
Abstract
Sexual health is a fundamental aspect of overall well-being, with erectile dysfunction (ED) being one of the most prevalent sexual disorders. Nurses play a crucial role in addressing the needs of patients experiencing ED, yet their specific roles and responsibilities remain underexplored. We conducted a mixed-methods systematic review to examine the general and specific roles of registered nurses (RNs) and nurse practitioners (NPs) in caring for patients with ED. Relevant studies were identified through searches in Academic Search Complete (EBSCO), Embase, PubMed, ProQuest, Cochrane Library, and Google Scholar. Two independent researchers assessed the methodological quality of the included studies (N = 14; 12 quantitative and two qualitative) using the Joanna Briggs Institute Critical Appraisal Checklist and performed data extraction, transformation, integration, and synthesis. Five responsibilities of nursing roles in ED care were identified: (1) risk factor assessment, (2) needs clarification and/or diagnosis, (3) individual or couple education, (4) facilitation and/or provision of treatment, and (5) continuous monitoring. RNs play a fundamental role in assessing and identifying problems, promoting sexual health, educating and supporting treatment adherence, and facilitating interventions or treatments. In contrast, NPs have a distinct role in monitoring laboratory testing, diagnostics, counseling and treating patients, and collaboration with specialists. Both RNs and NPs use a multidisciplinary approach to provide care activities; RNs provide referrals for to get better services internally or externally, while NPs refer for specialists or urologists’ consultations to promote comprehensive care. Findings underscore the need for enhanced education and training programs for RNs—to improve their knowledge of assessment, understanding of ED care—and for NPs—to improve knowledge of diagnosis, counseling, treatment, and patient monitoring—to ensure comprehensive and multidisciplinary ED team care.
Introduction
Sexual health is a key component of the overall health and well-being of individuals, their sexual partners, and families (World Health Organization, 2024). Erectile dysfunction (ED) is one of the most common sexual dysfunctions, defined as “the condition of insufficient penile erection for appreciated vaginal intercourse and satisfactory sexual performance” (Ismail, Gressy, et al., 2024; Ismail, Yusof, et al., 2024). ED is an increasing public health problem globally; the prevalence of ED about 16% in men aged 20 to 75 years worldwide (Nicolosi et al., 2003; Rosen et al., 2001). Similarly, the projections for 2025 indicate that 322 million men will be affected by ED worldwide (Ayta et al., 1999; Ismail & Abdelghany, 2022). Men affected by COVID-19 were 3.3 times more likely to experience ED (Ismail, 2022c). The physiology of keeping an erect penis involves integration of organic (endocrine, neurological, vascular, and structural) and psychogenic etiologies, the scleroses to arteries, endothelial cells dysfunction, cavernous smooth muscle relaxation, cavernosal nerve injury, nitric oxide dysfunction, venous leakage, aging, psychological conditions such as anxiety and depression, endocrine conditions, and certain medications, which affect erectile function due to side effects resulting in altered blood flow to and from the penis (Ismail, 2022c; Ismail & Hamed, 2024; Kessler et al., 2019; Peate, 2012; Primanda et al., 2023). According to the 2018 American Urological Association guidelines, changing patients’ comorbid conditions, adjustable risk factors, or unhealthy lifestyle is the first-line treatment approach. Oral phosphodiesterase type 5 (PDE5) inhibitors are the preferred therapy for ED and are often combined with testosterone therapy if the patient has testosterone deficiency. Other alternative treatments, including vacuum therapy, intraurethral or intracavernosal therapy, low-intensity extracorporeal shock wave therapy, and prosthesis implantation have also demonstrated substantial therapeutic impact among patients who do not respond to pharmacotherapeutic interventions (Burnett, Nehra, et al., 2018).
ED has an economic burden; the total Medicare expenditures from 2009 to 2015 in the United States following an ED diagnosis were 33% greater in patients during year 1 and 20% higher in patients during year 5 compared with non-ED patients (Burnett, Zhong, & Amorosi, 2018). ED is linked to the global aging population (Johannes et al., 2000), perhaps due to longer lifespans and chronic conditions, and is the precursor of more serious medical issues like diabetes mellitus, lack of or decreased testosterone, cardiovascular disease, hypertension, benign prostatic hyperplasia, neurological disease, dislipidemia, atherosclerosis, obesity, chronic plaque psoriasis (CPP), metabolic syndrome, COVID-19 infection, human immunodeficiency virus (HIV), chronic hepatitis C, or tinnitus (Burnett, Zhong, & Amorosi, 2018; Ismail, 2022a, 2022b, 2022c; Ismail & El Melhat, 2024; Ismail, 2023; Ismail & Abd El-Azeim, 2022; Ismail & Abdelghany, 2022; Ismail, Gressy, et al., 2024; Ismail & Hamed, 2024; Ismail, Yusof, et al., 2024; Raheem et al., 2017; Turkoski, 2008). Lifestyle risk factors, certain medications, undergoing radiation or surgery for prostate cancer, spinal cord injury, surgery to the spine or pelvic area, or neurologic diseases can contribute to ED symptoms (Albaugh et al., 2002; Boyd, 2007; Mola, 2015; Primanda et al., 2023; Turkoski, 2008). Psychological complications that accompany a decreasing sex drive associated with ED included anxiety, stress, fatigue, depression, anger, mental illness, and dementia (Albaugh et al., 2002; Boyd, 2007; Mola, 2015). ED significantly affects mental and psychological well-being and the quality of life (QoL) of men’s partners. Female partners of men with ED experience decreased sexual desire, arousal, orgasm, and a decrease in sexual satisfaction, commensurate with the degree of ED in men (Fisher et al., 2005; Primanda et al., 2023).
ED management is a fundamental component in achieving beneficial, quality care (Albaugh et al., 2002; Lewis, 2000). ED management facilitates patients’ knowledge about the illness, enhances patients’ treatment compliance, improves care for the physical, emotional, and psychosocial needs of patients, and improves males’ and their sexual partners’ health care quality (Albaugh et al., 2002; Lewis, 2000; Mola, 2015). Educating and supporting patients with ED helps to improve men’s and their sexual partners’ QoL, enhance patients’ assertiveness and self-disclosure skills for communication, address physical, emotional, and psychological issues that occur with ED, avert potential harm of drugs prescribed to treat ED, and increase coping with ED (Green & Kodish, 2009; Primanda et al., 2023; Schreiber, 2019; Turkoski, 2008). In addition, possessing knowledge and staying up to date with approaches to ED care helps patients to select suitable treatment options and helps providers deliver more comprehensive information to patients (Peate, 2012).
