
Abstract
Mixed methods research offers a unique opportunity to advance understanding of a phenomenon. However, practical guidance on the use of mixed methods to develop theoretical frameworks is limited. We present a novel adaptation of the Pillar Integration Process (PIP) to support development and refinement of a theoretical framework explaining the processes by which healthcare factors influence cancer survivors’ quality of life. Deductive integration of quantitative and qualitative data, guided by an a priori conceptual model, illuminates the nuances of the relationship between the concepts of interest, producing a theoretical framework, the Model of Healthcare factors influencing Quality of Life in Cancer Survivorship (MoHaQ-CS).
Keywords
Introduction
Mixed methods research (MMR) has an advantage over quantitative or qualitative research in its potential to produce knowledge that is unavailable in either method alone (Creswell and Clark, 2017). However, there is often a failure to adequately integrate the findings of MMR to realize their full potential (O'Cathain et al., 2007). The products of integration are the meta-inferences drawn from combining quantitative and qualitative results, yielding a more complete understanding of a research problem (Creswell and Clark, 2017). However, in sequential MMR studies, quantitative and qualitative data analysis are often undertaken and presented sequentially, potentially compromising the development of meta-inferences (Bazeley, 2018).
Theoretical frameworks are essential drivers of empirical research, linking concepts and variables to understand complex phenomena, based on established and emerging evidence (Hammer et al., 2019). Theoretical frameworks provide schemas to situate the research problem, guide the selection of data collection instruments and support the development of complex health interventions and services (Hammer et al., 2019). However, discussion of the theoretical bases of research is often not sufficiently visible in the development, implementation, evaluation or reporting of complex interventions, limiting evaluation and evidence synthesis (Cuthbert et al., 2019). Underutilization of theoretical frameworks in the field of implementation science has been attributed to users’ knowledge, confidence, skills and experience with their use (Lynch et al., 2018).
Development and refinement of theoretical models are traditionally based on literature reviews and qualitative methodologies, with testing and validation via predominantly quantitative methods (Kivunja, 2018). However, MMR offers a unique opportunity to comprehensively evaluate and refine theory to advance understanding of a phenomenon, representing a high standard of integration in MMR. However, practical guidance in the use of MMR in the advancement or development of theoretical frameworks is limited (Evans et al., 2011).
