
Abstract
This study aimed to assess men’s health awareness, attitudes, and use of primary health care (PHC) services in Almaty across occupational groups. A cross-sectional study was conducted among men aged 18 and older, recruited from four occupational groups: office employees and civil servants, military personnel, industrial and service workers, and unskilled laborers. The results showed that men often pay insufficient attention to their health, with clear disparities across occupational groups. Men in unskilled professions demonstrated the riskiest health behaviors, including earlier initiation of smoking and alcohol consumption, more frequent drinking (two to three times per week, p = .005), and lower physical activity (p = .004). This group also showed lower health literacy and lower trust in the health care system, while visiting public polyclinics more frequently (38.6% visited three to five times per year, p = .005), likely for acute conditions rather than preventive care. At the same time, 72.6% of office workers reported significant gaps in knowledge about chronic diseases and self-management skills, despite their higher educational level. Logistic regression analysis identified satisfaction with care quality (adjusted odds ratio [AOR] = 4.27), adherence to doctors’ recommendations (AOR = 3.24), and regular visits to private clinics (odds ratio [OR] = 2.86) as the most stable predictors of health care engagement. These findings suggest that PHC services in Almaty should better respond to the needs of men working in different occupational contexts. Improving health literacy, addressing structural and behavioral barriers, and implementing workplace-based health interventions may help encourage earlier and more consistent use of preventive services.
Keywords
Introduction
The Sustainable Development Goals (SDGs) aim to achieve universal health coverage (UHC) by 2030, which means ensuring that all people have access to affordable and quality health services, including health promotion, prevention, treatment rehabilitation, and palliative care, without financial constraints (World Health Organization [WHO], 2019). The quality of health care can be defined as the ability of patients to access necessary health services and achieve expected outcomes (Stein et al., 2015). Improving patient satisfaction is a central goal of the health care system (Reed et al., 2021). Understanding how individual expectations influence satisfaction with medical services, including the comparison of personal experiences with expectation, is a key issue in this context (Batbaatar et al., 2015; Dyer et al., 2016; Will et al., 2019).
Low quality of medical care, including reduced patient satisfaction, can lead to more frequent hospitalizations and increased health care costs. Identifying patient needs is essential for improving the organization and delivery of services (Alnemer et al., 2015; Xesfing & Vozikis, 2016). Patient care should remain the primary focus of health care personnel, with patient satisfaction being a critical component of service delivery (Leźnicka et al., 2014).
In recent years, greater attention has been given to the specific needs and experiences of different patient groups (Beck et al., 2019; Birkelien, 2017). Patient satisfaction may depend on multiple factors, including demographic and socio-cultural characteristics such as age, gender, education, religion, ethnicity, and marital status (Adhikari et al., 2021; Gupta et al., 2012).
The study of men’s health is an important element in addressing health disparities and inequalities. Interest in this area stems from the recognition of specific risks and vulnerabilities faced by men and the importance of integrating them into gender-sensitive health programs (Oliffe, 2023). According to the Bureau of National Statistics Agency of the Republic of Kazakhstan (2024), over the past two decades, there has been a significant difference in life expectancy, with men having about 7–8 years lower compared to women.
To examine in greater detail the challenges faced by men working in various sectors when accessing primary health care (PHC), as well as their attitudes toward the quality of care and their awareness of health issues, our research team conducted a survey among the male population. The purpose was to provide health care managers evidence to inform decision-making and guide the development of targeted interventions.
Materials and Methods
Organization and Data Collection
A cross-sectional study was conducted in Almaty. The questionnaire was designed to assess men’s awareness of health issues and their use of PHC services in Almaty. It consisted of four sections: (a) attitudes toward personal health; (b) awareness of a healthy lifestyle; (c) perceptions of the quality and accessibility of health services; and (d) barriers to accessing health services, along with demographic information.
