
Abstract
Background
15–30% of breast cancer patients will develop brain metastases (BM) during their illness. The prognosis of this entity remains poor. Several scores were established to predict the prognosis of BM from breast cancer stating by the recursive partitioning analysis to the breast-graded prognostic assessment score (B-GPA) and the modified breast-graded prognostic assessment score (m B-GPA). The objective of this study was to compare the B-GPA and the m B-GPA in the prediction of overall survival.
Methods
This was a retrospective and analytical study carried out within the medical oncology department of Sfax between 2008 and 2018, including all patients with breast cancer brain metastases with a known hormone receptor (HR) status and of HER2. We analyzed the overall survival (OS), the B-GPA, and the m-BGPA.
Results
60 patients were included. 32 patients (53%) had a preserved general condition (PS 80–90) while 4 patients (7%) presented an alteration in general condition (KPS ≤ 50). 24 cases (40%) had HR+/HER2-profile, 17 cases (28%) had HR+/HER2+, 9 cases (15%) HR−/HER2+, and 10 cases (17 %) had triple negative profile. Overall survival at 1 year from the diagnosis of BM was 16.7%. The prognostic factors influencing survival were general condition and IHC status (p = 0.038 and 0.013, respectively). Both B-GPA and mB-GPA scores were correlated with overall survival (p < 0.001 for each score). In the predicting of 1-month survival, m B-GPA was superior to the B-GPA (AUC B-GPA: 0.65 vs AUC mB-GPA: 0.67). For 1-year survival, the B-GPA score showed significant superiority with a better AUC index (AUC B-GPA: 0.85 vs AUC mB-GPA: 0.82).
Conclusion
Our study concluded that mB-GPA was better in predicting 1-month OS. However, B-GPA was more interesting in predicting 1-year OS. This means that the prognostic value of the number of brain metastases fades at 1 year.
Introduction
Breast cancer ranks first in terms of incidence and mortality in women. In 2020, 2.3 million women were diagnosed with breast cancer. 685,000 women died from breast cancer worldwide. 1 Thanks to the constant increase in the therapeutic arsenal for breast cancer, patient survival has improved over the last decades. This results in an increase in the incidence of brain metastases (BM) of up to 15–30%.2,3 They can occur synchronously or metachronously.4,5 Histological grade usually correlates with metastasis. The higher the grade, the more chances of metastasis there are. The RPA (Recursive Partitioning Analysis) classification is the first prognostic score to classify patients with brain metastases. It is composed of the Karnofsky index (KPS), age, and the presence or absence of extra-cranial metastases. 6
Several scores have been refined over time. They provided specific risk indices based on histological type and biomolecular variants in breast cancer. In recent years, B-GPA (Breast-Graded Prognostic Assessment) scores, and in particular mB-GPA (modified Breast-Graded Prognostic Assessment), have become an integral part of the classifications and prognostic scales used in patients with BM to predict the median duration. The objective of our study was to assess the value of prognostic scores in predicting the median duration of overall survival.
Methods
This was a retrospective descriptive study, involving patients with metastatic breast carcinoma to the brain in the medical oncology and radiotherapy departments of the Habib Bourguiba hospital in Sfax during a period of 10 years, between 2008 and 2018. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institution and the national research committee of Habib Bourguiba hospital and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. We included in this study patients aged 18 years and over with histologically proven breast carcinoma with known hormone receptor and HER2 status, metastatic to the brain at the time of diagnosis or during the course of the disease.
HR was considered positive if the level of estrogen receptors (ER) and/or progesterone receptors (PR) was greater than or equal to 1%.
HER2 status was defined as overexpressed if there was intense and complete membrane labeling of at least 30% of cells. From 2015, according to ASCO/CAP (American Society of Clinical Oncology/College of American Pathologist), HER2 overexpression was defined by a labeling threshold of at least 10% of cells. HER2 status was considered positive if the marking score was equal to 3+ or equal to 2+ with a positive FISH study.
For each patient followed for breast carcinoma and presenting neurological signs, we requested an emergency brain CT scan supplemented, if necessary, by a brain MRI in case of strong suspicion.
Breast-graded prognostic assessment (B-GPA) and modified breast-graded prognostic assessment (mB-GPA).