This paper presents the adaptation of the Pillar Integration Process (PIP) (Johnson et al., 2019) to support the development and refinement of a theoretical framework to explain the processes by which healthcare factors may influence colorectal cancer (CRC) survivors’ QoL, the Model of Healthcare factors influencing Quality of Life in Cancer Survivorship (MoHaQ-CS). PIP advocates for an inductive approach to analysis; in the first stage, raw data are listed in separate quantitative and qualitative columns. In the second stage, the data is matched through a process of coding and categorizing similar qualitative and quantitative data in a joint display. In the third stage, the data and categories of the joint display are checked for completeness, ensuring data are appropriately matched, and no raw data could provide an appropriate match for identified gaps in the joint display. In the fourth and final stage, Pillar Building is conducted through comparison and contrast of findings developed through the listing, matching and checking of data. Here, we present an alternative, deductive approach to PIP, guided by the Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life.
Study Background
A primary goal of healthcare is to optimize an individuals’ QoL. Follow-up care is an integral part of life after cancer treatment, to identify symptoms of potential cancer recurrence and support recovery and management of long-term side-effects (Institute of Medicine, 2006). Despite the importance of follow-up care for physical and psychosocial recovery, there is little understanding of how the experience of healthcare may affect cancer survivors’ well-being, including access, continuity, outcomes of and satisfaction with care (Drury et al., 2017; Sisler et al., 2012).
CRC survivors experience a range of distressing physical, psychological and social issues which may impact their well-being for many years after cancer treatments (Drury et al., 2017, 2021). Cancer survivors require high-quality survivorship care to support recovery and adjustment to chronic physical, psychological and social issues after cancer. However, the organization of healthcare services tasked with survivorship care are complex, encompassing many variables, involving multiple healthcare providers, in often fragmented care pathways spanning several organizations (Gordon et al., 2012; Sisler et al., 2012; Snyder et al., 2008). Furthermore, surveillance for cancer recurrence may be prioritized above the management of survivorship issues in some circumstances (Di Fabio et al., 2008; Tofthagen, 2010). As a result, cancer survivors may experience a range of unmet information and supportive care needs affecting their QoL (Cheng et al., 2016; Hallett et al., 2014).
