
Abstract
Male infertility is an escalating global health concern, yet it remains under-researched in Bangladesh. The factors contributing to this issue have not been thoroughly studied. This study aims to identify the factors associated with male infertility in the Chuadanga district of the Khulna division of Bangladesh. A cross-sectional study design was employed, involving 690 male participants seeking infertility treatment at community clinics and hospitals within the district. Participants were recruited through a two-stage sampling technique and interviewed using a structured questionnaire. The infertility status of the males served as the outcome variable, while sociodemographic characteristics, contextual factors, lifestyle behaviors, and health-related information were treated as explanatory variables. Data analysis employed descriptive statistics, Chi-square tests, and binary logistic regression models. The study revealed that 16.5% of participants were classified as infertile, while a substantial majority (83.9%) was aware of their condition. Key factors significantly associated with male infertility included educational attainment (AOR = 0.239, p = .032), occupation (AOR = .317, p = .044), monthly income (AOR = 6.324, p = 0.032), monthly expenditure (AOR = 0.184, p = 0.031), type of residence (AOR = 0.139, p < 0.001), sources of drinking water (AOR = 11.615, p < 0.001), and smoking habits (AOR = 3.304, p < 0.001) in the study area. This study underscores critical factors contributing to male infertility in Chuadanga, emphasizing the need for targeted public health interventions. Strategies should emphasize promoting healthy lifestyles, ensuring environmental safety, and improving access to clean drinking water. Raising awareness and enhancing education on male reproductive health can help improve outcomes and reduce infertility rates in low-resource settings.
Introduction
Infertility is a significant global health concern, affecting millions of individuals and couples worldwide (Leslie et al., 2023). This condition is defined as the inability to conceive after one year of regular, unprotected sexual intercourse (Leslie et al., 2023). According to the World Health Organization (WHO), approximately 15% of couples globally experience infertility (Babakhanzadeh et al., 2020). In Bangladesh, infertility is notably prevalent, with 20%–30% of couples affected (Babakhanzadeh et al., 2020). Among infertility cases, male factors account for about one-third, while a combination of male and female factors is observed in another one-third, and female factors contribute to roughly half of the cases (Babakhanzadeh et al., 2020). Despite this, societal perceptions in Bangladesh often place sole blame on females, although males are responsible for 40%–50% of infertility cases (Nahar et al., 2024).
Male infertility has unidentified causes in approximately 30%–50% of cases. Among identified causes, 10%–15% involves azoospermia, 25%–30% oligospermia, 5%–10% asthenospermia and teratozoospermia (Agarwal et al., 2021). These sperm abnormalities may result from infections of the reproductive tract, sexually transmitted diseases (STDs), varicocele, diabetes, high body mass index, cystic fibrosis, or hypogonadism (Iktidar et al., 2022). Beyond reproductive implications, male infertility poses substantial emotional, social, and financial burdens on individuals and families, often leading to relationship challenges, psychological stress, and increased expenses related to treatment (Biggs et al., 2024; Njagi et al., 2023). Male infertility has been associated with elevated risks of testicular cancer, melanoma, colon cancer, and prostate cancer (Behboudi-Gandevani et al., 2021). As a multifactorial health issue, male infertility is influenced by genetic, medical, socioeconomic, and lifestyle factors. Previous research worldwide has explored these contributors.
Genetic and medical conditions such as chromosomal abnormalities, hormonal imbalances, and diseases of the testis and prostate can impair sperm production, function, or transport (Nunes et al., 2023; Sharma et al., 2021; Touré et al., 2021). Infections such as chlamydia, gonorrhea, and tuberculosis may damage the male reproductive system or disrupt sperm production (Alzaidi & Kareem, 2024). Environmental factors, including exposure to toxins and pollutants such as pesticides, heavy metals, radiation, and endocrine-disrupting chemicals, are significant risk factors, particularly in agricultural, mining, and industrial sectors (Bala et al., 2021; Gautam et al., 2024). Lifestyle factors, including smoking, alcohol consumption, recreational drug use, obesity, stress, and mental health conditions like anxiety and depression, are also strongly associated with male infertility (Abdoli et al., 2022; Bala et al., 2021). Despite the importance of addressing male infertility, research on this issue remains limited in Bangladesh (Fatima, 2021; Fatima et al., 2022). Notably, existing studies have not systematically examined the associated factors of male infertility. This research aims to fill that gap by investigating the risk factors of male infertility in the Chuadanga district of the Khulna division in Bangladesh. The findings of this study will contribute to developing effective prevention and treatment strategies to improve male reproductive health in Bangladesh and other developing countries.
