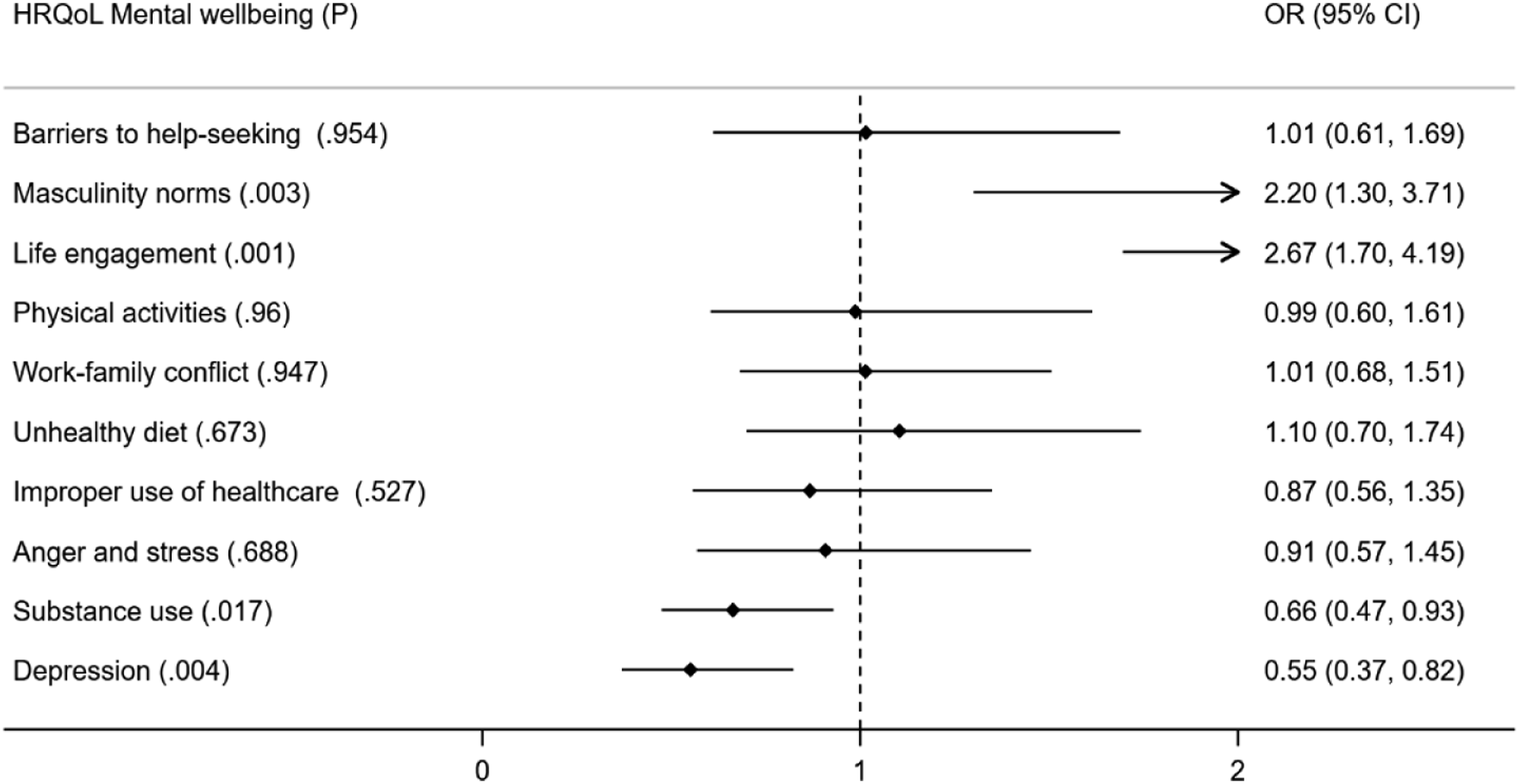
Factors influencing mental wellbeing.