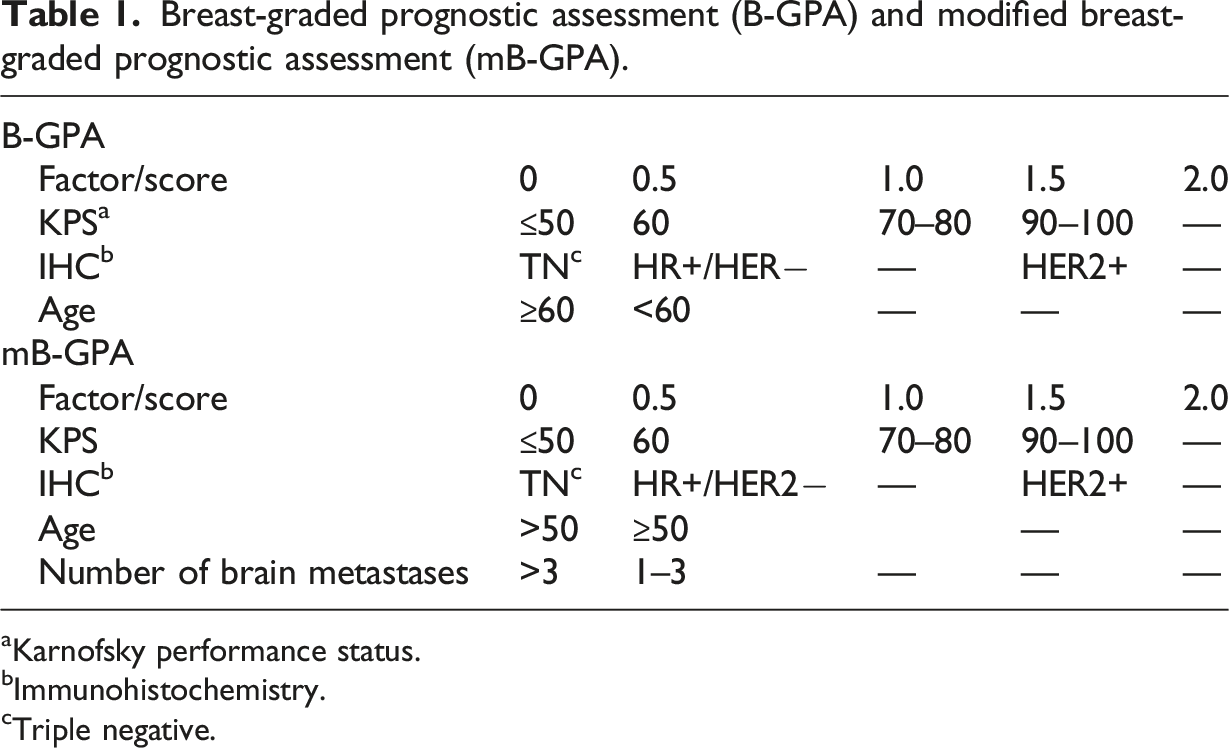
aKarnofsky performance status.
bImmunohistochemistry.
cTriple negative.
To study the prognostic performance of these different scores, we evaluated the impact of each of the factors constituting these scores, namely, age, molecular subtype, general condition, and number of BMs, on survival separately in a univariate analysis.
Overall survival was measured from the date of BM diagnosis to the date of death or the date of last follow-up.
Computer processing was carried out for all the information thus collected and analyzed from each patient using the SPSS software for Windows (Statistical Package for Social Science: SPSS Inc, Chicago, IL) in version 20. The qualitative variables were expressed in percentages and frequencies. Quantitative variables were expressed as means, medians, and standard deviations. Comparison (or hypothesis) tests make it possible to study the relationship between two variables. The p-value (p) is the probability of obtaining the same value (or an even more extreme value) of the test if the null hypothesis were true. The significance threshold is set at 5%, that is to say the test is considered significant (and therefore a correlation exists between the 2 variables) if p is less than 0.05. To evaluate the prognostic performance of B-GPA and mB-GPA scores regarding 1-month and 1-year survival, we compared B-GPA to mB-GPA using survival ROC curves.