Methods
Study Area, Sampling Technique, and Sample Size
This study utilized a cross-sectional design to examine the factors associated with male infertility in the Chuadanga district of Bangladesh. Located in the southwestern Khulna division, the Chuadanga district spans an area of 1,157.42 square kilometers. The district is home to approximately 1.2 million residents across four administrative sub-districts (upazilas): Chuadanga Sadar, Alamdanga, Damurhuda, and Jibannagar. Primary data were collected between January and June 2024 using a two-stage sampling technique. In the first stage, a convenience sampling method was employed to ensure representation from all four upazilas, selecting one community clinic or hospital from each as a data collection point. The second stage involved recruiting respondents through the snowball sampling method, which effectively identifies study participants with specific criteria or populations.
The sample size in a random sampling technique can be calculated using the following formula (Khatun et al., 2022) to ensure statistical rigor and adequate representation for analysis:

where n = the requisite sample size, Z = the tabularized value (Z = 1.96 at 5% level of significance), p = the proportion of infertility (in the absence of an estimate, we consider p = .5), q = the proportion of fertility (q = 1 − p = .5), and ∈ = the margin of sampling error (∈ = 0.05). Based on the formula above (1), the required sample size is 384 male respondents.
To enhance the study’s robustness, 720 participants were initially interviewed across four selected community clinics and hospitals. The eligibility criteria for participation included being male, married for over 2 years, 18 years or older, and residing in the Chuadanga district. Data collection was conducted through structured face-to-face interviews utilizing a pretested questionnaire. This questionnaire gathered participants’ sociodemographic characteristics, contextual factors, lifestyle behaviors, and health-related data. To ensure the quality and reliability of the data, inadequate responses and duplicated or displayed potential biases were excluded. Following this rigorous vetting process, data from 690 participants were ultimately deemed valid and were included in the final analysis.
Outcome Variable
The primary outcome variable in this study was male infertility, which is defined as a man’s inability to impregnate his female partner after one year of regular, unprotected sexual intercourse. In this study, male infertility was assessed through self-reported data from the participants regarding their own and their partners’ inability to conceive for at least 1 year. During the face-to-face interviews, participants were asked a direct question to ascertain the presence or absence of male infertility. This variable was then dichotomized, assigning a value of 1 to indicate the presence of male infertility and 0 to represent its absence.
Explanatory Variables
This study considered a range of explanatory variables, including various sociodemographic characteristics, contextual factors, lifestyle-related behaviors, and health-related information. The explanatory variables were selected based on their potential association with male infertility (Fatima et al., 2022; Iktidar et al., 2022; Marić et al., 2021; Parvez & Hussain, 2025; Sharif et al., 2020; Snow et al., 2022). A detailed list of the explanatory variables and their specific classifications can be found in Appendix.
Statistical Analysis
Descriptive statistics were initially employed to explore the background characteristics of the study participants. Subsequently, Chi-square tests were applied to examine the associations between various factors and male infertility. To identify the key factors associated with male infertility, binary logistic regression models (Khatun et al., 2022) were utilized. The formula for the binary logistic regression model is as follows:

where ln(p/1 − p) is the natural logarithm of the odds of the binary dependent variable (i.e., the logit); β0 is the intercept; β1 to βk are the coefficients for the explanatory variables; X1 to Xk are the explanatory variables; p is the probability of the binary dependent variable taking the value 1 (i.e., the success or event occurrence).
Multicollinearity was evaluated by analyzing the standard errors (SEs) of the regression coefficients in the logistic regression analyses. An SE exceeding 2.0 suggests multicollinearity among the independent variables. The SEs for the independent variables in the adjusted model were less than 1.0, signifying the absence of multicollinearity (Islam et al., 2024).