Registered nurses (RNs) should have completed either an Associate’s Degree in Nursing (ADN) or a Bachelor of Science in Nursing (BSN) and provide direct care under a physician supervisor (Aberle et al., 2024). Nurse practitioners (NPs) first earn a BSN, then pursue a Master of Science in Nursing (MSN) or a Doctor of Nursing Practice (DNP) and provide direct patient care, mostly without physician supervision (American Association of Nurse Practitioners, 2025; Ljungbeck et al., 2024). NPs are at the forefront of holistic care for the physical, emotional, and psychosocial needs of patients with ED, serving as the main source of sexual health care information and positively affecting health outcomes (Albaugh et al., 2002; Mola, 2015; Primanda et al., 2023). In addition, NPs deliver knowledge and care regarding patient and team communication, perform assessments and diagnoses, prescribe medication, provide patient education, perform invasive treatment, refer patients to specialists, and conduct patient monitoring (Boyd, 2007; Green & Kodish, 2009; Lewis, 2000). RNs also perform valuable yet challenging roles, which include offering care about patient assessment, providing treatment-related information, facilitating appropriate intervention and treatments, providing education and support, consulting with health care professionals, providing suggestions for referrals for further diagnosis or therapeutic options, and following-up for treatment adherence (Intili & Nier, 1998; Lombraña et al., 2012; Mkonyi et al., 2024; Nicolai et al., 2014; Peate, 2012; Primanda et al., 2023; Schreiber, 2019; Turkoski, 2008).
ED management is influenced by various factors such as nurses’ education level, training, and experience regarding to ED (Mkonyi et al., 2024; Turkoski, 2008). Clarifying these roles among RNs and NPs can inform formal education and training programs about ED for nurses. Such programs can improve the quality of nursing care and enhance nurses’ ability to manage patients with ED.
Previous studies have explored whether RNs or NPs focus on managing ED for specific chronic diseases (Boyd, 2007; Burbage-Vieth, 2020; Green & Kodish, 2009; Lewis, 2000; Mkonyi et al., 2024), but few have combined RNs and NPs to examine their expert function regarding ED care (Albaugh et al., 2002; Mola, 2015). To the best of our knowledge, few review articles have examined the nursing role or function in specific organic disease patients with ED (Meek & Croston, 2017; Rogers et al., 2022), and no systematic review has been conducted to explore the roles and responsibilities specifically related to ED patients, including organic and psychogenic conditions addressed by nurses. Therefore, a systematic review is warranted to investigate the roles and responsibilities of RNs and NPs caring for patients with ED. Nursing interventions have specific benefits over other traditional treatments for ED patients, such as tailoring treatments to an individual’s needs, providing patient education and counseling on strategies to alleviate symptoms, maintaining intimate relationships outside of intercourse, strengthening sexual partners’ involvement, and to improving patients’ coping skills (Darst, 2007; Eduardo et al., 2016; Lee & Park, 2013; Son et al., 2016). This research aimed to clarify the roles and responsibilities of RNs and NPs in the management of patients with ED.
Method
Study Design
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009).
Inclusion and Exclusion Criteria
The inclusion criteria were studies published in English, quantitative or qualitative articles, peer-reviewed articles, and full-text studies involving the roles or responsibilities of RNs or NPs who took care of patients with ED or had a chronic illness that complicated with ED, or studies that examined the perceptions of patients with ED related to RNs and NPs care activities. Studies involving nurse executives, head nurses, academic nurses, nurse assistants, practice nurses, clinical nurse specialists, or aides were excluded, as their jobs did not involve caring for patients with ED. All articles were evaluated using the Joanna Briggs Institute critical appraisal checklist (JBI; Aromataris & Munn, 2020). PICoS guidelines are presented in Table 1.
Inclusion and Exclusion Criteria.
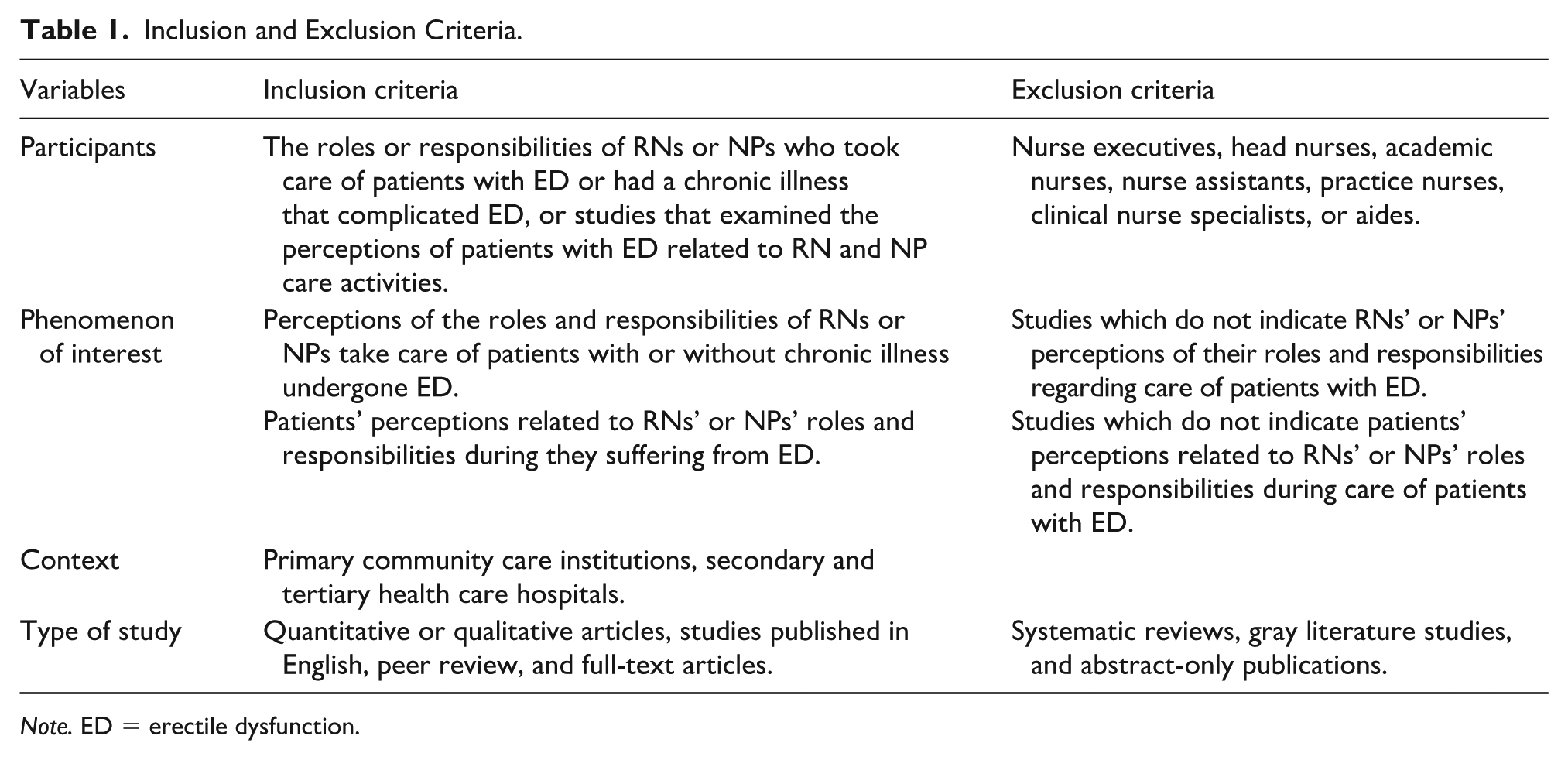
Note. ED = erectile dysfunction.
