
Abstract
Inclusion of fathers in research and initiatives related to maternal and infant health outcomes is limited, though fathers’ involvement with their families has been associated with positive family health outcomes. Engagement of fathers must be done with an understanding of how men view health and fatherhood. This study explores if and how fatherhood influences men’s health perceptions and health care-seeking behaviors. This observational study utilized a mixed-method approach to collect data from fathers who were either expecting or had a child under 12 months old. Fathers were invited to complete an electronic survey, and eligible fathers were invited to participate in a focus group discussion. Focus group questions covered four topic areas, and responses were qualitatively analyzed and themed by these topics. Out of 73 eligible fathers who completed the electronic survey, 13 participated in the focus groups. Physical health and mental health were mentioned more often, along with prioritizing healthy routines and habits, and self-improvement were predominant. Fathers also highlighted being positive role models and being committed to their partners. When discussing personal experiences in fatherhood, fathers focused on their family’s health over their own. Fatherhood is a rewarding and challenging time that brings many changes to men’s lives. This study demonstrates how men’s health habits may change because of fatherhood. This evidence can inform how targeted programs can empower men to ensure their highest well-being while optimizing their family’s health.
Introduction
Becoming a new father can be a pivotal time for men. Going through the journey of pregnancy and childbirth with their partner has been shown to have a notable impact on their psychological and physical health (Bartlett, 2004). Fatherhood can even have long-term beneficial effects on men’s health, and the stability of a father’s relationship with his partner can impact the health outcomes of both mother and child (Behere et al., 2017; Langton & Berger, 2011; Meadows et al., 2008; Sharma, 2013). Beyond the examination of family structure and dynamics, the inclusion of fathers in research related to maternal and infant health outcomes is limited.
Limited father engagement in maternal-child health research and programming is a global trend (Panter-Brick et al., 2014). Some studies and initiatives focus on co-parenting and couple engagement, but few target fathers alone. This perceived exclusion of fathers is not merely academic. Recent qualitative studies have observed new fathers expressing their difficulty in understanding how to fulfill their role as supportive partners or find opportunities to bond with their children (Leahy-Warren et al., 2023; Sihota et al., 2019). While there is a clear desire among fathers to be engaged with their young families, they receive little support from their partners, families, or maternity care teams during pregnancy and childbirth (Leahy-Warren et al., 2023; Salvesen Von Essen et al., 2021). Moreover, this lack of support and engagement has been shown to negatively impact fathers’ mental health and reduce their involvement in perinatal care (Rominov et al., 2017). Thus, limited support and inclusion of fathers in pregnancy and childbirth have the potential to be detrimental to family health.
There is a critical need for greater engagement of fathers in perinatal care, but identifying the most effective engagement strategies may require additional evidence from researchers and training among health care providers. Existing evidence-based practice for maternity care solely focuses on research that targets mothers’ health habits and risks (Khanani et al., 2010; Meehan et al., 2014; Panter-Brick et al., 2014; Partridge et al., 2012; Salihu & Wilson, 2007). At the same time, engagement of fathers through health education and social support is an identified strategy for addressing health disparities among infants and mothers of racial and ethnic minority groups (Alio et al., 2010; Close et al., 2013; Quinn et al., 2009; Threlfall et al., 2013). The Health Resources and Services Administration also published strategies for evidence-based engagement of fathers that include individualized support, well-defined objectives, and well-trained staff (Bronte-Tinkew et al., 2012). Incorporating such strategies into perinatal care can provide holistic solutions to include men’s health in family health discussions.
There is a global trend of men having a shorter life expectancy than women, and health outcomes have been causally linked with this trend (Yan et al., 2024). Some men can be hesitant to focus on developing personal health habits (Salvesen Von Essen et al., 2021). It should then be unsurprising that new or expecting fathers are more likely to engage in perinatal care with their partner than utilize regular primary care services for their own health. These health-related behaviors highlight opportunities for engagement with fathers about their personal health care needs during prenatal care. This opportunity can also help in understanding how the transition to fatherhood affects men’s ideas on their health and health care-seeking behaviors to address the health gaps that could exist.