Results
Background Characteristics
As seen from Table 1, the highest number of participants (25.2%) were in the age group of 35 to 39 years. The distribution of body weight showed that 39.0% of participants weighed between 65 and 74 kg. Regarding educational qualifications, the most prevalent category was primary education (24.3%), followed by HSC/ Diploma holders (21.0%). 36.1% of participants were employed in service-related jobs, while 35.4% were engaged in business. More than half (58.4%) of participants lived in nuclear families. Sleep patterns showed that more than half of the participants (57.1%) slept 6 to 7 hours per night, and 52.2% reported never smoking. A majority of the participants (86.5%) reported regularly consuming nutritious food, while 77.2% admitted to not engaging in regular physical exercise.
Association of Background Characteristics and Male Infertility in Chuadanga District (n = 690).

Notes. kg, Kilogram; SSC, Secondary school certificate; HSC, Higher secondary certificate; BSc, Bachelor of science; MSc, Master of science; BDT, Bangladeshi taka; p-values are of chi-square tests.
Regarding infertility status, approximately 16.5% of the participants reported being infertile. Knowledge of male infertility was widespread, with 83.9% of participants indicating they were aware of the condition. Concerning family planning, 87.6% of participants did not use any long-term family planning methods. Similarly, 83.0% of participants did not take any long-term medications.
Prevalence of Male Infertility by Selected Characteristics
Also seen from Table 1 that the prevalence of male infertility was notably higher among men weighing 85–94 kg (29.4%). It was also more common among those with higher educational qualifications (MSc = 30.6%) and service holders (22.5%). Men with a monthly income or expenditure of 40,000 BDT or more showed a higher prevalence, with rates of 30.0% and 32.4%, respectively. In addition, male infertility prevalence was higher among men living in brick-built houses (27.8%) and those drinking water from non-tube-well sources (31.8%), compared with tube-well (17.0%) and supply sources (7.4%). Other factors linked to a higher prevalence included smoking occasionally (23.3%), sleeping less than 8 hours (19.0%), and using a laptop/computer on their lap for 2 to 3 hours (43.8%).
Factors Associated With Male Infertility
From Table 2, we see that educational qualification, occupation, monthly income and expenditure, residence types, drinking water source, and smoking habits were significantly associated with male infertility. The odds of male infertility were 11.6 times higher among men who used other drinking water sources than those using tube-well/supply (AOR = 11.615, 95% CI = [2.634–51.206], p < .001). Men who smoked occasionally had 3.3 times higher odds of infertility than nonsmokers (AOR = 3.304, 95% CI = [1.750–6.239], p < .001). In addition, men with a monthly income of 40,000 BDT or more had 6.3 times higher odds of infertility (AOR = 6.324, 95% CI = [1.167–34.253], p = .032), while those with a monthly expenditure below 40,000 BDT had a 75%–82% lower chance of infertility. Men with no formal education had 24% higher odds of infertility compared with those with a BSc degree (AOR = 0.239, 95% CI = [0.065–0.886], p = .032). Laborers had 31% higher odds of infertility compared with those involved in agriculture (AOR = 0.317, 95% CI = [0.103–0.970], p = .044). Finally, men living in raw houses had an 86% lower likelihood of infertility (AOR = 0.139, 95% CI = [0.042–0.465], p < .001).
Logistic Regression Results on the Determinants of Male Infertility in Chuadanga District (n = 690).