Search Strategy
An initial literature search was carried out using key terms to generate a search strategy and identify relevant literature. The following databases were searched from 1938 to May 11, 2025: Academic Search Complete (EBSCO), Embase, PubMed, ProQuest, Cochrane Library, and Google Scholar. The following keywords were used to identify the studies: (1) erectile dysfunction AND (2) nurse OR nursing staff; and (3) nurse role OR nursing role OR nurse duty OR nursing responsibility OR nurse intervention.
Study Selection
Studies identified by the search were reviewed based on the keywords; duplicates were removed. Two authors (H-CC and C-YL) screened each article based on the title and abstract. Relevant articles were selected from full-text articles. Three authors (H-CC, C-YL, and C-HL) evaluated the full text against the inclusion and exclusion criteria, and any discrepancies were resolved by consensus. The flow diagram for study selection is presented in the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA; Figure 1; Shamseer et al., 2015).

Flow Diagram for Study Selection: PRISMA.
Quality Appraisal
Using the JBI critical appraisal tool to assess study quality (Aromataris & Munn, 2020; Munn et al., 2020), each study was assessed by two authors (H-CC and C-YL). Articles extracted for the following critical appraisal of quantitative studies included four parts: (1) internal validity, (2) statistical conclusion validity, (3) comprehensiveness of reporting, and (4) external validity (Barker et al., 2023). Assessment of the methodological quality of qualitative studies included three parts: (1) the philosophical perspective, the chosen methodology, the data collection methods, and appropriateness of it, (2) the process of data collection and the meaning of all participants’ view, and (3) data analysis and interpretation (Lockwood et al., 2015).
Articles were not excluded based on significant methodological errors that may affect the quality of review articles. This was done to avoid excluding any significant articles due to the methodological quality of the studies (Butler et al., 2016; Korhonen et al., 2013). Review discrepancies were addressed by discussions with three authors until consensus reached; articles were excluded if the reviewer perceived the article did not accurately include “the role or responsibilities of nurses to care for ED.”
Data Extraction
Relevant data were extracted by two authors (H-CC and C-YL), and a third author (C-HL) assessed the accuracy or disagreements of the extracted data. The extracted data for quantitative studies did not undergo statistical analysis to assess the risk of bias owing to the heterogeneity of the research methodology. We extracted data relevant to the aims of the present review.
Data Synthesis and Integration
Following the JBI approach to mixed methods systematic reviews (MMSRs), we employed a methodology of combining and integrating both quantitative and qualitative evidence in a the convergent integrated approach to address the research topic (Stern et al., 2021). This process focuses on quantitative data transformation (e.g., transforming textual descriptions of results from quantitative format), data integration (e.g., pooling with qualitative data and the textual descriptions of quantitative data), and data synthesis (e.g., combining extracted data from qualitative studies and generation of qualitative evidence (Stern et al., 2021). We combined this evidence to produce comprehensive findings. Studies were categorized based on whether they reported nurses’ perspectives, patients’ perspectives, or both. Articles that included disease-specific roles were noted but not analyzed quantitatively due to insufficient comparable data.
Results
Search Results
In total, 206 articles were identified. After removing duplicate articles, 175 remained. After screening the titles and abstracts, 43 were excluded, and 132 underwent full-texts assessment. Following a review of the eligibility criteria, 118 articles were excluded, and 14 eligible articles were finally included, including 12 quantitative and two qualitative papers. The search results are presented in the PRISMA flowchart (Figure 1; Shamseer et al., 2015).
Study Characteristics
All included studies had quantitative, qualitative, or mixed-method designs. The studies were conducted in six counties, included in United States (Burbage-Vieth, 2020; Green & Kodish, 2009; Intili & Nier, 1998; Mkonyi et al., 2024), United Kingdom (Boyd, 2007), Spain (Johannes et al., 2000), the Netherlands (Nicolai et al., 2014), Indonesia (Primanda et al., 2023), and Tanzania (Mkonyi et al., 2024), with participants aged 20 to 94 years. Notably, a significant number of the studies were conducted in community settings (website surveys, professional nursing organizations, professional associations, or universities). The sample sizes of these studies ranged from 15 to 456 participants (Green & Kodish, 2009; Intili & Nier, 1998). The characteristics of the included studies are presented in Tables 2 and 3.
Summary of Included Studies (Quantitative Studies).

Summary of Included Studies (Qualitative Studies).

Quality Appraisal
The assessment of methodological quality is presented in Tables 4 to 7. Among the four cross-sectional quantitative studies, the majority accurately portrayed the study participants’ characteristics, validated measurements, confounding factors, outcome assessments, and data analysis. However, one study failed to address confounding factors, thus leaving a gap in justifying the methods by which they evaluated their findings (Table 4). In the single cohort study, there was congruity between the participants, data measurement, collection, and analysis; however, it failed to declare the influence of incomplete follow-up assessments, thereby warranting caution in the interpretation of the validity of the study or risk of selection bias (Table 5). Among the seven expert opinion studies, all articles logically included the opinion, were upstanding in the field of expertise, expressed logically, and included references. However, they were missing any literature-defended considerations, thereby warranting consideration in the wider support of their opinion (Table 6). The two qualitative studies stated the philosophical perspective, research questions and methodology, data collection methods, analytical procedures, and interpretation (see Table 7).
Summary of Quality Assessment: Quality Appraisal Using JBI Checklist for Cross-Sectional Studies (n = 4).

Note. Y = Yes, N = No, U = Unclear, N/A = Not applicable.
Q1 = Were the criteria for inclusion in the sample clearly defined?
Q2 = Were the study subjects and the setting described in detail?
Q3 = Was the exposure measured in a valid and reliable way?
Q4 = Were objective, standard criteria used for measurement of the condition?
Q5 = Were confounding factors identified?
Q6 = Were strategies to deal with confounding factors stated?
Q7 = Were the outcomes measured in a valid and reliable way?
Q8 = Was appropriate statistical analysis used?
Summary of Quality Assessment: Quality Appraisal Using JBI Checklist for Cohort Studies (n = 1).