The purpose of this study is to explore the impact of pregnancy or being a caregiver for a newborn on the perceptions and philosophies of personal and family health among fathers. The results from the study can help to address gaps in this research and provide an understanding of effective engagement of fathers and future research.
Methods
This observational study utilized a mixed-method approach and was approved by the Indiana University Institutional Review Board (protocol # 2008426049).
Study Population and Recruitment
The target population for this study included men living in the greater Indianapolis, Indiana, area who had a pregnant partner or a child under 12 months of age. Utilizing community-based partnerships with social programs, new or expecting fathers were sought through flyers that were distributed to prenatal classes hosted by Indiana University Health prenatal care services and the Fathers and Family Center located in central Indianapolis. The flyers provided a QR code that, when scanned by a mobile device, directed fathers to a recruitment letter that explained the purpose of the study, the study activities, and compensation after completion of all study activities. Those who were interested in participating in the study were directed to the recruitment survey. Recruitment began in August 2022 and concluded in December 2023.
Data Collection
The recruitment survey collected information on fathers’ demographics and familial characteristics. Demographic indicators included age and self-identified race and ethnicity. Familial characteristics included relationship status, languages spoken, and partner’s pregnancy status. Fathers who met the study criteria and agreed to participate in a focus group were contacted by researchers to schedule a focus group session. Fathers who preferred text messages were invited to upcoming focus groups via text message. Text messages included details for in-person sessions or virtual participation. Those who preferred email received similar invitations with confirmation prompts and reminders. Each participant was asked to confirm attendance. A reminder message was sent the day before each focus group via the participant’s preferred communication method. Fathers who provided a telephone number and did not respond to the initial text message invite received at least one phone call attempt to confirm participation. If participants did not confirm attendance after three attempts, communication ceased. In-person focus group sessions were hosted at the Fathers and Family Center, and food and refreshments were provided. Virtual sessions were hosted using Zoom.
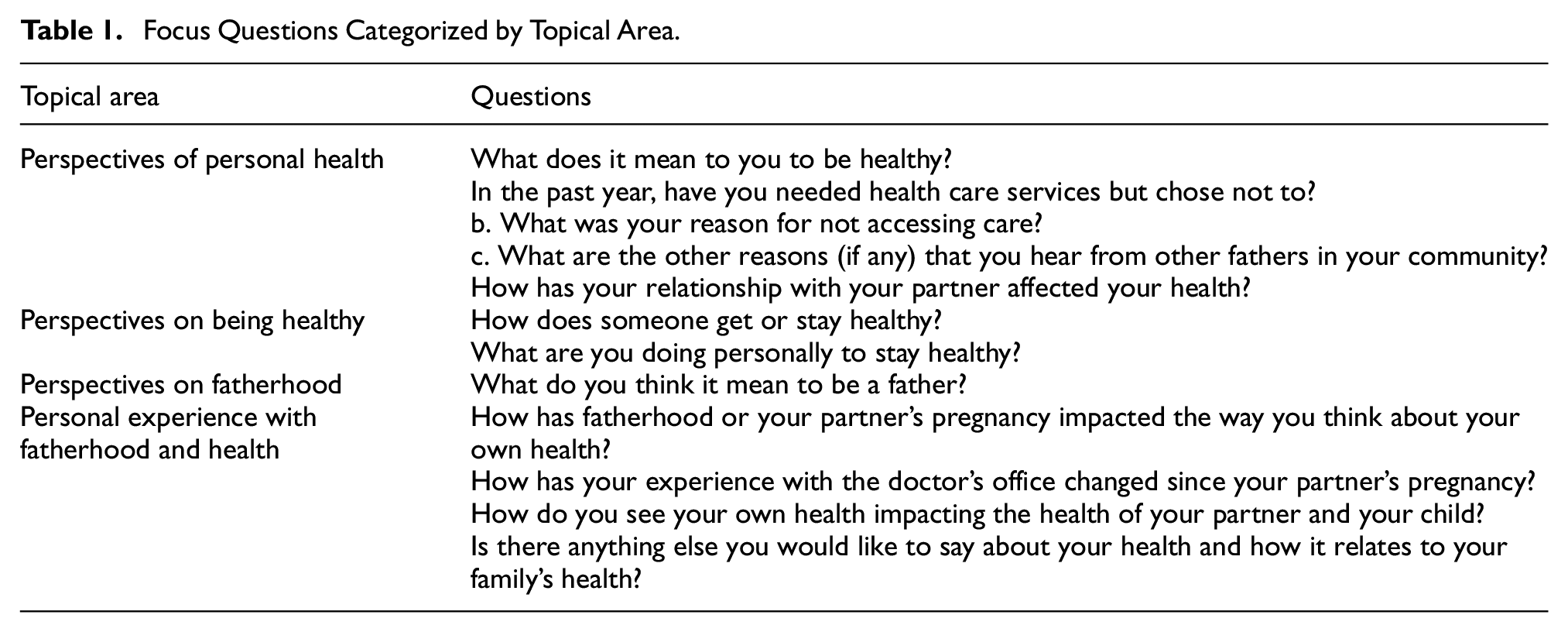
Each question asked in the focus group focused on one of four topic areas: philosophies of health, personal experiences in health, perspectives on fatherhood, and personal fatherhood experience. More information on this framework is outlined in Table 1. Focus groups lasted no longer than one hour, and fathers were provided a $40 Walmart gift card at the conclusion of the focus group.