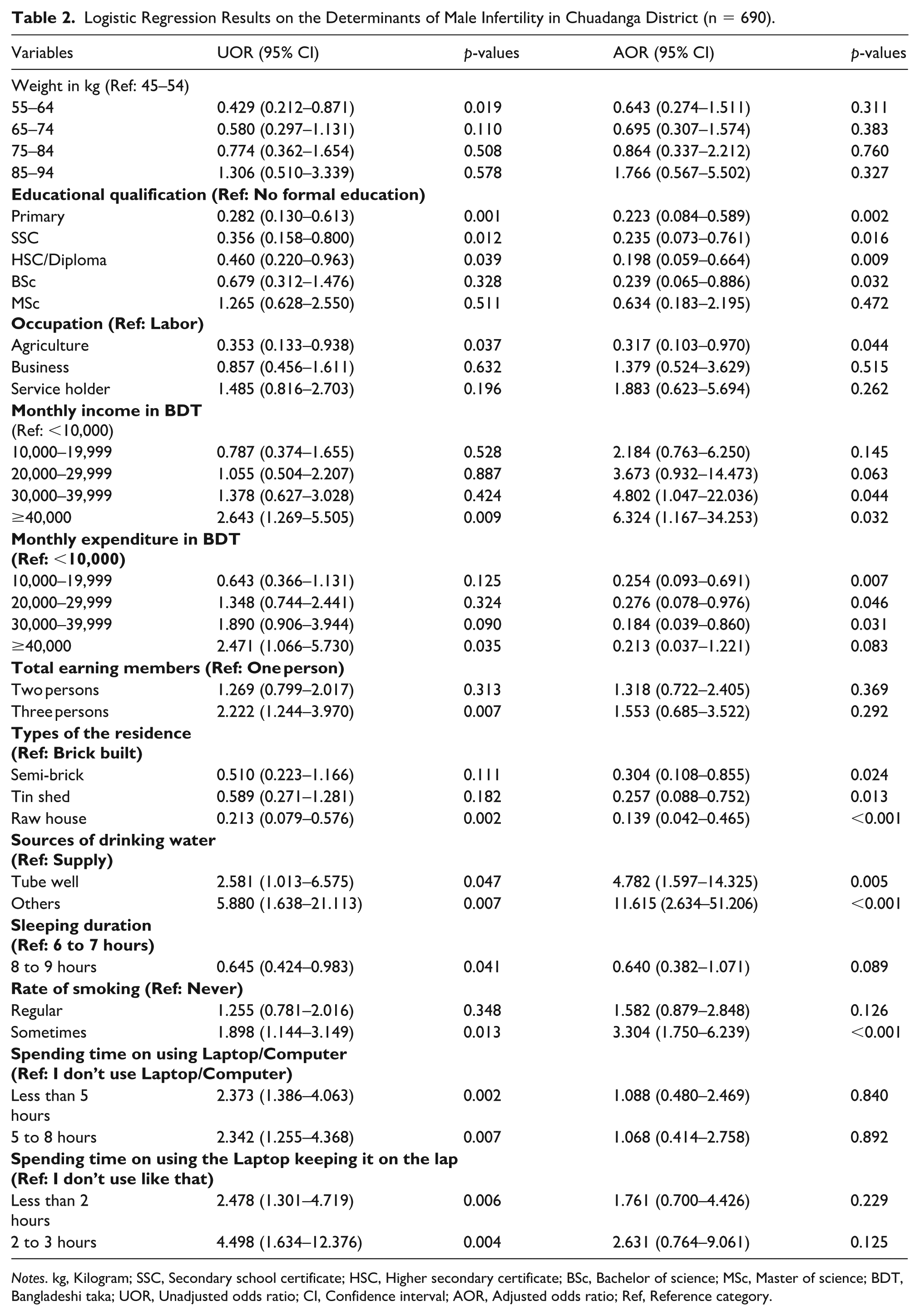
Notes. kg, Kilogram; SSC, Secondary school certificate; HSC, Higher secondary certificate; BSc, Bachelor of science; MSc, Master of science; BDT, Bangladeshi taka; UOR, Unadjusted odds ratio; CI, Confidence interval; AOR, Adjusted odds ratio; Ref, Reference category.
Discussion
This study explored the factors contributing to male infertility in the Chuadanga district of Bangladesh. The prevalence of male infertility in this study was notably high at 16.5%, with a significant association observed between male infertility and various factors, including education level, occupation, monthly income and expenditure, types of residence, sources of drinking water, and smoking habits. In addition, this study emphasizes the critical impact of environmental and lifestyle factors on male reproductive health, aligning with findings from other countries. The results underscore the complexity and multifactorial nature of this issue, adding to the growing body of evidence concerning male infertility in South Asia.
The study found that men with higher levels of education were at a lower risk of infertility, a finding consistent with previous studies that show higher educational attainment reduces the risk of male infertility (Snow et al., 2022). This could be due to the fact that educated individuals often have better access to health-related information, allowing them to adopt healthier behaviors that promote fertility (Martins et al., 2024). Education provides better employment opportunities, which can improve financial stability and access to health care, ultimately lowering the risk of infertility (Bala et al., 2021). These findings underline the importance of public health and education policies in Bangladesh and other low-income countries, suggesting that improving education access and promoting higher educational attainment could reduce male infertility rates and improve reproductive health.
