
Abstract
Fathers can experience psychological distress during the paternal perinatal period. The effects of paternal perinatal psychological distress (PPPD) are multileveled. Little research is available about PPPD in first-time fathers. The purpose of this review is to explore the literature on risk factors contributing to PPPD in first-time fathers. The Arksey & O’Malley framework was used to guide this scoping review. The Population, Concept, and Context (PCC) framework was used for answering the review question “What evidence is available about factors contributing to PPPD in first-time fathers?” Five databases (CINAHL, EMBASE, MEDLINE, PsycINFO, and PubMed) were used to retrieve relevant, full-text, English references from January 01, 2020, to January 04, 2023. A data extraction tool was developed to identify risk factors assessed in the included studies. The Socio-Ecological Model (SEM) was used for analyzing the extracted data according to the four socio-ecological levels, i.e., individual, relationship, community, and societal. A total of 18 references reporting on 16 studies were included in the review. Fifty-six tools were used for assessing the risk factors contributing to PPPD in first-time fathers. Limited understanding was established about risk factors because tools lacked gender sensitivity. Risk factors aligned with 12 domains (e.g., psychological, relationship, social, and physical). Most domains corresponded with the individual level of SEM. Only two domains corresponded with the societal level of SEM. The literature indicates there are few studies about PPPD experienced by first-time fathers. This scoping review adds to the literature on the mental health care gaps for this population. Further research on measuring PPPD may improve individual and family functioning during the perinatal period.
Keywords
Introduction
Major life transitions, including changes that occur in the perinatal period for fathers, can induce psychological distress in fathers (Antoniou et al., 2021; Clark et al., 2019; Kumar et al., 2018); especially first-time fathers. Maternal mental health during the perinatal period has received considerable attention globally from existing health care systems, researchers, and policy makers (Azzam et al., 2022; Burgess, 2018). There is little data on paternal perinatal mental health (Burgess, 2018; Trindade et al., 2019). Studies conducted internationally have provided evidence that fathers experience psychological distress during their partner’s perinatal period (Antoniou et al., 2021; Azzam et al., 2022; Philpott, 2023). In this scoping review, we explored literature, globally, related to risk factors contributing to paternal perinatal psychological distress (PPPD) among first-time fathers.
Effects of Paternal Perinatal Psychological Distress
A person’s health is affected by the multileveled interactions and relationships between themselves, community, and society (Kilanowski, 2017). Scholars have described these levels of interactions and relationships as occurring within and across the intrapersonal, interpersonal, community, and societal levels PPPD, the psychological distress that some fathers may experience during the paternal perinatal period, is an important area of study because of its widespread effects within and across each of these four social-ecological levels (i.e., intrapersonal, interpersonal, community, and society).
The effects of PPPD on intrapersonal and interpersonal levels may manifest in the mental health of a father, his family, and on his relationships with his partner and children (Canadian Mental Health Association, 2016; Kumar et al., 2018; Philpott, 2023), including his child’s psychological and psychosocial behavior, and academic performance (Fisher, 2017; O’Brien et al., 2017; Philpott, 2023; Sweeney & MacBeth, 2016). At the community level, the effects of PPPD can be witnessed on fathers’ work performance (Peate, 2020), and on the economic growth of the family (Philpott, 2023; World Health Organization, 2017). At the societal level, the burden of PPPD may be observed at the national level through increased health care cost (Philpott, 2023; Takehara et al., 2020), potentially resulting in the decreased economic growth of a country (World Health Organization, 2017). Ultimately, PPPD can negatively influence all socio-ecological levels and the quality of life of a father (interpersonal level), his family (interpersonal level), community (community level), and society (societal level) in which he lives.
It is important to note that despite researchers exploring the negative effects that perinatal psychological distress can have on couples, children, families, communities, and nations; PPPD has not been explored at global or national levels (Takehara et al., 2020).
Prevalence of Paternal Perinatal Psychological Distress
The prevalence of PPPD has been reported in Australia, Brazil, Canada, China, Denmark, Finland, Germany, Greece, Hong Kong, Ireland, Israel, Italy, Japan, Mexico, Netherlands, New Zealand, Norway, Poland, Portugal, Spain, Sweden, Taiwan, Turkey, United Kingdom (UK), United States of America (USA), and Vietnam (Cameron et al., 2016; Gawlik et al., 2014; Koh et al., 2014; Lara et al., 2021; Leach et al., 2016; Mangialavori et al., 2020). PPPD is reported separately as symptoms of anxiety, or depression (Cameron et al., 2016; Gawlik et al., 2014; Koh et al., 2014). Some studies reported a combination of vague symptoms including, anxiety and depression (Lara et al., 2021; Mangialavori et al., 2020).