Results
During a period of 12 years (2008–2018), 2789 cases of breast cancer were treated at Habib Bourguiba hospital in Sfax of which 96 developed brain metastases. 60 patients, with known hormone receptor and HER2 status, were included with an average age of 43 years. 32 patients (53%) had a preserved general condition (PS 80–90) while 4 patients (7%) presented an alteration in general condition (KPS ≤ 50). Brain radiotherapy was performed in 58 patients (96%), surgery in 4 patients (6.6%), and systemic treatment in 40 patients (66%). It was HR + HER2+ in 28%, HR + HER2− in 40%, HR−HER2+ in 15%, and triple negative in 17%.
After the diagnosis of cancer, the onset times of BM vary between 1 and 108 months. The medians of occurrence vary according to the histological subtype, ranging from 15.9 months for cohorts with triple-negative tumors to 19.6 months for cohorts with tumors overexpressing HER2 and finally 39.2 months for cohorts with HR+/HER2− tumors. These were multiple brain metastases in 85% of cases (42% in case of triple-negative cancer, 41% in case of HER+++, and 17% in case of HR+). 96.7% of patients had brain radiotherapy, 6.6% had surgery, and 3.3% had no treatment due to their general condition. Chemotherapy was done in 96.7% of cases.
Distribution according to B-GPA and mB-GPA scores.
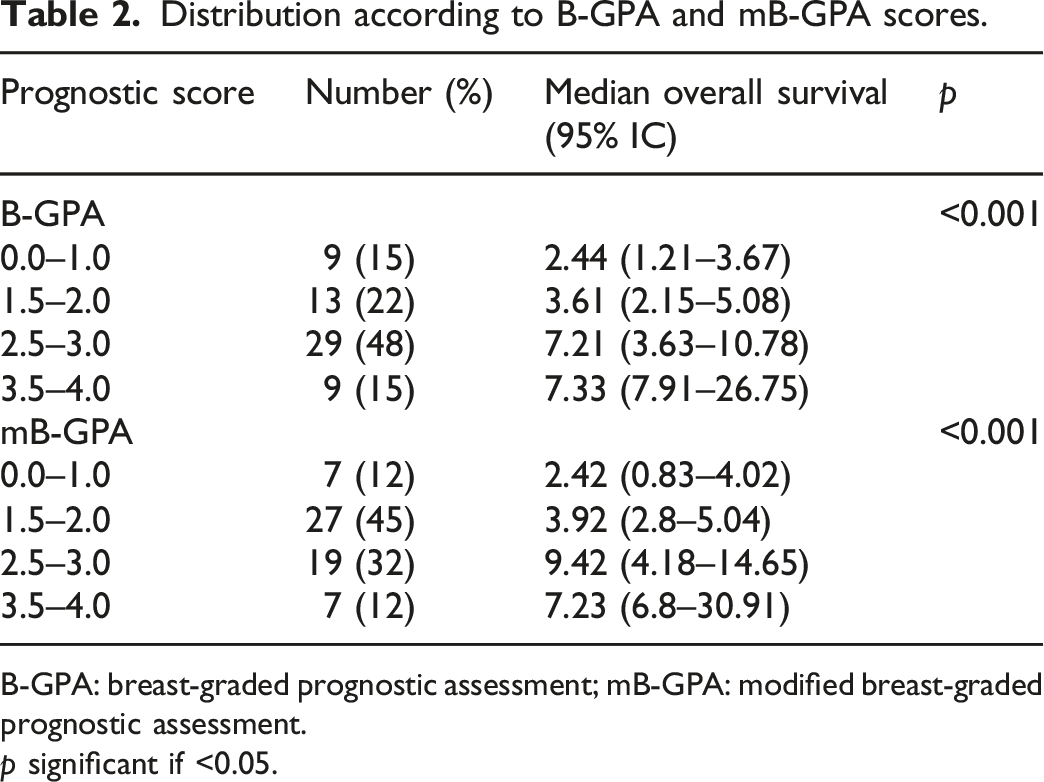
B-GPA: breast-graded prognostic assessment; mB-GPA: modified breast-graded prognostic assessment.
p significant if <0.05.
Analysis of overall survival according to prognostic factors of B-GPA and mB-GPA scores.