Regarding the significant moderating effects in the interaction models (LRT.p < .05 in the likelihood ratio test), findings are only discussed where the relationship between the independent and dependent variable in the interaction model was consistent with the relationship in the adjusted model (same direction) and was still significant (p < .05 in the interaction model). Age was found to be a significant moderator of the relationship between BHSS and SRSA (LRT.p = .042). Interaction results show that the negative association between BHSS and SRSA was stronger for men over 65 years (β = −3.26, 95% CI = −6.55, −.03, p = .042) than for those men between 45 and 64 years. Similarly, age also modified the positive association between life engagement and mental wellbeing (OR = .401, 95% CI = .18, .89, p = .02, LRT. p = .02), whereby such association was stronger in the older group. We also found the positive association between life engagement and good physical health was modified by residential location. This association appeared to be weaker for men living in major urban areas compared to those living in other areas (OR = .55, 95% CI = .306, .893, p = .04, LRT. p = .038).
Mixed Methods Data: Integration of the Research Findings
Joint Displays of Qualitative and Quantitative Results.
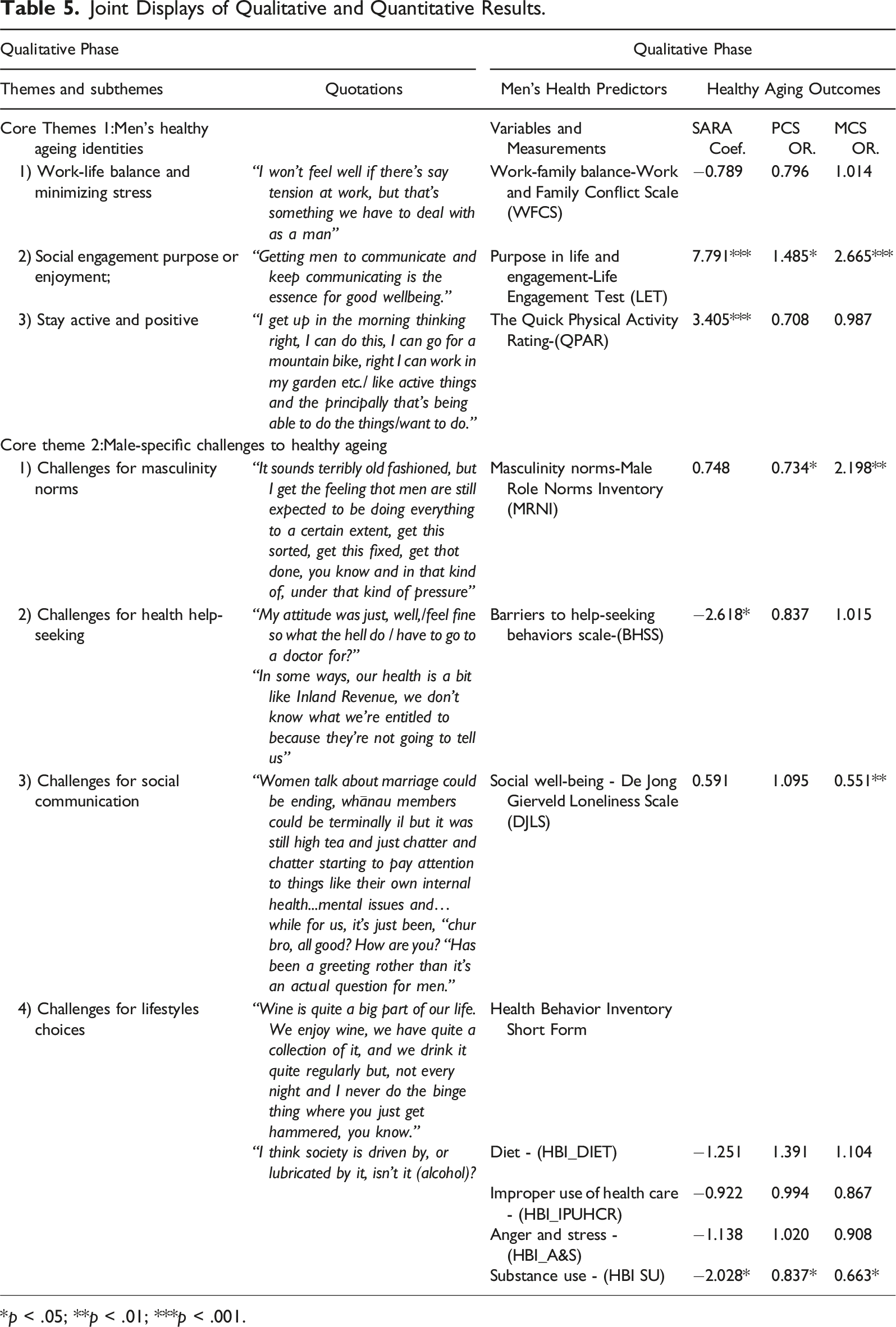
*p < .05; **p < .01; ***p < .001.
