
Abstract
This study aimed to examine whether contextual social deprivation is independently associated with health outcomes. A cross-sectional, multistage sampling design was employed to interview participants from six selected cities in China. A standardized questionnaire was used to collect data on individual socioeconomic characteristics and contextual social deprivation. Multilevel logistic regression models were used to assess the association between social deprivation and self-rated health. A total of 5,782 valid questionnaires were collected in this study. The prevalence of poor health was 5.3% (95% CI [4.2%, 6.3%]). Multilevel logistic regression analysis revealed a negative association between social deprivation and self-rated health. The odds ratios for contextual social deprivation scores of 2, 3, and 4 were 1.89 [1.31, 2.72], 4.21 [2.55, 6.94], and 4.63 [2.77, 7.73], respectively. This study offers new insights into the impact of social deprivation on poor health among urban male residents in China. The research emphasizes the urgent need to address poor health as a key measure to protect the well-being of socially and economically vulnerable populations.
Introduction
Ecological models emphasize that health is influenced by both individual and contextual aspects. From a socioeconomic perspective, varying individual and environmental socioeconomic statuses contribute to different health outcomes among people (Y. Yang et al., 2021). In contrast to individual socioeconomic indicators, social deprivation can be seen as a contextual variable that shapes health outcomes across populations. It influences individuals’ behaviors, access to resources, and overall well-being, reflecting the broader conditions in which people live, work, and interact. This perspective extends beyond personal socioeconomic status, underscoring the importance of the surrounding environment in shaping health.
The Exposure-Resources Theory suggests that people’s ability to meet their needs depends on the resources they have access to (Wilkinson & Marmot, 2003; X. Y. Yang, 2022). When people face more negative exposures and have fewer resources, they may be less equipped to cope with these challenges, thereby increasing the likelihood of negative health outcomes. An individual’s socioeconomic status, including education level, occupation, income, and others, represents key resources that influence health. Many studies have explored the association between individual-level socioeconomic status and health status (Macleod et al., 2006; Matthews et al., 2008; Prescott et al., 2007; H. Wang et al., 2015). However, these studies suffer from low stability and weak inter-coordination among variables, which complicates the interpretation of the findings. Social deprivation, as a composite indicator, reflects the fundamental resources available to individuals, which are closely linked to health. People living in more socially deprived areas tend to have a higher prevalence of poor health compared to those in less socially deprived areas (Blau, 1964; Lynch & Kaplan, 2000; Monroe & Simons, 1991).
Thus, there is a pressing need to investigate the influencing of social deprivation on health. Social deprivation is a well-established determinant of health, associated with a wide range of diseases (Bellizzi et al., 2024; Macleod et al., 2006; Pampalon et al., 2012; Woodward et al., 2007). It has been linked to declines in physical function; studies show that individuals living in areas with higher levels of social deprivation report significantly lower self-assessment scores in physical function and greater pain interference compared to those in less deprived areas. This disparity is consistent across multiple orthopedic sub-specialties, indicating that environmental factors play a crucial role in affecting physical health (Wright et al., 2019; T. Yang et al., 2025). Furthermore, there is a strong correlation between social deprivation and mental health issues, such as depression and anxiety. Individuals residing in more deprived communities typically report higher levels of depressive and anxiety symptoms (Eibner et al., 2004; Wright et al., 2019). Social deprivation also significantly impacts cardiovascular health outcomes, with populations experiencing higher levels of deprivation showing markedly lower life expectancy (Hawkins et al., 2012; Mackenbach et al., 2008). This body of evidence underscores the critical role that social deprivation plays in shaping health outcomes across various dimensions.
However, these studies are primarily conducted in Western societies and economically developed countries, with few conducted in economically underdeveloped regions (You et al., 2020). This gap in research is particularly concerning as social deprivation is not solely a consequence of economic conditions; it is also shaped by broader social systems and cultural factors. For instance, in many contexts, social networks, cultural attitudes toward health and well-being, and the availability of community resources can significantly influence how social deprivation manifests and affects health. Understanding these dynamics in diverse settings is essential for developing effective public health interventions and policies that address the unique challenges faced by socially deprived populations, particularly in less economically developed regions.