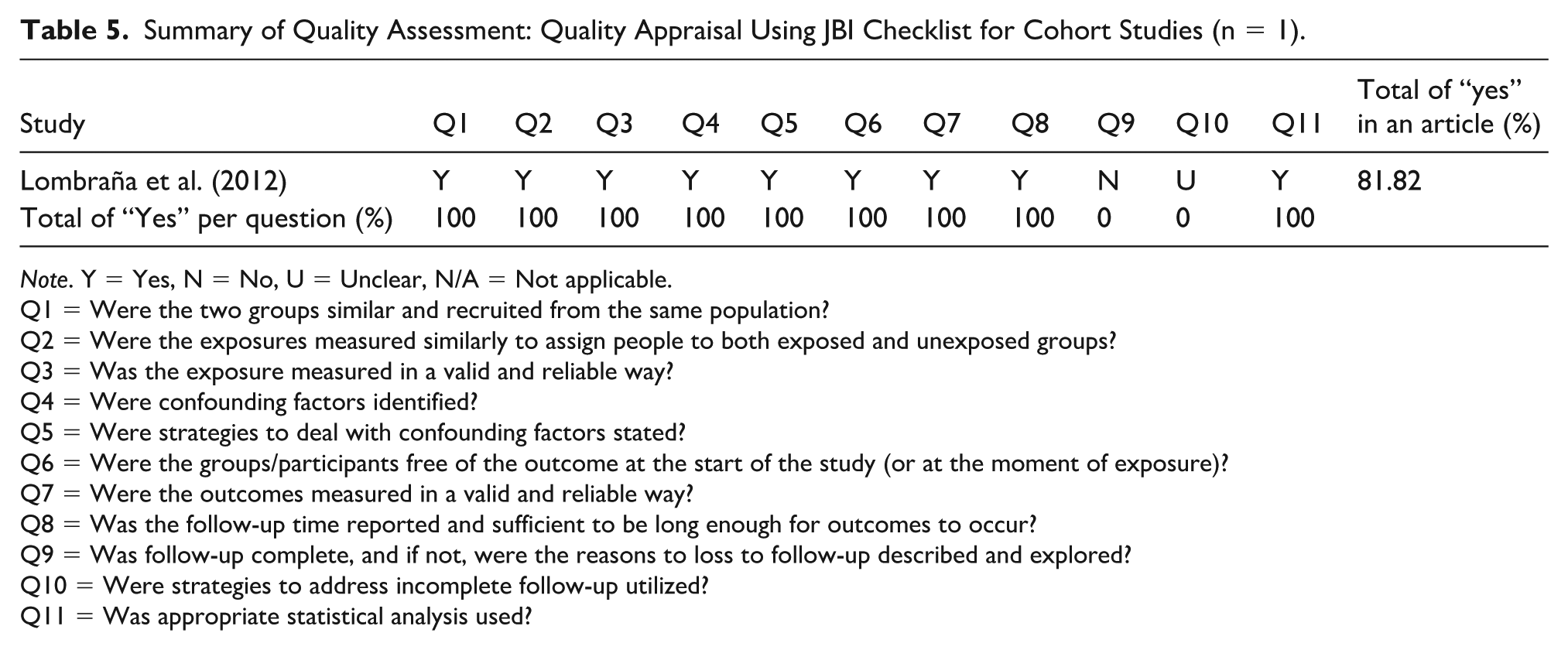
Note. Y = Yes, N = No, U = Unclear, N/A = Not applicable.
Q1 = Were the two groups similar and recruited from the same population?
Q2 = Were the exposures measured similarly to assign people to both exposed and unexposed groups?
Q3 = Was the exposure measured in a valid and reliable way?
Q4 = Were confounding factors identified?
Q5 = Were strategies to deal with confounding factors stated?
Q6 = Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)?
Q7 = Were the outcomes measured in a valid and reliable way?
Q8 = Was the follow-up time reported and sufficient to be long enough for outcomes to occur?
Q9 = Was follow-up complete, and if not, were the reasons to loss to follow-up described and explored?
Q10 = Were strategies to address incomplete follow-up utilized?
Q11 = Was appropriate statistical analysis used?
Summary of Quality Assessment: Quality Appraisal Using JBI Checklist for Text and Expert Opinion (n = 7).

Note. Y = Yes, N = No, U = Unclear, N/A = Not applicable.
Q1 = Is the source of the opinion clearly identified?
Q2 = Does the source of opinion have standing in the field of expertise?
Q3 = Are the interests of the relevant population the central focus of the opinion?
Q4 = Is the stated position the result of an analytical process, and is there logic in the opinion expressed?
Q5 = Is there reference to the extant literature?
Q6 = Is any incongruence with the literature/sources logically defended?
Summary of Quality Assessment: Quality Appraisal Using JBI Checklist for Qualitative Research (n = 2).

Note. Y = Yes, N = No, U = Unclear, N/A = Not applicable.
Q 1 = Is there congruity between the stated philosophical perspective and the research methodology?
Q2 = Is there congruity between the research methodology and the research question or objectives?
Q3 = Is there congruity between the research methodology and the methods used to collect data?
Q4 = Is there congruity between the research methodology and the representation and analysis of data?
Q5 = Is there congruity between the research methodology and the interpretation of results?
Q6 = Is there a statement locating the researcher culturally or theoretically?
Q7 = Is the influence of the researcher on the research, and vice-versa, addressed?
Q8 = Are participants, and their voices, adequately represented?
Q9 = Is the research ethical according to current criteria or, for recent studies, and is there evidence of ethical approval by an appropriate body?
Q10 = Do the conclusions drawn from the research report flow from the analysis, or interpretation, of the data?
Quantitating Data Synthesized Findings
Quantitative data synthesis was conducted for all articles to identify the overarching roles and responsibilities of nurses who care for patients with ED. Some articles emphasized that RNs should be either and- or BSN-trained and provide direct care under a physician supervisor in a clinical setting, while others pointed out that NPs should first earn a BSN, then pursuing an MSN or a DNP, and serve as direct patient care mostly without physician supervision. These two types of nursing professions have both general and specific roles and functions. The synthesis of key findings led to the identification of these similar and specific functions, summarizing that nursing professionals have five components of duties to manage patients with ED and their partners: risk factor assessment, diagnosis and/or clarification, individual or couple education, facilitation and/or provision of treatment, and continuous monitoring (Table 8). Supplementary Table 1 summarized the disease contexts represented in the included studies.
Quantitating Data Synthesis of the Key Findings, the Role, and Responsibilities of Caring for Erectile Dysfunction.

Risk Factor Assessment
Studies reported that problem identification was the first tasks in the assessment of ED among patients. Five articles mentioned that nurses identify problems or concerns by applying a questionnaire, such as International Index of Erectile Function (IIEF), International Index of Erectile Function five (IIEF-5) (Burbage-Vieth, 2020; Lombraña et al., 2012; Mola, 2015; Primanda et al., 2023), or sexual health inventory for men (SHIM) (Albaugh et al., 2002; Burbage-Vieth, 2020; Primanda et al., 2023) to inquire about sexual matters. Several studies have highlighted that nurses have a duty to assess any potential causes that contribute to ED, encompassing physical, psychological, sexual, and spiritual aspects (Albaugh et al., 2002; Boyd, 2007; Burbage-Vieth, 2020; Green & Kodish, 2009; Intili & Nier, 1998; Lewis, 2000; Lombraña et al., 2012; Mkonyi et al., 2024; Mola, 2015; Peate, 2012; Primanda et al., 2023; Schreiber, 2019; Turkoski, 2008). Physical assessment regarding organic or undiagnostic diseases includes screening for a variety of conditions, all of which are related causes of ED (Albaugh et al., 2002; Boyd, 2007; Burbage-Vieth, 2020; Intili & Nier, 1998; Lombraña et al., 2012; Mkonyi et al., 2024; Mola, 2015; Peate, 2012; Primanda et al., 2023; Schreiber, 2019; Turkoski, 2008). Psychological assessment via screening for psychogenic causes can assess if patients have achieved normal erection and orgasm through self-masturbation or other means than with a sexual partner with whom ED persists. Psychological assessments can be useful screening tools (Albaugh et al., 2002; Burbage-Vieth, 2020; Intili & Nier, 1998; Lewis, 2000; Mkonyi et al., 2024; Mola, 2015; Peate, 2012; Primanda et al., 2023; Turkoski, 2008).