QoL and perceptions of well-being are unique to each person, influenced by individual values, expectations and culture (World Health Organisation Quality of Life Group, 1995). While healthcare is recognized as a determining factor in cancer survivors’ QoL outcomes, few QoL models explicitly acknowledge the broader healthcare context. The Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life has been developed and tested with ethnically and culturally diverse samples of breast and cervical cancer survivors. However, the models’ focus on and basis in cancer survivorship and the recognition of healthcare as influencing QoL outcomes, alongside demographic, socio-ecological and cultural factors means it provides a comprehensive framework to explore factors placing cancer patients and survivors at greater risk of experiencing poorer QoL (Ashing-Giwa and Lim., 2008, 2011). To date, few studies have attempted to advance understanding of the interaction between healthcare experiences and QoL outcomes. To ensure complex interventions are responsive to the supportive care needs and QoL of cancer survivors, a comprehensive theoretical framework is required. We present the MoHaQ-CS, which describes the processes by which healthcare systems may influence QoL outcomes among cancer survivors.
Methods
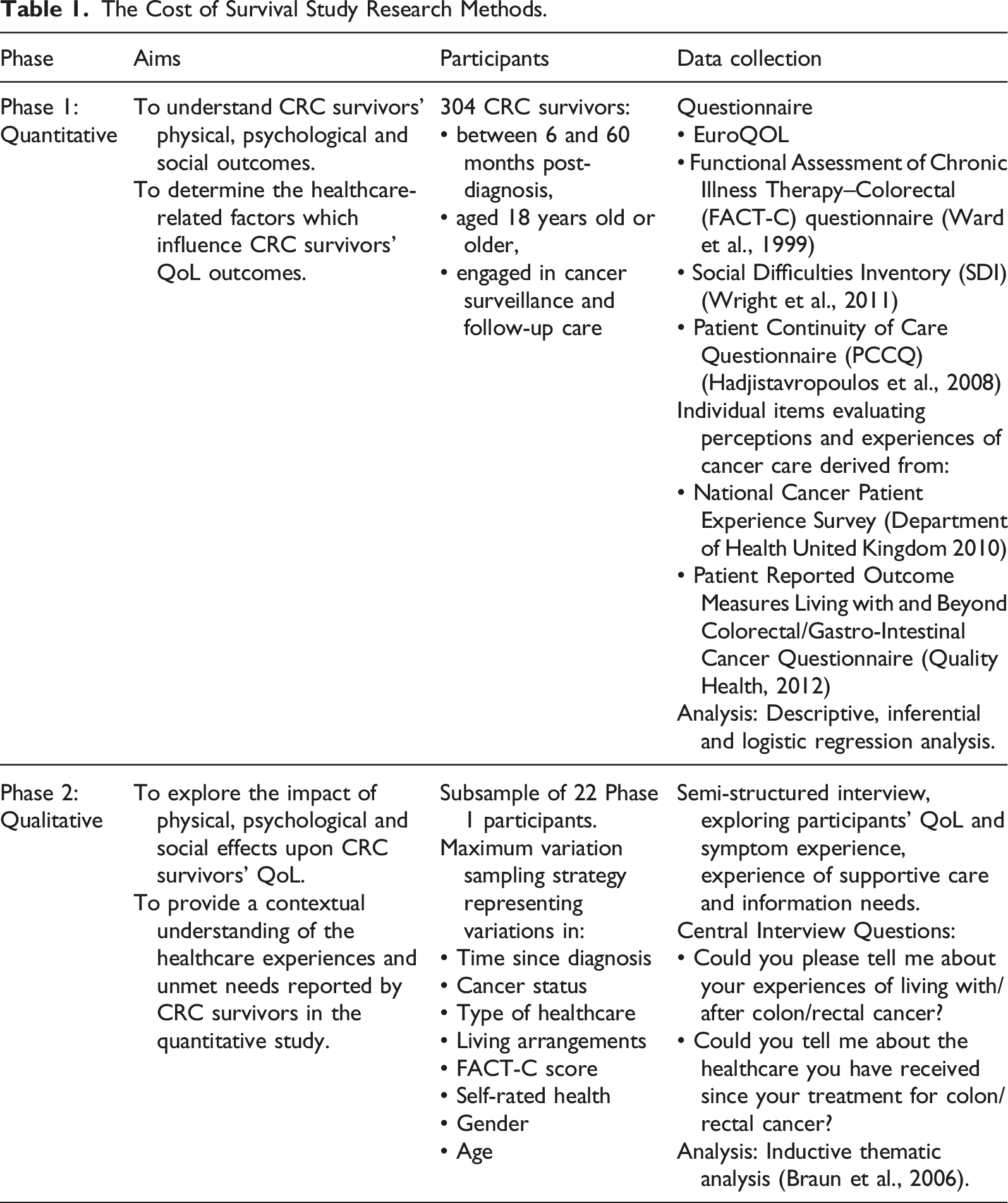
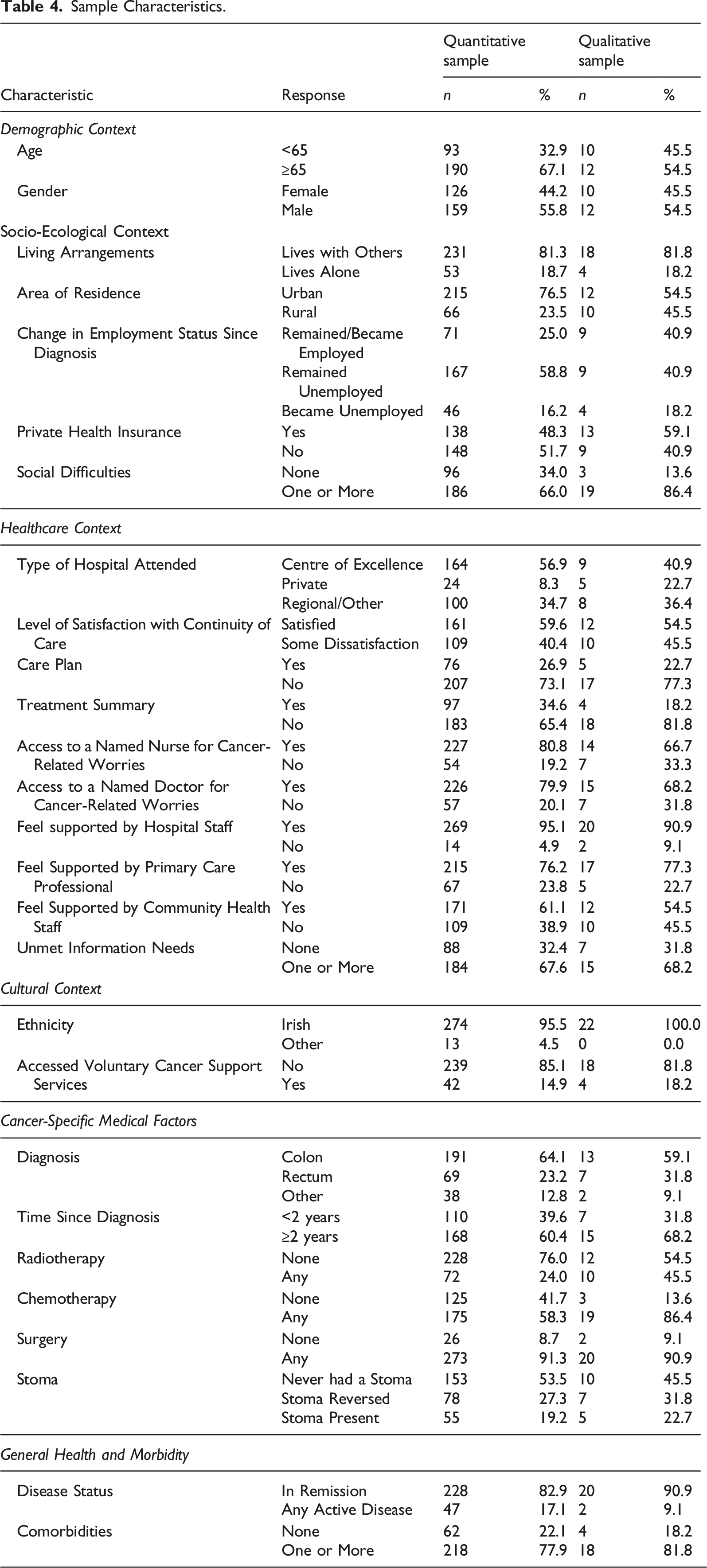
The MoHaQ-CS was developed based on the integration of quantitative and qualitative phases of The Cost of Survival Study, a pragmatic mixed methods sequential explanatory study exploring the healthcare factors associated with CRC survivors’ QoL (Figure 1). The design and methods of each phase of the study are reported elsewhere (Drury et al., 2020a, 2020b, 2021). Table 1 summarizes the aims, sampling and data collection methods utilized within each phase of the study. Participants of the study were CRC survivors of any disease stage, between 6 and 60 months post-diagnosis, aged 18 years old or older and actively engaged in cancer surveillance and follow-up care in Ireland. 304 CRC survivors were recruited to the quantitative phase from public and private hospitals and voluntary cancer support centres (response rate = 75.6%). For the qualitative phase, a subsample of 22 consenting survey participants (n = 238, 92.2%) were invited to participate in semi-structured interviews using a maximum variation sampling strategy to ensure representation of key demographic, health and healthcare-related variables associated with CRC survivors’ QoL outcomes in the quantitative phase of the study (Table 1). During the quantitative phase, participants completed subjective measures of QoL with established validity and reliability with English-speaking samples of CRC survivors (Table 1) (Sisler et al., 2012; Ward et al., 1999; Wright et al., 2011). Semi-structured telephone interviews were conducted with CRC survivors to explore their experiences of cancer survivorship and the perceived impact of cancer-related care upon their QoL. The Cost of Survival Study Mixed Methods Sequential Explanatory Study Design. The Cost of Survival Study Research Methods.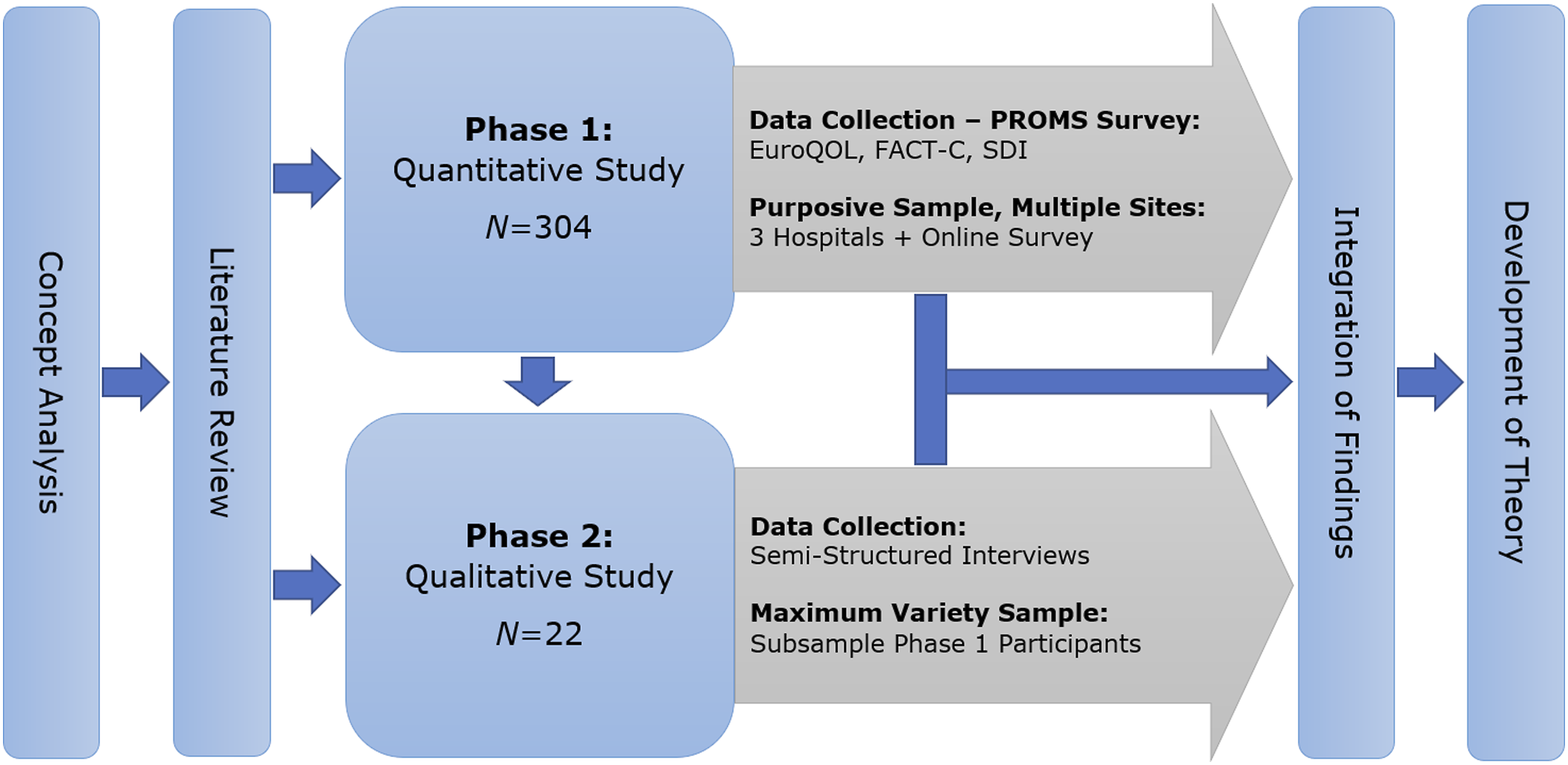
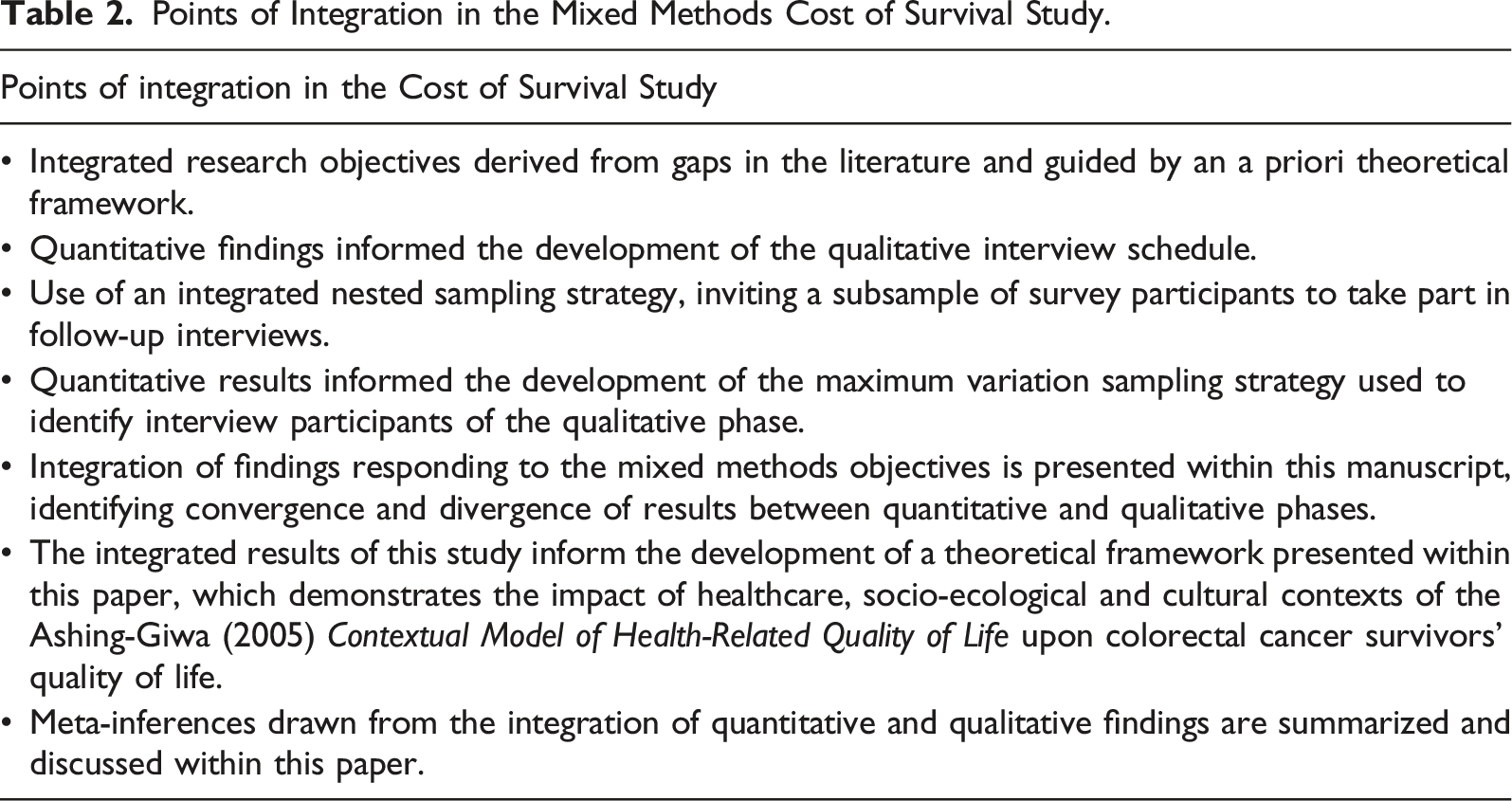
Points of Integration in the Mixed Methods Cost of Survival Study.