The questionnaire was developed in Russian and Kazakh by three public health researchers. It was peer-reviewed by two independent, fluently bilingual public health experts. Following initial modification, the questionnaire was pilot-tested with 12 male respondents of different ages to evaluate clarity and readability. Respondents were invited to suggest alternative wording for questions to ensure cultural and linguistic appropriateness. After incorporating feedback, the revised questionnaire was reviewed by two additional external reviewers.
Men aged 18 years and older were eligible to participate. Data collection took place between October 2023 and February 2024, using both online and paper-based formats. The online survey was distributed via PHC nurses providing preventive services to their catchment populations. Paper questionnaires were distributed at workplaces, including bus stations, construction companies, and cleaning services organizations in Almaty. Each questionnaire included a question about the participant’s occupation. For analysis, occupations were grouped into four categories: (a) administrative, managers, and civil servants (office workers); (b) military personnel; (c) industry workers, technical and production specialists, construction and transport workers, service staff, and sales personnel; and (d) unskilled workers, including auxiliary laborers, production equipment operators, assemblers and cleaners, warehouse workers, etc.
Participation was voluntary and anonymous. Written informed consent was obtained from all participants prior to inclusion in the study. The consent form explained the purpose of the research, procedures, potential risks and benefits, confidentiality measures, and the right to withdraw at any time without consequences. Participants completed the survey independently, and contact details of the research team were provided at the beginning of the questionnaire for any questions or clarifications.
Data Analysis
The sample size was calculated based on the total number of men aged 18 years and older residing in Almaty (651,887). With a precision level of 5% and a 95% confidence interval (CI), the minimum required sample was 384 respondents. To account for possible attrition or incomplete questionnaires, the target sample was doubled to 768. A total of 768 responses were collected (400 paper-based, 368 online). After quality control, 47 questionnaires were excluded due to missing or erroneous data, resulting in a final analytical sample of 721 respondents.
Descriptive statistics were used to summarize demographic characteristics and overall response distributions. Frequencies, proportions, and 95% CIs were reported. Wilson’s method was applied to calculate CIs for proportions.
Bivariate comparisons were conducted to examine associations between occupational group and key outcomes, including attitudes toward health care, perceived accessibility, and satisfaction with services.
Binary logistic regression analysis was used to evaluate the association between respondents’ attitudes toward medical personnel and various predictor variables (Bühl & Zöfel, 2005). This method of multivariate analysis approach was chosen to control for potential confounding variables and to account for the combined influence of all independent variables in the model. Respondents’ attitudes toward health care workers were entered into the logistic regression model as independent categorical variables.
The strength of associations between predictors and the outcome variable was expressed in terms of odds ratios (ORs) with corresponding 95% CIs. Unadjusted ORs were obtained from univariate regression analyses, assessing each factor independently. Adjusted ORs, controlling for other covariates, were obtained through multivariate regression using the forced entry method. A p-value of less than .05 was considered statistically significant (Grjibovski et al., 2016).
All statistical analyses, including binary logistic regression and exploratory factor analysis, were performed using SPSS software version 13.0 (IBM Corp., Armonk, NY, USA).
Ethical Approval
The research received approval from the Local Ethics Committee (IRB00011496) under protocol number No. 4 (140), dated May 3, 2023.
Results
A total of 721 men participated in the survey, with the majority belonging to Groups 1 and 3. About one-third of respondents were unmarried (30.2%), most of them aged 30–44 years (37.6%). Higher education was most common among men from Group 1 (62.2%), whereas only 9.1% from Group 4 reported having higher education. In contrast, men in Groups 2 and 4 were more likely to have secondary specialized education (51.4% and 63.6%, respectively). Most men with average income levels belonged to Groups 1 and 3, while the lowest income was reported among men in Groups 2 and 4 (64.9% and 40.9%, respectively; Table 1).
Characteristics of the Survey Participants.

Note. Group 1—employees in the field of administration, managers, and civil servants (office workers); Group 2—military personnel; Group 3—industrial workers, technical and production specialists, construction and transport workers, service sector, and sellers; Group 4—handymen as unskilled auxiliary workers, operators of production equipment, assemblers and cleaners, warehouse workers, etc.