Social deprivation can be defined as the inability of individuals to participate fully in their community or society (Chandola & Conibere, 2015). Specifically, it refers to a condition where individuals or groups lack the resources, opportunities, and social amenities typically available to others, resulting in reduced quality of life and social exclusion. A deprivation index serves as a measure that indicates socioeconomic hardship and disadvantage through a synthetic value (Nolan & Whelan, 1996). This index generally reflects the living conditions of residents within a specific geographical or administrative area, which can be defined both topographically and normatively (Caranci et al., 2010; Lillini et al., 2012).
Since the late 1980s, China has transitioned from a centrally planned economy to a market-oriented one. This transformation has resulted in significant social changes throughout the country. The move toward a market economy has greatly enhanced economic development, leading to improved living standards and providing the Chinese population with more choices in areas such as consumption, education, healthcare, and employment. However, this transition has also given rise to several social issues, including disparities between urban and rural development, regional inequalities, and an increasing gap between the rich and the poor (Zhang et al., 2023; Zhou, 2000). Our study, conducted in the context of China, aimed to explore poor health by incorporating a social deprivation index—based on living arrangements—as a factor that may operate independently of traditional socioeconomic factors such as income, education, and occupation.
It is important to recognize that living arrangements can reveal family structure, indicate the acquisition and distribution of resources, reflect social connections and support systems, and highlight various aspects related to socioeconomic status. In the Chinese context, living arrangements are particularly significant as an independent factor from traditional socioeconomic indicators due to their cultural importance, especially in terms of family dynamics and filial piety. Central to Chinese culture is the value of family, which profoundly influences both individual lives and societal norms. Family values emphasize the collective nature of individual behavior, fostering a strong sense of obligation and responsibility to one’s family, which is regarded as a cherished virtue (T. Yang, 2025).
It should be emphasized that this study focuses on men, as they may be more susceptible to certain health issues. On one hand, traditional Chinese culture regards men as the dominant figures in society. In China, men often bear greater social and familial responsibilities, which can lead to significant mental stress (Lu, 2006). This stress may result in long-term psychological burdens that negatively impact their overall health. On the other hand, over the years, consumerism in Chinese society has led the media to strongly promote and exaggerate the superiority of women, placing men in a disadvantaged position in marital relationships and family (T. Yang, 2025). This can also negatively affect their health. In addition, men are more likely to cope with stress through unhealthy behaviors, such as smoking and excessive alcohol consumption, which can increase the risk of various health problems (T. Yang, 2010). An increasing body of evidence indicates that men and women experience stress from different sources. Men are more prone to identifying financial and work-related events as stressors, while women tend to cite family and health-related issues as their primary sources of stress (J. L. Wang et al., 2008). Currently, Chinese society is highly competitive, and in this context, men bear significant mental stress, as supported by a study (T. Yang et al., 2025), which differs from other studies (Anbumalar et al, 2017; Infortuna et al., 2020). In Chinese society, due to coping with mental stress or other purposes such as social communication driven by certain achievement motivations, men exhibit higher rates of unhealthy behaviors than women. The smoking prevalence is 52.5% in men and 2.2% in women (China CDC, 2018) problematic alcohol use is more common in men, with a prevalence of 12.7% compared to 2.9% in women (T. Yang et al., 2018). Men also have a higher prevalence of internet addiction, with 19.9% compared to 8.3% in women (p < .01) (T. Yang, Yu, et al., 2017). So men, generally experience higher mortality rates related to non-communicable diseases compared to women (GBD 2019 Diseases and Injuries Collaborators, 2020), which may contribute to a shorter life expectancy for men (Seifarth et al., 2012). Therefore, it can also be seen that men’s health issues are a very serious public health and social problem.
The information obtained from this study could be helpful in informing health policy, planning prevention strategies, and designing and implementing appropriate, targeted interventions to address men’s health and inequalities problems.