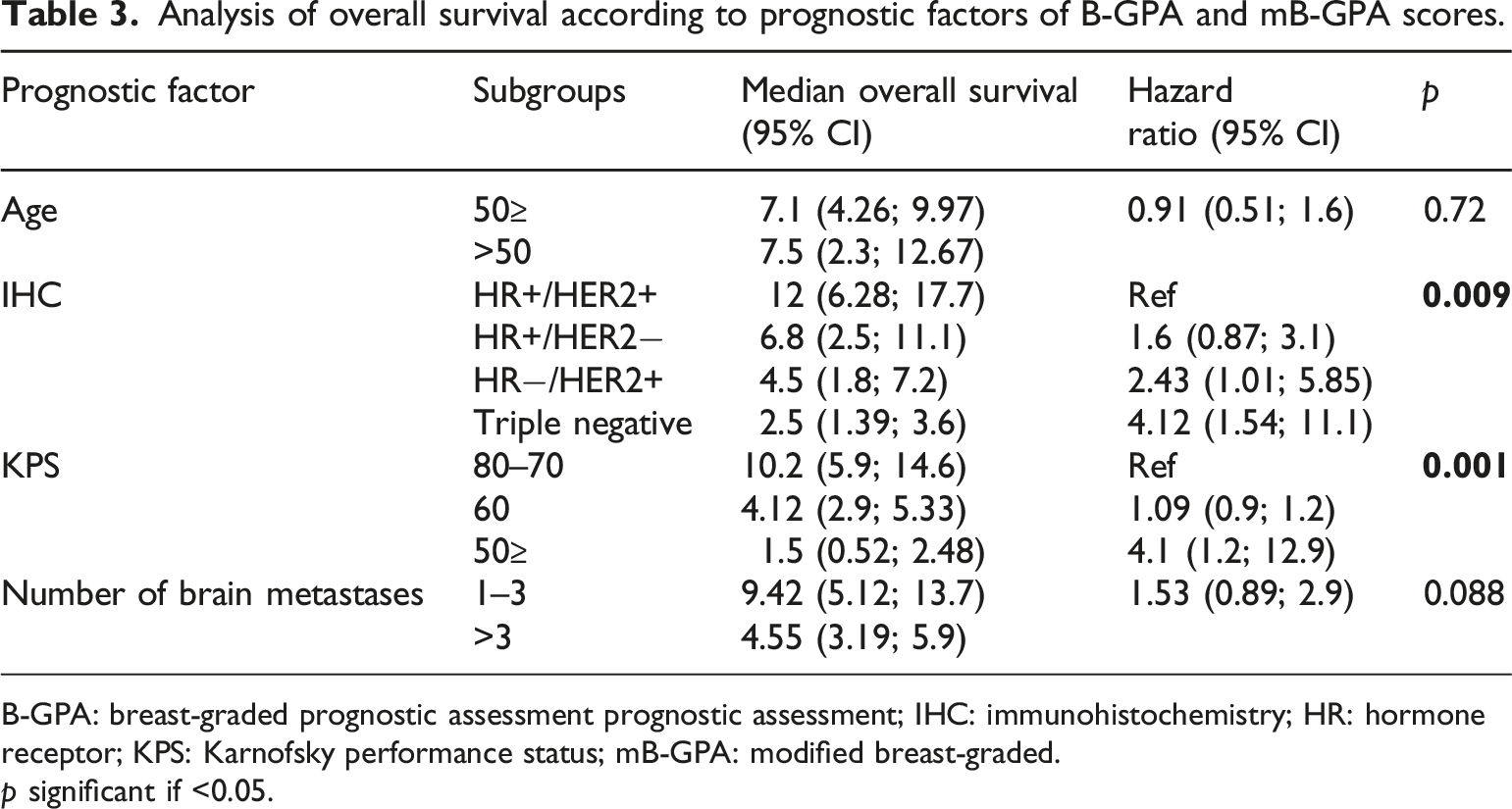
B-GPA: breast-graded prognostic assessment prognostic assessment; IHC: immunohistochemistry; HR: hormone receptor; KPS: Karnofsky performance status; mB-GPA: modified breast-graded.
p significant if <0.05.
All B-GPA and mB-GPA survival predictions were compared to observed overall survival. Regarding survival at 1 month, in the B-GPA 0.0–1.0 group, a third of the patients died within 1 month, while 42.9% of patients in the mB-GPA group died within 1 month.