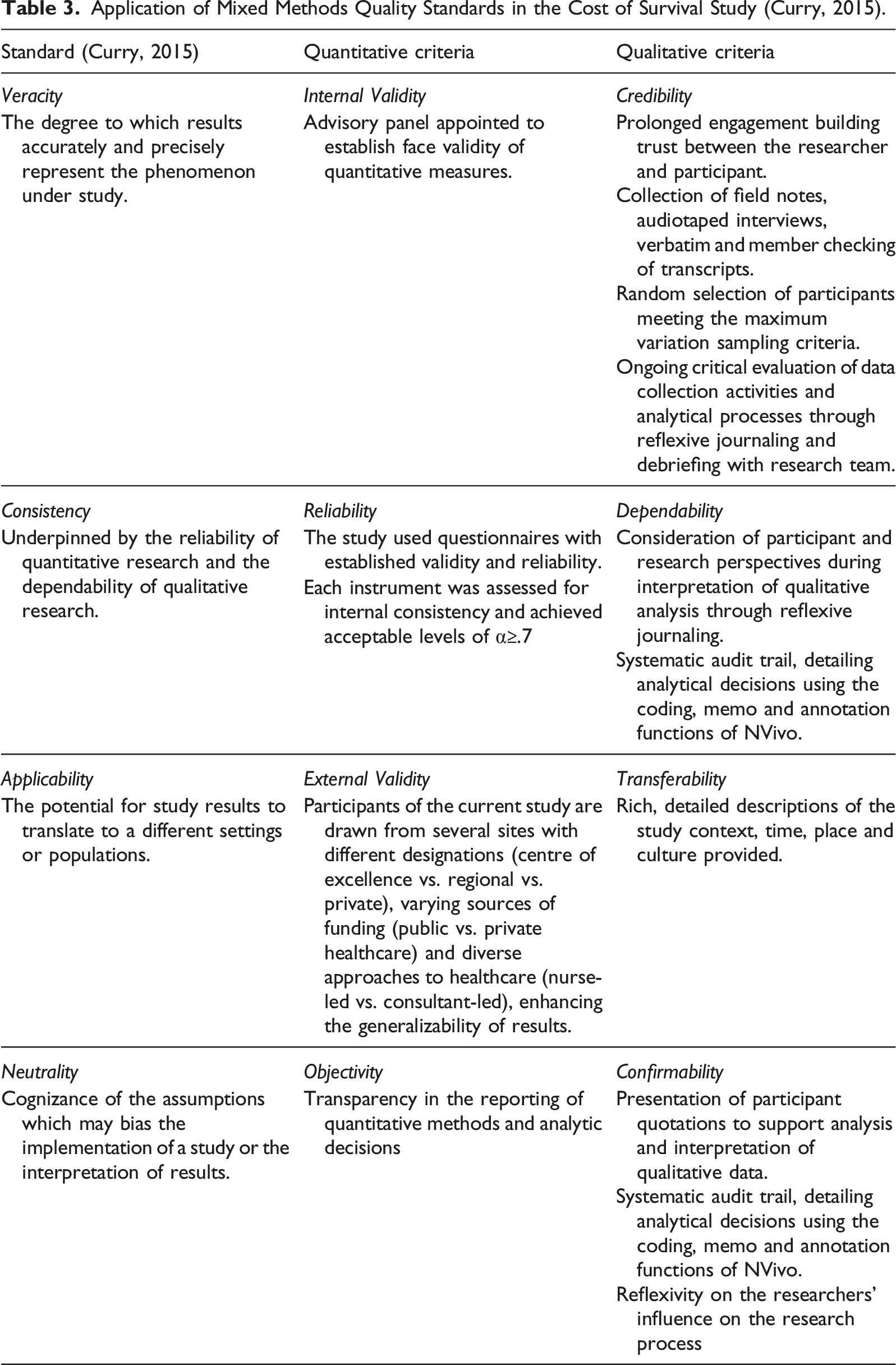
Application of Mixed Methods Quality Standards in the Cost of Survival Study (Curry, 2015).
Data Analysis and Integration
The approach to data analysis and integration within this study was iterative, whereby quantitative and qualitative data were analysed sequentially, and subsequent integrated analysis was guided by a modified, deductive PIP (Figure 2) (Johnson et al., 2019). Stages 1–3 of the 4-stage PIP were conducted deductively, whereby the domains of the Contextual Model of Health-Related Quality of Life provided the pillars of analysis. In the first stage of the modified PIP, raw quantitative and qualitative data and key findings were listed. In stage 2, the contents of the quantitative and qualitative lists were matched to the pillar domains of the Ashing-Giwa (2005) model, and in stage 3, they were checked for completeness and appropriate matching. In the fourth and final stage, Pillar Building, the joint display was analysed to formulate meta-inferences which provide a more comprehensive understanding, explanation and context of the healthcare factors influencing CRC survivors’ QoL. This analysis enabled the generation of a visual illustration of the MoHaQ-CS, demonstrating the processes by which cancer-related healthcare factors may influence cancer survivors’ QoL, moderated by individual and macro/systemic domains of the Ashing-Giwa (2005) Model. Modified Pillar Integration Process adapted for the Cost of Survival Study Study.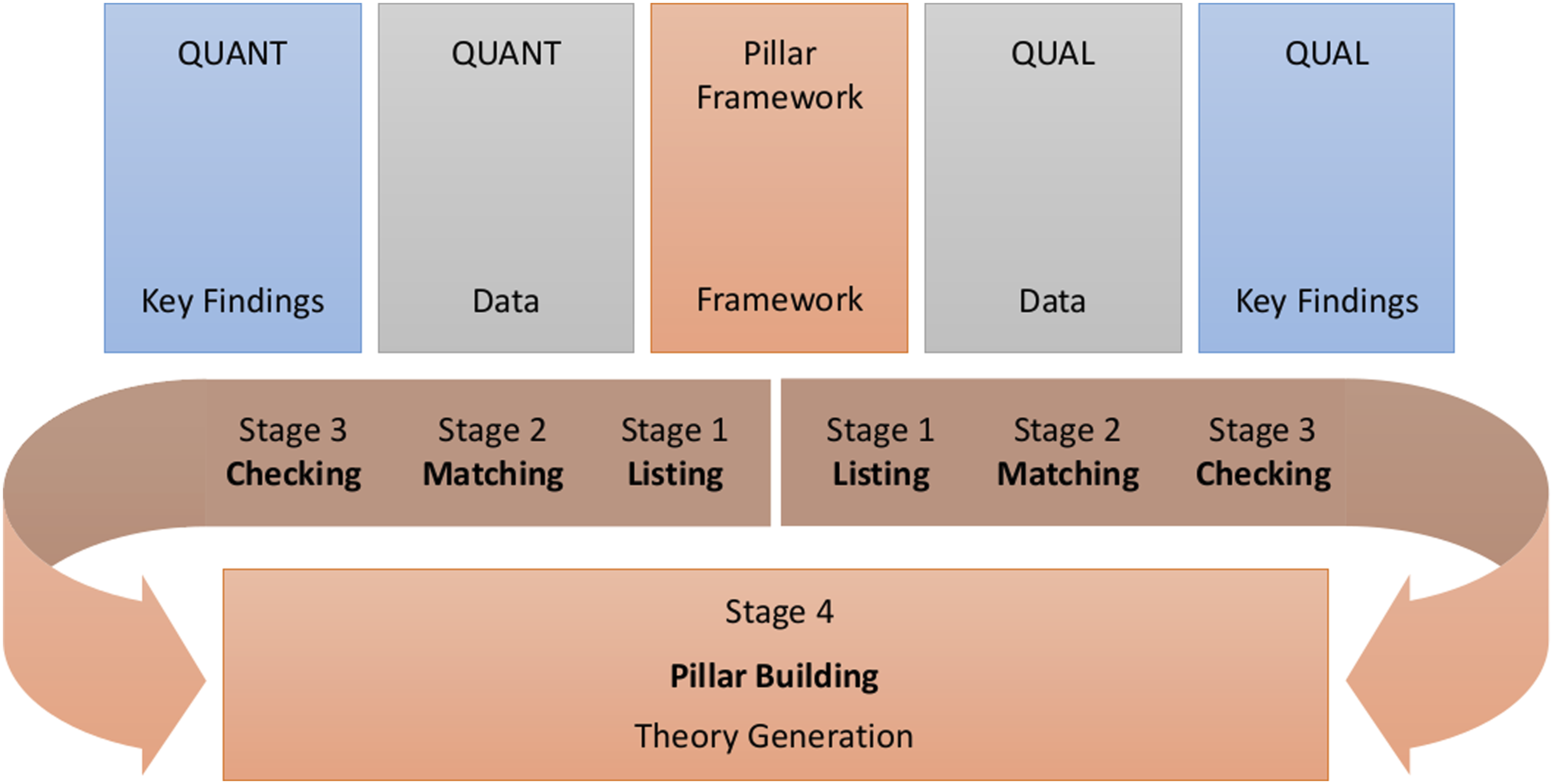
Results
Sample Characteristics
Sample Characteristics.