Symptoms of Anxiety
In a systematic review of paternal perinatal anxiety disorders, 43 studies identified from five databases; PubMed, PsycINFO, Cochrane, SCOPUS, and Web of Science, were reviewed (Leach et al., 2016). The sample size of the included studies ranged from 37 to 739 fathers. Prevalence of paternal perinatal anxiety disorders across the reviewed studies ranged from 4.1% to 16.0% during the antepartum period and 2.4% to 18.0% during the postpartum period.
Symptoms of Depression
Symptoms of perinatal depression in expectant fathers have been documented in multiple countries (Gawlik et al., 2014; Koh et al., 2014). This research includes survey-based observational studies conducted in Germany and Hong Kong (Gawlik et al., 2014; Koh et al., 2014). A longitudinal survey conducted in Germany documented the prevalence of paternal perinatal depression among a sample of 102 expectant fathers (Gawlik et al., 2014). Perinatal depression was experienced by 9.8% (n = 10) of the fathers and 7.8% (n = 8) of fathers experienced postnatal depression. In addition to documenting rates of depression, the study explored the connection between depression and birth-related and future concerns. In Hong Kong, the prevalence and risk factors of paternal perinatal depression and associations between antepartum and postpartum depression among expectant fathers were studied (Koh et al., 2014). A total of 622 expectant fathers were recruited and only 187 (30.1%) of them completed the survey at all three study timepoints. A statistically significant number of expectant fathers experienced depression during the perinatal period [F(2, 156) = 51.56, p < .000], and the fathers who experienced paternal antenatal depression were more likely to experience postnatal depression. An updated meta-analysis was conducted regarding the prevalence of perinatal depression among fathers (Cameron et al., 2016). The meta-analysis included 74 studies (n = 41,480 participants), which were identified from four electronic databases, namely CINAHL with Full Text, PsycINFO, Medline, and Health Source: nursing/academic edition. The studies included were conducted in 23 countries (i.e., Australia, Brazil, Canada, China, Denmark, Finland, Germany, Greece, Ireland, Italy, Japan, Netherlands, New Zealand, Norway, Poland, Portugal, Spain, Sweden, Taiwan, Turkey, UK, USA, and Vietnam); from five continents. The study determined that the meta-prevalence of perinatal depression in fathers was 8.4% (95% confidence interval [CI], 7.2%–9.6%; Cameron et al., 2016).
Combinations of Symptoms
A cross-sectional study for early signs of paternal perinatal affective disorder in expectant fathers (n = 350, 82.74%) was conducted in Italy (Mangialavori et al., 2020). The study determined that 14.9% (n = 52) of Italian expectant fathers experienced perinatal psychological distress. A recent cross-sectional study was conducted in Mexico to describe the prevalence of perinatal psychological distress in 997 fathers (Lara et al., 2021). The results of this study determined a moderate level of perinatal psychological distress in fathers during the prenatal period (n = 128, 25%), and during the postnatal period (n = 142, 29.5%). Serious levels of perinatal psychological distress were reported among fathers during the antenatal period (n = 5, 1%) and during the postnatal period (n = 9, 1.9%).
Summary
The existing literature indicates varied prevalence rates of PPPD among fathers. The reasons for having variations in prevalence rates of PPPD may be due to methodological and assessment issues (Azzam et al., 2022; Chavis, 2022). For example, criteria for diagnosing PPPD and official recognition of PPPD are nonexistent in the fifth and text-revision edition of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5-TR; American Psychiatric Association, 2013; Azzam et al., 2022; Bruno et al., 2020; Chavis, 2022).
In summary, fathers reported experiences of depression and anxiety that are higher during the perinatal period (Livingston et al., 2021). When fathers experience these symptoms of psychological distress, the profound impacts on mothers’ and children’s well-being and health are magnified (Glasser & Lerner-Geva, 2019). Unfortunately, there is diminished visibility of these issues in the research literature (Glasser & Lerner-Geva, 2019; Livingston et al., 2021).
The symptoms and risk factors contributing to the development of PPPD in first-time fathers have been documented but the socio-ecological levels (i.e., individual/intrapersonal, interpersonal, community, and society/societal) from where these risk factors originate have not. Exploration of the risk factors for developing PPPD among first-time fathers across socio-ecological levels may support researchers, health care professionals and policymakers to develop and implement interventions to reduce perinatal psychological distress among first-time fathers and in turn improve health outcomes for all family members. The use of the Socio-Ecological Framework (SEM) can assist researchers to identify potential sources of risk factors that contribute to the development of PPPD among first-time fathers.