The survival ROC curves for B-GPA and mB-GPA were very similar, with a slightly higher AUC for the mB-GPA curve (AUC B-GPA: 0.65 vs AUC mB-GPA: 0.67) (Figure 1). 1-Month survival ROC curves for B-GPA and mB-GPA scores.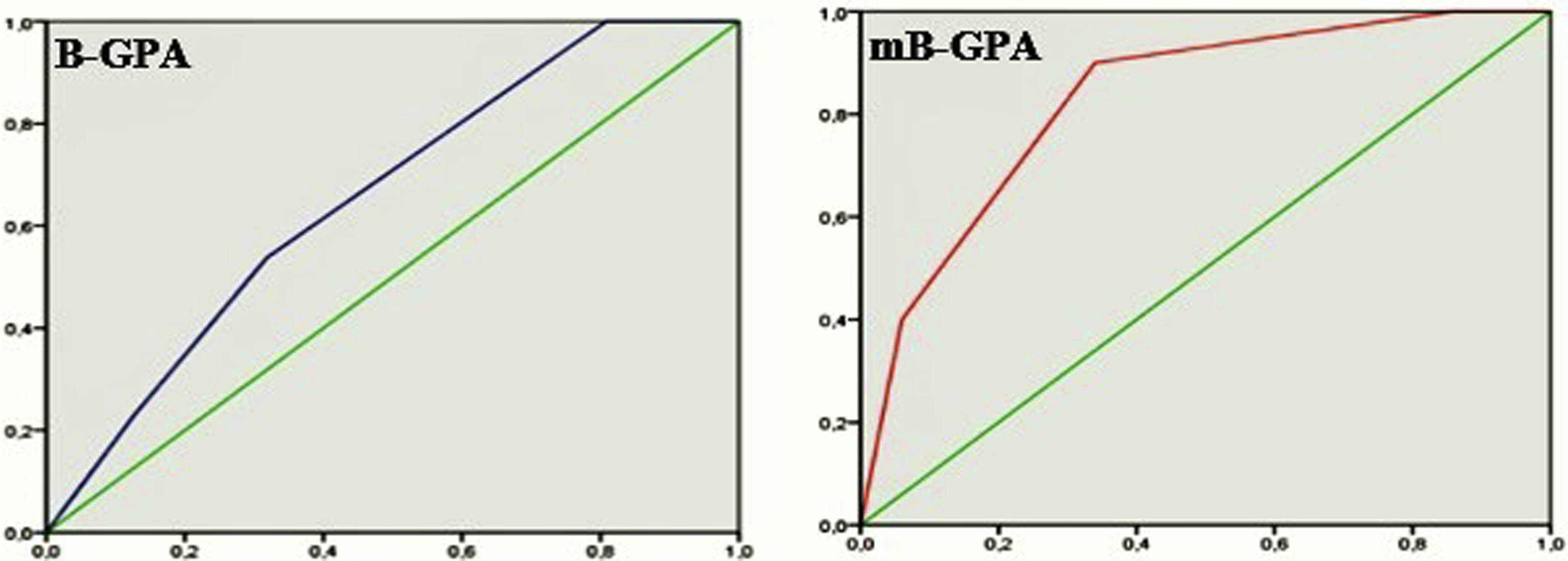
Regarding overall survival at 1 year, in the B-GPA 3.4–4.0 group, 66.7% of patients survived 1 year, while 57% of patients in the mB-GPA group survived 1 year.