Regarding fit, the quantitative findings primarily confirmed the qualitative findings. The most significant and universal influencing factor of healthy ageing and HRQoL was found to be life engagement and purpose in life (positive influence), followed by substance misuse (negative influence) and masculinity norms (dual influence). These factors were apparent in the qualitative findings and statistically associated with healthy ageing outcomes in the quantitative findings. Work–family conflict, anger, and stress, however, were two themes in the qualitative phase but showed divergence in the quantitative results as they are not associated with either of the two outcome variables.
Some of the quantitative moderation effects (age and location) are also reflected in the qualitative data. For example, the interaction of age in the relationship between life engagement and health outcomes (stronger effect in older groups) was consistent with the focus group findings that men from older groups were more inclined to report life engagement as a fundamental and essential component of healthy ageing. In contrast, younger men had more aspects of their lives to consider including work-family balance, ill-health, and the overall environment such as climate change and the COVID-19 pandemic. Beyond this, younger men in the focus groups also claimed that there were generational differences in terms of how men acknowledge masculinity and help-seeking behaviors. They argued that there was a generational difference in awareness of traditional or hegemonic masculinity and the motivation of seeking help. This is also in line with the age interactions in the survey results, which indicated weaker negative effects of BHSS on successful ageing in the younger group, compared with that in the older group.
Discussion
This mixed methods study examined men’s expectations and experiences of healthy as they aged and explored if the factors identified by them were significant influential factors of their healthy ageing and how these differed by intersectional circumstances. Life engagement and purpose was a universally influential factor and is likely to be an independent predictor of healthy ageing among ageing males across all social contexts. Men are successful in terms of being physically active and eating a healthy diet, but substance misuse remains a significant risk factor for healthy ageing. The duality of masculinity norms was also acknowledged as it was shown in our analysis to negatively affect physical health but positively affect mental wellbeing.
Finding Implications: Contributions to Literature and Current Knowledge
This study contributes to neglected areas within the field of healthy ageing in men. Two key contributions to knowledge and wider literature have emerged. First, the results document that for older men, the most significant determinant of healthy ageing and HRQoL is life engagement and purpose. The qualitative findings revealed healthy ageing for older men was related to life purpose and feeling comfortable and enjoyable in themselves on a day-to-day basis. This was also verified as the most prominent influencing factor associated with healthy ageing and HRQoL in the subsequent quantitative phase. In line with this, previous studies have shown that life participation, engagement (Hackett et al., 2019), and networking (Fiori et al., 2006) are the key beneficial psychosocial elements of healthy ageing. The importance of being socially engaged and having purpose or enjoyment in daily life has previously been reported in an NZ cross-sectional survey (Neville et al., 2018). It indicated a significant and interdependent association between low purpose in life, poor mental health, and loneliness among men aged 60 years and over (Neville et al., 2018). The empirical research conducted on lay understandings of healthy ageing also adds to this. It has been found that older adults viewed healthy ageing as a balance between self-acceptance and self-contentedness on the one hand, and engagement with life and self-growth in later life on the other (Reichstadt et al., 2010). In effect, these findings have shifted the focus away from the conventional biomedical view of disease prevention and greater longevity as the most important components of health and wellbeing in later life. Men view their internalized life satisfaction, enjoyment, and independence as the more valuable components of healthy ageing (Fernández-Ballesteros et al., 2010).
Substance misuse was the most significant risk factor influence in healthy ageing and HRQoL in the causal models. Tobacco use, drug use, and alcohol consumption are the most common risk factors for poorer health and wellbeing, and have been identified previously in both recent and earlier works (Beaglehole, 2017; Lash et al., 1998). Generally, more men than women experience substance abuse problems in both NZ (Snijder et al., 2020) and the international context (Greaves, 2020). Despite this, consistent with the finding from the focus group study, the descriptive data showed relatively low substance misuse scores in both Māori (median = 2, ranges from 1–7) and non-Māori men (median = 1.34, ranges from 1–7). The low prevalence of reporting substance misuse may be because of the fact that participants in this study were all men over the age of 45 years old. It has been shown that fatherhood can be a turning point in men’s self-identity, impacting their future health-related behaviors (Schinkel, 2019). Ageing also encourages a “settling down for men,” leading them to become less self-centered and more giving, and helping them to achieve greater maturity and a sense of direction (Bottorff et al., 2006). Men may decrease risky behaviors not only substance misuse, but also drinking and smoking and engage in more health-protective behaviors as they age (Gordon et al., 2013).