Socio-Ecological Framework (SEM)
In the 1970s, Urie Bronfenbrenner presented the Socio-Ecological Model (SEM) framework which was developed into Ecological Systems Theory in the 1980s (Kilanowski, 2017; Lawrence & Ajibola, 2019). This model/theory is based on the interactions of an individual occurring with or between five ecological systems (i.e., microsystem, mesosystem, exosystem, macrosystem, and chronosystem), and its effects on human development (Kilanowski, 2017). In 1994, Bronfenbrenner revised the Ecological Systems Theory and renamed it the Bioecological Model (Evans, 2022).
The model/theory developed by Bronfenbrenner has several limitations (Evans, 2022). Research analyzing the mesosystems is inadequate in nature; hence, the scope of effects of mesosystems on human development is ill-defined (Evans, 2022). The empirical testing of this theory is difficult because the direction by which the effects were produced by these ecological systems cannot be determined (Evans, 2022). This theory assumes that human development cannot be completed in absence of the effective ecological systems (Evans, 2022). This assumption can be validated for some individuals, but not for all humans (Evans, 2022).
In 2007, based on socio-ecology theory, the Centers for Disease Control and Prevention (CDC) developed a Socio-Ecological Model (SEM) Framework for guiding its disease prevention and health promotion programs (ATSDR, 2022). This CDC framework includes four levels of factors—individual, relationship, community, and societal—that affect a person’s health (ATSDR, 2022).
Level 1: Individual (Intrapersonal)
The first level consists of biological factors and further personal characteristics affecting the health of an individual such as age, education, income, health history, etc. (ATSDR, 2022; CDC, 2022).
Level 2: Relationship (Interpersonal)
The second level assesses the effects of close relationships on an individual’s health like grandparents, parents, siblings, family members, peers, coworkers, etc. (ATSDR, 2022; CDC, 2022).
Level 3: Community
The third level investigates the effects of setting, in which social relationships take place, for example, school, neighborhood, workplace, health care facilities, worship places, etc. (ATSDR, 2022; CDC, 2022).
Level 4: Society (Societal)
The fourth level explores the effects produced by the wide-ranging societal factors on an individual’s health. Factors at this level include policies, laws, norms, values, and culture (ATSDR, 2022; CDC, 2022).
Research Purpose and Significance
Previous studies have documented that fathers experience psychological distress during the perinatal period of their partner. While searching databases for review studies, no review was found that was conducted identifying the risk factors of PPPD among first-time fathers. The purpose of this scoping review is to identify the available evidence related to the risk factors contributing to the development of PPPD among first-time fathers. The results from this scoping review will inform researchers to conduct further studies into the potentially existing gaps identified in the field of PPPD.
Methods
The original steps of the framework guided this scoping review: (Step 1) identify the research question; (Step 2) identify relevant studies; (Step 3) study selection; (Step 4) charting the data; and (Step 5) collating, summarizing, and reporting the results. A description of these steps is provided below. The results of this review and discussion of the results are reported under the fifth step of Arksey & O’Malley’s framework.
Step 1: Identify Research Question
After having thoughtful and deliberate discussions among the research team members, the question that emerged from the purpose of this review was: What evidence is available about factors contributing to PPPD among first-time fathers? The population, concept & context (PCC) framework recommended by the Joanna Briggs Institute (JBI) was used to define this review question (Peters et al., 2022); the population is first-time fathers, the concept is risk factors for developing psychological distress, and the context is the paternal perinatal period, which extends from antepartum through intrapartum to postpartum.