The B-GPA score appears to have a better prognostic performance (AUC B-GPA: 0.85 vs AUC mB-GPA: 0.82) for 1-year survival (Figure 2). 1-Year survival ROC curves for B-GPA and mB-GPA scores.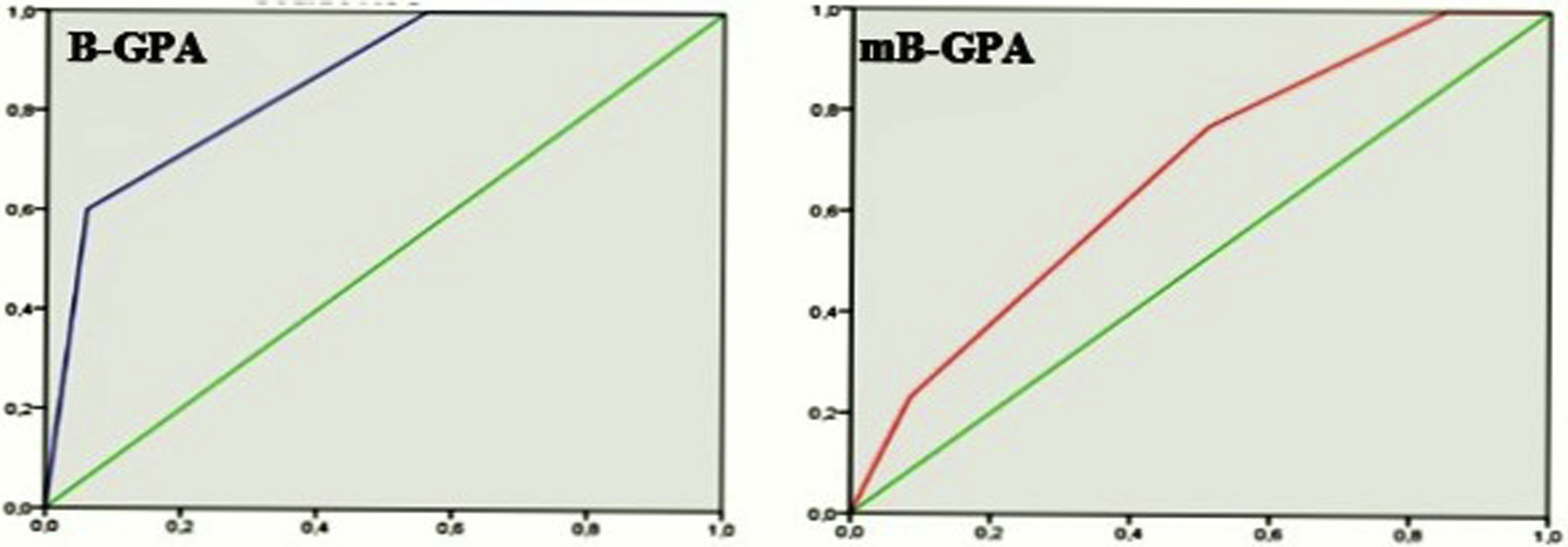
Discussion
Our study concluded that mB-GPA was better in predicting 1-month OS. However, B-GPA was more interesting in predicting 1-year OS. This means that the prognostic value of the number of brain metastases fades at 1 year.
According to the latest recommendations, single BMs should be considered for surgical resection. Multiple resectable BMs may be considered for surgical resection. Stereotactic radiosurgery is recommended for patients with a limited number1–4 of BM. Whole brain radiotherapy should be considered for treatment of multiple BMs, depending on the presence of neurological symptoms, size, number and location of BMs, and the choice and availability of active systemic therapy. 6
Several studies have attempted to clarify the role of MC number in predicting survival. A series of 162 patients from a single institution identified better OS among patients with solitary brain lesions treated with radiotherapy than those with multiple intracranial metastases (median OS 11 months vs 5.8 months). 2 The study by Nieder et al. involving 82 patients noted that the presence of more than one metastasis had prognostic importance (p < 0.05). 7
In 2015, Subbiah et al., in an analysis of 1552 patients, modified the B-GPA score to incorporate the number of MCs as a fourth variable, thus creating the modified B-GPA. 8 They confirmed its prognostic role with a significantly higher median survival time in patients with one to three brain lesions than those with three brain metastases (13.2 months vs 6.3 months; p < 0.001). 8 This was not found in our series, the number of MCs did not significantly affect survival (p = 0.08).
By comparing the two B-GPA scores and the mB-GPA, the latter seems to be a better prognostic tool. The concordance index for the original B-GPA was 0.78 (95% CI, 0.77–0.80) while the concordance index for the proposed mB-GPA was 0.84 (CI at 95%, 0.83–0.85).9,10 Since then, it has been the subject of two independent validations.9,10 In our series, mB-GPA was better at predicting 1-month survival (AUC of 0.67 vs 0.65) but not at predicting 1-year survival.
Although our study spans 10 years, it has some limitations that must be taken into account. The retrospective nature may affect the widespread application of our results and the relatively small sample size.