Nurses’ Perspectives
Nurse’s inquiry about sexual function manifests in various forms, including direct questioning and allowing patients or couples to discuss sexual problems (Burbage-Vieth, 2020; Green & Kodish, 2009; Lombraña et al., 2012), or applying the steps of the Permission, Limited information, Specific Suggestions, and Intensive Therapy (PLISSIT) sexual health model (e.g., seeking or allowing patients to have sexual concerns) to collect information on sexuality (Lewis, 2000; Mkonyi et al., 2024). This information can cover many sexual function topics (Albaugh et al., 2002; Lewis, 2000; Mkonyi et al., 2024; Mola, 2015; Turkoski, 2008). Spiritual assessment usually heightened screening problems by asking sensitive questions related to negative relationships with partners, emotional and physical conditions of couples, current relationship concerns or any stressors, sexual relationship communication in couples, couples’ mutual mistrust, perceptions of losing support from partner or infidelity, or whether problems occurred frequently with their sexual partner, and sexual situation corresponded to detecting ED (Albaugh et al., 2002; Boyd, 2007; Lewis, 2000; Mkonyi et al., 2024; Mola, 2015; Primanda et al., 2023). In addition, studies underscored the duty of nurses performing individual examinations. Albaugh et al. (2002) expressed that qualified and trained nurses or physicians can perform physical examinations as a review of genito-urinary, endocrine, vascular, and neurologic systems; however, Boyd (2007) reported that physicians should undertake this physical examination to rule out alternative causes of sexual dysfunction. Nurses perform laboratory testing according to potential illness causes to rule out potential comorbid factors and abnormal findings using common testing techniques (Albaugh et al., 2002; Intili & Nier, 1998; Schreiber, 2019).
Patients’ Perspectives
One article reported that 55% patients with ED indicated it would be helpful if they could ask sexual questions while consultation with a nurse (Nicolai et al., 2014).
Specific Works of RNs
Studies stated that RNs should have special training in urology, or cardiology (Intili & Nier, 1998; Nicolai et al., 2014), perform assessments and discuss examination procedures with patients to identity risk factors of symptoms (Schreiber, 2019). Researchers have expressed that RNs may have knowledge of sexual health and erectile problem-related information to identify erectile problems and refer patients for appropriate therapy (Turkoski, 2008). If nurses lack assessment skills, assess to assessment and treatment facilities, or have uncertainly or inadequate training about ED management, they may refer patients to practitioners or physicians for further assessment or treatment (Albaugh et al., 2002; Mkonyi et al., 2024). Studies have shown that RNs should act as active listeners and promote dialogue with patients (Lombraña et al., 2012) and be sensitive to patient’s feelings and cultural or religious beliefs (Schreiber, 2019).
Specific Works of NPs
NPs have the function of monitoring laboratory data, ordering laboratory testing (Albaugh et al., 2002), and referring to or consulting specialists if need further therapy (e.g., abnormal testosterone levels, uncontrolled blood pressure, or overweight in patients) (Boyd, 2007), and referral to or consultation with a physician or specialist for further management if lacks of training or skills, complicated mental or couples’ problems (Albaugh et al., 2002; Boyd, 2007).
Needs Clarification and/or Diagnosis
Studies highlighted that patients have unmet needs regarding ED (Schreiber, 2019). Nurses have a duty to sensitively identify patients’ or couples’ individual needs and expectations. In addition, one article pointed out that nurses should provide emotional support and responsiveness to patients’ unmet needs and expectations (Mkonyi et al., 2024).
Specific Works of RNs
RNs’ have a duty to use the PLISSIT sexual health model (e.g., provide limited information) to help assess and understand the potential physical and psychological causes of the disease (Mkonyi et al., 2024). Lombraña et al. (2012) expressed the importance of RNs in promoting sexual health and addressing sexuality concerns among patients and the influence of chronic illness.
Specific Works of NPs
Studies have indicated that NPs should have clinical knowledge and communication skills (Burbage-Vieth, 2020; Lewis, 2000) and perform and order diagnostic tests (Lewis, 2000). NPs use PLISSIT sexual health model (e.g., to deal with specific sexual problems, dispel myths, and provide specific information) to sensitively understand and identify patients’ or couples’ opinion about sexual matters (Lewis, 2000).
Individual or Couple Education
Nurses’ Perspectives
Nurses have a duty to educate patients or couples, primarily regarding the physiology and relationship of sexuality. Articles demonstrated that enhanced knowledge about the physiology of sexuality includes direct education about sexual health, treatment options, and lifestyle modification (Albaugh et al., 2002; Boyd, 2007; Intili & Nier, 1998; Lewis, 2000; Lombraña et al., 2012; Mkonyi et al., 2024; Mola, 2015; Nicolai et al., 2014; Peate, 2012; Schreiber, 2019; Turkoski, 2008). Two articles pointed out the major causes and consequences and risks and benefits of treatments, including medication effects or illness-induced sexual problems that induce erectile problems (Albaugh et al., 2002; Boyd, 2007). Patient Education includes discussions related to treatment options available before and after treatment of ED (Albaugh et al., 2002; Intili & Nier, 1998), making treatment decisions, and problem prevention (Albaugh et al., 2002; Boyd, 2007; Intili & Nier, 1998; Lewis, 2000; Lombraña et al., 2012; Mola, 2015; Nicolai et al., 2014; Peate, 2012; Schreiber, 2019; Turkoski, 2008).
Two articles demonstrated knowledge about sexuality and provided information on sexual communication and stimulation. Albaugh et al. (2002) demonstrated that engaging in forms of sensate-focused body massage to improve sexual intimacy, using techniques such as books or videotapes for arousing, or satisfying sexual partners’ sexual needs helps to increase sexual communication and sexual stimulation.
Patients’ Perspectives
One article stated that 58% of patients expressed it would be helpful if they could consult with a nurse and receive written information about treatment options (Nicolai et al., 2014).