Methods
Study Type and Sampling Design
This study was observational, cross-sectional, and multilevel, using a multistage cluster sampling design. The sample cities were chosen from different regions of China. Within each city, two residential districts were randomly selected from the main urban areas. Then, four communities were randomly chosen within each district, and five building blocks were randomly selected from each community. Finally, one out of every twenty households was randomly selected from the family household registration list within each building block. The household registration list was obtained from the management office of the building block, with the inclusion criteria being households that had a male resident aged 15 or older and had lived in 1 of the 6 study cities for at least 1 year. To ensure robust random sampling methods while maintaining household privacy, the family household registration list was customized to include only the building and unit numbers within the community’s jurisdiction. In the final stage of sampling, if a household contained two or more male residents, the individual whose birth date was closest to the contact date was selected for the survey.
Data Collection
Once an individual was identified and agreed to participate, a self-administered questionnaire was provided. All responses were anonymous, and respondents were given the opportunity to ask for clarification on any survey questions. A consistent survey protocol was followed across all six cities to ensure uniformity in the interview process and data collection. The survey was administered privately to participants either at their homes or at a quiet, designated location, such as a backyard or community park. Data collection occurred on weekends, evenings, or other times that were convenient for the participants. Completing the survey took approximately 10 min. The study protocol received approval from Zhejiang university School of medicine ethics committee and verbal consent was obtained from all participants after being briefed by an investigator. Upon completing the questionnaire, respondents were given a gift worth 10 RMB (approximately 1.6 USD) as a token of appreciation (Jiang et al., 2021).
Variable Definition and Measurement
Dependent Variable
Self-reported health status has become an increasingly prevalent measure of health in empirical research, with studies showing a strong correlation with other continuous health indicators (Crossley & Kennedy, 2002). Many studies found that this method has acceptable sensitivity and specificity values (Cousins, 1997; Haddock et al., 2006; Ramos et al., 2013). The self-reported health method is also widely used in China (Liu et al., 2024; Nie et al., 2021; Yu et al., 2024). Self-rated health was evaluated using the question, “How would you assess your health compared to most people around you?” The responses were then recoded dichotomously for data analysis, with 1 representing excellent/good/fair and 2 representing poor/bad (Idler & Benyamini, 1997; Wu & Yang, 2023).
Independent Variable
Our index of contextual social deprivation, based on living arrangements, consisted of three components: residential overcrowding, lack of car ownership, and household unemployment. This combination of factors effectively and comprehensively assesses individuals’ socioeconomic status (Morris & Carstairs, 1991; Stansfeld et al., 2004; Townsend, 1987; T. Yang et al., 2022). The amount of living space was assessed by the question: “How many square meters (m2) is your home?” The response options were: “less than 10 m2,” “10 to less than 20 m2,” “20 to less than 30 m2,” or “more than 30 m2.” Residential overcrowding was defined as having less than 10 m2 of living space per person. Car ownership was measured by asking, “Does your household own a car?” The response choices were: “no,” “one,” “two,” or “three or more.” A response of “no” was categorized as a household without a car.
Household unemployment was assessed with the question: “How many unemployed persons are there in your household?” The three possible answers were: “no persons,” “one,” or “two or more.” A response of “one” or “two or more” indicated the presence of unemployed household members. Each of these living arrangement variables was dichotomized: 0 = Yes (positive indicator) and 1 = No. The total score, reflecting the number of positive responses, ranged from 0 to 3, representing varying levels of social deprivation (T. Yang, Yang, et al., 2017).
Covariates
Individual socioeconomic status included age, gender, ethnicity, educational attainment, occupation, and household income. There were two family related variables here. The first was the participants’ original family location, where they lived before the age of 13. This was categorized into three types: rural area or township, county town, county-level city, and medium or large city. The second variable, household income, was determined by asking respondents to report the average income per person in their household over the past year. Educational level, original family location, household income, and living arrangements all have the potential to reflect social deprivation in different ways.