Other concerns raised by previous studies, in terms of men’s lack of healthy help-seeking behaviors (Galdas et al., 2005), social communication (Haferkamp et al., 2012), poor mental health (Marsters et al., 2021), and self-recognition of hegemonic masculinity (Messerschmidt, 2019) appear to also represent challenges to men healthy ageing in NZ. These findings have provided convincing theoretical foundations to shift traditional stereotypes of “old age” to “healthy ageing” as a multidimensional concept. This is useful for policymakers as they capture elements of healthy ageing for men which can be considered when they are developing ageing policies in social, economic, and civic affairs, and to optimise opportunities for older men’s health and social participation. For example, rather than steering older men towards predetermined male social roles, the achievement of healthy ageing to empower older men to have life purpose and engagement should become a new expectation for policymaking.
Methodology Implications: Contributions to Mixed Methods Research
This study benefited from a mixed methods approach from several perspectives. First, men’s health and healthy ageing are complex topics, with multiple aspects. Mixed methods with abductive reasoning allow a greater comprehensive understanding of the topic and minimized the inherent biases of using a single method. The abductive approach generates plausible explanations that are supported by multiple lines of evidence or data sources. This is consistent with merging, the convergence and agreement between qualitative and quantitative results strengthen the overall validity of the integrated findings. Embracing the abductive in the mixed methods approach enables a more detailed contextualize understanding of these broad topics being explored through the use of qualitative data and the ability to better able to generalize findings through the use of quantitative data (Regnault et al., 2018). In this study, the findings of the focus groups informed the design of a larger survey and, in an iterative process, the survey results furthered the interpretation of the qualitative data.
Second, from a methodological perspective, both predictor and outcome variables were unclear before the study. One key contribution to this is adopting a mixed methods approach and incorporating the thematic analysis results to inform the causal modeling. More specifically, the ultimate regression model to answer the main research question was built on the combination of theory-driven qualitative evidence and data-driven quantitative evidence. Although the integrated mixed methods findings seem broad and less focused, they inform the potential direction of the future research agenda including a focus on more specific factors that influence healthy ageing for men.
Third, this study also contributes to mixed methods research by demonstrating how the intersectional model can be used in integrating the design, conducting, and interpreting of mixed methods research. Mixed methods approach and intersectionality have important conceptual overlaps. The similarity in terms of epistemological stance between intersectionality and mixed methods approach has been elaborated by Perry (Perry, 2009). Mixed methods researchers are concerned with the mixing of quantitative and qualitative data for diverse, converging perspectives and multiple ways of knowing. Likewise, intersectionality scholars have long focused on the mixing of interdependent identities and discriminations (Perry, 2009). Mixed methods are adopted when the research question is complex and requires answers beyond the presentation of numbers in a quantitative sense or words in a qualitative. Combining both approaches provides a more comprehensive understanding of the research question. Similarly, intersectionality is also often thought of as being the best to explore the complexity of the socio-demographics of the participants in qualitative research (Christensen & Jensen, 2012), and quantitative studies with large sample sizes to simultaneously examine the influence on variables of interest (Cole, 2009).
Fourth, the mixed methods methodology contributes to improving the understanding of intersectional identities of men’s healthy ageing. Our mixed methods analysis confirms the consistency of intersectionality in both qualitative and quantitative research regarding men’s healthy ageing issues while being cognizant of their social context. As intersectionality-informed mixed methods research, the applicability of the intersectional model has been highlighted by further examining the moderating effects of age, location, and ethnicity. Including these intersectional contexts in the mixed methods study may allow us to uncover nuances in men’s healthy ageing across the life course, including during the important period of men’s social life transitions.