Labor-intensive occupations are more strongly associated with male infertility than agricultural work, consistent with existing studies (Jeng et al., 2023; López-Botella et al., 2021). This is likely due to exposure to hazardous substances and physical strain, which can adversely affect the male reproductive system. Factors such as oxidative stress, hormonal imbalances, and sperm abnormalities are common among those engaged in physically demanding jobs, and these can lead to infertility (Marić et al., 2021). Laborers in chemical industries are particularly at risk due to exposure to harmful chemicals like pesticides and heavy metals, which have been linked to decreased sperm quality (Parvez & Hussain, 2025). Laborers, due to time away from their families, frequent travel, irregular working hours, and job dissatisfaction, face an increased risk of STDs and stress, which contribute to hormonal imbalances and infertility (Abdoli et al., 2022; Ahn et al., 2021). This highlights the need for targeted occupational health interventions and better working conditions to mitigate these risks.
Men with higher incomes and lower expenditures were also found to be at increased risk of infertility. Previous research has suggested that higher socioeconomic status may contribute to male infertility due to increased stress levels, which can negatively affect sperm quality (Majid et al., 2025; Odetayo et al., 2024). Men in higher income brackets are more likely to engage in ghoulish lifestyle behaviors, including smoking and excessive alcohol consumption, which can damage the reproductive systems (Bundhun et al., 2019). This study corroborates the findings that smoking, mainly occasional smoking, is a significant risk factor for male infertility. Smoking is well-documented as a contributor to decreased sperm concentration, motility, and morphology (Osadchuk et al., 2023; Rehman et al., 2019). Toxic substances in cigarette smoke, including nicotine, can also damage sperm deoxyribonucleic acid (DNA), increasing the risk of genetic abnormalities and infertility (Bundhun et al., 2019). Therefore, these results suggest the importance of promoting healthy lifestyle choices and providing education and counseling on the risks of smoking and alcohol consumption, particularly among higher-income men.
The study found that living in brick-built houses and using unimproved sources of drinking water were associated with higher rates of male infertility. Environmental factors such as exposure to pollutants and toxins have long been recognized as detrimental to male fertility. Brick-built houses, often found in industrial or urban areas, may be exposed to higher levels of air pollution, which has been linked to reduced sperm quality (Margiana et al., 2025). Notably, unimproved drinking water sources, such as rivers or lakes, may contain harmful chemicals like heavy metals and pesticides that negatively affect sperm quality (Gautam et al., 2024). Poor sanitation and water contamination can also lead to infections that damage the male reproductive system, further increasing the risk of infertility (Goulart et al., 2020). This emphasizes the need for interventions aimed at improving environmental conditions, including better access to safe drinking water and proper sanitation in the study area.
This study had a notable limitation. The cross-sectional design limits the ability to establish causal relationships between risk factors and male infertility. In addition, the reliance on self-reported data may have introduced recall or social desirability bias, as participants may underreport sensitive behaviors. Importantly, the study’s strength lies in its large and diverse sample from Chuadanga district, enhancing the generalizability of the findings. Rigorous data collection methods, including standardized questionnaires and face-to-face interviews, ensured consistency and reliability in the responses.
Conclusion
This study highlights the multifactorial nature of male infertility in Chuadanga district, Bangladesh, with a prevalence of 16.5% and significant associations with factors such as smoking, education level, occupation, income, expenditure, residence type, and water sources. The findings underscore the critical need for targeted public health interventions aimed at enhancing reproductive health outcomes associated with male infertility in low-resource settings. There is a critical need to implement strategies such as awareness campaigns, smoking cessation programs, initiatives to mitigate environmental toxins and pollutants, the establishment of occupational health policies, and the provision of improved access to safe drinking water.
Footnotes
Appendix
Details of the Explanatory Variables.