Statistical Analysis
All data were entered into a Microsoft Excel database, and the dataset was subsequently imported into SAS (version 9.4) for statistical analysis. Descriptive statistics were calculated to determine the prevalence of poor health. Unadjusted logistic models were developed for each primary predictor. To examine the associations between social deprivation and poor health, a multiple-variable logistic regression analysis was conducted. We aim to construct a series of ecological models that incorporate individual socioeconomic status and contextual social deprivation. The first model was the base model, which included sociodemographic variables (Model 1). In the base model, family economic variables, such as original family location and household income, were added to create the family model (Model 2). The social deprivation model (Model 3) extended Model 1 by incorporating a contextual social deprivation variable based on living arrangements. Data analysis was performed using SAS 9.3, with communities serving as the clustering unit to account for intra-cluster correlation.
All analyses were weighted. The weights included: (a) sampling weights, which were the inverse of the selection probability, calculated at the city and district levels and then multiplied; (b) nonresponse weights, accounting for household and individual factors; and (c) post-stratification weights, based on age categories (<25, 25–34, 35–44, 45–54, and ≥55 years), derived from national survey estimates (National Bureau of Statistics, 2012). The final overall weight was calculated as the product of these three sets of weights.
Results
A total of 6,500 individuals were identified as potential participants for this study, of whom 6,010 (93.9%) agreed to participate in the survey. Of the 6,010 surveys collected, 5,782 (96.2%) were complete and valid. The demographic characteristics of the sample are presented in Table 1. The majority of the sample (95.6%) was of Han ethnicity; 19.9% were under 25 years old, while 23.5% were aged 55 or older. More than half of the participants (n = 3,236, 57.4%) had a high school education or less. Approximately two-thirds of the sample (63.7%) was married, and 4.9% were divorced or widowed. In terms of occupation, most participants were employed in operational roles (24.3%) or in commerce and service positions (19.5%).