Focus Questions Categorized by Topical Area.
Study Analysis
Descriptive statistics of demographics were conducted for the quantitative data collected from electronic surveys. An examination of all fathers who completed the recruitment survey identified whether any notable differences existed between those who participated in the focus groups and those who did not. No statistical tests were conducted due to the small number of fathers who completed all study activities.
Qualitative analysis of focus group data included a multistep approach. Two researchers individually reviewed each response to questions under each topic area and assigned themes that captured the basic ideas conveyed in each question. Next, the entire research team convened to review the themes and refine them based on consensus. The final themes were grouped based on the topic areas into which the original questions were grouped.
Results
A total of 87 fathers indicated in the recruitment survey that they were interested in participating in this study. After completing the recruitment survey, 73 fathers were identified as eligible to participate in the focus group, and 52 indicated that they would be interested in participating in the study. Of those interested, 35 were contacted via text message and 17 were contacted via email to schedule focus group sessions. In total, 13 attended and participated in the focus groups. Seven focus groups were hosted, with no more than three fathers attending each session. Figure 1 shows the criteria for the final study sample.
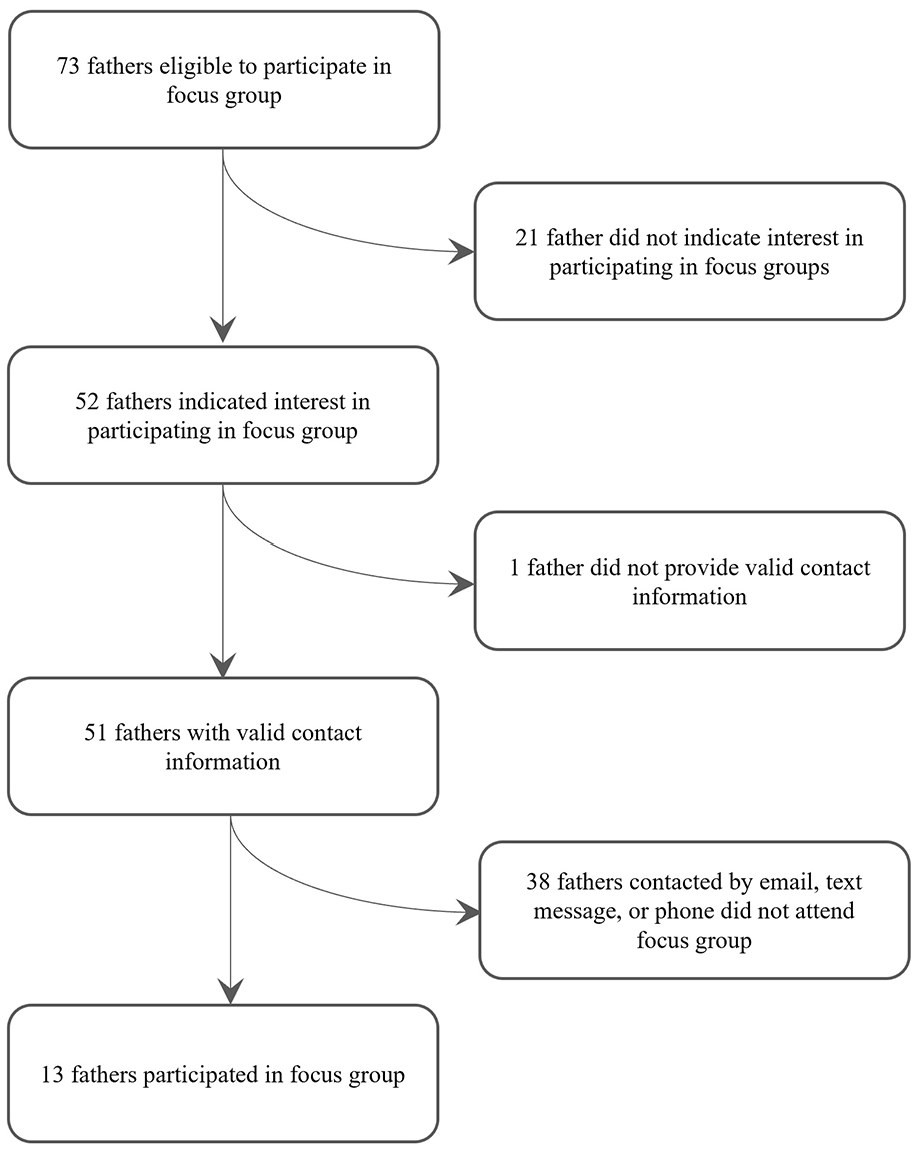
Breakdown of Final Study Sample of Fathers Who Participated in Focus Group Discussions.
Descriptive Statistics
The majority of fathers who completed the focus groups were under the age of 35 (53.9%), self-identified as White/Caucasian (61.5%), and were not Hispanic or Latino (84.6%). Most were married (92.3%), spoke English as their primary language (76.9%), and had a partner who was pregnant (76.9%).