Men’s Awareness of Behavioral Risk Factors
Significant differences between occupational groups were observed in several behavioral risk factors (Table 2). Men in Groups 3 and 4 reported starting smoking at a younger age compared to other groups (p = .011). Similarly, the age of first alcohol consumption was lower among Groups 3 and 4 (p < .001). Frequency of alcohol consumption differed significantly: men in Group 4 reported drinking two to three times per week more often than other groups (p = .005). In addition, higher per-occasion alcohol intake (five to six units or more) was significantly more common among Groups 3 and 4 (p = .007). Physical activity levels varied across groups, with men in Group 4 less likely to engage in regular activity (p = .004).
Men’s Awareness and Behavioral Risk Factors.

Note. Group 1—employees in the field of administration, managers, and civil servants (office workers); Group 2—military personnel; Group 3—industrial workers, technical and production specialists, construction and transport workers, service sector, and sellers; Group 4—handymen as unskilled auxiliary workers, operators of production equipment, assemblers and cleaners, warehouse workers, etc.
Men’s Attitudes Toward Their Health
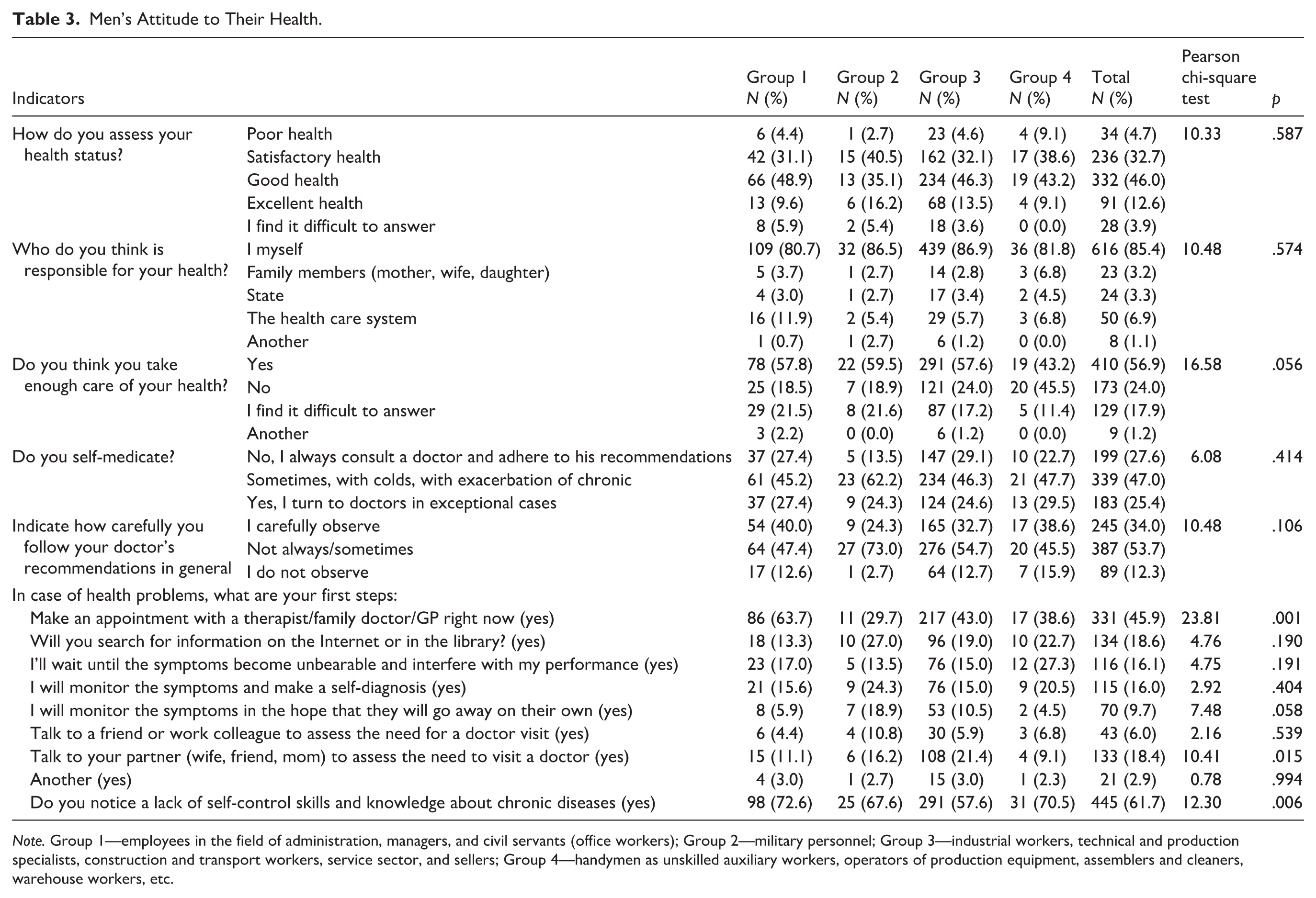
Overall self-assessment of health status did not differ significantly across groups, with only 4.7% reporting poor health (Table 3). However, significant differences emerged in health-seeking behavior and self-care practices. Men from Group 4 were more likely