Demographic Characteristics of the Sample and Poor Health Prevalence
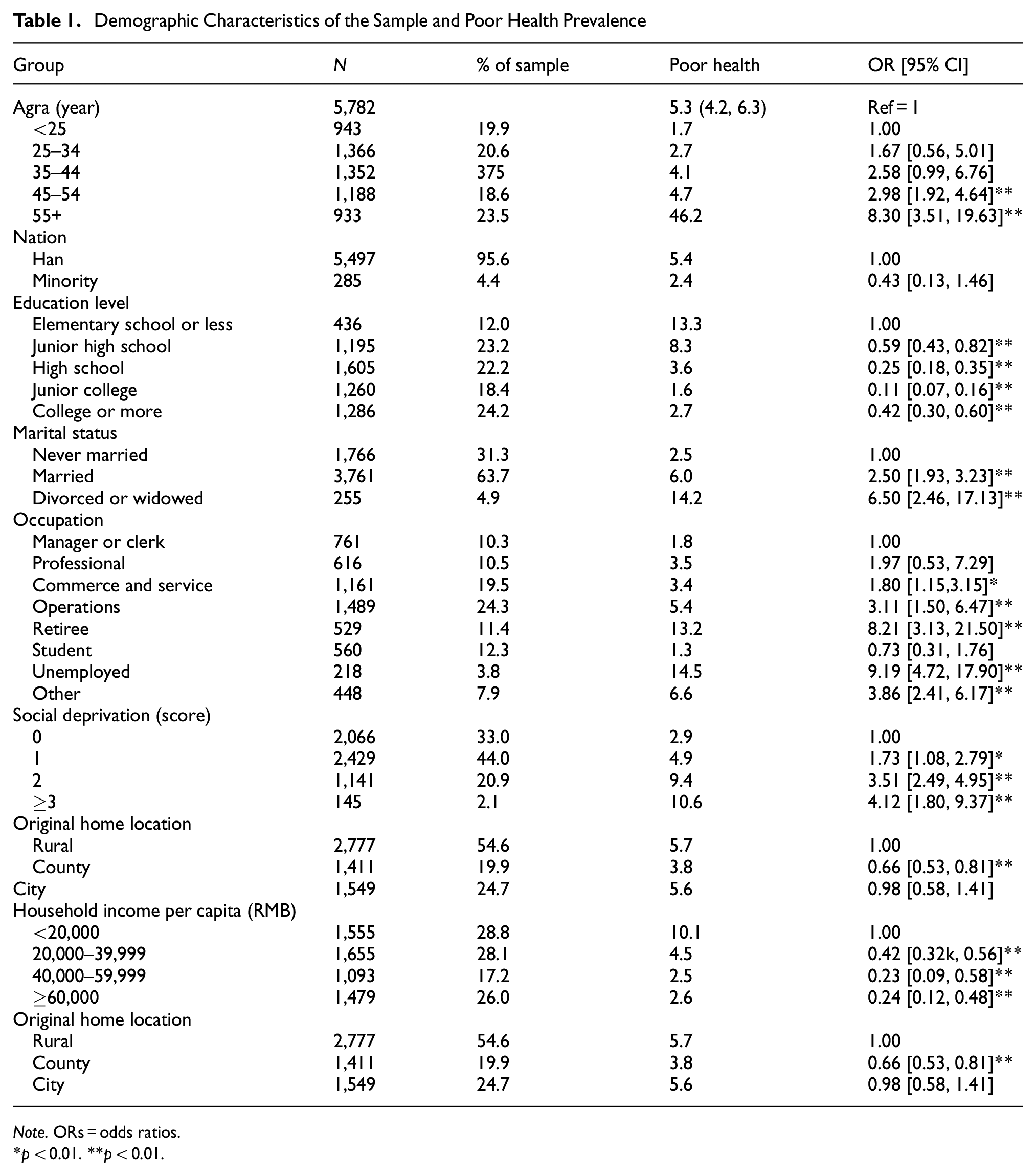
Note. ORs = odds ratios.
p < 0.01. **p < 0.01.
The prevalence of poor health was 5.3% (95% CI [4.2%, 6.3%]). Poor health prevalence varied across age, education, marital status, occupation, original home location, household income, and degree of social deprivation (Table 1). Multivariable analysis revealed that education, marital status, occupation, original home location, household income, and degree of social deprivation were all significantly associated with poor health (Table 2).
Multilevel Analysis Results of Poor Health

*p < 0.01. **p < 0.01.
Model 1 showed that compared to the group with elementary school education or less, individuals with higher education levels (junior high school, high school, junior college, and college or more) had significantly lower odds of poor health, with odds ratios (OR) of 0.77, 0.38, 0.19, and 0.76, respectively. Married participants had a higher prevalence of poor health compared to those who were never married (OR: 1.60). Participants in operational, retired, and unemployed roles had a higher prevalence of poor health compared to those in managerial or clerical positions, with ORs of 2.08, 4.48, and 5.23, respectively (Table 2).
Model 2 showed that, compared to the reference group (household income < 2,000 RMB), individuals with higher per capita household income (2,000–4,000 RMB and ≥6,000 RMB) had significantly lower prevalence of poor health, with OR of 0.45, 0.26, and 0.25, respectively. Participants living in county towns had a lower prevalence of poor health compared to those living in rural areas (OR: 0.64) (Table 2).
Model 3 indicated that individuals in the groups with social deprivation scores of 1, 2, and ≥3 had a significantly higher prevalence of poor health compared to the group with a score of zero. The ORs for these groups were 1.89 (95% CI [1.31, 2.72]), 4.21 [2.55, 6.94], and 4.63 [2.77, 7.73], respectively (Table 2).