Integrated Findings
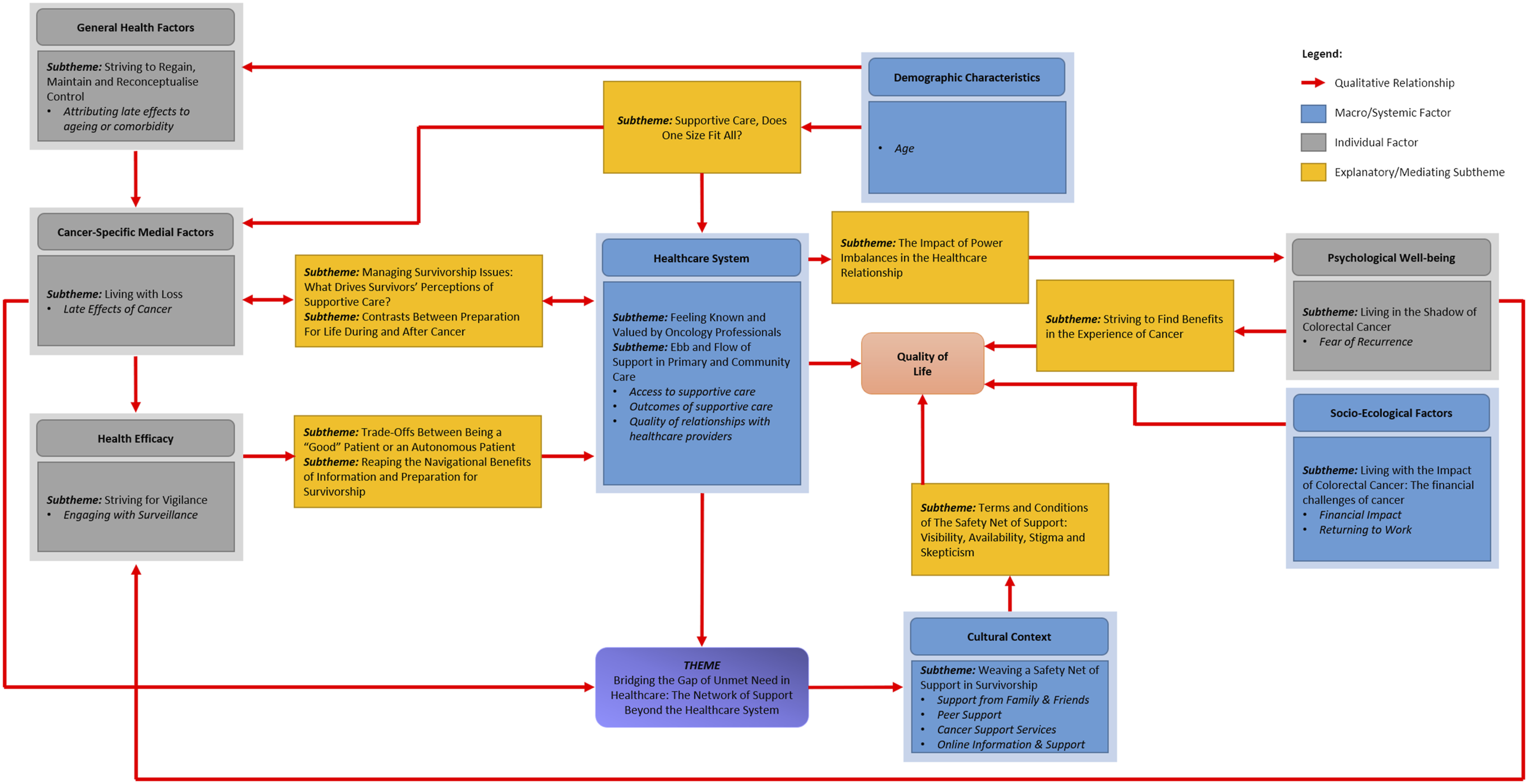
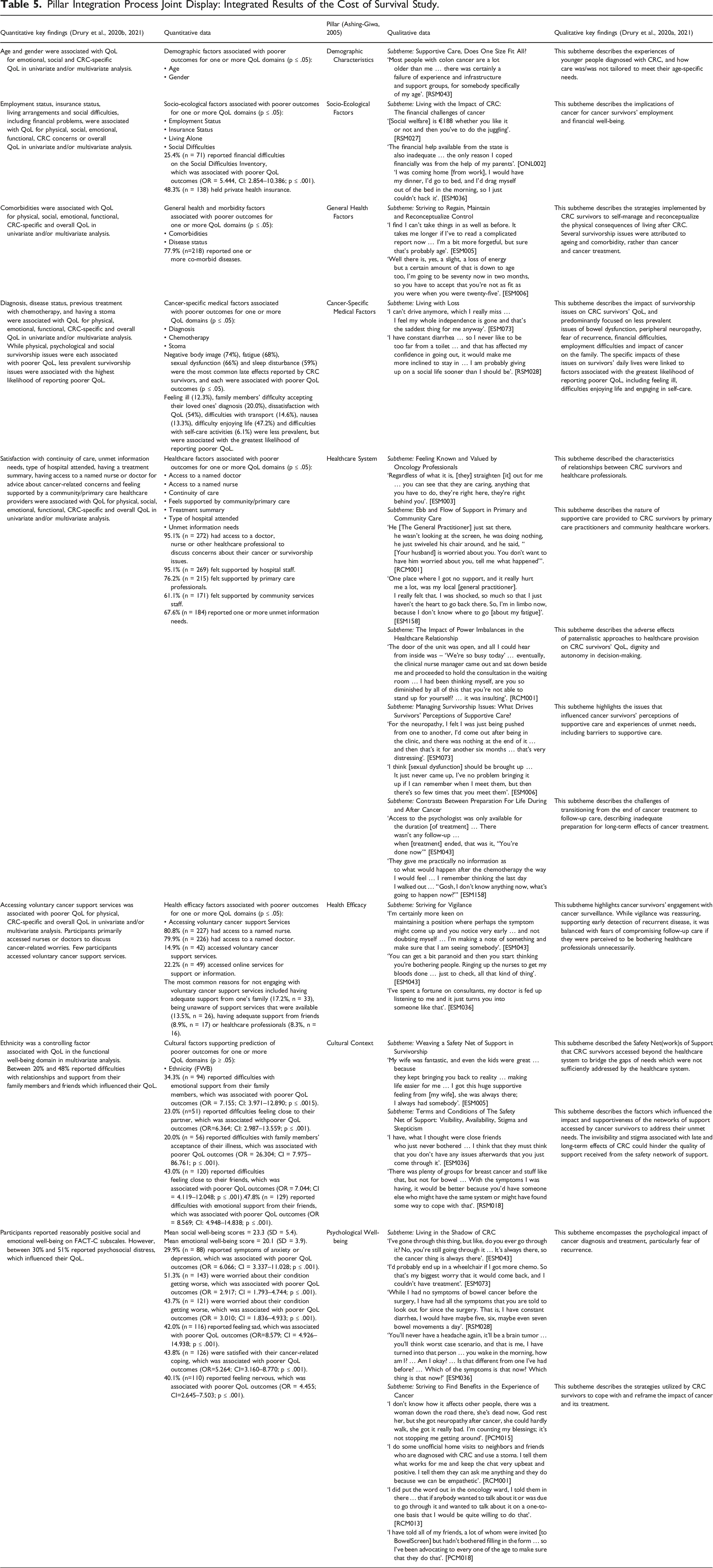
The quantitative and qualitative findings each aligned with the core domains of the Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life during initial sequential analysis of each dataset. The regression models developed in the quantitative phase fit with Ashing-Giwa’s conceptualization of QoL, highlighting the importance of demographic, socio-ecological, healthcare and cultural contexts in predicting CRC survivors’ QoL (Figure 3). The qualitative findings support and extend these results, suggesting that formative healthcare experiences, particularly failures in relational, informational and management aspects of continuity of care during diagnosis and treatment may continue to adversely affect QoL, even 5 years after diagnosis (Figure 4). Quantitative and qualitative data were subsequently integrated following the modified PIP process (Table 5), which are thematically summarized below. Quantitative factors associated with colorectal cancer survivors’ quality of life outcomes, grouped according to the domains of the Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life. Conceptual map of qualitative of factors influencing colorectal cancer survivors’ quality of life outcomes, grouped according to the domains of the Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life. Pillar Integration Process Joint Display: Integrated Results of the Cost of Survival Study.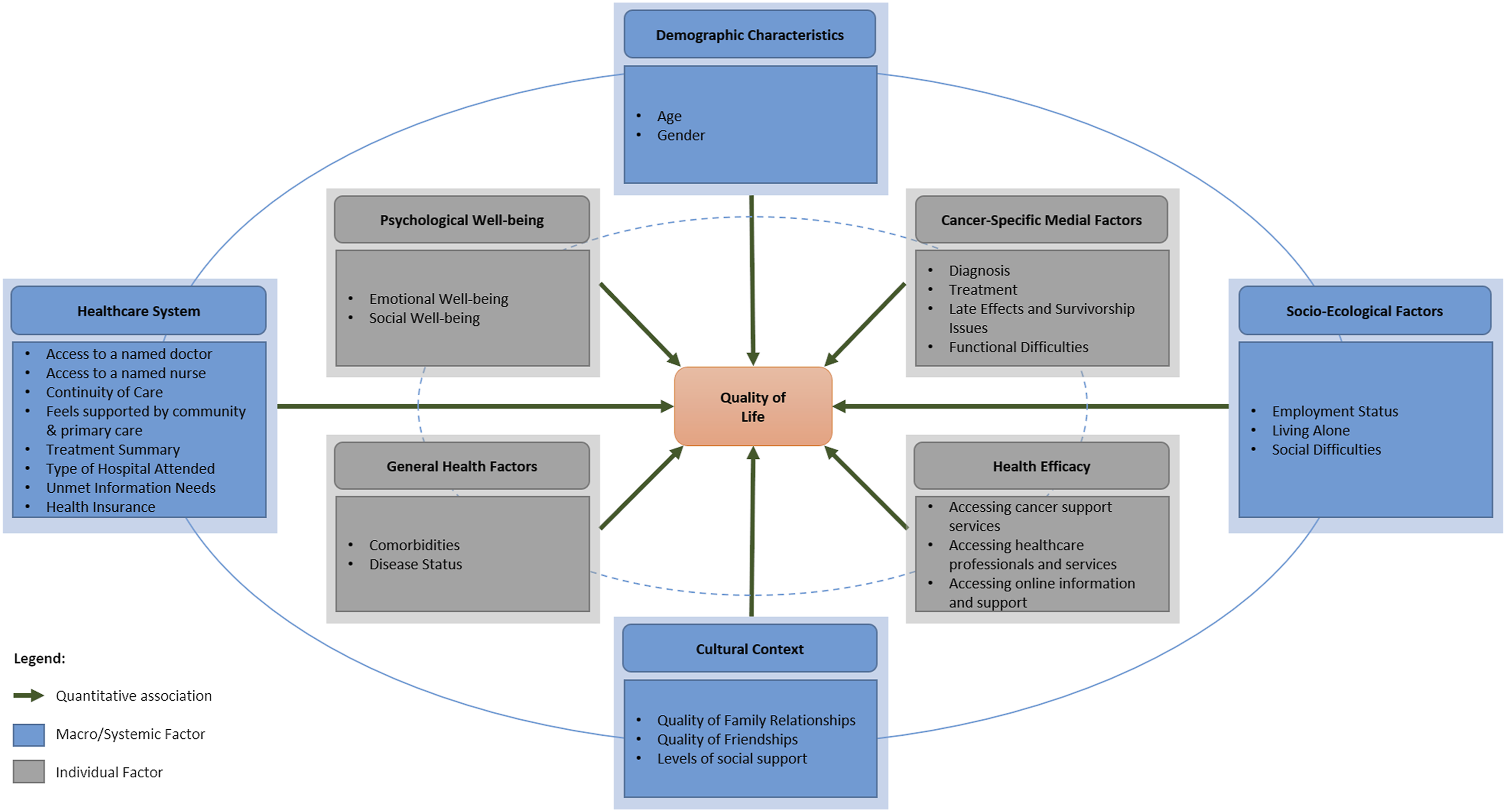
Demographic Characteristics
The quantitative and qualitative findings converged regarding the impact of age on QoL. Younger CRC survivors consistently reported poorer emotional, social and CRC-specific well-being. This finding was supported and explained by the findings of the qualitative phase, where younger CRC survivors described age-related disparities in care, as services were designed to address the needs of an older age group who were more likely to be diagnosed with CRC. As a result, younger survivors felt their cancer-related needs related to their life stage were not addressed, and limited supports were available beyond the health system.
Socio-Ecological Factors
Socio-ecological factors are comprised of socio-economic status, social support and life burden, where daily stressors compromise a persons’ ability to cope with unanticipated circumstances. Quantitative and qualitative results converged to quantify and explain the financial impact of cancer which persisted beyond the period of treatment. Financial difficulties were associated with poorer QoL and were reported by one-quarter (25.7%) of questionnaire participants. Interviews highlighted difficulties survivors experienced in returning to work and shortcomings in financial support available from social services.
General Health Factors
Within the general health domain, health and comorbidity are important considerations in modelling cancer survivors’ QoL outcomes. Converging quantitative and qualitative findings indicate that comorbidity and disease status were associated with poorer QoL. However, qualitative data described the confounding effect of ageing and comorbidity upon QoL. In particular, cancer survivors attributed survivorship issues such as fatigue, changes in cognitive function and sexual dysfunction to the process of ageing or comorbid conditions.
Cancer-Specific Medical Factors