Specific Works of RNs
Studies have shown that RNs use the steps of the PLISSIT sexual health model (e.g., provide specific suggestion) to educate and counsel about illness (Mkonyi et al., 2024). Four articles mentioned the valuable role of RNs as supporters of treatment adherence through the process of providing information to reduce a sense of stigma and embarrassment with sexual issues, and discussing realistic goals and achievable outcomes (Albaugh et al., 2002; Lombraña et al., 2012; Mola, 2015; Schreiber, 2019). One article expressed that RNs should educate patients to engage in other forms of counseling to resume their sexual intimacy without attempting penetration (Mola, 2015). Studies have indicated that RNs have up-to-date knowledge about ED to educate patients on the physiological impact of ED, identify any comorbid or medication-related potential impacts to erection function, and educate to help prevent potential harms of ED drugs (Turkoski, 2008). Several researchers expressed that RNs have a function to refer or consult with health care professionals, such as specialized nurse, practitioners, urologists, sexologists, or relationship therapists for further therapy if they lack comfort, skills, or training (Albaugh et al., 2002; Mkonyi et al., 2024; Mola, 2015; Nicolai et al., 2014; Turkoski, 2008).
Specific Works of NPs
NPs have a duty to coordinate with physicians and patients by communicating the appropriate medication for best erectile response, discussing with patients about appropriate treatments and possible side effects (Boyd, 2007). They use the steps of the PLISSIT sexual health model (e.g., solving specific sexual problems, defining course of therapy, and understanding the patient’s ideas about sexual problem and goals for therapy) to deliver correct information (Lewis, 2000). Two articles stated that NPs require counseling skills to providing suggestions for couples counseling to further discuss their likes and dislikes, encourage intimacy and interest in each other’s bodies without intercourse (Lewis, 2000; Nicolai et al., 2014), and closely collaborate with professional specialists for further advice (Albaugh et al., 2002). In addition, Boyd (2007) expressed that NPs have knowledge about chronic illness and appropriate therapy for ED, including diabetic causes to ED, the effectiveness and appropriate doses of therapeutic interventions, and possible side effects to assist patients in receiving the appropriate treatment. Two articles mentioned that NPs may refer to specialists or urologists for consultation if they are suffering from uncertainty of how to manage conditions or if patients need further invasive diagnostic procedures or surgical intervention. Referring to psychosexual counselors may also happen if they do not address patients’ psychological problems themselves (Boyd, 2007; Lewis, 2000).
Facilitation and/or Provision of Treatment
Nurses have the function of providing appropriate information about medical treatments, discussing the pros and cons of each therapy, informing patients of the impact of lifestyle and sexual practice, and providing appropriate therapy according to each patient’s erectile problem (Albaugh et al., 2002; Lewis, 2000).
Specific Works of RNs
Studies have demonstrated that RNs are responsible for facilitating appropriate interventions or treatments to improve couples’ sexual health (Primanda et al., 2023) and resolving doubts about the treatment of ED (Lombraña et al., 2012). They use the steps of the PLISSIT sexual health model (e.g., intensive therapy) help to provide counseling and medication to manage the disease (Mkonyi et al., 2024). Articles showed that nurses apply a multidisciplinary team approach to account for comorbidities, such as internal referrals (e.g., within the same unit facility) or referring externally (e.g., higher-level unit facilities) according to the severity of illness, to ensure patients to get the appropriate services (Mkonyi et al., 2024; Schreiber, 2019).
Specific Works of NPs–Nurses’ Perspectives
NPs have the function to providing adequate information for patients to make treatment decisions, or using the steps of the PLISSIT sexual health model (e.g., provide interventions, and offer specialized treatment skills) to help patients to achieve better control of existing health problems (Lewis, 2000). Five articles mentioned NPs providing individualized suggestions regarding specific issues with patients or couples (Lewis, 2000; Mkonyi et al., 2024), discussing drug therapies, such as available offerings and dose titration (Boyd, 2007), prescribing medications or provide intervention or specialized treatment therapies, including oral medications and hormone therapy (Albaugh et al., 2002; Burbage-Vieth, 2020; Lewis, 2000), vacuum erection devices and intracavernous injections (Burbage-Vieth, 2020), and treatment with ED comorbidities (Burbage-Vieth, 2020). Studies indicate that NPs should have up-to-date clinical knowledge and communication skills (Lewis, 2000). Using a multidisciplinary approach to manage ED, such as referral for specialist consultation (e.g., psychology, psychiatry, endocrinology, and pharmacy) can help to improve quality of care; referring a patient who needs surgical treatment of invasive diagnostic procedures to a urologist can help to provide a comprehensiveness care (Burbage-Vieth, 2020; Lewis, 2000).
Specific Works of NPs–Patients’ Perspectives
One article mentioned that 65% of patients used a Phosphodiesterase 5 inhibitors (PDE5 inhibitors) that was prescribed by nurse practitioner (Nicolai et al., 2014).
Continuous Monitoring
Articles pointed out that nurses are responsible for continuing follow-ups (e.g., pre-and post-therapy periods) as well as supporting treatment adherence (Lombraña et al., 2012; Mkonyi et al., 2024; Nicolai et al., 2014), dosage titration, adjustment, further education, and medical and psychosocial reassessment with patients (Albaugh et al., 2002; Boyd, 2007; Lombraña et al., 2012).
Discussion
This review provides a comprehensive synthesis of the current literature on the multifaceted roles of RNs and NPs in managing ED, drawing attention to significant gaps in knowledge and care activities. In general, both RNs and NPs have knowledge about sexual health and can identify potential risk factors of ED. Nurses working or training in urology or cardiology environments are better versed in the nuances of erectile function compared with nurses working in other clinics. The findings support the need for structured role definitions and integration of sexual health competencies into nursing education and practice. Leadership within nursing management must prioritize ED-related education, especially for RNs who are often the first point of contact with patients, yet consistently report lower confidence in knowledge of sexual health assessment, treatment, and education. Moreover, urology physician organizations as well as urology nursing organizations should develop clinical guidelines and interprofessional pathways that empower NPs to act autonomously in laboratory data monitoring, patient diagnosis, counseling, invasive treatment, and collaboration with specialists to further provide surgical therapy or psychological or sexual counseling. Most NPs also play a role as sexual medicine specialists, thereby reducing care fragmentation and improving patient satisfaction.
Organizationally, the results underscore the importance of managerial support to foster environments where discussions of sexual health are normalized and encouraged. This includes access to continuing professional development, interdisciplinary referral systems, and time allocation for sensitive patient communications. As ED management intersects with physical, emotional, and psychosocial care domains, a holistic nursing approach—collaboration with interprofessional team members through enforced RNs and NPs responsibilities, effective health care team communication, mutual respect, and understanding of unique roles—will ensure more responsive and equitable care delivery.
The findings identify five major tasks of nursing practice in ED care: (1) risk factor assessment, (2) needs clarification and/or diagnosis, (3) individual or couple education, (4) facilitation and/or provision of treatment, and (5) continuous monitoring. RNs play a fundamental role in assessing and identifying the problem, promoting sexual health, educating and supporting treatment adherence, and facilitating interventions or treatments. In contrast, NPs have a distinct role in monitoring laboratory testing, diagnostics, counseling and treating patients, and collaborating with specialists. Both RNs and NPs use a multidisciplinary approach to provide care activities; RNs provide internal or external referrals for patients to get better services, while NPs refer to specialists or urologists to get comprehensive care. These findings underscore the need to enhance sexual health education and develop targeted training programs for nursing professionals, for RNs to improve their knowledge of assessment and education about ED care, and for NPs to improve their knowledge of diagnosis, counseling, treatment, and patient monitoring to ensure comprehensive and multidisciplinary ED team care.