Discussion
This study examined the association between social deprivation, based on living arrangements, and poor health status in China. Socioeconomic inequalities are widely recognized as being linked to health problems (Dey et al., 2022). Our study also incorporated several conventional socioeconomic variables, including educational level, occupation, original home location, and household income. The findings confirmed that both educational level and occupation were significantly associated with poor health, which aligns with the results of other studies (Chen & Wang, 2021; Dixon & Richter, 2020; Smith & Johnson, 2021). We found that household income was negatively associated with poor health, which supports the findings of many previous studies (Braveman et al., 2020; Marmot et al., 2021). People’s health beliefs and lifestyles are often shaped before the age of 13, making the living environment during this period crucial ( T.Yang, 2010). This study also found that participants living in county towns had a lower prevalence of poor health compared to those living in rural areas, consistent with Cottrell and McKenzie’s (2001) argument. The long-term implementation of China’s urban-rural dual economic policy has created a significant gap between urban and rural areas in terms of economic development and living standards. This gap provides strong practical support for the findings of this study. Lower socioeconomic status is associated with fewer educational opportunities, lower health awareness, limited social networks, and less safe working conditions (Cottrell & McKenzie, 2001). As a result, this combination of factors may contribute to an increased prevalence of poor health (T. Yang, Yu, et al., 2017).
This study identified a significant and novel link between social deprivation—characterized by factors such as living in a household without a car, in overcrowded conditions, or with unemployed members—and poor health. According to the fundamental cause theory of health, health outcomes are influenced by a range of intermediary processes, including health beliefs, attitudes, and behaviors toward environmental hazards, as well as the capacity to cope with risks. Individuals can mobilize their flexible resources to either avoid detrimental factors or enhance beneficial ones during these processes (Link & Phelan, 2020). More importantly, the allocation of these flexible resources—such as education, housing, financial capital, social support, and networks—tends to be uneven across society, often leading to competition for limited resources. The restricted availability and unequal distribution of these resources prevent socially deprived individuals from accessing critical health information and services. Personal social deprivation plays a pivotal role in shaping the quantity and quality of an individual’s health beliefs and behaviors, which, in turn, influences their ability to manage and reduce health risks. Those with fewer resources also face reduced opportunities, smaller social networks, limited personal freedom, poorer working conditions, and lower self-confidence when it comes to managing health challenges. Due to their lower status in a hierarchical social structure, people experiencing social deprivation often perceive themselves as having less control over their lives and diminished ability to achieve their goals. This sense of diminished control and self-efficacy can increase the likelihood of developing mood disorders and other mental health problems. Although these dynamics are speculative, they may also apply to individuals in socially disadvantaged positions (T. Yang, Yang, et al., 2017).
Understanding how contextual social deprivation impacts health is critical for mitigating the exacerbating effects it has on various health issues, as seen in other studies (Greco & Roger, 2003; Lynch & Kaplan, 2000; Monroe & Simons, 1991). This relationship can be explained by Exposure-Resources Theory (Wilkinson & Marmot, 2003; Yang, 2022). People with lower socioeconomic status or those in socially disadvantaged groups are more likely to be exposed to higher levels of health risks (Greco & Roger, 2003; Shaver & Mikulincer, 2012). Moreover, individuals in disadvantaged social positions often have lower health literacy, limited understanding of the harmful effects of risk exposure, and lack effective strategies to mitigate such exposure, leading to increased poor health status (Greco & Roger, 2003; T. Yang, Yang, et al., 2017). Especially, socially disadvantaged individuals living in harsher environmental conditions are likely to have fewer stress-reducing resources to cope with stressful events compared to their counterparts with higher socioeconomic status (T. Yang, Yang, et al., 2017).