Aligning with the Ashing-Giwa model, diagnosis, disease status and previous treatments were each associated with cancer survivors’ QoL in multivariate analysis. Regarding the long-term effects of cancer and its treatment, quantitative and qualitative data converged, describing the direct link between survivorship issues and cancer survivors’ QoL outcomes. While physical, psychological and social survivorship issues were each individually associated with poorer QoL, quantitative analysis suggested functional decline and social upheavals reported by a small number of participants were associated with the highest likelihood of reporting poorer QoL. These difficulties included feeling ill (12.3%), difficulties with self-care activities (6.1%), dissatisfaction with QoL (54%), difficulty enjoying life (47.2%) and family members’ difficulty accepting their loved ones’ diagnosis (20%).
During interviews, CRC survivors’ narratives provided an enhanced understanding of how less prevalent survivorship issues mediated the relationship between physical symptoms attributed to cancer treatments and QoL. Participants’ narratives focused on the impact of survivorship issues, with issues related to peripheral neuropathy, bowel dysfunction, fear of recurrence, financial toxicity, employment difficulties and impact of cancer on the family identified as common sources of functional difficulty and psychosocial distress. Survivors described how survivorship issues impacted on multiple domains of their QoL and contributed to their feeling unwell, feeling dissatisfied with their QoL and having difficulties with independence and enjoying life, which they attributed to greater psychological distress and social isolation.
Healthcare System
Healthcare system factors include access to healthcare, quality of healthcare and quality of relationships with healthcare professionals. The quantitative and qualitative data converged to confirm, explain and expand understanding of the impact of healthcare systems on CRC survivors’ QoL outcomes. Continuity of care was a consistent predictor of CRC survivors’ QoL. Although health insurance was associated with differences in QoL outcomes, cancer survivors did not describe any differences in perceptions of access to or support from healthcare professionals in the post-treatment period based on their health insurance status or location of care (public vs. private healthcare systems) during qualitative interviews.
Healthcare professionals were described as accessible, and 95.1% of participants (n = 272) had access to a doctor, nurse or other healthcare professional to discuss concerns about their cancer or survivorship issues. However, characteristics of the relationship between participants and healthcare professionals in various settings could influence QoL, including the quality of relationships, feeling known and supported by healthcare professionals and feeling informed about the long-term implications of cancer and its treatment. Feeling supported by primary and community care professionals was associated with physical well-being in multivariate analyses, but fewer participants reported support from these sources (61.1%–76.2%) compared to hospital-based professionals (95.1%). Qualitative data suggested that access to support from primary and community care professionals was inconsistent. For participants who received support from primary or community care professionals, psychosocial support from these professionals was of greatest significance and value to CRC survivors. While quantitative data suggested that specialist oncology professionals were accessible to cancer survivors, several survivors described difficulties accessing supportive care to address physical effects of cancer treatment. Perceptions of support from specialist oncology professionals appeared to be influenced by the location of care, resources available and whether pathways to access support were direct to the professional or indirectly through another service or referral.