Step 2: Identify Relevant Studies
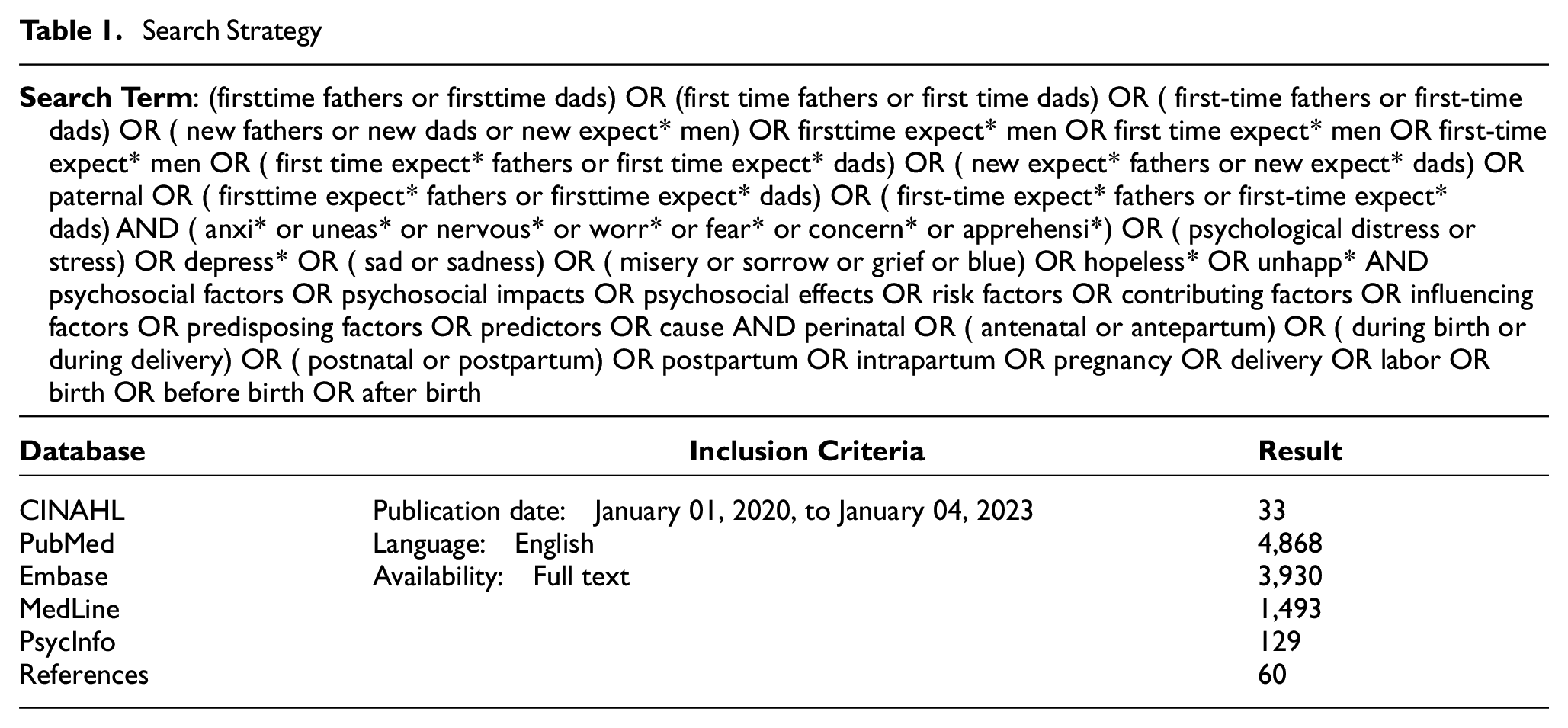
Eligibility criteria used to search for relevant studies were derived from the PCC framework (See Supplemental File 1; Peters et al., 2022). In general, studies conducted on first-time biological fathers, having opposite sex relationships, published full-text articles in English language from January 01, 2020, to January 04, 2023, were included. During the hand-search of included studies, we identified literature that included instruments that were published as early as 2000, which were included to capture the original publication date for the instruments included in those publications.
Due to the large number of studies found in the initial pilot search, the eligibility criteria were revised and four criteria that had been included earlier were excluded for this scoping review; these were: (a) any outcome of pregnancy, (b) any outcome of delivery, (c) any result of anomaly scan, and (d) intervention studies.
An initial search was conducted in the CINAHL (i.e., Cumulative Index to Nursing and Allied Health Literature) and PsycINFO databases to identify the relevant terms separately (e.g., first-time fathers, new fathers, new expectant fathers, first-time expectant men, new expectant men, paternal; anxiety, worry, fear, apprehension, concern, nervousness, depression, sad, sadness, depressed, blue, grief, unhappy, hopeless, misery, sorrow, stress, psychological distress, psychosocial factors, psychosocial impacts, psychosocial effects, risk factors, contributing factors, influencing factors, predisposing factors, predictors, and cause) which helped in developing a comprehensive search strategy (See Supplemental File 2).
After validation of the search strategy on CINAHL, it was translated and replicated for other databases. The electronic databases used for subsequent searching for published articles using MeSH (i.e., Medical Subject Headings) terms and Boolean operators included: CINAHL, EMBASE (i.e., Excerpta Medica database), MEDLINE, PsycINFO, and PubMed. Refined search terms were used for conducting this subsequent search. Finally, reference lists of all included studies were screened to find additional relevant studies. In this regard, a search strategy for the terms was developed in consultation with a health sciences librarian (See Table 1).