| Explanatory variables | Measurements | Scale of measurements |
|---|---|---|
|
|
||
| Age (in years) | 20–24, 25–29, 30–34, 35–39, 40–44, 45–49 | Discrete, categorical |
| Weight (in kg) | 45–54, 55–64, 65–74, 75–84, 85–94 | Discrete, categorical |
| Educational qualification | No formal education, Primary, SSC, HSC/Diploma, BSc, MSc | Categorical |
| Occupation | Labor, Agriculture, Business, Service holder | Categorical |
| Types of the family | Nuclear, Joint | Binary |
| Monthly income (in BDT) | <10,000, 10,000–19,999, 20,000–29,999, 30,000–39,999, ≥40,000 | Discrete, Categorical |
| Monthly expenditure (in BDT) | <10,000, 10,000–19,999, 20,000–29,999, 30,000–39,999, ≥40,000 | Discrete, Categorical |
| Total earning members | 1 person, 2 persons, 3 persons | Discrete, Categorical |
|
|
||
| Types of the residence | Brick built, Semi-brick, Tin shed, Raw house | Categorical |
| Types of the toilet | Raw, Sanitary, Brick built | Categorical |
| Sources of drinking water | Supply, Tube well, Others | Categorical |
|
|
||
| Sleeping duration | 6 to 7 hours, 8 to 9 hours | Categorical |
| Rate of smoking | Never, Regular, Sometimes | Categorical |
| Drinking alcohol | No, Yes | Binary |
| Spending time on watching television (TV) | I don’t watch TV, Less than 2 hours, 2 hours & above | Categorical |
| Spending time on using Laptop/Computer | I don’t use Laptop/Computer, Less than 5 hours, 5 to 8 hours, | Categorical |
| Spending time on using the Laptop keeping it on the lap | I don’t use like that, Less than 2 hours, 2 to 3 hours | Categorical |
| Types of underpants | I don’t use that, Loose, Normal, Tight | Categorical |
| Regular exercise | No, Yes | Binary |
| Regularly eat nutritious food | No, Yes | Binary |
|
|
||
| Knowledge about male infertility | No, Yes | Binary |
| Worried about male infertility | No, Yes | Binary |
| Lacking microelement/vitamins in the body | Vitamin C, Vitamin E, Zinc, All of these, None of them | Categorical |
| Hormonal or pituitary gland–related problems | No, Yes | Binary |
| Diabetic | No, Yes | Binary |
| Hypertension | No, Yes | Binary |
| Long-term family planning method | No, Yes | Binary |
| Any major surgery | No, Yes | Binary |
| Currently receiving any types of medical treatment | No, Yes | Binary |
| Long-term medication | No, Yes | Binary |
Notes. kg, Kilogram; SSC, Secondary school certificate; HSC, Higher secondary certificate; BSc, Bachelor of science; MSc, Master of science; BDT, Bangladeshi taka.
Acknowledgements
The authors gratefully acknowledge the authority of community clinics/hospitals in the Chuadanga district for permitting the acquisition of data from the respondents. Special thanks to the students of the Department of Public Health, First Capital University of Bangladesh, Chuadanga, for their genuine help in data collection. Finally, we would like to gratefully acknowledge the study’s participants, reviewers, and the academic editors of this manuscript.
Ethical Considerations
The study received ethical approval from the Ethics and Compliance Committee of the Faculty of Health Science and Technology at First Capital University of Bangladesh in Chuadanga (Reference number: FCUB/FHST/02/2023/0027; date: October 28, 2023). All data collection procedures were carried out in a manner that protected the rights and confidentiality of participants. Verbal consent was obtained from each individual involved. Considerable effort was made to create a respectful and supportive environment that fostered participants’ comfort and trust throughout the data collection process. Prior to their involvement in the study, participants received thorough information regarding the study’s objectives, procedures, potential risks, and benefits. They were assured that their responses would remain confidential and anonymized, with no personally identifiable information associated with the data. Furthermore, participants were clearly informed of their right to withdraw from the study at any time without experiencing any negative consequences.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization: SI, MSI, SA, AMMI, and MIT.
Data curation: MSI, AMMI.
Formal analysis: MSI.
Funding acquisition: Not Applicable.
Investigation: SI, MSI, SA, and MIT.
Methodology: MSI.
Project administration: SI, MSI.
Resources: MSI.
Software: MSI.
Supervision: SI, MSI, and MIT.
Validation: SI, MSI, SA, AMMI, and MIT.
Visualization: Not Applicable.
Writing—original draft: MSI.
Writing—review & editing: SI, MSI, SA, AMMI, and MIT.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that underpin the findings of this study are available from the corresponding author upon a reasonable request.