Health Efficacy
Within the Ashing-Giwa model, health efficacy manifests as survivors’ health practices and engagement with healthcare services. Quantitative and qualitative data converged to quantify and explain patterns of health and support service utilization within the sample. The quantitative phase identified multiple sources of information and support to address cancer-related concerns; the majority of participants had access to a nurse (80.8%) or doctor (79.9%), who represented the primary sources of information and support. Few participants accessed voluntary cancer support (14.9%) or online information or support (22.2%). Having access to a named doctor was associated with more positive CRC-related well-being and overall QoL in multivariate analysis, while having access to a named nurse was associated with more positive emotional well-being. Notably, feeling supported by hospital staff was not associated with QoL outcomes in multivariate analysis. Meanwhile those who accessed voluntary cancer support services were more likely to report poorer physical, CRC-specific and overall QoL.
Qualitative data provided an enhanced understanding of the factors driving survivors’ engagement with healthcare, voluntary and online support services. Survivors expressed a desire to be both compliant with the recommendations of healthcare professionals and also autonomous, exercising their knowledge of their condition to self-manage survivorship issues and make decisions about their care. Many participants endeavoured to self-manage survivorship issues and self-navigate the healthcare system and avoid contacting healthcare professionals unless absolutely necessary. Qualitative data suggested that survivors’ experiences of late effects contributed to unmet information and supportive care needs, which were mediated by survivors’ perceptions of accessibility, supportiveness and continuity of healthcare services, which in turn affected QoL.
Cultural Context
The cultural context of the Ashing-Giwa model focuses on ethnicity, language, social networks and quality of family and social relationships. Qualitative data provided greater insight to the mechanisms by which healthcare system factors and health efficacy factors could influence QoL. Family members, friends and communities were central to participants’ well-being and feeling supported. Cancer survivors who described experiencing unmet needs and shortcomings in healthcare services attempted to address these needs, describing networks of support they developed beyond the healthcare system. These networks of support encompassed family members, social networks and cancer peers and were conceptualized as a safety net(work), which bridged the gap of unmet needs.
Narratives regarding support from family members were overwhelmingly positive. However, support from wider social networks, voluntary services and online supports were subject to terms and conditions and cultural barriers. Integration of quantitative and qualitative data identified some divergence in experiences of accessing and using the safety net(work) of support. While qualitative data suggested familial support was unconditional, quantitative data in contrast, revealed that in reality, many survivors experienced difficulties with the quality of relationships and nature of support from their family members (20.0% and 34.3%, respectively). More than two-fifths of questionnaire participants described difficulties with the quality of relationship and nature of support received from friends (43.0% and 47.8%, respectively). Qualitative data highlighted barriers to support from social networks, including the invisibility of CRC, as its treatment did not manifest outward indicators of a cancer diagnosis such as alopecia or significant weight loss.
Voluntary and peer cancer support services were not widely accessed by questionnaire participants (14.9%). Quantitative data suggested that accessing voluntary and online support services was affected by the survivors’ cultural context, including the accessibility and local availability of services, levels of support from family, friends and wider community. Qualitative and quantitative data converged, confirming and further explaining how cultural factors could further influence survivors’ utilization of voluntary, peer and online services. Stigma associated with discussion of bowel dysfunction, visibility of survivorship issues, availability of supports in local communities and scepticism of online resources limited the range of supports available to cancer survivors and their openness to seeking support from social networks and generic cancer support services.
Psychological Well-being
Psychological well-being is concerned with psychological functioning and the experiences of psychological distress, depression and anxiety. While quantitative data suggested cancer survivors experienced reasonably positive psychological and social well-being, between 30% and 51% of survivors described psychological issues related to fear of recurrence, anxiety and depression. Convergent qualitative data highlighted the complexity of cancer survivors’ fears and emotional distress and the factors driving their fears. Fear of recurrence was described as one of the most difficult to manage survivorship issues, driven by fears of reliving the experience of cancer, of difficulties differentiating between symptoms of recurrence and non-threatening symptoms, and the potential for living with worsening effects of cancer treatments. However, qualitative data contained rich descriptions of the strategies cancer survivors used to cope with and derive benefit from the experience of cancer. Several survivors compared themselves to others with more complex illnesses; others described altruistic motivations for providing support to others affected by cancer. In deriving benefits from the experience, survivors consistently described the positive impact of cancer on the closeness of relationships within families.
The Model of Healthcare Factors Influencing Quality of Life in Cancer Survivorship
The meta-inferences yielded from PIP analysis underpin the The Model of Healthcare factors influencing Quality of Life in Cancer Survivorship (MoHaQ-CS).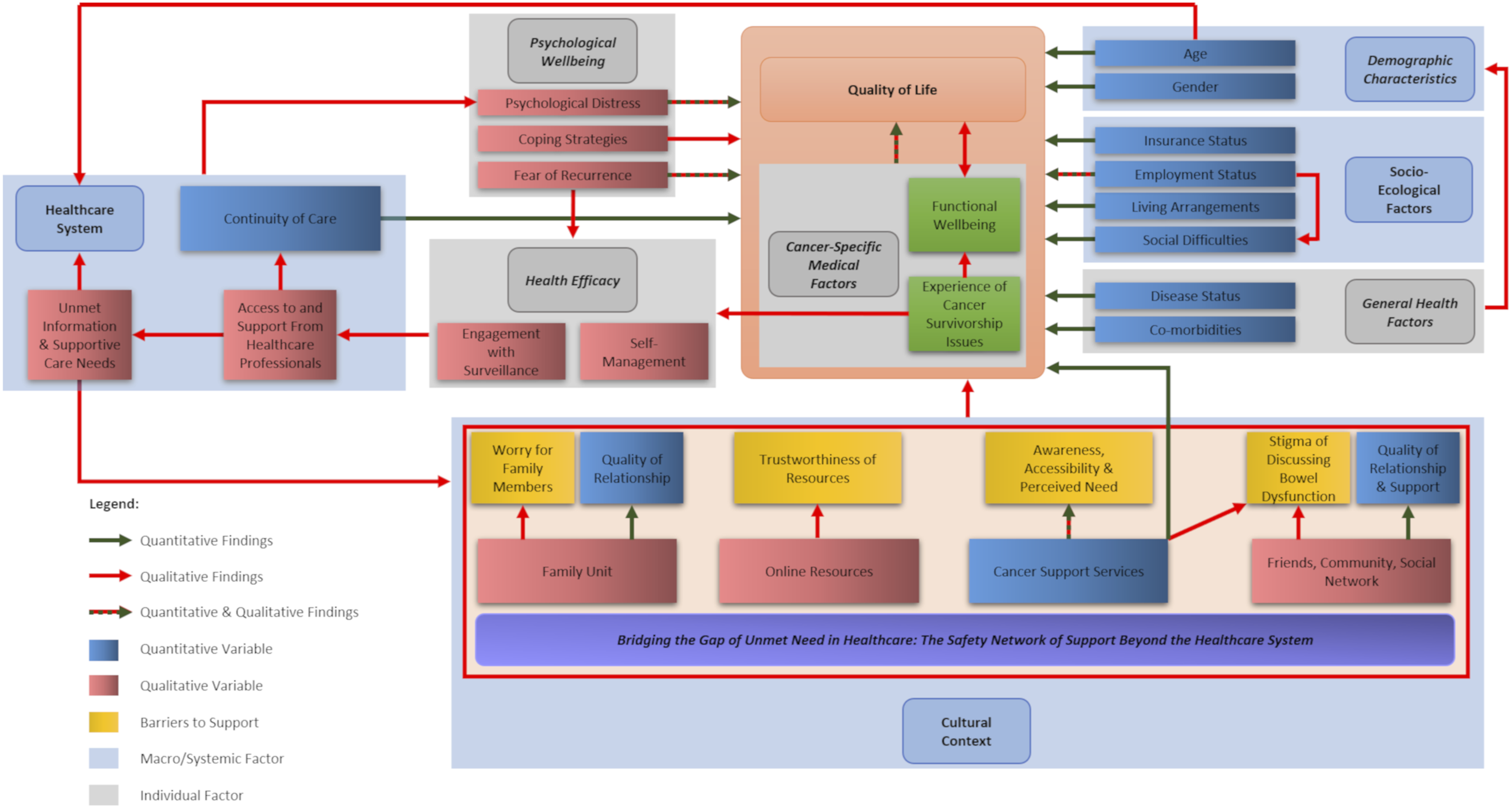
For some survivors, their encounters with the healthcare system did not meet their expectations for support, and these encounters contributed to psychological distress, arising from interpersonal interactions or perceived shortcomings in support. Where the support received from healthcare services was inadequate, this manifested and exacerbated unmet information and supportive care needs. In these circumstances, survivors sought further support beyond the realms of formal oncology healthcare services to address unmet needs. Survivors attempted to Bridge the Gap of Unmet Need through a Network of Supports Beyond the Healthcare System, encompassing their family members, their social network, cancer advocacy services and online resources. However, the nature of the Network of Supports Beyond the Healthcare System were dependent upon the cultural context in which the individual resided and received healthcare, as beliefs relating to survivors’ acculturation, interconnectedness and worldview could hinder access to psychosocial support. Survivors’ ability to cultivate a support network directly and indirectly influenced QoL. Positive experiences of support from support networks could positively affect QoL and provide practical support or information to self-manage late effects. However, even where survivors identified sources of support, the accessibility and effectiveness of this support could be influenced by the quality of relationships, worries about burdening or distressing others, social stigmas about the discussion of embarrassing late effects, difficulties discerning the trustworthiness of online resources, lack of local cancer support services specific to CRC or a belief that cancer support was not required.