Search Strategy
Step 3: Study Selection
References of all identified studies were collected and uploaded into the reference manager software Zotero, version 5.0.90. A two-stage screening process was used for selecting relevant studies. During the first stage, the research team screened the title and abstract of all identified literature, to verify literature relevance to the set eligibility criteria for the scoping review. Potentially relevant full texts were retrieved. Two independent reviewers (Author 1, and Author 4) examined the full texts of selected literature, in detail, during the second stage. A third reviewer was not consulted because the first two reviewers achieved consensus about including studies through discussion among themselves.
The study selection process is presented in a flow diagram (See Figure 1; Page et al., 2021b). As depicted in Figure 1, a total of 10,513 studies were selected from the five databases (i.e., CINAHL, EMBASE, PsycINFO, MEDLINE, and PubMed), and reference lists of the studies. After removing duplicates, title and abstract screening of 10,382 studies was conducted. Full-text review was conducted for 115 studies. Out of these 115 studies, 97 studies did not meet inclusion criteria and were excluded from the scoping review. Finally, 18 articles were included in the review representing 16 distinct studies. Two studies were reported in 2 articles each from different perspectives with different research questions (Boyce et al., 2007; Condon et al., 2004; Da Costa et al., 2017, 2019).

PRISMA Flowchart
Step 4: Charting Data
A data extraction tool was developed by the researchers through in-depth discussions. There were no disagreements in developing and charting the Data Extraction Tool among team members. The data extraction tool is available on request.
Step 5: Collating, Summarizing, and Reporting Results
We initially intended to analyze the data using the Qualitative Content Analysis (QCA) technique. The data analysis process revealed that studies naturally fell into categories or themes that aligned with the Socio-Ecological Model Framework (SEM; ATSDR, 2022). Because of the similarities of patterns observed between the data and the SEM, the SEM framework was used for categorizing the data for further analysis. The SEM afforded a means to organize the discussion of the data and situate it within the context of the scoping review. Cohen’s Kappa Statistics showed an acceptable interrater reliability of 56%.
Results
The included studies (n = 16) were conducted in seven different countries. Most studies were conducted in Australia (n = 4, 25%; Boyce et al., 2007; Buist et al., 2003; Chhabra et al., 2022; Condon et al., 2004; Matthey et al., 2000); the remaining studies were conducted in China (n = 3, 18.75%; Lu et al., 2012; Mao et al., 2011; Zhang et al., 2016), United States of America (n = 3, 18.75%; Gjerdingen & Center, 2003; Leathers & Kelley, 2000; Pollock et al., 2005), Sweden (n = 2, 12.5%; Bergström, 2013; Thomas et al., 2011), United Kingdom (n = 2, 12.5%; Baldwin et al., 2019; Castle et al., 2008), Canada (n = 1, 6.25%; Da Costa et al., 2017, 2019), and Taiwan (n = 1, 6.25%; Wang & Chen, 2006). These studies reported risk factors that may have contributed to PPPD among first-time fathers (See Table 2). Most studies (n = 14, 87.5%) used quantitative research methods (Bergström, 2013; Boyce et al., 2007; Buist et al., 2003; Castle et al., 2008; Condon et al., 2004; Da Costa et al., 2017, 2019; Gjerdingen & Center, 2003; Leathers & Kelley, 2000; Lu et al., 2012; Mao et al., 2011; Matthey et al., 2000; Pollock et al., 2005; Thomas et al., 2011; Wang & Chen, 2006; Zhang et al., 2016). A few studies used qualitative research approaches (Baldwin et al., 2019), or mixed methods (Chhabra et al., 2022; See Table 2).