When compared to eligible fathers who did not participate in the focus groups, there are notable differences. A greater proportion of those fathers who did not participate identified as Black or African American (40.4%). In addition, 23.3% of those who were eligible to participate in this study reported that they were living with their partner but not married. More information on the comparison of the demographics of fathers based on their participation status is found in Table 2.
Comparison of Fathers’ Demographics Based on Participation Status.

Qualitative Analysis
From the qualitative analysis of the focus group questions, several major themes emerged in each topic area (Table 3). When responding to questions regarding philosophies on health, fathers more often mentioned the importance of physical health (n = 10) and mental health/mindfulness (n = 7). One father addressed both themes in his response: “…being healthy is being balanced. So, you know, eating somewhat healthy. Getting a bit of exercise, enjoying yourself, maybe having a drink at a weekend, and being mentally healthy as well as physically healthy.”
Results from Qualitative Analysis: Perspectives of Personal Health.

Under the topic of personal experiences in health, the top themes were prioritizing healthy routines and habits (n = 13) and self-improvement (n = 12). Physical health was also a theme in this topic area. This was reflected by one father’s response: “Keeping on track, keeping focused. Not putting it on the back burner, keeping it ahead of you. And keep working past what you want so you can keep getting better.”
When asking fathers about their philosophies on fatherhood, the most common themes included being a positive role model (n = 8), being committed to their partner (n = 5), and learning from childhood experiences (n = 4). One father’s response refers to two of these themes: “I grew up without a father figure most of my life. So, for me being a father is…being a friend, being a guiding soul, being someone who’s a role model who is open and approachable…”
Finally, when discussing their individual experiences in fatherhood, all participants indicated focusing on their family’s health. For example, one father said: “…in the beginning it was just all about thinking about myself and now it’s thinking about [our son], [my partner]. What’s going on? How—why [is he] sick? Why [is she] sick. Taking care of them before I take care of myself.”