Discussion
The MoHaQ-CS represents the processes by which healthcare factors may influence CRC survivors’ QoL. The joint display (Table 5) illustrates the integration of quantitative and qualitative findings to address the study aim, in line with recommended approaches to integration (Creswell and Clark, 2017; Guetterman et al., 2015). The adapted model incorporates the quantitative factors which predicted CRC survivors’ QoL within the domains of the Ashing-Giwa Contextual Model of Health-Related Quality of Life (Figure 3). The qualitative findings confirm, explain and extend understanding of the statistical factors influencing QoL, identifying the pathways by which healthcare experiences may directly and indirectly affect cancer survivors’ QoL (Figure 4).
Contribution to the Field of Mixed Methods
This paper adds to the methodological discourse of MMR, illustrating the use of an explanatory sequential MMR design to build and test a theoretical framework, the MoHaQ-CS, responding to a reported gap in the literature (Evans et al., 2011; Kivunja, 2018). Using an established conceptual model to guide exploratory research can support the development of new and more nuanced understanding of complex phenomena; this knowledge may subsequently support the development of interventions and services which can more effectively respond to the needs of people living with chronic diseases (Lynch et al., 2018). Moreover, use of an a priori conceptual model, integrated throughout the study from conception, through design, analysis and interpretation has been found to support integration in MMR (Evans et al., 2011). The Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life was selected to guide this study as it could support an exploration of the complex factors which may influence QoL in cancer survivorship, including those derived from the healthcare context of particular interest to this study. The Ashing-Giwa (2005) model informed key decisions in the design of this study, including the selection of methods, the sampling strategy and data collection methods and provided a framework for sequential and subsequent integrated analysis of quantitative and qualitative data.
The PIP is a systematic and replicable technique to support integration and visualization of MMR data (Johnson et al., 2019). The implementation of PIP in this study has been modified, adopting a deductive analytical approach which leverages the use of a theoretical framework to guide The Cost of Survival study. PIP has enabled a more nuanced understanding of the variables driving QoL outcomes in cancer survivorship. Integration of qualitative and quantitative findings in this study supported expansion of the Ashing-Giwa (2005) model, for the first time, explaining the pathways by which healthcare systems may affect cancer survivors’ QoL and identifying factors which may potentially confound analysis of QoL outcomes among this population.
Integrating quantitative and qualitative data deductively following PIP illuminated contextual and cultural factors directly and indirectly influencing QoL outcomes. The process of centring the domains of the Ashing-Giwa (2005) model as pillar concepts ensured that analysis remained focused on the relationship between the concepts of interest, healthcare systems and QoL, enabling comparison and contrast between quantitative and qualitative data to illuminate the nuances of the interaction between these concepts. While the product of this study, the MoHaQ-CS, maintains the core domains of the Ashing-Giwa (2005) model, results of this study suggest that self-management skills and cultural context, specifically, the availability, accessibility and effectiveness of support, are critical drivers of healthcare utilization, unmet needs and consequently, QoL in cancer survivorship.
Implications for Cancer Survivorship Care
Given the vision for developing models for cancer survivorship care which integrate virtual or remote follow-up, and shared nurse-led and primary care-led models of care, there is a need for greater understanding of the mechanisms by which healthcare services may impact upon cancer survivors’ QoL outcomes across varied healthcare systems and models of care. The MoHaQ-CS may support the development and adaptation of supportive care interventions which are sensitive to context and the personal needs of people living with and beyond cancer (Richards & Hallberg, 2015). Furthermore, the MoHaQ-CS could inform planning for comprehensive evaluation of factors influencing cancer survivors’ QoL within supportive care interventions and inform future studies to identify risk factors for poorer outcomes and disparities in QoL outcomes.
Limitations
PIP has been proposed as a rigorous, inductive approach supporting systematic integrated analysis and display of MMR data (Johnson et al., 2019). However, to our knowledge, this is the first example of a deductive approach to PIP, and as such, the results of the study should be interpreted in the context of this potential limitation. An inductive approach to integrated analysis may have yielded alternative findings. Given the context in which this study was conducted, the generalizability of the MoHaQ-CS may be limited by the funding and organization of cancer services in Ireland. Firstly, healthcare provision in Ireland operates in a mixture of both public and private settings, which is quite distinct from the privatized and universal models of healthcare operated in other international jurisdictions. Secondly, the structure of cancer-related follow-up care in Ireland is not currently standardized. In private healthcare systems, follow-up healthcare is primarily lead by physicians, while in public healthcare systems, follow-up care is largely nurse-led; however, additional physician-led care may be provided to some cancer survivors.
Conclusion
Integration of MMR data within this study serve to advance the utility of the Ashing-Giwa (2005) Contextual Model of Health-Related Quality of Life with broader populations of cancer survivors in international contexts, cohesively describing the processes by which healthcare factors may influence cancer survivors’ QoL. The use of a theoretical framework to guide exploratory MMR can enable more nuanced understanding of complex phenomena, while supporting high levels of integration in the design, analysis and interpretation of MMR. The use of a modified, deductive PIP to support integration within this study has enabled a focused analysis, allowing comparison and contrast between quantitative and qualitative data to illuminate the nuances of the interaction between the concepts of interest, healthcare system and QoL. The product of this analysis, the MoHaQ-CS can provide the pillars to enable comprehensive development and evaluation of complex interventions which are responsive to the supportive care needs and health-related QoL of cancer survivors.
Footnotes
Acknowledgements
The authors would like to thank the physicians, nurses and staff of the surgery and medical oncology departments of participating hospitals and voluntary cancer support services who facilitated data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by funding from the Health Research Board of Ireland (HPF.2014.715).
Data Availability
The datasets generated during and/or analysed during the current study are not publicly available. Excerpts of data are available from the corresponding author upon reasonable request.