to report insufficient attention to their health (45.5% vs. 18–24% in other groups, p = .056). When facing health problems, men from Group 1 were most likely to seek immediate medical consultation (63.7%), whereas this behavior was far less common among Groups 2 (29.7%) and 4 (38.6%; p < .001). In contrast, men from Group 3 were more likely to discuss symptoms with a partner before deciding whether to visit a doctor (21.4% vs. 11.1% in Group 1 and 9.1% in Group 4, p = .015). Recognition of insufficient self-management skills and limited knowledge of chronic diseases was significantly higher among Groups 1 (72.6%) and 4 (70.5%) compared to Group 3 (57.6%; p = .006).
Men’s Attitude to Their Health.
Note. Group 1—employees in the field of administration, managers, and civil servants (office workers); Group 2—military personnel; Group 3—industrial workers, technical and production specialists, construction and transport workers, service sector, and sellers; Group 4—handymen as unskilled auxiliary workers, operators of production equipment, assemblers and cleaners, warehouse workers, etc.
Satisfaction With the Quality of Medical Care
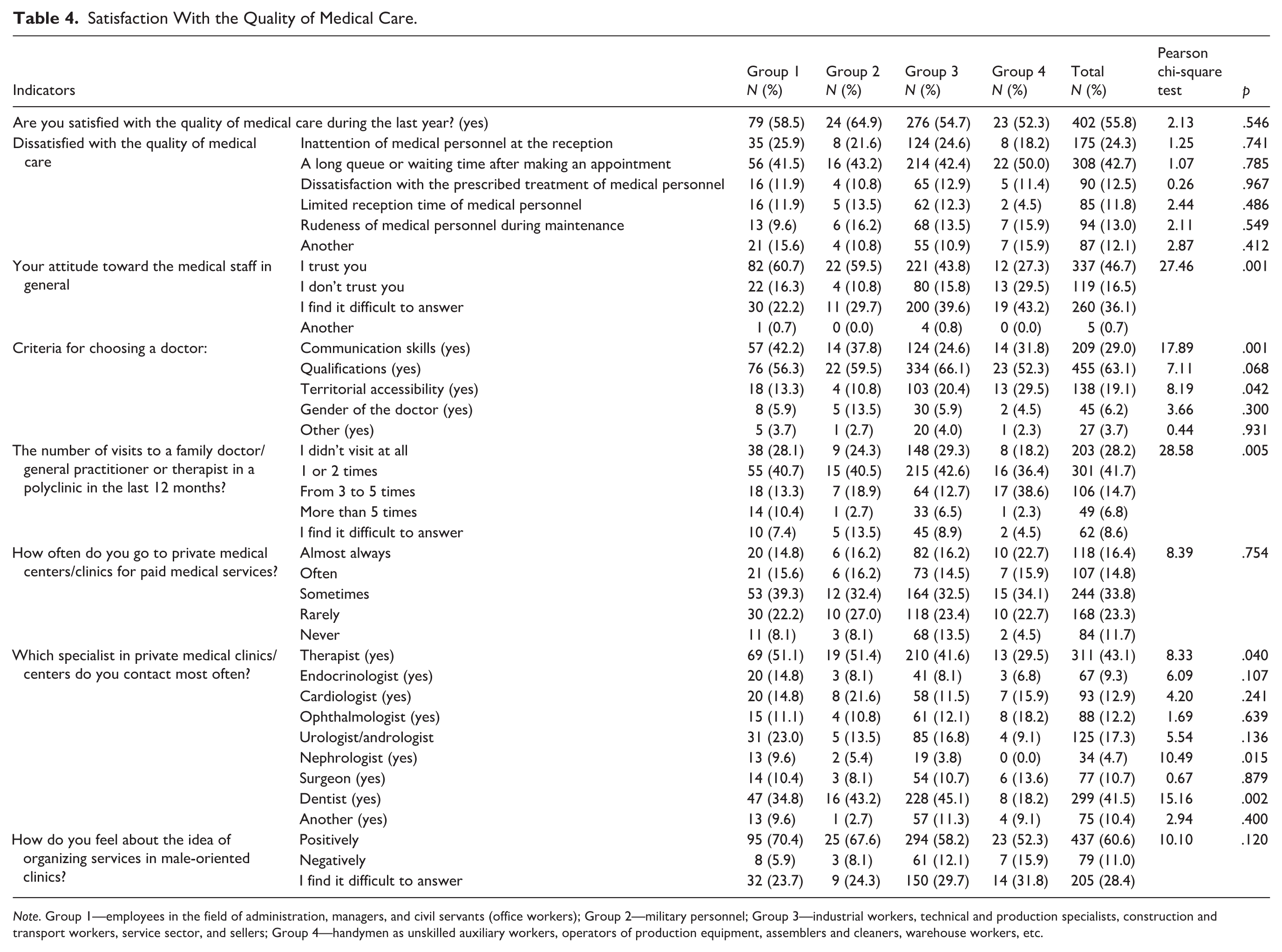
A total of 55.8% of men reported being satisfied with the quality of medical care, with no statistically significant differences between groups (Table 4). However, trust in medical staff varied: the highest levels of trust were observed in Groups 1 (60.7%) and 2 (59.5%), whereas in Groups 3 (43.8%) and especially 4 (27.3%), distrust or hesitation prevailed (p < .001). When choosing a doctor, men from Groups 1 and 2 more often prioritized communication skills (42.2% and 37.8%), while Groups 3 and 4 were more likely to consider territorial accessibility (20.4% and 29.5%; p < .001 and p = .042). Significant differences were found in the frequency of visits: men from Group 4 more often visited polyclinics three to five times per year (38.6%), whereas Groups 1–3 tended to limit themselves to one to two visits or none at all (p = .005).
Satisfaction With the Quality of Medical Care.
Note. Group 1—employees in the field of administration, managers, and civil servants (office workers); Group 2—military personnel; Group 3—industrial workers, technical and production specialists, construction and transport workers, service sector, and sellers; Group 4—handymen as unskilled auxiliary workers, operators of production equipment, assemblers and cleaners, warehouse workers, etc.
When turning to private medical centers, men most often sought care from general practitioners and dentists, reflecting both the demand for basic primary care and the fact that dental services are not covered by the national insurance system. At the same time, men from Group 4 were the least likely to visit general practitioners (29.5%) and dentists (18.2%; p = .040 and p = .002), which is likely linked to financial constraints. In contrast, Groups 1 and 3 more frequently used private health care services, which may indicate dissatisfaction with the quality and accessibility of care in the public sector.