Summary Characteristics of Reviewed Studies (n = 16)
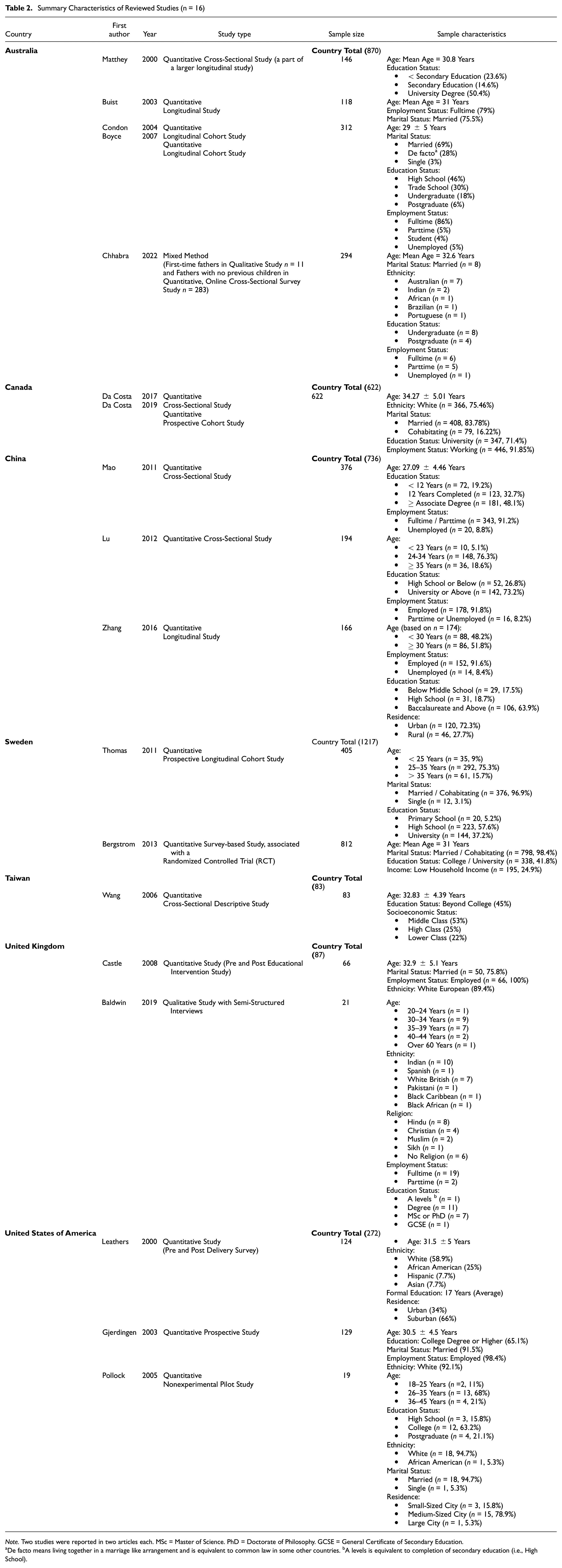
Note. Two studies were reported in two articles each. MSc = Master of Science. PhD = Doctorate of Philosophy. GCSE = General Certificate of Secondary Education.
De facto means living together in a marriage like arrangement and is equivalent to common law in some other countries. bA levels is equivalent to completion of secondary education (i.e., High School).
This scoping review included a combined sample of 3,887 men from around the world. Most were from Sweden (n = 1,217, 31.31%) followed by Australia (n = 870, 22.38%), China (n = 736, 18.93%), Canada (n = 622, 16.0%), United States of America (n = 272, 7.0%), United Kingdom (n = 87, 2.24%), and Taiwan (n = 83, 2.14%; See Table 2). Table 2 includes a summary of the sociodemographic characteristics of the men who participated in the included studies. Most participants ranged in age from 26 to 39 years old and their education status varied between lower middle level (i.e., below seventh grade) to postgraduate level (i.e., above 18 years of education).
From the studies included in this scoping review; 56 instruments were used to measure aspects of psychological distress or psychopathology according to 12 domains of risk factors that contribute to PPPD among first-time fathers (See Table 3). Conceptual categories of the instruments reviewed were developed from content analysis completed by our team. Most instruments measured aspects of the psychological domain (n = 19, 33.93%), followed by the domains related to relationship (n = 10, 17.86%), social (n = 7, 12.5%), physical (n = 5, 8.93%), family (n = 4, 7.12%), personality (n = 3, 5.36%), substance abuse (n = 2, 3.57%), quality of life (n = 2, 3.57%), gender role (n = 1, 1.79%), financial (n = 1, 1.79%), inter-role (n = 1, 1.79%), and self-esteem (n = 1, 1.79%; see Table 3). Of these 56 instruments, almost one-third of the instruments (n = 19, 33.93%) did not define all the constructs used in the instruments, or the articles describing the instrument could not be retrieved (n = 6; See Supplemental File 3).
Summary of Tools (n = 56) Used According to Constructs Measured

Across the studies reviewed, the psychological domain (n = 14, 87.5%) was the most frequently explored domain of risk factors that contributed to PPPD among first-time fathers. Additional domains explored were related to relationship (n = 8, 50%), social (n = 7, 43.75%), physical (n = 3, 18.75%), gender role (n = 2, 12.5%), quality of life (n = 2, 12.5%), family (n = 2, 12.5 %), substance abuse (n = 1, 6.25%), personality (n = 1, 6.25%), financial (n = 1, 6.25%), inter-role (n = 1, 6.25%), and self-esteem (n = 1, 6.25%; See Table 4).
Distribution of Risk Factors’ Domains (n = 12) According to the Included Studies (n = 16)

Note. Two studies reported in four papers, that is, Boyce et al. (2007) and Condon et al. (2004), are same studies, and those by Da Costa et al. (2017) and Da Costa et al. (2019) are same studies.