Social theory for stress attempts to understand stress from a sociological perspective, enabling us to have a deeper and more comprehensive understanding of mental stress (T. Yang et al., 2022). China has undergone decades of reform and opening-up, resulting in significant economic growth and substantial improvements in people’s living standards. However, social competition has intensified, and the phenomenon of involution—characterized by irrational competition—has become increasingly pronounced in today’s society. A study found that over one-third of urban male residents in China experience high levels of mental stress, highlighting the severity of mental health issues within this population. The prevalence of severe mental stress among urban male residents was 42.9% (95% CI [36.3%, 49.3%]) in 2001, 43.7% [36.4%, 51.5%] in 2008, and 31.6% [25.1%, 38.1%] in 2016 (Zhang et al., 2023), indicating no significant change in mental stress during this period. However, in 1978, the per capita GDP was 385 yuan, which rose to 24,121 yuan in 2008 and reached 53,935 yuan in 2016, showcasing tremendous growth. This contradictory phenomenon between economic development and mental stress indicates the defects and imperfections in the current social system. Excessive competition and involution have led to significant mental stress for individuals, particularly affecting men as they strive to secure stable positions and provide for their families. Traditional Chinese culture often positions men as dominant figures responsible for family and social welfare, which exacerbates this pressure. Excessive mental stress and the drive for achievement can lead individuals to develop unhealthy habits, ultimately resulting in negative health outcomes. Addressing men’s health is crucial not only for individual well-being but also for the overall health of society. To mitigate these issues, various measures should be adopted to maintain social competition within reasonable limits and alleviate the mental stress caused by excessive competition. Promoting a cultural transformation that redefines traditional masculine roles is essential, allowing men to express vulnerability and seek support. Policies that prioritize men’s health should be promoted, including the following: First, providing support groups and mental health resources to help men cope with mental stress. Second, emphasizing healthy coping mechanisms and encouraging positive lifestyle choices while reducing smoking and alcohol use. Third, promoting discussions and positive media representation of men’s health issues to eliminate stigma and improve overall health outcomes. By implementing these measures, we can effectively address men’s health problems and enhance societal well-being.
The impact of increasing social ills on people’s mental stress is an undeniable reality. Scholars have analyzed issues such as unfair resource distribution, unequal competition, widening wealth gaps, and corruption, all of which contribute to unfair competition for individuals and place some in disadvantaged positions within society (Zhou, 2000). Unequal competition or unfair competition can lead to social polarization and result in a large number of disadvantaged populations in society. This study found that individuals in groups with higher social deprivation had a significantly higher prevalence of poor health, with OR of 1.89 (95% CI [1.31, 2.72], 4.21 [2.55, 6.94], and 4.63, respectively. The findings of this study emphasize the need for focused attention on the health challenges faced by disadvantaged populations. There is an urgent need for national and local health policies to address poor health among these groups. Improving the current system, addressing social disadvantages, reducing inequality in men’s health, and fostering fair competition will help enhance social well-being and reduce stress for everyone. Public health campaigns should aim to raise awareness about health risks, with a particular focus on vulnerable populations. Media outlets such as television, mobile platforms, the internet, and billboards could be powerful tools for these educational efforts.
The study has both strengths and limitations. One key limitation is its cross-sectional design, which prevents us from drawing causal conclusions about the relationship between social deprivation and poor health. However, we utilized a multilevel approach that considered both individual and regional factors, and our findings met several criteria for suggesting causality, such as the strength and consistency of certain associations. While it seems unlikely that poor health causes contextual social deprivation, a longitudinal study could provide further insights into this relationship. Second limitation is that our definition and measurement of contextual social deprivation were limited to specific living arrangements. Future studies could broaden this concept to include other living conditions, such as whether housing is rented or owned, and the presence of multiple housing units, and could also incorporate factors related to workplaces and commonly visited public spaces. Another limitation is that poor health, social deprivation, and other variables were measured using self-reported methods rather than actual observations, which may lead to some bias in the results.
Conclusion
This study provides valuable new insights into the effects of social deprivation on poor health among urban male residents in China. The findings significantly deepen our understanding of the pervasive health issues faced by socially disadvantaged groups. By highlighting the intricate relationship between social deprivation and health outcomes, this research underscores the urgent need for targeted interventions. It emphasizes that addressing poor health is crucial for safeguarding the well-being of populations that are socially and economically vulnerable. Furthermore, the study calls for policymakers to prioritize health equity initiatives, ensuring that resources and support are directed toward those most in need, ultimately fostering a healthier and more equitable society.
Footnotes
Ethical Considerations
Ethical approval was obtained from the Ethics Committee at the Medical Center of Zhejiang University (Approval number: 2014-1-017).
Consent to Participate
Verbal informed consent was obtained from all participants before data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (Grant No. 71490733).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.