Discussion
This study contributes to the growing body of research on the perceptions of health among men and how it may be impacted by the transition to fatherhood. The participants in this study shared their personal perceptions of health and fatherhood and how these two facets of their lives intersect. Fathers demonstrated awareness of the importance of mental and physical health and more frequently highlighted personal responsibility for maintaining health than accessing professional health care services. Fathers saw their roles as focusing on and supporting the health of their partner or child rather than themselves. These findings are in alignment with existing research and highlight the importance of including fathers in the discussion of family health outcomes and understanding how fathers should be engaged during pregnancy and childbirth.
Fathers’ Philosophies on Health
Perceptions of healthy living have evolved from the historical gender roles that may have promoted less than healthy habits among men (Courtenay, 2000). However, what has not evolved is the sociologically “masculine” approach to healthy living, as men tend to define their own health routines. The same was true in our study, as participants were inclined to view health as being reliant on personal ability and self-improvement rather than seeking professional health services. This aligns with previous research that found that perceptions of health among men are influenced by social perceptions of masculinity (Ravenell et al., 2006). Understanding the underlying influences of men’s health habits is important to identifying how best to engage them in discussions of personal and family health.
Since perceptions of health among men and fathers are likely to be primarily focused on self-care (Reis de Sousa et al., 2023), there is a potential opportunity for positively influencing men’s health through individual empowerment. However, this tendency for men to rely solely on themselves for maintaining their health can also have detrimental outcomes. A national study conducted in 2023 by the Cleveland Clinic found that, even when experiencing a health concern, men still have a low likelihood of visiting their primary care provider (Buggey & Ely, 2023). This evidence demonstrates the need for balance in developing initiatives that empower men and fathers to care for their personal health and make health care services more accessible.
In addition to self-reliance, fathers in this study highlighted mental health and mindfulness as important to maintaining overall health. Mental health has become an emerging topic in men’s health, especially in the context of the COVID-19 pandemic (Buggey & Ely, 2023; Ellison et al., 2021). While mental illness is found to be less prevalent among men than women, only one-third of men who have received a mental health diagnosis utilize mental health services, compared to 51.6% of women who do so (Magas & Hoenig, 2024). The contributing factors to this gap in accessing care are likely to include the social, cultural, and personal stigmas among men surrounding mental health (Chatmon, 2020). Bringing awareness to men’s mental health is increasing within initiatives that provide support and resources for men with mental illness (Griffth et al., 2024). Awareness is only the first step, though. Research is needed to explore the most effective strategies for reducing stigma, developing supportive communities, and empowering men to seek care and maintain their mental health.
Philosophies of Fatherhood
As family dynamics have moved away from traditional roles, it should not be surprising that fathers’ parenting philosophies have evolved as well (Myers, 2013). Traditionally, the father’s role is defined as being the main family provider, authoritative, and holding primary responsibility for the family (Lamb et al., 1985). Part of this traditional function was present among fathers in this study, who frequently mentioned prioritizing the health of their family as an important part of their role. At the same time, other non-traditional views were mentioned, such as being willing to bear the responsibility of childcare. This is consistent with research showing fathers having both traditional and modern parental views and a greater willingness to share equal responsibility in childcare and bread-winning (Kaufman & Uhlenberg, 2000; Summers et al., 2006; Taylor et al., 2013). These philosophies are influenced by views on masculinity, along with cultural differences and personal experiences (Shears et al., 2006). Understanding these changing views on family dynamics and fatherhood can help inform social and public health initiatives that aim to provide resources for fathers based on their diverse needs. Some fathers may need resources that provide training on safe sleep methods and feeding, while others want classes on finances and social services. Timely availability of these resources would help to support greater family engagement among fathers.
In addition to being a primary provider and sharing parental responsibilities, participants in this study defined fatherhood as being a role model and supportive partner, and providing emotional safety to their children. Though fathers may have these desires for strong relationships with their families, they can face challenges in meeting these expectations due to our social or economic challenges (Roberts et al., 2014). Because of this, further research is needed to inform social initiatives that can provide individualized support and resources to fathers while optimizing family health outcomes.
Personal Experience with Fatherhood and Health
Philosophies of fatherhood may impact how men prepare for family life. However, philosophies can change based on personal experiences. In this study, fathers described their experience in parenthood as having a growing commitment to the well-being of their partner. This is unsurprising as previous research has shown fathers to have a more altruistic approach to their role, primarily having a greater commitment to the developmental and emotional needs of their children and partner than to their personal well-being (Chin et al., 2011; Eggebeen et al., 2010; McLaughlin & Muldoon, 2014). This observation, in combination with the knowledge that men are likely to take personal responsibility for their own health, may identify a vulnerable time for fathers in which their health is at the greatest risk.