Thus, men in Group 4 demonstrate the lowest level of trust in medical staff but, paradoxically, visit public polyclinics more often, most likely due to acute health problems and limited access to private medicine. In comparison, Groups 1 and 3 more actively rely on private health care as a way to compensate for the barriers in the public system.
Barriers to Receiving Medical Care
Men in Group 4 were more likely than others to report the remote location of clinics (36.4%; p = .042) and the lack of proper organization of medical services (20.5%; p = .038; Table 5). At the same time, staff shortages at the polyclinic level were more often noted in Groups 1 (21.5%) and 3 (18.4%) compared with Group 4 (4.5%; p = .028). In addition, men from Group 2 (40.5%) and Group 4 (29.5%) significantly more often than those from Group 1 (17.0%) expressed confidence in managing health problems independently (p = .019). Thus, men in Group 4 not only visit polyclinics more frequently (see Table 4) but also more often express confidence in their ability to cope with health problems independently. This likely reflects not a preventive approach but rather the necessity to address acute health issues in the context of limited resources and lower trust in the health care system.
Barriers to Receiving Medical Care.

Note. Group 1—employees in the field of administration, managers, and civil servants (office workers); Group 2—military personnel; Group 3—industrial workers, technical and production specialists, construction and transport workers, service sector, and sellers; Group 4—handymen as unskilled auxiliary workers, operators of production equipment, assemblers and cleaners, warehouse workers, etc.
Determinants of Men’s Health-Seeking Behavior Were Examined Using Binary Logistic Regression
The results, presented in both unadjusted and adjusted models, revealed several important factors associated with men’s health-seeking behavior (Table 6). Men who carefully followed their doctor’s recommendations were significantly more likely to engage with health care services (adjusted odds ratio [AOR] = 3.24; 95% CI = [1.25, 8.42]). Similarly, overall satisfaction with the quality of medical care showed a strong positive association (AOR = 4.27; 95% CI = [2.41, 7.57]). Regular visits to private clinics were positively linked to greater health care engagement (OR = 2.86; 95% CI = [1.49, 5.48]).
Logistic Regression Analysis of Determinants of Men’s Health-Seeking Behavior.

Other factors demonstrated significance only in unadjusted analyses. Men who practiced self-medication or visited doctors only in exceptional cases were less likely to access services (OR = 2.79; 95% CI = [1.72, 4.53]). Dissatisfaction due to inattentiveness or rudeness of medical staff (OR = 3.74; 95% CI = [2.04, 6.87]), perceived staff shortages (OR = 2.09; 95% CI = [1.29, 3.39]), unfriendly attitudes of health workers (OR = 2.35; 95% CI = [1.27, 4.34]), misconceptions about preventive screening (OR = 2.39; 95% CI = [1.08, 5.27]), and the belief that seeking medical help is a sign of weakness (OR = 2.42; 95% CI = [1.01, 5.76]) were all associated with reduced health care utilization before adjustment, but these associations weakened in multivariate models.
Discussion
Unskilled workers (Group 4) demonstrate high-risk health behaviors in early-age initiation of smoking and alcohol use, frequent drinking, low physical activity, and low health literacy. In addition, we identified a low level of trust in the health care system alongside more frequent visits to PHC services compared to men in other occupational groups, which is most likely related to acute health conditions rather than preventive measures. Similarly, the low health literacy highlighted among men is often associated with risky behavior and insufficient attention to disease prevention (Furuya et al., 2015; Svendsen et al., 2021; Vejrup et al., 2025).
A lack of knowledge about chronic diseases and self-management skills was characteristic not only of vulnerable, less-educated men but also of more highly qualified workers (Group 1). The high prevalence of self-reported knowledge gaps among office workers aligns with studies conducted in Malaysia, where men with higher education demonstrated insufficient awareness of health screening procedures despite greater familiarity with health promotion measures (Ng et al., 2020; Teo et al., 2017).