Risk Factor Assessment
Tasks for risk factor assessment related to nurses were frequently identified in these articles. Numerous studies highlighted that asking patients about organic, psychogenic, sexual function problems, and relationship concerns, and conducting individual examinations and laboratory testing should be done to clarify any problems related to erectile function (Albaugh et al., 2002; Burbage-Vieth, 2020; Lombraña et al., 2012; Turkoski, 2008). Nurses inquire about sexual function using the steps of the PLISSIT sexual health model (e.g., seeking permission) to understand information related to sexual problems, sexual relationships, and treatment and medication used. This information helps nurses to effectively understand patients’ sexual concerns (Lewis, 2000; Mkonyi et al., 2024). Studies both from nurses’ perspectives and patients’ perspectives about nurses raising sexual issues with patients showed positive results; due to nurses having the time to discuss sexuality more than physicians. Nurses conducted problem identification via various forms, such as IIEF, IIEF-5, or SHIM (Albaugh et al., 2002; Burbage-Vieth, 2020; Lombraña et al., 2012; Mola, 2015; Primanda et al., 2023). Validated questionnaires such as IIEF, IIEF-5, SHIM, which also included Erection Hardness Score (EHS), were helpful to assess sexual function but were not a replacement for physical examination (Hackett et al., 2018; Liu et al., 2021). Nurses who conduct physical examinations may reveal unknown physical findings or provide reassurance about normal genital bodily structure (Albaugh et al., 2002); physicians or qualified and well-trained nurses performed physical examinations to rule out alternative causes of sexual dysfunction (Boyd, 2007). The BSSM (British Society for Sexual Medicine) guidelines recommend physicians perform physical examinations, such as blood pressure, heart rate, weight, waist circumference, and genital examination to detect potentially reversible causes of ED (Hackett et al., 2018). Specific work related to RNs highlights that nurses act as active listeners and promote dialogue to discuss issues affecting patients with ED (Lombraña et al., 2012). Articles emphasized that nurses with adequate urologic or cardiology training and knowledge about sex and ED play an important role in identifying risk factors by conducting comprehensive assessments and discussions of examination procedures with patients and referral to specialists (e.g., practitioners or physicians) for further assessment or therapy (Albaugh et al., 2002; Intili & Nier, 1998; Mkonyi et al., 2024; Nicolai et al., 2014; Turkoski, 2008). Sensitivity to patients’ feelings and cultural or religious beliefs is a vital function of nurses (Schreiber, 2019).
In contrast, physical examinations that usually emphasize the genitourinary, endocrine, vascular, and neurologic systems and are consistent with medical history, monitoring, or ordering laboratory testing should be performed by NPs with credentials. Referral to or consulting with physicians or specialists for further management may be necessary if the nurse lacks training or assessment skills, patients complicated mental or couples’ problems (Albaugh et al., 2002; Boyd, 2007).
Needs Clarification and/or Diagnosis
Recommendations for nurses mostly included guidance to sensitively find patients’ or couples’ individual needs and expectations through direct inquiry of sexual health (Lewis, 2000; Lombraña et al., 2012; Mkonyi et al., 2024; Schreiber, 2019). Knowing patients’ beliefs or religiosity, attitudes, and feelings related to masculinity and sexuality, intimate feelings, and the need for emotional closeness of individuality helps to identify the risk of psychosocial dysfunction and information needs (Lewis, 2000; Lombraña et al., 2012; Schreiber, 2019). Nurses who provide emotional support and responsiveness to patients’ unmet needs give them confidence in the new mastery they attain to provide appropriate treatment for patients (Mkonyi et al., 2024).
Specific work related to RNs has highlighted that RNs using the PLISSIT sexual health model (e.g., provide limited information) help to assess and understand the potential causes related to physical and psychological causes of the disease (Mkonyi et al., 2024). Nurses play an active role as an expert professional by listening and resolving doubts that patients have regarding mitigating erectile problems; nurses also may raise awareness of the importance of ED and promote sexual health among patients (Lombraña et al., 2012).
In contrast, the specific works of NPs should possess adequate clinical knowledge and communication skills to order diagnostic tests and clarify possible risk factors to ensure accurate diagnosis (Burbage-Vieth, 2020; Lewis, 2000). The general nurse practitioner’s role was highlighted as early diagnosis and management of cardiovascular or endocrine conditions (Hackett et al., 2018). Articles mentioned that NPs use the PLISSIT sexual health model (e.g., deal with specific sexual problems, dispel myths, and provide specific but not detailed information) to provide specific sexual health information to address patients concerns (Lewis, 2000).
Individual or Couple Education
Educating couples on treatment options allows them to make decisions related to treatments (Mola, 2015). Nurses need to help patients improve their erection problems and assist them in preventing cardiovascular problems (Peate, 2012). Studies both from nurses’ perspectives and patients’ perspectives about nurses who provide education options showed a positive effect. Nurses who provide advice about available treatment can help patients to make therapy decision. In addition, regular stimulation, regular intercourse, and frequent morning erections may promote erection (Mola, 2015). Enhancing knowledge about the relationship between sexuality and patients encompasses information on sexual communication and stimulation.
Specific work related to RNs has highlighted that using the steps of the PLISSIT sexual health model (e.g., provide specific suggestions) can also be used to provide education and counseling about illness (Mkonyi et al., 2024). RNs play a supportive role by providing support for treatment adherence to reduce the sense of stigma and embarrassment with sexual issues, and discussing realistic goals and achievable outcomes with patients (Albaugh et al., 2002; Lombraña et al., 2012; Mola, 2015; Schreiber, 2019). RNs educate patients on other forms of counseling to resume their sexual intimacy without attempting penetration, which helps patients to get adequate knowledge on ED (Mola, 2015). RNs in interprofessional primary care teams have focused primary on patient-centered care to provide health promotion with patients (Cappiello et al., 2016; Saus-Ortega et al., 2021). To date, knowledge about ED regarding illness or mental health has negatively affected erection and mediation hesitation; available treatment helps nurses educate patients (Peate, 2012; Turkoski, 2008). Knowledge about ED helps nurses identify problems, educate patients to avert potential harm, and provide referrals for specialist therapy (Turkoski, 2008). Referral or consultation with health care professionals has emphasized the function of nurses due to lack of comfort, lack of available skills, lack of training in ED, and interpersonal problems between couples (Albaugh et al., 2002; Lombraña et al., 2012; Mkonyi et al., 2024; Mola, 2015; Nicolai et al., 2014; Turkoski, 2008).