Consistent with a previous study, some fathers in this study voiced uncertainty about their role and how they can support their families (Chin et al., 2011). This uncertainty can result in fathers experiencing stress with their new identity, which can have implications for their mental health (Baldwin et al., 2018). Increased awareness of these risks among health care and public health professionals is important for ensuring they can provide timely support and resources that can empower fathers to confidently step into their role and maintain their own health. Bringing fathers’ health care needs into discussions that occur during prenatal care and well-child visits is a low-cost effort where health care professionals can effectively identify an opportunity for intervention or to provide resources to men.
Men’s Participation in Research
Despite identifying over 50 eligible fathers who were interested in participating in this study’s focus group discussions, only 13 participated. While there has been growing interest in research focusing on men’s health, this study demonstrates that participation remains low (Law, 2019). Potential reasons that can impact men’s participation include sampling bias from researchers, recruitment methods that are more targeted to women, or men’s perceptions of research (Affleck et al., 2013; Law, 2019). Relatedly, members of population groups that are underrepresented in social research may have misconceptions that impact their willingness to fully trust researchers and engage in topics that may leave them emotionally vulnerable (Ellard-Gray et al., 2015).
The descriptive statistics examining demographic differences between the eligible fathers who participated in the focus group discussions and those who did not found notable differences. The eligible fathers who participated were more likely to be married and White as compared to those who did not participate. However, an examination of all eligible fathers shows that the authors reached a diverse group of fathers with varying relationships and family statuses. More than that, the study provided multiple modalities for participating in focus groups to accommodate barriers that fathers may face. The exclusion of unmarried men from research has been highlighted as a major gap in information on fatherhood and an area that will need to be accounted for when engaging in future studies on holistic family care (Law, 2019). Previous research has documented the barriers that can lead to demographic disparities in study participation, including limited awareness or understanding, cultural or religious views, and other logistical or financial concerns.
Diverse recruitment and participation strategies are important to ensure a representative study sample can be attained (Affleck et al., 2013). Community-based recruitment, which was incorporated in this study’s recruitment strategy, has been developed as a strategy to encourage underrepresented minorities to participate in research and community programs (Collins et al., 2018). Other validated communication strategies have included utilizing “informal gatekeepers” (e.g., friends, family, colleagues), mailing, and Facebook/social media, with informal gatekeepers being most effective (Bonevski et al., 2014; Law, 2019). The authors in this study communicated with eligible participants through text messages, and that was found to be the least successful at getting fathers to participate in focus groups. Though the findings of this study come from a small sampling, there is a demonstrated need for further exploration of effective recruitment strategies in research focused on men and fathers.
Limitations
As with any research, this study had limitations that should be noted. Because of the small study sample, no statistical analysis was possible for this study. In addition, the participation rate from this study’s recruitment survey was around 15%, and the comparative descriptive statistics showed a demographic difference based on participation status. This could point to potential participation bias. Finally, the study sample that participated in focus groups lacked the intended demographic diversity, limiting the generalizability of the study results.
Conclusions
Pregnancy and childbirth can be both rewarding and challenging, especially as parents work together in establishing new routines, responsibilities, and expectations. The findings of our study provide valuable insights into the perspectives of expecting fathers on personal and family health. As was discussed in this article, fathers are likely to experience increased emotional distress and exclusion during this time, increasing the negative impact on fathers’ mental health. Relatedly, the fathers in this study expressed greater awareness of mental health and their responsibilities to their families. More in-depth research is needed to explore the support needed by fathers to ensure the highest well-being possible, especially during pregnancy and childbirth. Moreover, further exploration is needed into strategies that can incorporate fathers in perinatal care discussions that could aid in improving family health outcomes.
Footnotes
Acknowledgements
None.
Ethical Considerations
This study was approved as exempt by the Indiana University School of Medicine Institutional Review Board.
Consent to Participate
Written informed consent was obtained from study participants prior to their inclusion in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.