Discussion
This scoping review aimed to explore the existing literature related to the risk factors contributing to the development of PPPD among first-time fathers, with the intent to identify ways to support new fathers in Pakistan during this phase of their life transition. Sixteen studies were reviewed using the Arksey and O’Malley (2005) framework.
Results Interpretation
Out of fifty-six tools used in these sixteen studies, only one tool (i.e., Edinburgh Postnatal Depression Scale—EPDS) was developed for detecting postnatal depression for mothers (See Table 3).
Measurement Tools
Tools used to measure perinatal psychological distress among fathers in terms of depression, anxiety, or stress; have been developed for screening women in the perinatal period or for assessing people independent of the perinatal period (Philpott, 2020, 2023). Prevailing tools for measuring PPPD have their own limitations in making accurate diagnosis of psychological distress in fathers during the perinatal period (Philpott, 2023). For instance, experiencing inadequate sleep and fatigue are normal during the perinatal period but included as diagnostic criteria in the tools developed for assessing anxiety or depression in general populations (Philpott, 2023). Similarly, these tools have included the depressive symptoms, i.e., sadness and crying, which are mostly expressed by women, and men who express these emotions are often stigmatized as weak (Chatmon, 2020; Philpott, 2023).
Due to unavailability of a contextual (i.e., gender-specific) tool for assessing perinatal psychological distress in fathers; risk factors for developing PPPD are inadequately understood (Bruno et al., 2020; Chavis, 2022). Consequently, there is a lack of criteria for diagnosing PPPD and no official recognition of PPPD in the DSM-5-TR (5th ed.; American Psychiatric Association, 2013; Azzam et al., 2022; Bruno et al., 2020; Chavis, 2022). The development of a gender-specific tool for assessing PPPD is highly recommended with the intent to assist policymakers and health care practitioners for including PPPD in a future version of the Diagnostic and Statistical Manual of Mental Disorders (DSM). It is noteworthy to remain mindful that the purpose of including PPPD in DSM is not to medicalize it, rather to identify and modify the risk factors contributing to it, to administer nonpharmacological interventions to fathers, and to provide support to fathers and their families during perinatal period through prevention and health promotion initiatives.
SEM Levels
After reviewing the extracted data from the 16 included studies, it was observed that the 12 domains of risk factors contributing to PPPD among first-time fathers aligned with the 4 SEM levels (ATSDR, 2022; See Supplemental File 4). These levels include individual, relationship, community, and societal (ATSDR, 2022). Out of these 12 domains; most of them (n = 11, 91.67%) corresponded with the individual level of the SEM framework. Eight domains (i.e., 66.67%) aligned with the relationship and community levels, and only 2 domains (i.e., 16.67%) were associated with the society / societal level (See Supplemental File 5).
Similarly, most of the instruments (n = 39, 72.22%) studied the risk factors related to the SEM individual level, followed by instruments (n = 25, 46.30%) studying the risk factors associated with relationship, community (n = 15, 27.78), and societal levels (n = 2, 3.7%; See Supplemental File 6).
Individual
This level of the SEM includes sub-factors of biological sex, age, income, education, and history of substance abuse (Krug et al., 2002; McCloskey et al., 2011). According to this criterion, all identified domains in this scoping review fall under the SEM individual level, except the domain of Inter-Role. However, people performing roles cannot be kept in silos, without their personality and sociodemographic characteristics having an effect on their roles and health (McDowell, 2023).
Relationship
This level studies the role of relationships affecting the health of an individual (Krug et al., 2002; McCloskey et al., 2011). The included studies in this review did not address the effects of relationships on substance abuse, individual’s personality, physical, and financial situation. A person is surrounded by people, tied in different relationships with them, and may not function properly alone or in isolation. Relationships; whether romantic, friendly, spiritual and / or professional, have a central role in sustaining individuals’ mental and physical health and well-being (Kadiri, 2023).
Community
This level of SEM includes neighborhood environment and social institutions such as living, studying, working, and worship conditions and settings are equally important for impacting an individual’s health (Krug et al., 2002; McCloskey et al., 2011; Qiu et al., 2019). Studies included in this review did not consider the impact of these settings as a risk factor for developing PPPD among first-time fathers. This may represent an additional area for potential intervention to prevent psychological distress and promote family functioning and men’s mental health during the perinatal period.