The specific works of NPs acts as a coordinator between physicians and patients to communicate, with appropriate medicine and erectile responses, by discussing suitable treatments with patients (Boyd, 2007). This coordination ensures that patients receive safe and effective treatment and are educated regarding the chosen therapy. They use the steps of the PLISSIT sexual health model (e.g., solving specific sexual problems, defining course of therapy, and understanding the patient’s ideas about sexual problem and goals for therapy) to solve specific problems identified by clinicians (Lewis, 2000). Providing suggestions for couples counseling and paying attention to intimacy or each other’s bodies without intercourse (Lewis, 2000) helps resolve psychological or interpersonal problems and achieve intimacy within couples (Albaugh et al., 2002; Lewis, 2000). NPs in interprofessional primary care teams have population-focused professional competence to address the unique needs of specific patients (Cappiello et al., 2016; Saus-Ortega et al., 2021). Giving adequate training for nurse specialists can help to identify the unmet needs of patients and provide information related to treatment. The role of NPs in ED management may allow patients to move toward successful treatment and generate patient referrals (Lewis, 2000). Referring to specialists can help patients provide education, assessment, and treatment of symptoms (Boyd, 2007).
Facilitation and/or Provision of Treatment
Tasks of facilitation and/or provision of treatment related to nurses have demonstrated that helping couples find suitable treatments that best fit their needs by discussing the risks and benefits of available treatment in detail, understanding the impact on lifestyle and sexual practice, to assisting patients in finding the treatment options that best fit their needs (Albaugh et al., 2002; Lewis, 2000). The information on treatment options should be provided with accurate, clear, and emotional expressions to help patients make informed choices (Albaugh et al., 2002).
Specific work related to RNs has highlighted that nurses have facilitated suitable treatments and resolved the problems of patients (Lombraña et al., 2012; Primanda et al., 2023). Nurses are able to propose solutions and treatments best fit each individual (Lombraña et al., 2012). They use the steps of the PLISSIT sexual health model (e.g., intensive therapy) to provide counseling and medication to manage the disease (Mkonyi et al., 2024), and apply a multidisciplinary team approach to account for comorbidities, such as internal or external referrals (Mkonyi et al., 2024; Schreiber, 2019). RNs in multidisciplinary teams play a key role among internal stakeholders (e.g., physicians, NPs, or other specialists) and external stakeholders (e.g., patients) (Cappiello et al., 2016; Saus-Ortega et al., 2021).
Conversely, the specific works of NPs have provided treatments for patients, including offering the choice of treatment according to individual’s needs, and giving information to make an informed choice (Lewis, 2000), providing suggestions to solve problems (Lewis, 2000; Mkonyi et al., 2024), prescribing medications or specialized treatment therapies (e.g., oral therapies, vacuum devices, and intracavernous injections) (Albaugh et al., 2002; Burbage-Vieth, 2020; Lewis, 2000), and addressing comorbidities of ED (Burbage-Vieth, 2020). Using a multidisciplinary approach to manage of ED, including referral for specialist consultation (Burbage-Vieth, 2020; Lewis, 2000), such as a urologist indicated that the erectile condition is deemed end stage and need urological surgeons; a psychologist or psychiatrist indicated that patients accept any specific physical or psychological treatments (Hackett et al., 2018).
Continuous Monitoring
Nurse tasks of continuous monitoring include support for treatment adherence, dosage adjustment or further education, and medical and psychosocial reassessment with patients (Albaugh et al., 2002; Boyd, 2007; Lombraña et al., 2012; Nicolai et al., 2014). Nursing programs aim to enable patients to benefit from treatments and improve their care goals; regular follow-up visits are essential to monitor that process and identify problems related to ED (Lombraña et al., 2012).
This review examined various research methodologies related to the nursing management of ED; however, the synthesis of findings was primarily based on textual data and expert opinion studies, which may limit the strength of the conclusions. While the inclusion of both qualitative and quantitative studies provided valuable insights into the roles of nursing professionals in ED care, further research incorporating objective clinical outcomes and broader empirical evidence is needed to enhance the robustness of these findings. In addition, the meta-analysis was not performed due to heterogeneity of the research methodology, which may limit subgrouping disease conditions and decrease analytical depth in our results summarizing the disease contexts represented in the included studies, such as diabetes mellitus, cardiology, urology, and prostate cancer with radical prostatectomy (Supplementary Table 1). Future studies should propose disease-specific subgrouping as a direction for research. Furthermore, this review was restricted to studies published in English, which may limit the generalizability of the findings. Including research from non-English sources could provide a more comprehensive understanding of global nursing practices in ED management.
Conclusion
This mixed-method systematic review highlights the critical role of nursing professionals in the management and promotion of sexual health among patients with ED. The findings identify vital tasks of nursing practice in ED care: (1) risk factor assessment, (2) needs clarification and/or diagnosis, (3) individual or couple education, (4) facilitation and/or provision of treatment, and (5) continuous monitoring. RNs play a fundamental role in assessing and identifying the problem, promoting sexual health, educating and supporting treatment adherence, and facilitating interventions or treatments. In contrast, NPs have a distinct role in monitoring laboratory testing, diagnostics, counseling and treating patients, and collaborating with specialists. Both RNs and NPs use a multidisciplinary approach to provide care activities; RNs provide internal and external referrals, while NPs refer to specialists or urologists’ consultation to get comprehensiveness care. These findings underscore the need to enhance sexual health education and develop targeted training programs for nursing professionals, for RNs to improve knowledge of assessment and education about ED care, and for NPs to improve knowledge of diagnosis, counseling, treatment, and patient monitoring to ensure comprehensive and multidisciplinary ED team care.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883261426900 – Supplemental material for Nurses’ Roles in Managing Erectile Dysfunction: A Mixed-Method Systematic Review
Supplemental material, sj-docx-1-jmh-10.1177_15579883261426900 for Nurses’ Roles in Managing Erectile Dysfunction: A Mixed-Method Systematic Review by Hui-Chun Chen, Chieh-Yu Liu and Chun-Hou Liao in American Journal of Men's Health
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to all the researchers whose work contributed to this review. Special thanks are extended to Dr. Chun-Hong Chang for providing guidance during the systematic review process. We also appreciate the support of National Science and Technology Council and the contributions of peer reviewers whose insightful feedback helped improve the quality of this manuscript.
Ethical Approval
This study involved the analysis of publicly available data derived from previously published literature. No human participants were directly recruited, and no identifiable private information was accessed. In accordance with institutional and international research guidelines, studies based exclusively on publicly available secondary data are exempt from institutional review board approval.
Informed Consent
Because this study utilized publicly available data from existing literature and did not involve direct interaction with human participants or access to identifiable personal information, informed consent was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants NSTC112-2314-B-255-001-MY2 from the National Science and Technology Council of Taiwan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analyzed in this review are derived from previously published studies, which are publicly available through academic databases. No new data were generated or collected during this study. A full list of included studies is available upon request. The data that support the findings of this study are available from the corresponding author, Chieh-Yu Liu, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.