Taken together, these results highlight that low health literacy, lack of trust in the health care system, and barriers to accessing quality services are characteristic not only of vulnerable, less-educated men but also of more educated groups, although the mechanisms of these differences vary. Therefore, in developing PHC services, it is essential to consider the socio-professional aspect of health literacy and to design strategies aimed at improving the accessibility of preventive programs and strengthening trust in the health care system among men across different occupational groups.
Men with colds and exacerbations of chronic diseases often resort to self-medication or consult doctors only in exceptional cases, while the majority report a lack of self-management skills and insufficient knowledge about chronic conditions. Previous studies suggest that such behavior may be influenced by dominant male norms, including competitiveness, strength, and confidence in one’s own abilities, which make men more inclined to independently seek information before visiting medical institutions (Rosu et al., 2017).
The results showed that men often discussed health problems with their partners or family members before deciding to visit a doctor. This emphasizes the role of family support in shaping men’s health-seeking behavior. Similar patterns have been observed internationally, where partners and close relatives serve as mediators in men’s access to health care (Forbat et al., 2014; Nyamai et al., 2022; Son et al., 2022). Involving family members in health communication and decision-making may represent an important strategy to increase men’s participation in preventive care and timely medical consultations.
When choosing a physician, men most often prioritized a doctor’s qualifications, communication skills, and territorial accessibility of medical facilities. These findings are consistent with international evidence showing that professional competence and respectful physician–patient communication are key factors in fostering trust and encouraging health care utilization (Grant, 2009; Lerch et al., 2024; Smith et al., 2008). At the same time, evidence shows that territorial accessibility is a critical factor, as poor geographic access reduces health care utilization (Hsu et al., 2018).
This study highlights that one of the main reasons why men avoid visiting PHC is their confidence in being able to manage their health independently, along with fears of potential financial costs, a lack of clear information about how medical services are organized and delivered, and competing life priorities. It was identified that unskilled workers are significantly less likely to use private clinics, which is most likely due to low wages. In addition, we identified that most men prefer private PHC services, primarily visiting dentist, therapist, cardiologist, and urologist/andrologist. Under the compulsory medical insurance system, services from all these specialists, except dentists, who are covered only for certain population groups, are available (Government of the Republic of Kazakhstan, 2019). This preference for private care may stem from dissatisfaction with previous public PHC experiences or low awareness of available services, both of which contribute to high out-of-pocket health care spending in Kazakhstan (Shaltynov et al., 2024). Our study identified several factors contributing to men’s dissatisfaction with medical services, including perceived inattentiveness of medical staff, long wait times, inconvenient appointment schedules, difficulty accessing specialists, and remote clinic locations. These barriers often lead men to seek private care and highlight that health care services are not well tailored to their needs. Enhancing communication quality in health care settings could help address these challenges, particularly for patients with limited health literacy. Barriers to men’s participation in health care include lack of health insurance, beliefs about masculinity that conflict with sexual and reproductive health care, stigma associated with accessing services, and lack of knowledge about available services (Burns et al., 2021).
The logistic regression analysis identified three stable predictors of men’s health care-seeking behavior: satisfaction with the quality of care, adherence to doctors’ recommendations, and regular visits to private medical centers. These findings are consistent with international evidence showing that positive experiences with the health care system and higher levels of trust in medical personnel are strongly associated with increased patient engagement (Mbokazi et al., 2020; Tong et al., 2011). Adherence to medical advice has been recognized as a key determinant of the effectiveness of both preventive and treatment programs (Vincent et al., 2018; Wynia & Osborn, 2010). Finally, regular visits to private clinics may also reflect attempts to compensate for barriers in the public health care system, as private facilities are often better equipped and more responsive (Berendes et al., 2011). Taken together, these results underscore the importance of improving satisfaction with health care quality and supporting adherence to medical recommendations as strategies to strengthen men’s trust in the health care system and enhance their participation in preventive and treatment programs.
Nurse practitioners play a key role in engaging men in community-based interventions, as seen in the Australian Bendigo model, where comprehensive health assessment, education, and flexible services, including workplace and after-hours care, are effectively delivered through a men’s health clinic (Strange & Tenni, 2012).