Overall, the intersectional perspective highlights a more comprehensive and complex picture of men’s healthy ageing rather than just dichotomous categorizing it as either “good” or “bad.” For example, we found that men from older groups were more likely to be affected by BHSS (as a risk factor) and life engagement (as a protective factor) to their successful ageing. Correspondingly, they were less likely to be affected by masculinity norms (as a protective factor) on their risk of depression, compared with men from the younger group. Masculine identities among men must therefore consider the effect of ageing as well as other factors such as ethnicity and location when exploring its relationship with health and wellbeing. This is a particularly important finding if we are to accurately reflect the ways in which ageing males negotiate their mental wellbeing, help-seeking, and health service use. The ways men negotiate and sustain, as well as move away from, traditional hegemonic masculinity may change as they age, given most older men defined healthy ageing in terms of positive life satisfaction with activated purpose and engagement.
Limitations
Since we have conducted a single intersectional analysis with an emphasis on age, location, and ethnicity. Double or multiple intersections are needed to further explore the differences and similarities across age plus ethnicity and location groups. Further studies are recommended using large national data sets (fit the sample size requirement of multiply intersection analysis), which can shed light on how help-seeking behaviors might differ among superimposed groups of men (e.g., urban older men vs. rural younger men). Meanwhile, to fully address the intersectionality of men’s healthy ageing issues, other potential interactions, as shown in the outermost circle of Figure 1, sexual orientation, religion, and disability also require further considerations. It would be valuable if future qualitative research focused on how to engage minority men including ethnic minority, sexual minority men, migrant men, disabled men, and men who live in poverty.
The cross-sectional survey design was appropriate as the research questions aimed to determine influential factors at one point in time. The limitation of the cross-sectional study design has been acknowledged as it is only able to provide associations between men’s health predictors and healthy ageing outcomes, but it has limited implications for causal inference. Evidence is also needed on the mediating effects, for example, help-seeking behaviors could be the mediator between masculinity norms and mental health as masculinity norms may affect help-seeking behaviors (Staiger et al., 2020) and help-seeking behaviors may affect mental health (Mackenzie et al., 2008) (indirect effect). We recommend that future research should be conducted using an iterative or longitudinal design using a time-dependent receiver-operating characteristic (ROC) curve to assess the predictive abilities of identified risk factors for healthy ageing indices (Kamarudin et al., 2017).
This research does not claim to have established a “correct” single metric, but it sought to find appropriate ways to separately measure each domain of healthy ageing. The outcome variables HRQoL and successful ageing reflex the health status of ageing males but may not fully cover all domains of healthy ageing. For example, some men in our study indicated positive health outcomes in one domain but negative in another. Future researchers could try to cluster the similarities based on the health indicator of each domain, to identify distinct groups of participants. This may be achieved by unsupervised machine learning (hierarchical clustering) to discover unknown subgroups across different variables (James et al., 2013). This advanced technology could be applied appropriately in the future to measure healthy ageing in men multidimensionally and precisely by visualizing observations with measurements on a set of features.
Conclusion
Overall, our findings extend the sparse literature related to men’s health in NZ and suggest men’s narratives and responses to healthy ageing and HRQoL were classed, cultured, and structured by differences in a social context, thus, highlighting the importance of intersectional and interactional analysis in the field of men’s healthy ageing. The identification of the most influential indicators of healthy ageing in men is instructive for exploring country-specific public health practices to support the health and wellbeing of older males. The integrated mixed methods findings will be useful for policymakers to capture key elements of healthy ageing in men when they are updating the New Zealand Healthy Ageing Strategy and when they develop a men’s health policy. This project also provides new knowledge to help guide the development of mixed methods research programs with a focus on how such determinants contribute to men’s health needs in their ageing process. Ultimately this project supports the quest to improve men’s health by addressing the significant determinants of their healthy ageing.
Supplemental Material
Supplemental Material - Intersectional Perspective on Factors Influencing Healthy Ageing Amongst Older New Zealand Men: An Exploratory Mixed Methods Study
Supplemental Material for Intersectional Perspective on Factors Influencing Healthy Ageing Amongst Older New Zealand Men: An Exploratory Mixed Methods Study by Hui Xiao, Fiona Doolan-Noble, Alan White, Wentian Lu, Lizhou Liu, and G. David Baxter in Journal of Mixed Methods Research
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.