Societal
The extensive effects of risk factors (e.g., policies, norms, culture, etc.) related to the societal level of SEM were not addressed in most of the domains (n = 10, 83.33%) of the included studies except the relationship and family domains. Societal factors, including policies, norms and culture have been the harsh realities of our world for ages and have deep roots that affect people’s health and mental well-being (Alegría et al., 2018; Krug et al., 2002; McCloskey et al., 2011). The lack of research into the effects of the other domains at the societal level represents an additional opportunity for future research to improve family functioning and men’s mental health during the perinatal period.
Study Implications
This scoping review has implications for researchers to further study the identified gaps in the field of PPPD. For example, most of the studies included are quantitative and have not explored the origins of risk factors contributing to experiences of PPPD in first-time fathers. Researchers can explore risk factors and their origins by using mixed method, multi-method, and qualitative study approaches, which can add contextual details to quantitative studies. Similarly, results from the reviewed studies indicate a need for tool development to assess perinatal psychological distress in men. This could support practitioners in making reliable diagnosis of PPPD in fathers and provide opportunities to intervene to promote men’s mental health.
Our scoping review findings may help policymakers to frame relevant policies for investigating and managing PPPD on national and global levels. The findings may help policymakers and educators to include the topic of PPPD in medical and nursing curriculums. These collective efforts will bring improvement in the mental health of fathers during the perinatal period, especially first-time fathers.
Limitations and Strengths
Only primary research articles published in English were reviewed which might have resulted in missing relevant articles in other languages and gray literature. To the best of the researchers’ knowledge, this is the first scoping review conducted about risk factors contributing to the development of PPPD in first-time fathers. This is the first time that origins of those risk factors have been identified using the SEM framework.
Conclusion
Articles reviewed in this scoping review indicate a need to monitor fathers for psychological distress, especially first-time fathers during the perinatal period. We used the SEM framework to document the potential origin of risk factors for developing PPPD among first-time fathers, which can assist researchers and clinicians working with new fathers to develop relevant interventions corresponding to the SEM levels and support their smooth transition to fatherhood. We identified that currently available instruments designed to measure aspects of psychological distress may be insufficient to meet the needs of fathers experiencing psychological distress during the perinatal period. There is a need to develop instruments that capture the essence of the experiences of fathers during this major life transition, especially first-time fathers. There is a need to develop interventions to support fathers who experience psychological distress during the perinatal period.
Use of the SEM framework offers clues about the levels at which interventions can be developed to address PPPD. The findings of this scoping review can help build a foundation for further research that may alleviate the psychological distress experienced by fathers, and ultimately inform interventions to improve the health and well-being of fathers and their families.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883251320035 – Supplemental material for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review
Supplemental material, sj-docx-1-jmh-10.1177_15579883251320035 for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review by Sadaf Zindani, Julie Chartrand, Jean Hannan and J. Craig Phillips in American Journal of Men's Health
Supplemental Material
sj-docx-2-jmh-10.1177_15579883251320035 – Supplemental material for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review
Supplemental material, sj-docx-2-jmh-10.1177_15579883251320035 for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review by Sadaf Zindani, Julie Chartrand, Jean Hannan and J. Craig Phillips in American Journal of Men's Health
Supplemental Material
sj-docx-3-jmh-10.1177_15579883251320035 – Supplemental material for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review
Supplemental material, sj-docx-3-jmh-10.1177_15579883251320035 for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review by Sadaf Zindani, Julie Chartrand, Jean Hannan and J. Craig Phillips in American Journal of Men's Health
Supplemental Material
sj-docx-4-jmh-10.1177_15579883251320035 – Supplemental material for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review
Supplemental material, sj-docx-4-jmh-10.1177_15579883251320035 for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review by Sadaf Zindani, Julie Chartrand, Jean Hannan and J. Craig Phillips in American Journal of Men's Health
Supplemental Material
sj-docx-5-jmh-10.1177_15579883251320035 – Supplemental material for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review
Supplemental material, sj-docx-5-jmh-10.1177_15579883251320035 for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review by Sadaf Zindani, Julie Chartrand, Jean Hannan and J. Craig Phillips in American Journal of Men's Health
Supplemental Material
sj-docx-6-jmh-10.1177_15579883251320035 – Supplemental material for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review
Supplemental material, sj-docx-6-jmh-10.1177_15579883251320035 for First-Time Father’s Risk Factors of Paternal Perinatal Psychological Distress: A Scoping Review by Sadaf Zindani, Julie Chartrand, Jean Hannan and J. Craig Phillips in American Journal of Men's Health
Footnotes
Author Contributions
SZ and JCP examined the full texts of selected literature, in detail. SZ interpreted the selected studies and made a major contribution in writing the manuscript. All authors edited, reviewed, read, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets supporting the conclusions of this article are included within the article and its Supplemental files. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.