Limitations
First, it was conducted among men living and working in an urban setting (Almaty), which may limit the generalizability of the findings to men in smaller towns or rural areas of Kazakhstan. Second, data were collected through self-reports, which may introduce information bias, including socially desirable responses or recall inaccuracies. Third, the cross-sectional design does not allow causal inferences to be drawn between the identified factors and men’s health-seeking behavior. Fourth, although socio-professional groups were considered, there may be substantial heterogeneity within these groups that was not fully explored.
Future Directions
PHC in Kazakhstan has a medical and preventive department that carries out timely screening and provides counseling in the form of educating patients about a healthy lifestyle and health promotion, thereby increasing the level of health literacy. Evidence from international studies suggests that health system design and accessibility play a significant role in men’s health. PHC services were often considered inadequate to meet men’s needs, being staffed predominantly by female nurses, operating only during limited daytime hours, and remaining closed on weekends. These challenges reflect the insufficient responsiveness of health systems to accommodate men (Beia et al., 2021; Chikovore et al., 2016; Onyango et al., 2010). In addition, there is limited understanding of men’s expectations regarding male-friendly and male-oriented PHC, largely due to the lack of research in this area (Ab Aziz et al., 2022). The World Health Organization’s (WHO) European Strategy for Men’s Health 2018 recommended improving understanding of men’s health needs to improve the delivery of health services to men in the future (WHO, 2018). In Kazakhstan, it is important to review PHC services by focusing on the needs of men in different occupations. Measures should be taken to improve preventive health technologies and provide information about services through workplaces, online resources, or partners (wife, girlfriend, mother) to reduce the risks of self-medication among men. For the implementation of the SDGs, it is important to develop intersectoral cooperation (Darrudi et al., 2022), which can contribute to the inclusion of interventions in the workplace, thereby improving the health of the population. In addition, the attention to health promotion and disease prevention programs should be paid more to middle-aged and working-age people, who are at greater risk of developing health problems (Finger et al., 2019; Foster et al., 2018; Khaw et al., 2022). Future research could further include examining healthy life expectancy (Kim et al., 2022) among men and conducting a comparative analysis with women in Kazakhstan. Information about the influence of social and labor factors on the likelihood of maintaining a healthy lifestyle in the local population is important for the development of public health policy, as it identifies appropriate target areas for appropriate interventions at the population level and in the workplace, among others.
Conclusion
This study highlights that men in Almaty tend to give limited attention to their health, with notable disparities in access to preventive and PHC depending on their occupational status. The findings suggest that socio-occupational factors significantly influence men’s health awareness and attitudes toward medical services. Men in low-skilled occupations demonstrated the riskiest health behaviors, the lowest levels of trust in the health care system, and more frequent visits to public polyclinics, most likely for acute conditions rather than preventive care. At the same time, even men in highly qualified positions reported gaps in knowledge about chronic diseases and self-management, underlining that health literacy challenges are not limited to vulnerable groups. Moreover, men’s engagement with health care was strongly linked to their satisfaction with service quality, adherence to medical advice, and the use of private clinics as an alternative to public care.
In light of these results, it is crucial to adapt PHC approaches by considering the working conditions and professional diversity of the male population. Targeted health education and the development of male-friendly PHC services can contribute to improving health literacy and health outcomes among men. Policymakers and health care providers should prioritize interventions that reduce structural and perceptual barriers for men, particularly those in physically demanding or low-skilled occupations. Future research should further explore these associations and test tailored interventions in real-world PHC settings.
Footnotes
Ethical Considerations
The study protocol was reviewed by the Local Ethics Commission of the Asfendiyarov Kazakh National Medical University (IRB00011496), who issued a conclusion on approval of the study [Protocol No. 4 (140) of the meeting of ethics commission experts dated May 3, 2023]. All participants were informed about the purpose of the study and provided written informed consent prior to participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.